
Adverse Outcome Following Mild Traumatic Brain Injury Is Associated with Microstructure Alterations at the Gray and White Matter Boundary
 , ,
, ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Diagnostic and Clinical Assessments
2.2.1. Assessment of mTBI
2.2.2. Assessment of Post-Concussion Symptom Severity
2.2.3. Assessment of Functional Impairment
2.2.4. Assessment of Cognitive Functioning
2.2.5. Assessment of Psychiatric Comorbidities
2.3. MRI Acquisition and Image Processing
2.3.1. Image Acquisition
2.3.2. Image Pre-Processing
2.3.3. Structural Image Processing
2.3.4. Diffusion-Weighted Image Processing
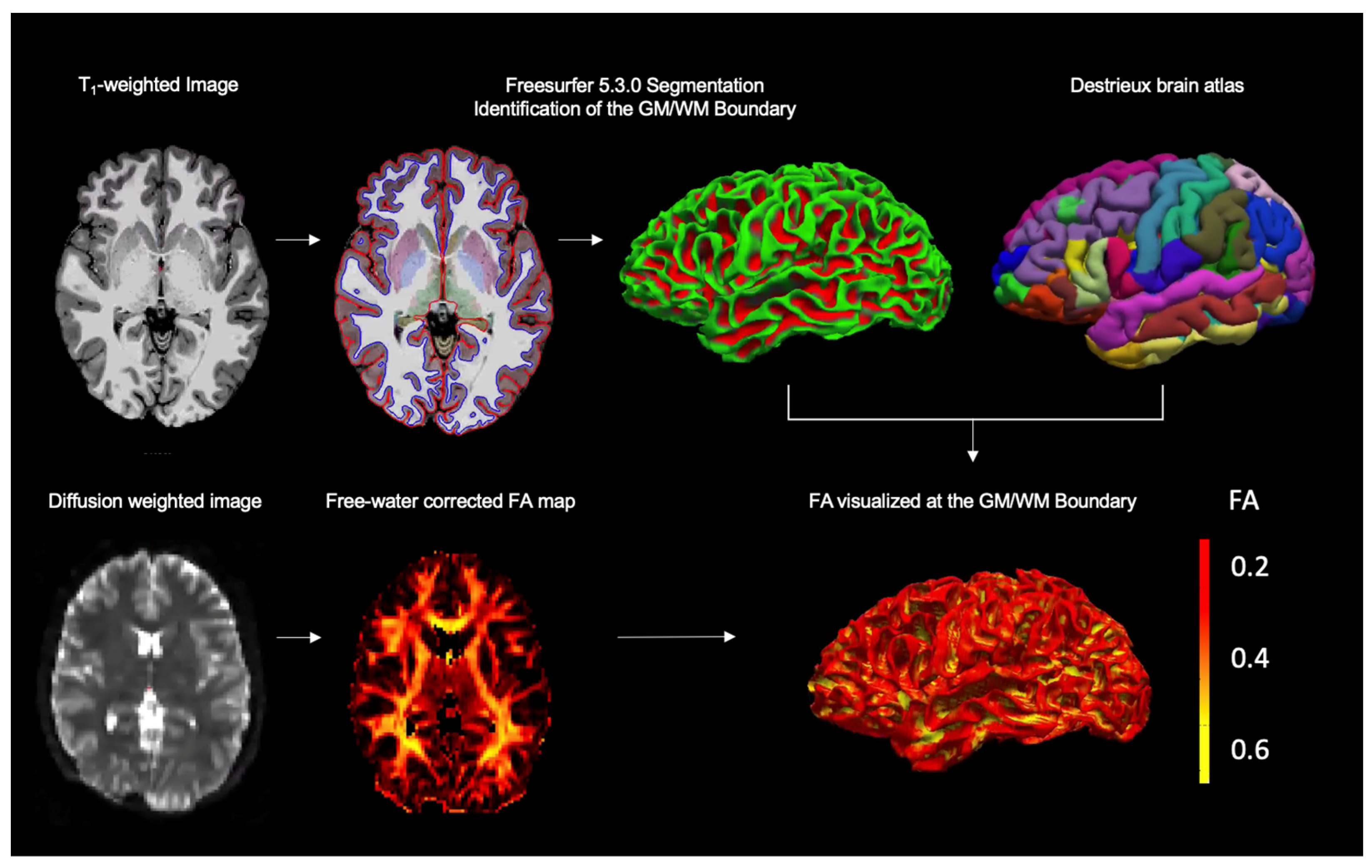
2.3.5. Registration and Extraction of Diffusion Metrics at the GM/WM Boundary
2.4. Statistical Analysis
2.4.1. Group Differences in GM/WM Boundary Diffusion, Deep WM Diffusion, and Cortical Thickness
2.4.2. Correlation between GM/WM Boundary Diffusion and Post-Concussive Symptoms, Functional Impairment, and Cognitive Functioning
3. Results
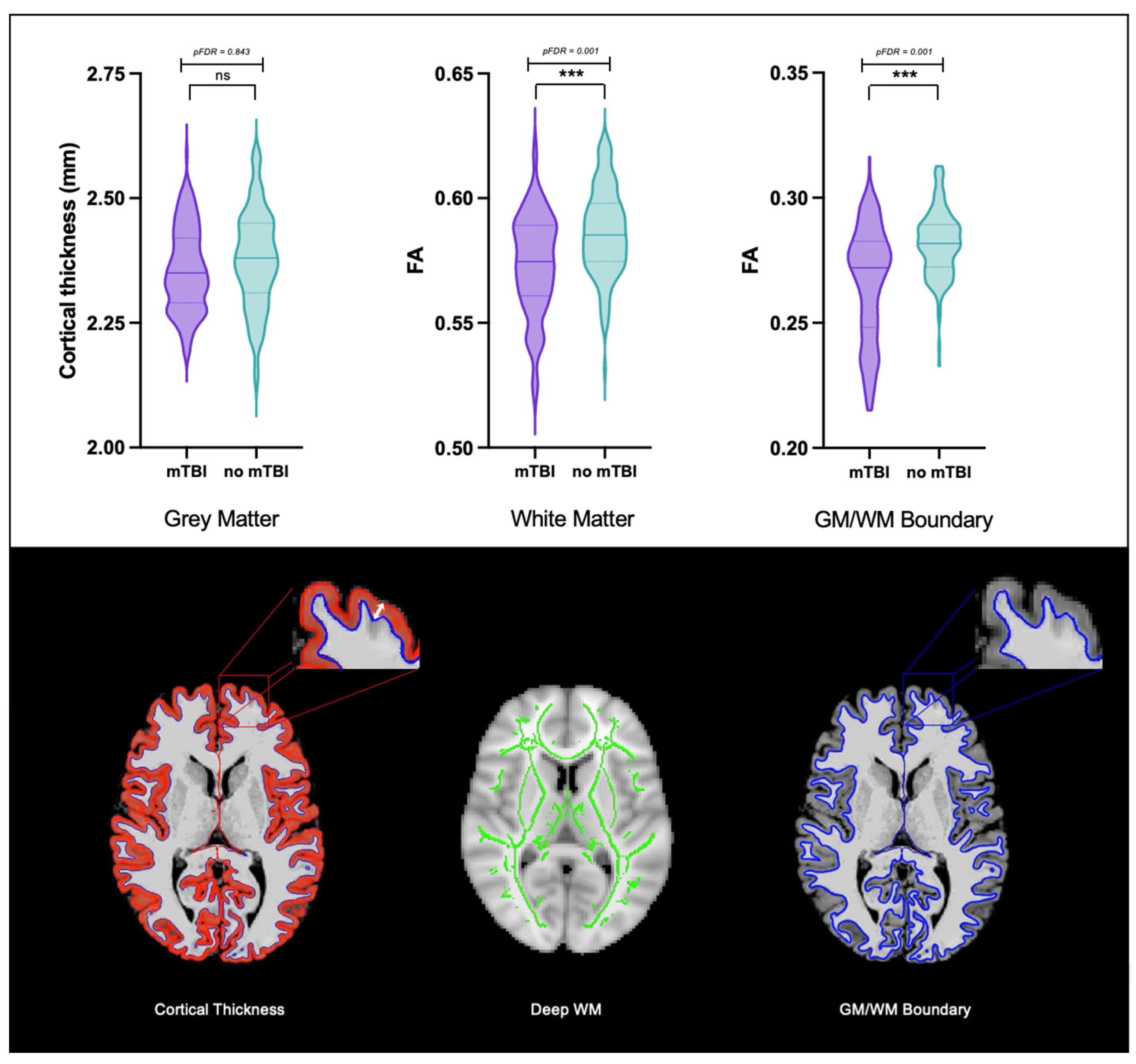
3.1. Group Differences in GM/WM Boundary Diffusion, Deep WM Diffusion, and Cortical Thickness
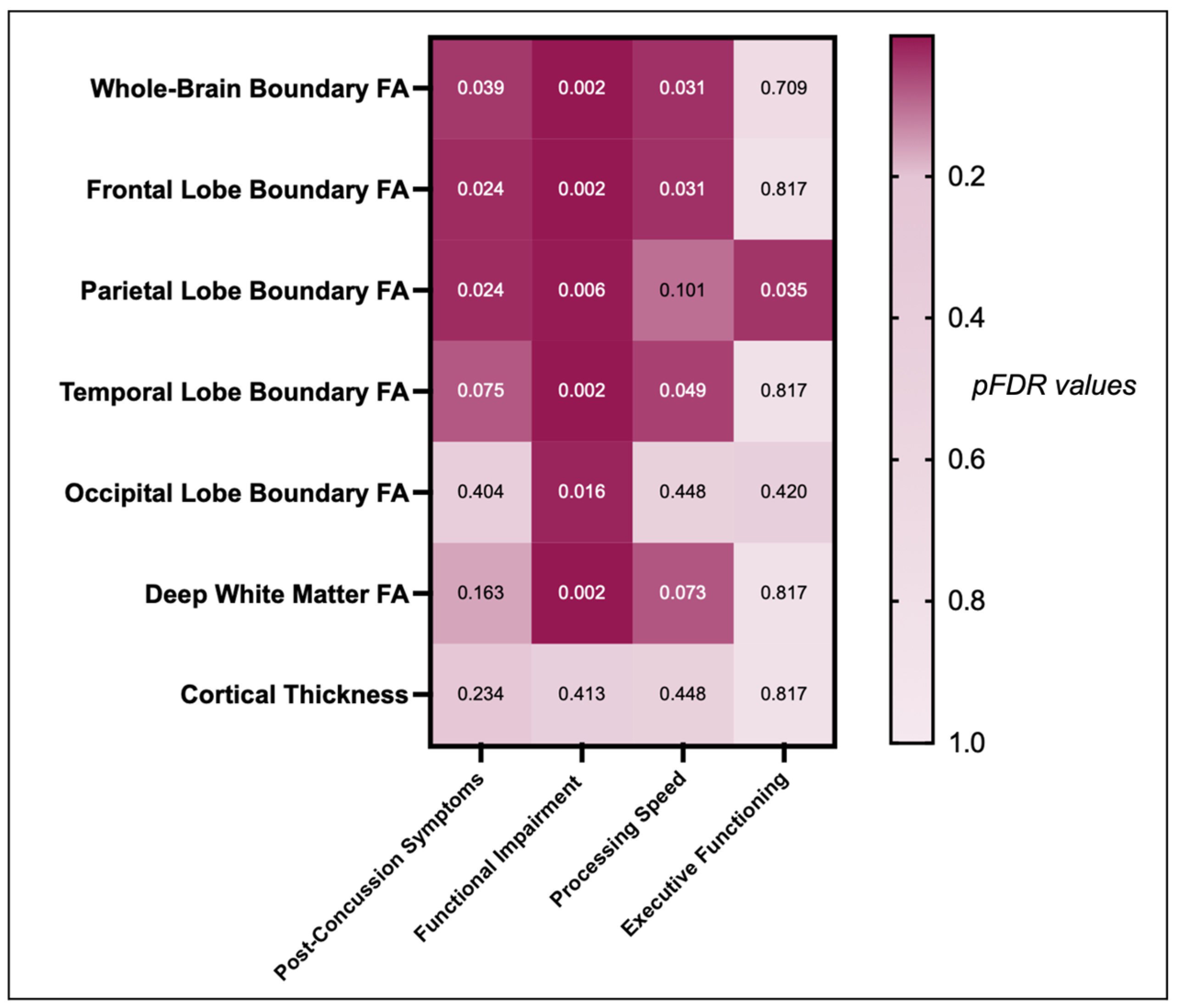
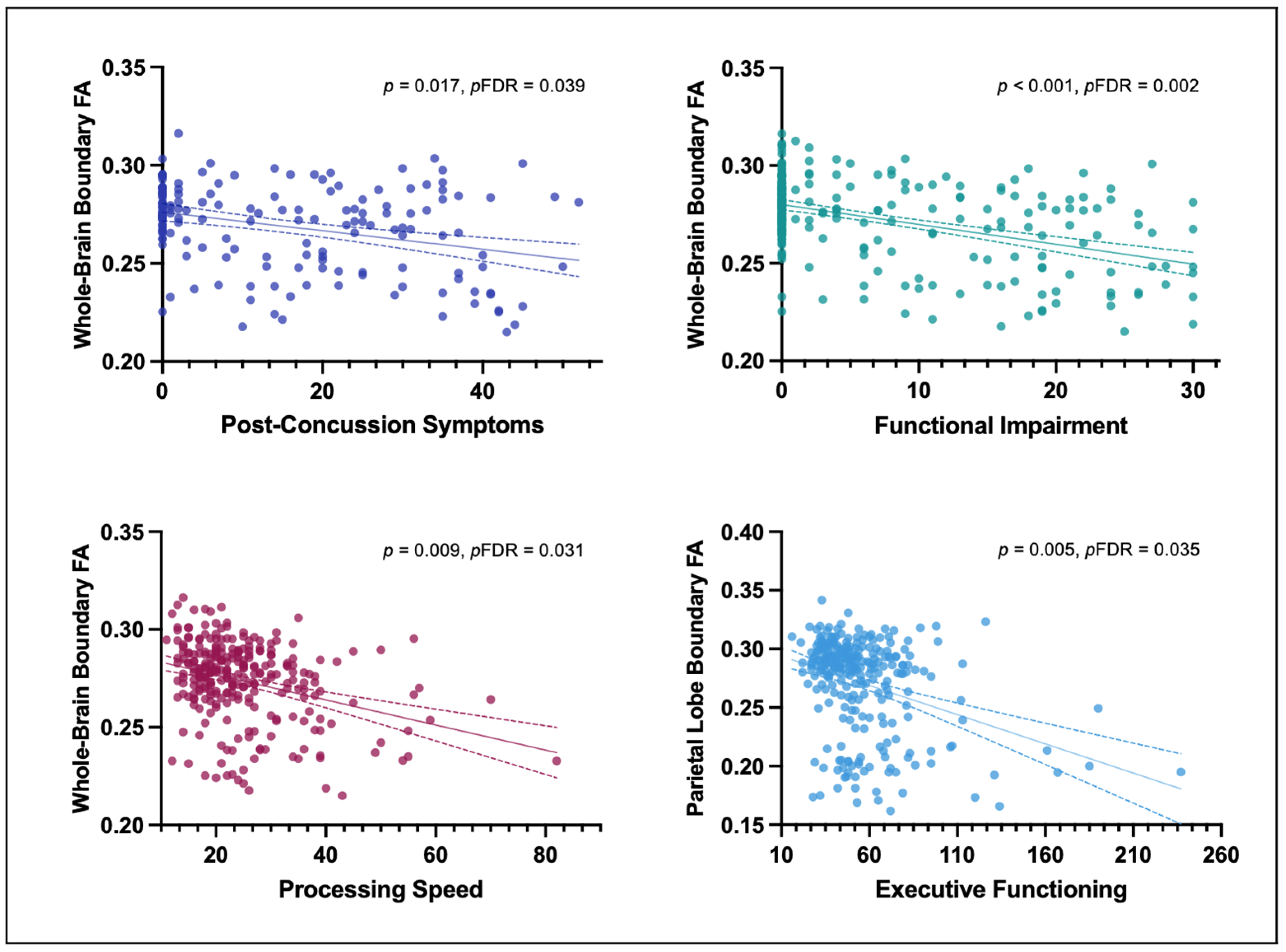
3.2. Correlation between GM/WM Boundary Diffusion and Post-Concussive Symptoms, Functional Impairment, and Cognitive Functioning
4. Discussion
4.1. WM and GM Alterations Following mTBI
4.2. Association between GM/WM Boundary Diffusion and Long-Term Outcome Following mTBI
4.3. Limitations and Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lindquist, L.K.; Love, H.C.; Elbogen, E.B. Traumatic Brain Injury in Iraq and Afghanistan Veterans: New Results from a National Random Sample Study. J. Neuropsychiatry Clin. Neurosci. 2017, 29, 254–259. [Google Scholar] [CrossRef]
- Schneiderman, A.I.; Braver, E.R.; Kang, H.K. Understanding Sequelae of Injury Mechanisms and Mild Traumatic Brain Injury Incurred during the Conflicts in Iraq and Afghanistan: Persistent Postconcussive Symptoms and Posttraumatic Stress Disorder. Am. J. Epidemiol. 2008, 167, 1446–1452. [Google Scholar] [CrossRef] [PubMed]
- Gardner, R.C.; Yaffe, K. Epidemiology of Mild Traumatic Brain Injury and Neurodegenerative Disease. Mol. Cell. Neurosci. 2015, 66, 75–80. [Google Scholar] [CrossRef] [PubMed]
- Maas, A.I.R.; Menon, D.K.; Manley, G.T.; Abrams, M.; Åkerlund, C.; Andelic, N.; Aries, M.; Bashford, T.; Bell, M.J.; Bodien, Y.G.; et al. Traumatic Brain Injury: Progress and Challenges in Prevention, Clinical Care, and Research. Lancet Neurol. 2022, 21, 1004–1060. [Google Scholar] [CrossRef]
- Cancelliere, C.; Verville, L.; Stubbs, J.L.; Yu, H.; Hincapié, C.A.A.; Cassidy, J.D.; Wong, J.J.; Shearer, H.; Connell, G.; Southerst, D.; et al. Post-Concussion Symptoms and Disability in Adults with Mild Traumatic Brain Injury: A Systematic Review and Meta-Analysis. J. Neurotrauma 2023, 40, 1045–1059. [Google Scholar] [CrossRef] [PubMed]
- Chen, Q.; Chen, X.; Xu, L.; Zhang, R.; Li, Z.; Yue, X.; Qiao, D. Traumatic Axonal Injury: Neuropathological Features, Postmortem Diagnostic Methods, and Strategies. Forensic Sci. Med. Pathol. 2022, 18, 530–544. [Google Scholar] [CrossRef]
- Johnson, V.E.; Stewart, W.; Smith, D.H. Axonal Pathology in Traumatic Brain Injury. Exp. Neurol. 2013, 246, 35–43. [Google Scholar] [CrossRef]
- Budday, S.; Nay, R.; de Rooij, R.; Steinmann, P.; Wyrobek, T.; Ovaert, T.C.; Kuhl, E. Mechanical Properties of Gray and White Matter Brain Tissue by Indentation. J. Mech. Behav. Biomed. Mater. 2015, 46, 318–330. [Google Scholar] [CrossRef]
- Alisafaei, F.; Gong, Z.; Johnson, V.E.; Dollé, J.P.; Smith, D.H.; Shenoy, V.B. Mechanisms of Local Stress Amplification in Axons near the Gray-White Matter Interface. Biophys. J. 2020, 119, 1290–1300. [Google Scholar] [CrossRef]
- Ghajari, M.; Hellyer, P.J.; Sharp, D.J. Computational Modelling of Traumatic Brain Injury Predicts the Location of Chronic Traumatic Encephalopathy Pathology. Brain 2017, 140, 333–343. [Google Scholar] [CrossRef]
- Liu, J.; Kou, Z.F.; Tian, Y.Q. Diffuse Axonal Injury after Traumatic Cerebral Microbleeds: An Evaluation of Imaging Techniques. Neural Regen. Res. 2014, 9, 1222. [Google Scholar] [CrossRef] [PubMed]
- Messé, A.; Caplain, S.; Pélégrini-Issac, M.; Blancho, S.; Montreuil, M.; Lévy, R.; Lehéricy, S.; Benali, H. Structural Integrity and Postconcussion Syndrome in Mild Traumatic Brain Injury Patients. Brain Imaging Behav. 2012, 6, 283–292. [Google Scholar] [CrossRef] [PubMed]
- Oehr, L.; Anderson, J. Diffusion-Tensor Imaging Findings and Cognitive Function Following Hospitalized Mixed-Mechanism Mild Traumatic Brain Injury: A Systematic Review and Meta-Analysis. Arch. Phys. Med. Rehabil. 2017, 98, 2308–2319. [Google Scholar] [CrossRef]
- Shenton, M.E.; Hamoda, H.M.; Schneiderman, J.S.; Bouix, S.; Pasternak, O.; Rathi, Y.; Vu, M.A.; Purohit, M.P.; Helmer, K.; Koerte, I.; et al. A Review of Magnetic Resonance Imaging and Diffusion Tensor Imaging Findings in Mild Traumatic Brain Injury. Brain Imaging Behav. 2012, 6, 137–192. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.; Yoo, R.E.; Seong, M.Y.; Oh, B.M. A Systematic Review and Data Synthesis of Longitudinal Changes in White Matter Integrity after Mild Traumatic Brain Injury Assessed by Diffusion Tensor Imaging in Adults. Eur. J. Radiol. 2022, 147, 110117. [Google Scholar] [CrossRef]
- Lippa, S.M.; Yeh, P.-H.; Ollinger, J.; Brickell, T.A.; French, L.M.; Lange, R.T. White Matter Integrity Relates to Cognition in Service Members and Veterans after Complicated Mild, Moderate, and Severe Traumatic Brain Injury, But Not Uncomplicated Mild Traumatic Brain Injury. J. Neurotrauma 2022. [Google Scholar] [CrossRef]
- Govindarajan, K.A.; Narayana, P.A.; Hasan, K.M.; Wilde, E.A.; Levin, H.S.; Hunter, J.V.; Miller, E.R.; Patel, V.K.S.; Robertson, C.S.; McCarthy, J.J. Cortical Thickness in Mild Traumatic Brain Injury. J. Neurotrauma 2016, 33, 1809–1817. [Google Scholar] [CrossRef]
- España, L.Y.; Lee, R.M.; Ling, J.M.; Jeromin, A.; Mayer, A.R.; Meier, T.B. Serial Assessment of Gray Matter Abnormalities after Sport-Related Concussion. J. Neurotrauma 2017, 34, 3143–3152. [Google Scholar] [CrossRef]
- Urban, K.J.; Riggs, L.; Wells, G.D.; Keightley, M.; Chen, J.K.; Ptito, A.; Fait, P.; Taha, T.; Sinopoli, K.J. Cortical Thickness Changes and Their Relationship to Dual-Task Performance Following Mild Traumatic Brain Injury in Youth. J. Neurotrauma 2017, 34, 816–823. [Google Scholar] [CrossRef]
- Dall’Acqua, P.; Johannes, S.; Mica, L.; Simmen, H.P.; Glaab, R.; Fandino, J.; Schwendinger, M.; Meier, C.; Ulbrich, E.J.; Müller, A.; et al. Prefrontal Cortical Thickening after Mild Traumatic Brain Injury: A One-Year Magnetic Resonance Imaging Study. J. Neurotrauma 2017, 34, 3270–3279. [Google Scholar] [CrossRef]
- Trotter, B.B.; Robinson, M.E.; Milberg, W.P.; McGlinchey, R.E.; Salat, D.H. Military Blast Exposure, Ageing and White Matter Integrity. Brain 2015, 138, 2278–2292. [Google Scholar] [CrossRef]
- Mac Donald, C.L.; Barber, J.; Andre, J.; Panks, C.; Zalewski, K.; Temkin, N. Longitudinal Neuroimaging Following Combat Concussion: Sub-Acute, 1 Year and 5 Years Post-Injury. Brain Commun. 2019, 1, fcz031. [Google Scholar] [CrossRef] [PubMed]
- Lange, R.T.; Yeh, P.H.; Brickell, T.A.; Lippa, S.M.; French, L.M. Postconcussion Symptom Reporting Is Not Associated with Diffusion Tensor Imaging Findings in the Subacute to Chronic Phase of Recovery in Military Service Members Following Mild Traumatic Brain Injury. J. Clin. Exp. Neuropsychol. 2019, 41, 497–511. [Google Scholar] [CrossRef] [PubMed]
- Zivanovic, N.; Virani, S.; Rajaram, A.A.; Lebel, C.; Yeates, K.O.; Brooks, B.L. Cortical Volume and Thickness in Youth Several Years After Concussion. J. Child. Neurol. 2021, 36, 186–194. [Google Scholar] [CrossRef]
- Mild Traumatic Brain Injury Committee, American Congress of Rehabilitation Medicine, Head Injury Interdisciplinary Special Interest Group. Definition of Mild Traumatic Brain Injury. J. Head. Trauma Rehabil. 1993, 8, 86–87. [Google Scholar] [CrossRef]
- Umminger, L.F.; Rojczyk, P.; Seitz-Holland, J.; Sollmann, N.; Kaufmann, E.; Kinzel, P.; Zhang, F.; Kochsiek, J.; Langhein, M.; Kim, C.L.; et al. White Matter Microstructure Is Associated with Serum Neuroactive Steroids and Psychological Functioning. J. Neurotrauma 2022. [Google Scholar] [CrossRef]
- King, N.S.; Crawford, S.; Wenden, F.J.; Moss, N.E.G.; Wade, D.T. The Rivermead Post Concussion Symptoms Questionnaire: A Measure of Symptoms Commonly Experienced after Head Injury and Its Reliability. J. Neurol. 1995, 242, 587–592. [Google Scholar] [CrossRef]
- Eyres, S.; Carey, A.; Gilworth, G.; Neumann, V.; Tennant, A. Construct Validity and Reliability of the Rivermead Post-Concussion Symptoms Questionnaire. Clin. Rehabil. 2005, 19, 878–887. [Google Scholar] [CrossRef] [PubMed]
- Sheehan, D.V.; Harnett-Sheehan, K.; Raj, B.A. The Measurement of Disability. Int. Clin. Psychopharmacol. 1996, 11 (Suppl. 3), 89–95. [Google Scholar] [CrossRef]
- Reitan, R.M. An Investigation of the Validity of Halstead’s Measures of Biological Intelligence. Arch. Neurol. Psychiatry 1955, 73, 28–35. [Google Scholar] [CrossRef]
- Stuss, D.T.; Stethem, L.L.; Hugenholtz, H.; Richard, M.T. Traumatic Brain Injury: A Comparison of Three Clinical Tests, and Analysis of Recovery. Clin. Neuropsychol. 1989, 3, 145–156. [Google Scholar] [CrossRef]
- Weathers, F.W.; Litz, B.T.; Herman, D.S.; Huska, J.A.; Keane, T.M. The PTSD Checklist (PCL): Reliability, Validity, and Diagnostic Utility. In Proceedings of the Annual Conference of the International Society for Traumatic Stress Studies, San Antonio, TX, USA, 24 October 1993. [Google Scholar]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.W. The PHQ-9: Validity of a Brief Depression Severity Measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef] [PubMed]
- Saunders, J.B.; Aasland, O.G.; Amundsen, A.; Grant, M. Alcohol Consumption and Related Problems among Primary Health Care Patients: WHO Collaborative Project on Early Detection of Persons with Harmful Alcohol Consumption—I. Addiction 1993, 88, 349–362. [Google Scholar] [CrossRef] [PubMed]
- Fedorov, A.; Beichel, R.; Kalpathy-Cramer, J.; Finet, J.; Fillion-Robin, J.C.; Pujol, S.; Bauer, C.; Jennings, D.; Fennessy, F.; Sonka, M.; et al. 3D Slicer as an Image Computing Platform for the Quantitative Imaging Network. Magn. Reson. Imaging 2012, 30, 1323–1341. [Google Scholar] [CrossRef] [PubMed]
- Fischl, B. FreeSurfer. Neuroimage 2012, 62, 774–781. [Google Scholar] [CrossRef]
- Destrieux, C.; Fischl, B.; Dale, A.; Halgren, E. Automatic Parcellation of Human Cortical Gyri and Sulci Using Standard Anatomical Nomenclature. Neuroimage 2010, 53, 1–15. [Google Scholar] [CrossRef]
- Fischl, B.; Dale, A.M. Measuring the Thickness of the Human Cerebral Cortex from Magnetic Resonance Images. Proc. Natl. Acad. Sci. USA 2000, 97, 11050–11055. [Google Scholar] [CrossRef]
- Mirzaalian, H.; Ning, L.; Savadjiev, P.; Pasternak, O.; Bouix, S.; Michailovich, O.; Grant, G.; Marx, C.E.; Morey, R.A.; Flashman, L.A.; et al. Inter-Site and Inter-Scanner Diffusion MRI Data Harmonization. Neuroimage 2016, 135, 311–323. [Google Scholar] [CrossRef]
- Chien, D.; Buxton, R.B.; Kwong, K.K.; Brady, T.J.; Rosen, B.R. MR Diffusion Imaging of the Human Brain. J. Comput. Assist. Tomogr. 1990, 14, 514–520. [Google Scholar] [CrossRef]
- Pasternak, O.; Sochen, N.; Gur, Y.; Intrator, N.; Assaf, Y. Free Water Elimination and Mapping from Diffusion MRI. Magn. Reson. Med. 2009, 62, 717–730. [Google Scholar] [CrossRef]
- Smith, S.M.; Jenkinson, M.; Johansen-Berg, H.; Rueckert, D.; Nichols, T.E.; Mackay, C.E.; Watkins, K.E.; Ciccarelli, O.; Cader, M.Z.; Matthews, P.M.; et al. Tract-Based Spatial Statistics: Voxelwise Analysis of Multi-Subject Diffusion Data. Neuroimage 2006, 31, 1487–1505. [Google Scholar] [CrossRef] [PubMed]
- Jahanshad, N.; Kochunov, P.v.; Sprooten, E.; Mandl, R.C.; Nichols, T.E.; Almasy, L.; Blangero, J.; Brouwer, R.M.; Curran, J.E.; de Zubicaray, G.I.; et al. Multi-Site Genetic Analysis of Diffusion Images and Voxelwise Heritability Analysis: A Pilot Project of the ENIGMA-DTI Working Group. Neuroimage 2013, 81, 455–469. [Google Scholar] [CrossRef] [PubMed]
- Greve, D.N.; Fischl, B. Accurate and Robust Brain Image Alignment Using Boundary-Based Registration. Neuroimage 2009, 48, 63–72. [Google Scholar] [CrossRef] [PubMed]
- Hochberg, Y.; Benjamini, Y. More Powerful Procedures for Multiple Significance Testing. Stat. Med. 1990, 9, 811–818. [Google Scholar] [CrossRef]
- Donat, C.K.; Yanez Lopez, M.; Sastre, M.; Baxan, N.; Goldfinger, M.; Seeamber, R.; Müller, F.; Davies, P.; Hellyer, P.; Siegkas, P.; et al. From Biomechanics to Pathology: Predicting Axonal Injury from Patterns of Strain after Traumatic Brain Injury. Brain 2021, 144, 70–91. [Google Scholar] [CrossRef]
- Simon, D.W.; McGeachy, M.J.; Baylr, H.; Clark, R.S.B.; Loane, D.J.; Kochanek, P.M. The Far-Reaching Scope of Neuroinflammation after Traumatic Brain Injury. Nat. Rev. Neurol. 2017, 13, 171–191. [Google Scholar] [CrossRef]
- Cramer, S.W.; Haley, S.P.; Popa, L.S.; Carter, R.E.; Scott, E.; Flaherty, E.B.; Dominguez, J.; Aronson, J.D.; Sabal, L.; Surinach, D.; et al. Wide-Field Calcium Imaging Reveals Widespread Changes in Cortical Functional Connectivity Following Mild Traumatic Brain Injury in the Mouse. Neurobiol. Dis. 2023, 176, 105943. [Google Scholar] [CrossRef]
- Hocke, L.M.; Duszynski, C.C.; Debert, C.T.; Dleikan, D.; Dunn, J.F. Reduced Functional Connectivity in Adults with Persistent Post-Concussion Symptoms: A Functional Near-Infrared Spectroscopy Study. J. Neurotrauma 2018, 35, 1224–1232. [Google Scholar] [CrossRef]
- D’Souza, M.M.; Kumar, M.; Choudhary, A.; Kaur, P.; Kumar, P.; Rana, P.; Trivedi, R.; Sekhri, T.; Singh, A.K. Alterations of Connectivity Patterns in Functional Brain Networks in Patients with Mild Traumatic Brain Injury: A Longitudinal Resting-State Functional Magnetic Resonance Imaging Study. Neuroradiol. J. 2020, 33, 186–197. [Google Scholar] [CrossRef]
- Mohammadian, M.; Roine, T.; Hirvonen, J.; Kurki, T.; Posti, J.P.; Katila, A.J.; Takala, R.S.K.; Tallus, J.; Maanpää, H.R.; Frantzén, J.; et al. Alterations in Microstructure and Local Fiber Orientation of White Matter Are Associated with Outcome after Mild Traumatic Brain Injury. J. Neurotrauma 2020, 37, 2616–2623. [Google Scholar] [CrossRef]
- Gaines, K.D.; Soper, H.v.; Berenji, G.R. Executive Functioning of Combat Mild Traumatic Brain Injury. Appl. Neuropsychol. Adult 2016, 23, 115–124. [Google Scholar] [CrossRef]
- Bullmore, E.; Sporns, O. The Economy of Brain Network Organization. Nat. Rev. Neurosci. 2012, 13, 336–349. [Google Scholar] [CrossRef] [PubMed]
- Cristofori, I.; Cohen-Zimerman, S.; Grafman, J. Executive Functions. Handb. Clin. Neurol. 2019, 163, 197–219. [Google Scholar] [CrossRef] [PubMed]
- Menon, V. Large-Scale Brain Networks and Psychopathology: A Unifying Triple Network Model. Trends Cogn. Sci. 2011, 15, 483–506. [Google Scholar] [CrossRef]
- Cristofori, I.; Zhong, W.; Chau, A.; Solomon, J.; Krueger, F.; Grafman, J. White and Gray Matter Contributions to Executive Function Recovery after Traumatic Brain Injury. Neurology 2015, 84, 1394. [Google Scholar] [CrossRef] [PubMed]
- Przekwas, A.; Garimella, H.T.; Tan, X.G.; Chen, Z.J.; Miao, Y.; Harrand, V.; Kraft, R.H.; Gupta, R.K. Biomechanics of Blast TBI With Time-Resolved Consecutive Primary, Secondary, and Tertiary Loads. Mil. Med. 2019, 184, 195–205. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total Sample | mTBI | No mTBI | |||||||
|---|---|---|---|---|---|---|---|---|---|
| ANCOVA | |||||||||
| Demographics | n | mean ± SD | n | mean ± SD | n | mean ± SD | F(df) | p | |
| Age | 278 | 36.27 ± 12.71 | 147 | 36.56 ± 11.97 | 131 | 34.62 ± 12.88 | 1.70(1, 276) | 0.193 | |
| Years between injury and scan | - | - | 101 | 7.57 ± 9.54 | - | - | - | - | |
| Fisher’s exact test | |||||||||
| % | % | % | χ2 | p | |||||
| Gender (male/female) | 54.3/45.7 | 65.3/34.7 | 41.9/58.1 | 15.31 | <0.001 | ||||
| Race | Native | 0.7 | 1.4 | - | 13.74 | 0.193 | |||
| Asian | 3.2 | 1.4 | 5.3 | ||||||
| Pacific | 0.4 | - | 0.8 | ||||||
| African American | 13.7 | 10.2 | 17.6 | ||||||
| White | 76.3 | 82.9 | 68.7 | ||||||
| Unknown | 5.7 | 4.1 | 7.6 | ||||||
| ANCOVA | |||||||||
| Imaging | n | mean ± SD | n | mean ± SD | n | mean ± SD | F(df) | p (pFDR) | |
| Whole-brain GM/WM Boundary FA | 278 | 0.27 ± 0.02 | 147 | 0.27 ± 0.02 | 131 | 0.28 ± 0.01 | 23.16(1, 271) | <0.001 (0.001) | |
| Frontal lobe GM/WM Boundary FA | 278 | 0.28 ± 0.02 | 147 | 0.28 ± 0.02 | 131 | 0.29 ± 0.02 | 18.62(1, 271) | <0.001 (0.001) | |
| Parietal lobe GM/WM Boundary FA | 278 | 0.27 ± 0.04 | 147 | 0.26 ± 0.05 | 131 | 0.28 ± 0.03 | 8.88(1, 271) | 0.003 (0.004) | |
| Temporal lobe GM/WM Boundary FA | 278 | 0.28 ± 0.02 | 147 | 0.27 ± 0.02 | 131 | 0.28 ± 0.01 | 27.78(1, 271) | <0.001 (0.001) | |
| Occipital lobe GM/WM Boundary FA | 278 | 0.25 ± 0.02 | 147 | 0.25 ± 0.02 | 131 | 0.26 ± 0.02 | 6.65(1, 271) | 0.010 (0.011) | |
| Deep white matter FA | 278 | 0.58 ± 0.02 | 147 | 0.57 ± 0.02 | 131 | 0.59 ± 0.02 | 25.21(1, 271) | <0.001 (0.001) | |
| Whole-brain cortical thickness | 278 | 2.37 ± 0.09 | 147 | 2.35 ± 0.08 | 131 | 2.37 ± 0.10 | 0.039(1, 271) | 0.843 (0.843) | |
| Psychiatric Symptoms | F(df) | p | |||||||
| PCL-C | 278 | 30.40 ± 17.58 | 147 | 36.66 ± 18.50 | 131 | 23.30 ± 13.38 | 35.35(1, 274) | <0.001 | |
| PHQ-9 | 278 | 4.40 ± 5.67 | 147 | 6.61 ± 5.99 | 131 | 1.92 ± 4.06 | 47.72(1, 274) | <0.001 | |
| Alcohol Use | |||||||||
| AUDIT-10 | 278 | 3.73 ± 5.50 | 147 | 4.67 ± 6.40 | 131 | 2.67 ± 4.03 | 6.63(1, 274) | 0.011 | |
| Post-Concussive Symptoms | |||||||||
| RPQ13 | 168 | 13.25 ± 15.04 | 139 | 17.35 ± 14.79 | 29 | 3.76 ± 11.23 | 21.83(1, 166) | <0.001 | |
| Functional Impairment | |||||||||
| SDS | 275 | 6.36 ± 9.07 | 147 | 10.44 ± 9.70 | 128 | 1.67 ± 5.28 | 74.47(1, 271) | <0.001 | |
| Cognitive Functioning | F(df) | p | |||||||
| TMT-A time (seconds) | 275 | 24.92 ± 10.21 | 145 | 26.58 ± 10.78 | 130 | 23.06 ± 9.24 | 6.10(1,271) | 0.014 | |
| TMT-B time (seconds) | 275 | 55.65 ± 27.52 | 145 | 58.19 ± 27.52 | 130 | 52.84 ± 26.83 | 0.89(1,271) | 0.348 | |
| Sequence | Parameter | SIEMENS | PHILIPS | GE |
|---|---|---|---|---|
| DTI | ||||
| Orientation | axial | axial | axial | |
| Phase Encoding Direction | a/p | p/a | l/r | |
| FOV (in mm) | 256 | 256 | 256 | |
| Bandwidth (in kHz or Hz/Px) | 1396 | 1271 | 250 | |
| Number of Directions | 87 | 64 | 86 | |
| b-value | 900 | 900 | 900 | |
| Number of b0 | 0 | 7 | 1 | |
| Resolution Matrix | 128 × 128 | 128 × 128 | 128 × 128 | |
| Voxel Size (in mm3) | 2 × 2 × 2 | 2 × 2 × 2 | 2 × 2 × 2 | |
| Number of Slices | 73 | 73 | 73 | |
| Acquisition Time (in min) | 14:08 | 14:21 | 14:40 | |
| T1w | ||||
| Sequence details | MP-RAGE | T1W_3D_TFE SENSE | SPGR-BRAVO | |
| Orientation | Sagittal | Sagittal | Sagittal | |
| Flip Angle (in degrees) | 7 | 7 | 10 | |
| FOV (in mm) | 256 | 256 | 256 | |
| Bandwidth (in kHz) | 25.6 | 24.5 | 25.0 | |
| TE (in ms) | 3.3 | 3.5 | 3.7 | |
| TR (in ms) | 2530 | 7600 | 9150 | |
| Inversion Time | 1100 | 1100 | 600 | |
| Resolution Matrix | 256 × 256 | 256 × 256 | 256 × 256 | |
| Voxel Size (in mm3) | 1 × 1 × 1 | 1 × 1 × 1 | 1 × 1 × 1 | |
| Number of Slices | 176 | 176 | 176 | |
| Acquisition Time (in min) | 6:03 | 5:13 | 5:15 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pankatz, L.; Rojczyk, P.; Seitz-Holland, J.; Bouix, S.; Jung, L.B.; Wiegand, T.L.T.; Bonke, E.M.; Sollmann, N.; Kaufmann, E.; Carrington, H.; et al. Adverse Outcome Following Mild Traumatic Brain Injury Is Associated with Microstructure Alterations at the Gray and White Matter Boundary. J. Clin. Med. 2023, 12, 5415. https://doi.org/10.3390/jcm12165415
Pankatz L, Rojczyk P, Seitz-Holland J, Bouix S, Jung LB, Wiegand TLT, Bonke EM, Sollmann N, Kaufmann E, Carrington H, et al. Adverse Outcome Following Mild Traumatic Brain Injury Is Associated with Microstructure Alterations at the Gray and White Matter Boundary. Journal of Clinical Medicine. 2023; 12(16):5415. https://doi.org/10.3390/jcm12165415
Chicago/Turabian StylePankatz, Lara, Philine Rojczyk, Johanna Seitz-Holland, Sylvain Bouix, Leonard B. Jung, Tim L. T. Wiegand, Elena M. Bonke, Nico Sollmann, Elisabeth Kaufmann, Holly Carrington, and et al. 2023. "Adverse Outcome Following Mild Traumatic Brain Injury Is Associated with Microstructure Alterations at the Gray and White Matter Boundary" Journal of Clinical Medicine 12, no. 16: 5415. https://doi.org/10.3390/jcm12165415