
Abstract
Aims
It is unclear whether type 2 diabetes diagnosed in young adulthood is associated with increased severity than that occurring later in life beyond longer lifetime exposure to hyperglycemia. This study aimed at assessing the independent association of age at type 2 diabetes diagnosis with all-cause mortality.
Methods
This prospective cohort study enrolled 15,773 Caucasian patients with type 2 diabetes in 19 Italian centers in 2006–2008. Cardiometabolic risk profile and presence of complications and comorbidities were assessed at baseline and participants were stratified by quartiles of age at diabetes diagnosis. All-cause mortality was verified on 31 October 2015.
Results
Valid information on vital status was retrieved for 15,656 participants (99.3%). Patients in the lowest quartile had the longest diabetes duration, the worst glycemic control and the highest prevalence of insulin treatment, obesity, atherogenic dyslipidemia, and smoking habits. All complications were inversely associated with age at diabetes diagnosis after adjustment for age and sex, but not after further adjustment for diabetes duration. Percentages of death, Kaplan–Meier estimates, and unadjusted hazard ratios and mortality rates increased from the lowest to the highest quartile. In contrast, when adjusting for age and sex, participants falling in the lowest quartile, showed the highest mortality risk [hazard ratio 1.321 (95% confidence interval 1.196–1.460), P < 0.0001]. However, differences among quartiles disappeared after adjustment for diabetes duration, complications/comorbidities, or other cardiovascular risk factors.
Conclusions
Type 2 diabetes onset in young adulthood is associated with increased mortality that is mainly driven by longer diabetes duration favoring the development of complications.
Trial registration: ClinicalTrials.gov, NCT00715481, retrospectively registered 15 July, 2008.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
According to estimates from the Global Burden of Diseases, Injuries, and Risk Factors Study, the age-standardized prevalence of diabetes, mostly type 2 diabetes, has increased worldwide by 90.5% between 1990 and 2021 and is expected to further increase by 59.7% between 2021 and 2050 [1]. However, the rising trend in diabetes prevalence is less pronounced in high-income countries such as Europe, where the incidence of diagnosed diabetes is stabilizing or declining [2]. In this scenario, there has been also an increasing trend in the prevalence of type 2 diabetes in adolescents and young adults alongside the obesity epidemic, though again only a modest increment was seen in Europe [3, 4].
Early-onset type 2 diabetes, generally defined as diagnosed before age 40-to-45 years, is a matter of concern because it has been shown to be associated with increased mortality from any-cause, cardiovascular disease (CVD) and non-CVD as well as with increased incidence of CVD events and microvascular complications [5,6,7,8,9,10,11,12]. However, it is unclear whether people with early-onset type 2 diabetes develop complications more rapidly than those with late-onset disease, i.e., irrespective of the longer lifetime exposure to hyperglycemia and other CVD risk factors [3, 13]. Indeed, this seems the case in children and adolescents diagnosed with type 2 diabetes, as risk was shown to increase steadily over time, with complications affecting most of these people by the time of young adulthood [14], and to be higher than in coeval individuals with type 1 diabetes [15,16,17,18]. In contrast, there is no conclusive evidence for type 2 diabetes occurring in young adults, also because this age group is under-represented in prospective and randomized clinical trials [19].
The present analysis aimed at assessing the independent association of age at type 2 diabetes diagnosis with all-cause mortality in the large cohort of the Renal Insufficiency and Cardiovascular Events (RIACE) Italian Multicenter Study, which included individuals diagnosed in young adulthood.
Methods
Study design and participants
The RIACE Study was an observational, prospective, cohort study on the impact of estimated glomerular filtration rate (eGFR) on morbidity and mortality in individuals with type 2 diabetes [20].
It enrolled 15,933 Caucasian adult patients with type 2 diabetes (after excluding 160 individuals with missing or implausible values), consecutively attending 19 hospital-based, tertiary referral Diabetes Clinics of the National Health Service throughout Italy in the years 2006–2008. Exclusion criteria were dialysis or renal transplantation.
Baseline data
Baseline data were collected using a standardized protocol across participating centers [20].
Participants underwent a structured interview to collect the following information: current age, family history of diabetes, smoking status, physical activity (PA) level, known diabetes duration, severe co-morbidities, and current treatments including glucose-, lipid-, and blood pressure (BP)-lowering therapies.
Body mass index (BMI) was calculated from weight and height, whereas waist circumference was estimated from log-transformed BMI values. Then, BP was measured with a sphygmomanometer with the patients seated with the arm at the heart level.
Hemoglobin A1c (HbA1c) was measured by HPLC using DCCT-aligned methods, whereas triglycerides and total and HDL cholesterol were determined in fasting blood samples by standard colorimetric enzymatic methods. Then, non-HDL cholesterol level was computed by subtracting HDL cholesterol from total cholesterol, whereas LDL cholesterol concentration was estimated using the Friedewald formula, i.e., LDL cholesterol = total cholesterol − HDL cholesterol − (triglycerides/5) (in mg/dl).
The presence of diabetic kidney disease (DKD) was assessed by measuring albuminuria and serum creatinine, as previously detailed [20, 21]. Briefly, albumin excretion rate was obtained from 24-h urine collections or calculated from albumin-to-creatinine ratio in early-morning, first-voided urine samples; albumin concentration in urines was measured by immunonephelometry or immunoturbidimetry, in the absence of interfering clinical conditions. Serum (and urine) creatinine was measured by the modified Jaffe method, traceable to IDMS, and eGFR was calculated by the 2009 Chronic Kidney Disease Epidemiology Collaboration equation. Patients were then assigned to one of the following DKD phenotypes [22]: no DKD, albuminuric DKD with preserved eGFR, non-albuminuric DKD, or albuminuric DKD with reduced eGFR.
The presence of diabetic retinopathy (DR) was assessed in each center by an expert ophthalmologist by dilated fundoscopy [23]. Patients with mild or moderate non-proliferative DR were classified as having non-advanced DR, whereas those with severe non-proliferative DR, proliferative DR, or diabetic macular edema were grouped into the advanced, sight threatening DR category. DR grade was assigned based on the worse eye.
Previous major adverse CVD events, including myocardial infarction, stroke, foot ulcer, gangrene and non-traumatic amputation, and cerebrovascular, carotid, and lower limb revascularization, were adjudicated based on hospital discharge records by an ad hoc committee in each center [24].
All-cause mortality
The vital status of study participants on 31 October 2015 was verified by interrogating the Italian Health Card database (http://sistemats1.sanita.finanze.it/wps/portal/), which provides updated and reliable information on all current Italian residents [25].
Statistical analysis
Data are expressed as mean ± SD for continuous variables and number of cases and percentage for categorical variables. Patients were stratified by quartiles of age at type 2 diabetes diagnosis (from earliest-onset to latest-onset). Comparisons among quartiles were performed by one-way ANOVA or Kruskal–Wallis test, according to the parametric or non-parametric distribution of continuous variables, and Pearson’s χ2 test, for categorical variables. Binary non-conditional multivariable logistic regression analysis with backward stepwise selection of variables was applied to assess the independent association of presence of DKD, DR, and CVD with age at diabetes diagnosis; covariates were sex (model 1), plus age (model 2), plus other CVD risk factors, i.e., smoking status, PA level, HbA1c, BMI, triglycerides, total and HDL cholesterol, systolic and diastolic BP, and anti-hyperglycemic, lipid-lowering, and anti-hypertensive therapy (model 3), plus other complications (model 4). As interdependence of age, age at diabetes diagnosis, and diabetes duration precluded considering all three variables simultaneously, age at diagnosis was included as quartiles instead as a continuous variable in model 5.
Crude mortality rates were described as events per 1000 patient-years from start of follow-up to censoring, with 95% exact Poisson confidence intervals (CIs) and adjusted for age and sex by a Poisson regression model. Kaplan–Meier survival probabilities for all-cause mortality were estimated according to the quartiles of age at diabetes diagnosis and differences were analyzed using the log-rank statistic. The hazard ratios (HRs) and their 95% CIs were estimated by Cox proportional hazards regression with backward selection of variables. These analyses were sequentially adjusted for age and sex (model 1), plus diabetes duration (model 2), or presence of other complications (DKD phenotypes, DR grade, and any CVD), and any severe comorbidity (model 3), or other CVD risk factors (model 4).
All p values were two-sided, and a p < 0.05 was considered statistically significant. Statistical analyses were performed using SPSS version 13.0 (SPSS Inc., Chicago, IL, USA).
Results
The baseline clinical features of participants stratified by age at type 2 diabetes diagnosis are shown in Table 1. Individuals falling in quartile I (earliest-onset) were diagnosed at 20.5–45.9 years, thus substantially meeting the criterion for disease onset in early adulthood [10]. Moreover, on average, they were 5.5, 8.2, and 14.7 years younger and had a history of diabetes 4.7, 9.2, and 13.3 years longer, compared with participants falling in quartiles II, III, and IV, respectively. Values of HbA1c, BMI, waist circumference, triglycerides, albuminuria, and eGFR as well as proportion of participants of male sex, on insulin treatment, and with a family history of diabetes, current smoking habits, and a moderately/highly active lifestyle decreased from earliest-onset to latest-onset quartile. The opposite was observed for total, HDL, non-HDL, and LDL cholesterol, systolic BP and pulse pressure, and prevalence of hypertension, anti-hypertensive, anti-platelet, and anti-coagulant treatment, any comorbidity, chronic obstructive pulmonary disease, and cancer. The prevalence of albuminuric DKD with preserved eGFR and any, non-advanced and advanced DR decreased, whereas that of both nonalbuminuric and albuminuric DKD with reduced eGFR increased from earliest-onset to latest-onset quartile. Prevalence of any CVD, myocardial infarction, and any coronary event did not differ among quartiles, whereas prevalence of stroke increased and that of the other CVD events decreased from earliest-onset to latest-onset quartile.
In the unadjusted and sex-adjusted models, there was a significant association of DKD (positive) and DR (negative), but not CVD, with age at diabetes diagnosis; however, all complications were inversely associated with age at diabetes diagnosis upon further sequential adjustments for age, CVD risk factors, and other complications (Table 2). No association was observed between each complication and quartiles of age at diabetes diagnosis when adjusted for sex, age, and diabetes duration (not shown).
As previously reported, valid information on vital status was retrieved for 15,656 participants (99.3% of the cohort). Of these individuals, 12,054 (76.99%) were alive, whereas 3602 (23.01%) had deceased (follow-up duration: 7.42 ± 2.05 years, death rate: 31.02 per 1000 person-years) [22, 26].
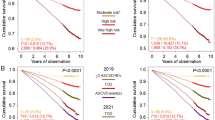
Percentages of death, Kaplan–Meier estimates, unadjusted HRs and mortality rates (Supplementary Figure S1A–B and Table 3) increased from earliest-onset to latest-onset quartile, as expected because of the increasing age. In fact, when adjusted for age and sex, participants falling in the earliest-onset quartile showed the highest mortality risk in terms of both HRs (Fig. 1A) and death rates (Table 3). However, differences among quartiles disappeared after further adjustment for diabetes duration, complications/comorbidities, or other CVD risk factors (Fig. 1B–D).

Cox proportional hazards regression by quartiles of age at type 2 diabetes diagnosis, adjusted for age and sex (A), plus diabetes duration (B), other CVD risk factors (C), or complications/comorbidities (D). HRs (95% CI) for mortality are shown for each group; quartile I includes patients with earliest-onset diabetes, whereas quartile IV includes patients with latest-onset diabetes. CVD = cardiovascular disease; HR = hazard ratio; CI = confidence interval
Discussion
This analysis of the RIACE cohort showed that type 2 diabetes diagnosed in early adulthood was associated with higher age- and sex-adjusted risk of all-cause death than that occurring later in life. However, no difference was observed when further adjusting for diabetes duration or complications/comorbidities. Of note, despite different prevalence trends across quartiles of age at diabetes diagnosis, all complications were inversely associated with age at disease onset after adjustment for age and sex, but not after further adjustment for diabetes duration.
Our study provides compelling evidence that, in a Caucasian population, the higher mortality risk associated with type 2 diabetes onset in early adulthood is attributable, at least predominantly, to the longer exposure to chronic hyperglycemia (and the other CVD risk factors clustering with it), which results in a higher burden from potentially life-threatening complications such as CVD and DKD. These results add to the existing literature by supporting previous findings obtained in Chinese people with type 2 diabetes. In fact, a prospective study from the Hong Kong Diabetes Registry showed that patients with early versus late disease onset had a higher CVD and DKD risk when adjusting for age and sex, but not when further adjusting for diabetes duration. Moreover, those with early-onset diabetes had a higher and lower cumulative incidence of all-cause mortality, CVD, and DKD at any attained age and disease duration, respectively [5]. Likewise, a cross-sectional survey using data from the China National HbA1c Surveillance System showed that the higher risk of non-fatal CVD in patients with early- versus late-onset type 2 diabetes was greatly attenuated when adjusting for diabetes duration [11]. Another cross-sectional survey in Chinese people participating in the REACTION study showed an increasing risk of CVD events with decreasing category of age at onset, but the effects of diabetes duration was not controlled for [12]. In contrast, a meta-analysis showed that each 1-year increase in age at diabetes diagnosis was associated with a 4% and 6% decreased risk of all-cause mortality and macrovascular and microvascular disease, when adjusting for current age or diabetes duration, respectively; however, these two variables could not be considered simultaneously because of the interdependence with age at diabetes diagnosis [8]. Moreover, a prospective study from the Swedish National Diabetes Registry showed that excess risk for total, CVD, and non-CVD mortality in individuals with type 2 diabetes versus matched non-diabetic controls, adjusted for sex and yearly time-updated duration, with age as the underlying time scale, was highest in patients diagnosed at ≤ 40 years and decreased with each increasing decade of age at diabetes diagnosis [7]. Similar results were obtained in two prospective studies in newly diagnosed individuals with type 2 diabetes from the Kaiser Permanente Northwest Registry [10] and the Kailuan Study [9]. Only in the latter study [9], results were further adjusted for potential confounding from CVD risk factors, though comparison with non-diabetic controls could still be affected by unmeasured confounders preferentially impacting on morbidity and mortality in older individuals. Finally, a study from Hong Kong showed that the adjusted risk for DKD associated with 5-year increase in diabetes duration was higher in people diagnosed at 20–29 years than in those diagnosed at ≥ 70 years, suggesting that early-onset diabetes amplifies the effect of disease duration on risk of DKD [27]. Indeed, a National Registry study from Australia showed that, in the first 10–15 years following type 2 diabetes diagnosis, the incidence of end-stage renal disease was highest in those with late-onset, whereas it became higher in those with early-onset only later, because they were more likely to survive to longer diabetes durations [28].
Differences in age- and sex-adjusted mortality risk among quartiles of age at diabetes diagnosis also disappeared when further adjusting for other CVD risk factors, suggesting that an adverse cardiometabolic risk profile in people with early disease onset may have favored the development of complications driving the increased risk of all-cause death. In fact, participants falling in the lowest quartile had worse glycemic control and higher prevalence of insulin treatment, obesity, atherogenic dyslipidemia, and smoking habits, but lower total and LDL cholesterol, systolic BP and prevalence of other treatments than those falling in the highest quartile. This is consistent with previous reports in patients with type 2 diabetes diagnosed in early adulthood, who were shown to have a worse cardiometabolic risk profile, except for BP, and to be treated more intensively with anti-hyperglycemic agents, but less intensively with cardioprotective drugs [5, 29, 30]. These differences in cardiometabolic risk profile between patients with early- and late-onset type 2 diabetes, which were shown to be present since diagnosis and to persist thereafter [29, 30], may reflect differences in the pathophysiology of the disease or in factors affecting diabetes care and self-management. The worse glycemic control and the greater proportion of insulin-treated individuals in this and other studies [5,6,7, 9,10,11,12, 29, 30] suggest a more severe insulin deficiency, consistent with the more rapid decline in β-cell function reported in early- versus late-onset type 2 diabetes [3, 13], though evidence is mainly derived from studies in individuals diagnosed in childhood or adolescence [31]. Moreover, the higher BMI and waist circumference in participants falling in the lowest versus the other quartiles of age at diagnosis is consistent with the central role of obesity in early disease onset [3, 13, 19], together with family history of type 2 diabetes, the effect of which may be mediated through shared genetic risk and environment favoring obesity [19]. Indeed, while the percentage of patients with grade II or III obesity was higher in the I than in the IV quartile of age at diagnosis (14.1% vs. 9.7%), that of patients with normal weight or under-weight was similar (22.6% vs. 22.4%), suggesting two extreme phenotypes of type 2 diabetes developing in early adulthood, i.e., one driven by severe obesity and the other one resembling the previously described subgroup of adult-onset diabetes in which severe insulin deficiency was associated with lower BMI and higher risk of DR [32], the prevalence of which was in fact highest in the RIACE participants falling in the lowest quartile of age at diagnosis. However, a prospective study showed that individuals with type 2 diabetes aged < 40 years were significantly more likely to be not only obese, but also from minority ethnic groups and the most deprived areas than those aged > 40 years [33], pointing to the importance of socioeconomic factors. Other factors contributing to the more severe disease phenotype when occurring in early adulthood include (a) delayed diagnosis due to a lower likelihood of opportunistic screening; (b) lower adherence to lifestyle recommendations and poorer diabetes self-care practices; and (c) less aggressive treatment owing to the underestimation of risk of complications and lack of specific guidelines, with those tailored for later-onset type 2 diabetes recommending drug prescription based on the assessment of 10-year risk, which is mainly driven by current age [3, 5, 7, 19, 34]. Finally, it was shown that the lower the age at diabetes diagnosis, the higher the prevalence of depression, anxiety and psychological distress [35], which may negatively impact on treatment adherence, thus resulting in worse cardiometabolic risk profile and poorer outcomes.
Strength of our study include the large sample size, the completeness of baseline and follow-up data and, particularly, the assessment of a wide range of clinical parameters which allowed accounting for several confounders. However, there are several limitations. First, the lack of information on the causes of death did not allow detecting differences in CVD versus non-CVD mortality. Second, the study included individuals with prevalent rather than new-onset type 2 diabetes and, hence, participants were not monitored from the time of diagnosis to evaluate trajectories of CVD risk factors and complications. Third, as assay of diabetes-specific auto-antibodies or genetic testing were not performed in all the RIACE participants at the time of diagnosis, it is possible that some cases of autoimmune or monogenic diabetes were misdiagnosed as type 2 diabetes. Fourth, the study findings may not be applicable to the general ambulatory population, as only part of the individuals with type 2 diabetes attend Diabetes Clinics in Italy. Finally, the observational design makes causal interpretation impossible.
Conclusions
This analysis in Caucasian patients with type 2 diabetes from the RIACE cohort showed that the lower the age at diabetes diagnosis, the higher the age- and sex-adjusted risk of all-cause death. However, the higher mortality risk associated with onset of type 2 diabetes in early adulthood appeared to be mainly driven by the longer disease duration and exposure to chronic hyperglycemia and other CVD risk factors, which explained the increased risk of complications and death. Differences in cardiometabolic risk profile according to age at diagnosis might also be responsible for differences in outcomes, though it is difficult to establish whether they reflect an intrinsically more aggressive disease or factors affecting diabetes care and self-management. These data point to the need for public health policies and tailored guidelines for preventing and treating early-onset type 2 diabetes to avoid premature morbidity and mortality from complications.
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- CVD:
-
Cardiovascular disease
- RIACE:
-
Renal Insufficiency and Cardiovascular Events
- eGFR:
-
Estimated glomerular filtration rate
- PA:
-
Physical activity
- BP:
-
Blood pressure
- BMI:
-
Body mass index
- HbA1c :
-
Hemoglobin A1c
- DKD:
-
Diabetic kidney disease
- DR:
-
Diabetic retinopathy
- CI:
-
Confidence interval
- HR:
-
Hazard ratio
References
GBD 2021 Diabetes Collaborators (2023) Global, regional, and national burden of diabetes from 1990 to 2021, with projections of prevalence to 2050: a systematic analysis for the Global Burden of Disease Study 2021. Lancet 402:203–234. https://doi.org/10.1016/S0140-6736(23)01301-6
Magliano DJ, Chen L, Islam RM, Carstensen B et al (2021) Trends in the incidence of diagnosed diabetes: a multicountry analysis of aggregate data from 22 million diagnoses in high-income and middle-income settings. Lancet Diabetes Endocrinol 9:203–211. https://doi.org/10.1016/S2213-8587(20)30402-2
Lascar N, Brown J, Pattison H et al (2018) Type 2 diabetes in adolescents and young adults. Lancet Diab Endocrinol 6:69–80. https://doi.org/10.1016/S2213-8587(17)30186-9
International Diabetes Federation. IDF Diabetes Atlas 2021—10th Edition. Available online at https://diabetesatlas.org/atlas/tenth-edition/. Accessed 19 Jan 2023
Chan JC, Lau ES, Luk AO et al (2014) Premature mortality and comorbidities in young-onset diabetes: a 7-year prospective analysis. Am J Med 127:616–624. https://doi.org/10.1016/j.amjmed.2014.03.018
Koye DN, Ling J, Dibato J et al (2020) Temporal trend in young-onset type 2 diabetes-macrovascular and mortality risk: study of U.K. primary care electronic medical records. Diabetes Care 43:2208–2216. https://doi.org/10.2337/dc20-0417
Sattar N, Rawshani A, Franzén S et al (2019) Age at diagnosis of type 2 diabetes mellitus and associations with cardiovascular and mortality risks. Circulation 139:2228–2237. https://doi.org/10.1161/CIRCULATIONAHA.118.037885
Nanayakkara N, Curtis AJ, Heritier S et al (2021) Impact of age at type 2 diabetes mellitus diagnosis on mortality and vascular complications: systematic review and meta-analyses. Diabetologia 64:275–287. https://doi.org/10.1007/s00125-020-05319-w
Zhao M, Song L, Sun L et al (2021) Associations of type 2 diabetes onset age with cardiovascular disease and mortality: the Kailuan study. Diabetes Care 44:1426–1432. https://doi.org/10.2337/dc20-2375
Hillier TA, Pedula KL (2003) Complications in young adults with early-onset type 2 diabetes: losing the relative protection of youth. Diabetes Care 26:2999–3005. https://doi.org/10.2337/diacare.26.11.2999
Huo X, Gao L, Guo L et al (2016) Risk of non-fatal cardiovascular diseases in early-onset versus late-onset type 2 diabetes in China: a cross-sectional study. Lancet Diabetes Endocrinol 4:115–124. https://doi.org/10.1016/S2213-8587(15)00508-2
Hu C, Lin L, Zhu Y et al (2021) Association between age at diagnosis of type 2 diabetes and cardiovascular diseases: a nationwide, population-based. Cohort Study Front Endocrinol (Lausanne) 12:717069. https://doi.org/10.3389/fendo.2021.717069
Magliano DJ, Sacre JW, Harding JL et al (2020) Young-onset type 2 diabetes mellitus - implications for morbidity and mortality. Nat Rev Endocrinol 16:321–331. https://doi.org/10.1038/s41574-020-0334-z
TODAY Study Group; Bjornstad P, Drews KL et al (2021) Long-term complications in youth-onset type 2 diabetes. N Engl J Med 385:416–426. https://doi.org/10.1056/NEJMoa2100165
Dabelea D, Stafford JM, Mayer-Davis EJ et al (2017) Association of type 1 diabetes vs type 2 diabetes diagnosed during childhood and adolescence with complications during teenage years and young adulthood. JAMA 317:825–835. https://doi.org/10.1001/jama.2017.0686
Dart AB, Sellers EA, Martens PJ et al (2012) High burden of kidney disease in youth-onset type 2 diabetes. Diabetes Care 35:1265–1271. https://doi.org/10.2337/dc11-2312
Jaiswal M, Lauer A, Martin CL et al (2013) Peripheral neuropathy in adolescents and young adults with type 1 and type 2 diabetes from the SEARCH for Diabetes in Youth follow-up cohort: a pilot study. Diabetes Care 36:3903–3908. https://doi.org/10.2337/dc13-1213
Constantino MI, Molyneaux L, Limacher-Gisler F et al (2013) Long-term complications and mortality in young-onset diabetes: type 2 diabetes is more hazardous and lethal than type 1 diabetes. Diabetes Care 36:3863–3869. https://doi.org/10.2337/dc12-2455
Misra S, Ke C, Srinivasan S et al (2023) Current insights and emerging trends in early-onset type 2 diabetes. Lancet Diabetes Endocrinol 11:768–782. https://doi.org/10.1016/S2213-8587(23)00225-5
Penno G, Solini A, Bonora E et al (2011) Clinical significance of nonalbuminuric renal impairment in type 2 diabetes. J Hypertens 29:1802–1809. https://doi.org/10.1097/HJH.0b013e3283495cd6
Pugliese G, Solini A, Fondelli C et al (2011) Reproducibility of albuminuria in type 2 diabetic subjects. Findings from the Renal Insufficiency And Cardiovascular Events (RIACE) study. Nephrol Dial Transpl 26:3950–3954. https://doi.org/10.1093/ndt/gfr140
Penno G, Solini A, Orsi E et al (2018) Non-albuminuric renal impairment is a strong predictor of mortality in individuals with type 2 diabetes: the Renal Insufficiency And Cardiovascular Events (RIACE) Italian multicentre study. Diabetologia 61:2277–2289. https://doi.org/10.1007/s00125-018-4691-2
Orsi E, Solini A, Bonora E et al (2023) Retinopathy as an independent predictor of all-cause mortality in individuals with type 2 diabetes. Diabetes Metab 49:101413. https://doi.org/10.1016/j.diabet.2022.101413
Solini A, Penno G, Bonora E et al (2012) Diverging association of reduced glomerular filtration rate and albuminuria with coronary and noncoronary events in patients with type 2 diabetes: the renal insufficiency and cardiovascular events (RIACE) Italian multicenter study. Diabetes Care 35:143–149. https://doi.org/10.2337/dc11-1380
Orsi E, Solini A, Bonora E et al (2018) Haemoglobin A1c variability is a strong, independent predictor of all-cause mortality in patients with type 2 diabetes. Diabetes Obes Metab 20:1885–1893. https://doi.org/10.1111/dom.13306
Penno G, Solini A, Bonora E et al (2018) Defining the contribution of chronic kidney disease to all-cause mortality in patients with type 2 diabetes: the Renal Insufficiency And Cardiovascular Events (RIACE) Italian Multicenter Study. Acta Diabetol 55:603–612. https://doi.org/10.1007/s00592-018-1133-z
Wu H, Lau ESH, Yang A et al (2021) Young age at diabetes diagnosis amplifies the effect of diabetes duration on risk of chronic kidney disease: a prospective cohort study. Diabetologia 64:1990–2000. https://doi.org/10.1007/s00125-021-05494-4
Morton JI, Liew D, McDonald SP et al (2020) The association between age of onset of type 2 diabetes and the long-term risk of end-stage kidney disease: a national registry study. Diabetes Care 43:1788–1795. https://doi.org/10.2337/dc20-0352
Ling J, Koye D, Buizen L et al (2021) Temporal trends in co-morbidities and cardiometabolic risk factors at the time of type 2 diabetes diagnosis in the UK. Diabetes Obes Metab 23:1150–1161. https://doi.org/10.1111/dom.14323
Steinarsson AO, Rawshani A, Gudbjörnsdottir S et al (2018) Short-term progression of cardiometabolic risk factors in relation to age at type 2 diabetes diagnosis: a longitudinal observational study of 100,606 individuals from the Swedish National Diabetes Register. Diabetologia 61:599–606. https://doi.org/10.1007/s00125-017-4532-8
Bacha F, Gungor N, Lee S et al (2013) Progressive deterioration of β-cell function in obese youth with type 2 diabetes. Pediatr Diabetes 14:106–111. https://doi.org/10.1111/j.1399-5448.2012.00915.x
Ahlqvist E, Storm P, Käräjämäki A et al (2018) Novel subgroups of adult-onset diabetes and their association with outcomes: a data-driven cluster analysis of six variables. Lancet Diabetes Endocrinol 6:361–369. https://doi.org/10.1016/S2213-8587(18)30051-2
Misra S, Holman N, Barron E et al (2023) Characteristics and care of young people with type 2 diabetes included in the national diabetes audit datasets for England. Diabet Med 40:e14940. https://doi.org/10.1111/dme.14940
Nanayakkara N, Pease AJ, Ranasinha S et al (2018) Younger people with Type 2 diabetes have poorer self-care practices compared with older people: results from the Australian National Diabetes Audit. Diabet Med 35:1087–1095. https://doi.org/10.1111/dme.13660
Liu S, Leone M, Ludvigsson JF et al (2022) Early-onset type 2 diabetes and mood, anxiety, and stress-related disorders: a genetically informative register-based cohort study. Diabetes Care 45:2950–2956. https://doi.org/10.2337/dc22-1053
Acknowledgements
The authors thank the RIACE Investigators for participating in this study (see the complete list in the Supplementary Appendix).
Funding
Open access funding provided by Università degli Studi di Roma La Sapienza within the CRUI-CARE Agreement. This research was supported by the Research Foundation of the Italian Diabetes Society (Diabete Ricerca) and the Diabetes, Endocrinology and Metabolism (DEM) Foundation, and by unconditional grants from Eli-Lilly, Sigma-Tau, Takeda, Chiesi Farmaceutici, and Boehringer-Ingelheim. The funding sources had no role in the design of the study and collection, analysis, and interpretation of data and in writing the manuscript.
Author information
Authors and Affiliations
Consortia
Contributions
MVi, EO, AS, GPe, and GPu conceived and designed the study. All authors contributed to data acquisition, analysis, or interpretation. GPu drafted the article and had full access to all the data and took responsibility for the integrity of data and accuracy of the data analysis in this study. MVi, EO, AS, MG, VG, EB, CF, RT, MVe, GPe, and AN revised the manuscript critically for essential intellectual content. All authors approved the submitted version of the manuscript and agreed to be personally accountable for the individual’s own contributions and to ensure that questions pertaining to the accuracy or integrity of any portion of the work are appropriately investigated and resolved.
Corresponding author
Ethics declarations
Conflict of interest
MVi: lecture fees from MundiPharma and Novo Nordisk. EO: consultant fees from Eli Lilly and Novo Nordisk, and lecture fees from Astellas. AS: consultant fees from Axxam, Bayer, and Novo Nordisk, and lecture fees from Eli Lilly, Novo Nordisk, and Sanofi-Aventis. MG: consultant fees from Eli Lilly, and lecture fees from Eli Lilly, Merck Sharp & Dohme, and Novo Nordisk. VG: lecture fees from Abbot, Astra-Zeneca, Medtronic, Novo Nordisk, Sanofi-Aventis, Theras, and Vertex. EB: consultant fees from Abbott, Bayer, Becton Dickinson, Boehringer Ingelheim, Daiichi-Sankyo, Eli Lilly, and Novo Nordisk. CF: lecture fees from Abbot, Boehringer Ingelheim, Daiichi Sankyo, Eli Lilly, Merck Sharp & Dohme, Mundipharma, and Theras Lifetech. RT: consultant fees from AstraZeneca, Bayer, Boehringer Ingelheim, Eli Lilly, Merck Sharp & Dohme, Novo Nordisk, and Sanofi-Aventis, and lecture fees from AstraZeneca, Boehringer Ingelheim, Eli Lilly, and Novo Nordisk. MVe: lecture fees from Lifescan and Novo Nordisk. AN grant from Artsana, Astra-Zeneca, Eli Lilly, Novo Nordisk, and Sanofi Aventis and personal fees from Eli Lilly and Novo Nordisk. GPe: consultant fees from Bayer and Eli Lilly, and lecture fees from AstraZeneca, Boerhinger Ingelheim, Eli-Lilly, Merck Sharp & Dohme, Mundipharma, Novo Nordisk, and Takeda. GPu: consultant fees from Abbot, Bayer, and Novo Nordisk, and lecture fees from AstraZeneca, Boehringer Ingelheim, Eli Lilly, Mundipharma, and Novo Nordisk.
Ethics approval
The study was conducted in accordance with the Declaration of Helsinki. The research protocol was approved by the ethics committee of the coordinating center (Sant’Andrea University Hospital, Rome, Italy) on 25 September 2006 (number 43/2006) and subsequently by the ethics committee of each participating center.
Consent to participate
Participants provided an informed consent.
Consent for publication
Not applicable.
Additional information
Managed by Massimo Federici .
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
*See Supplementary file 1: The RIACE Study Group, for a complete list of the RIACE Investigators.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Vitale, M., Orsi, E., Solini, A. et al. Association between age at diagnosis and all-cause mortality in type 2 diabetes: the Renal Insufficiency and Cardiovascular Events (RIACE) Italian Multicenter Study. Acta Diabetol (2024). https://doi.org/10.1007/s00592-024-02294-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s00592-024-02294-1