
Serum TARC Levels in Patients with Systemic Sclerosis: Clinical Association with Interstitial Lung Disease

 , , and
, , and
Abstract
:1. Introduction
2. Experimental Section
2.1. Patients
2.2. Clinical Assessment
2.3. Measurement of Serum TARC and IL-13 Levels
2.4. Statistical Analysis
3. Results
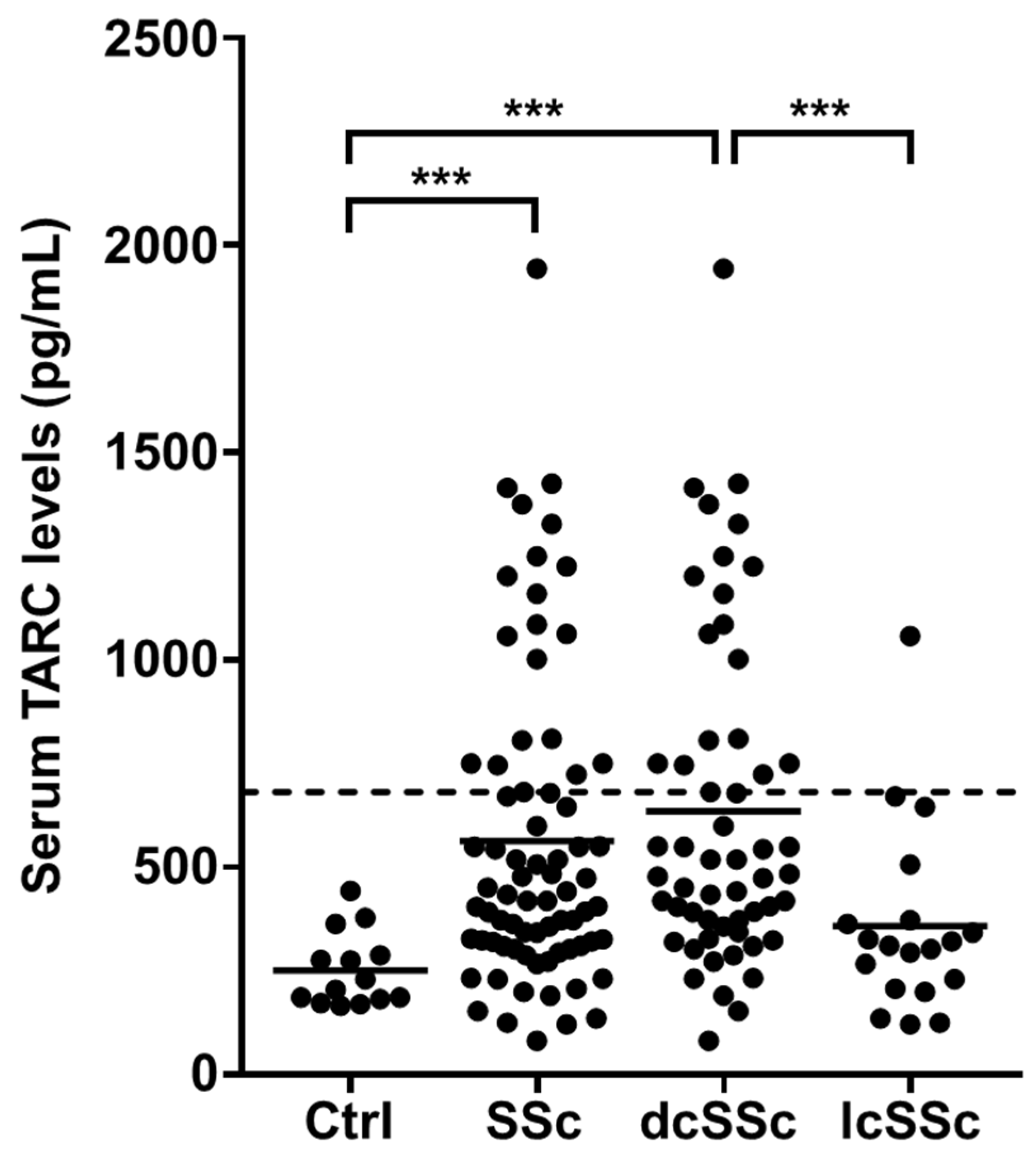
3.1. Serum TARC Levels in Patients with SSc
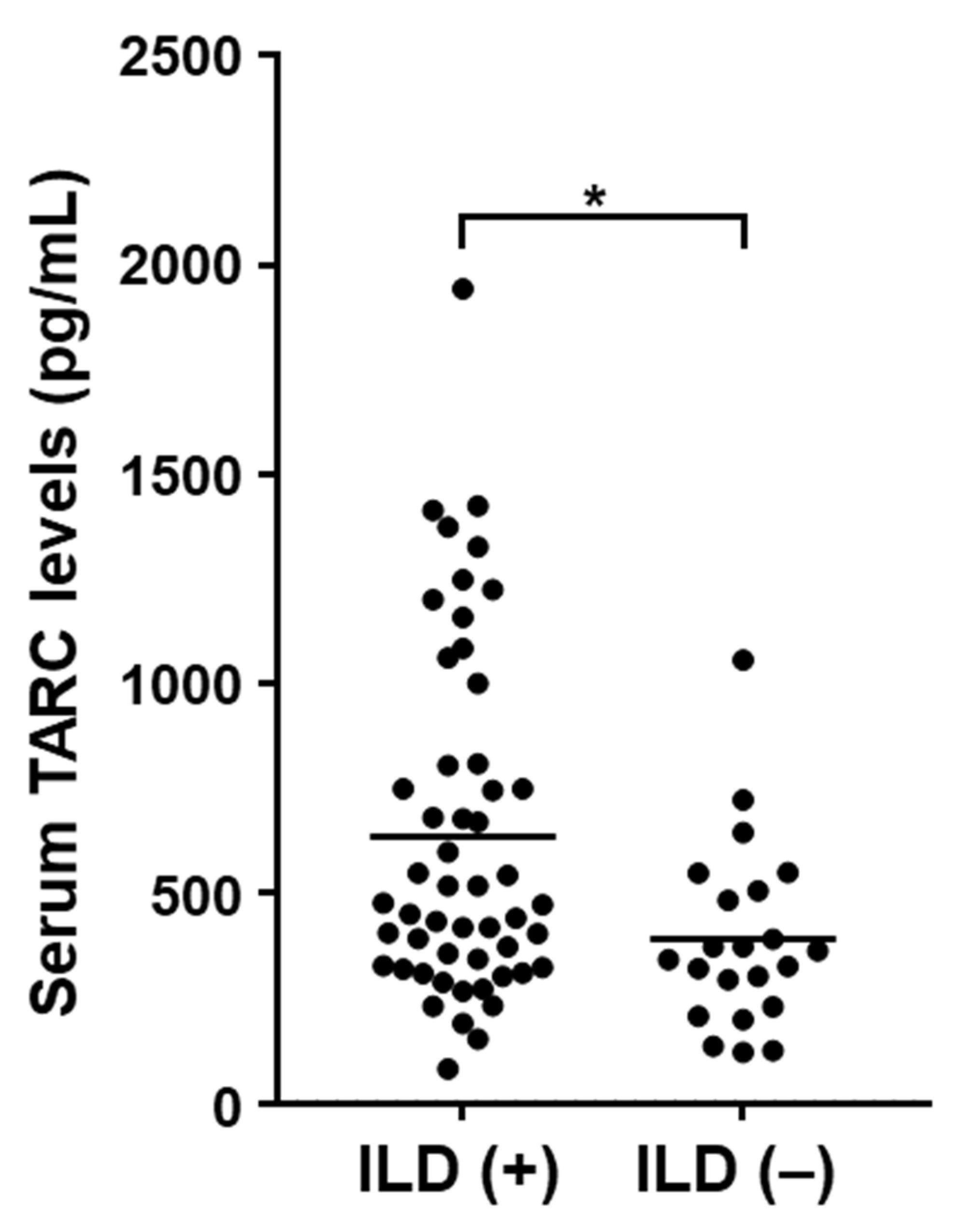
3.2. Clinical Association of Serum TARC Levels in SSc Patients
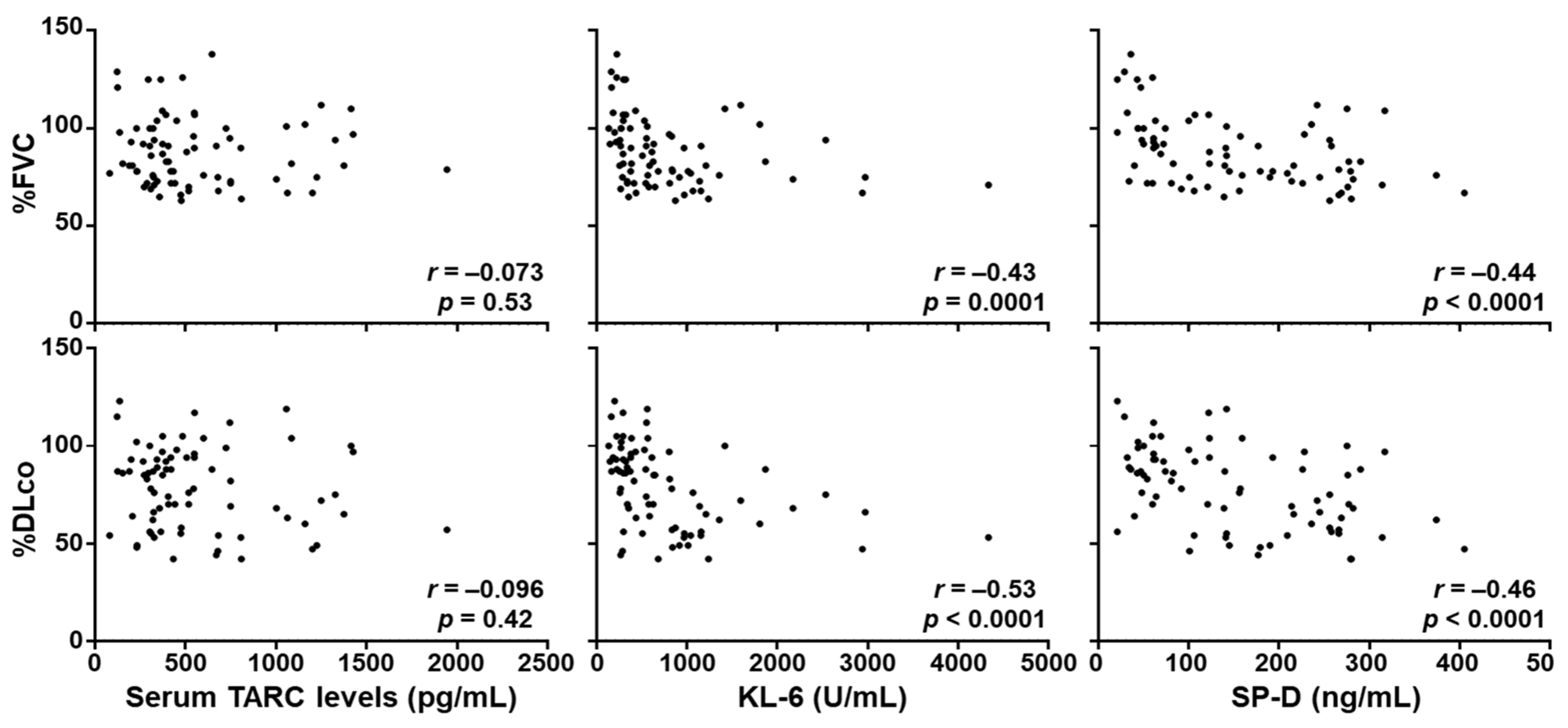
3.3. Correlation between Serum TARC Levels and the Severity of SSc-ILD
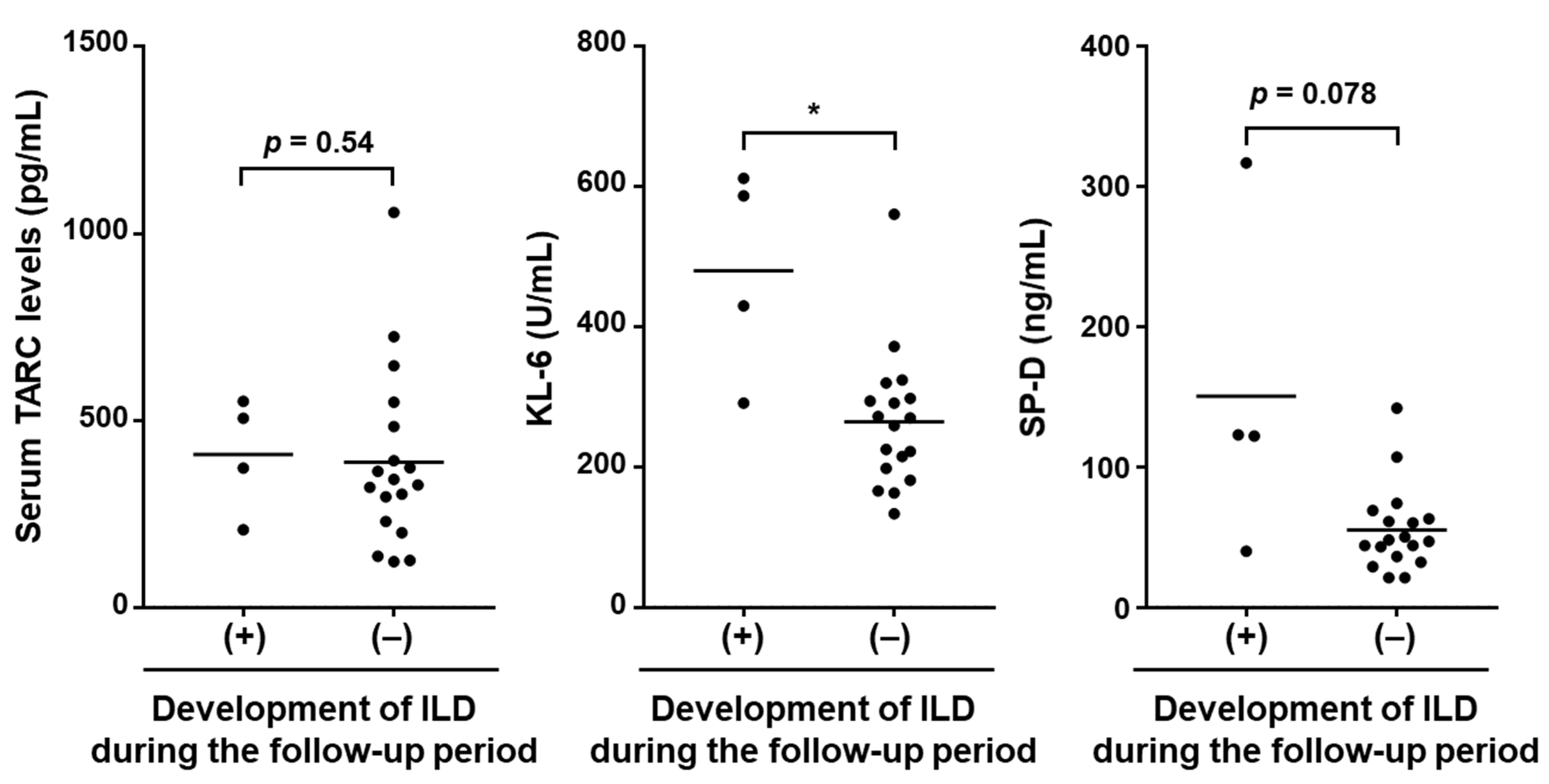
3.4. Correlation between Serum TARC Levels at the First Visit and the Development of SSc-ILD during the Follow-up Period
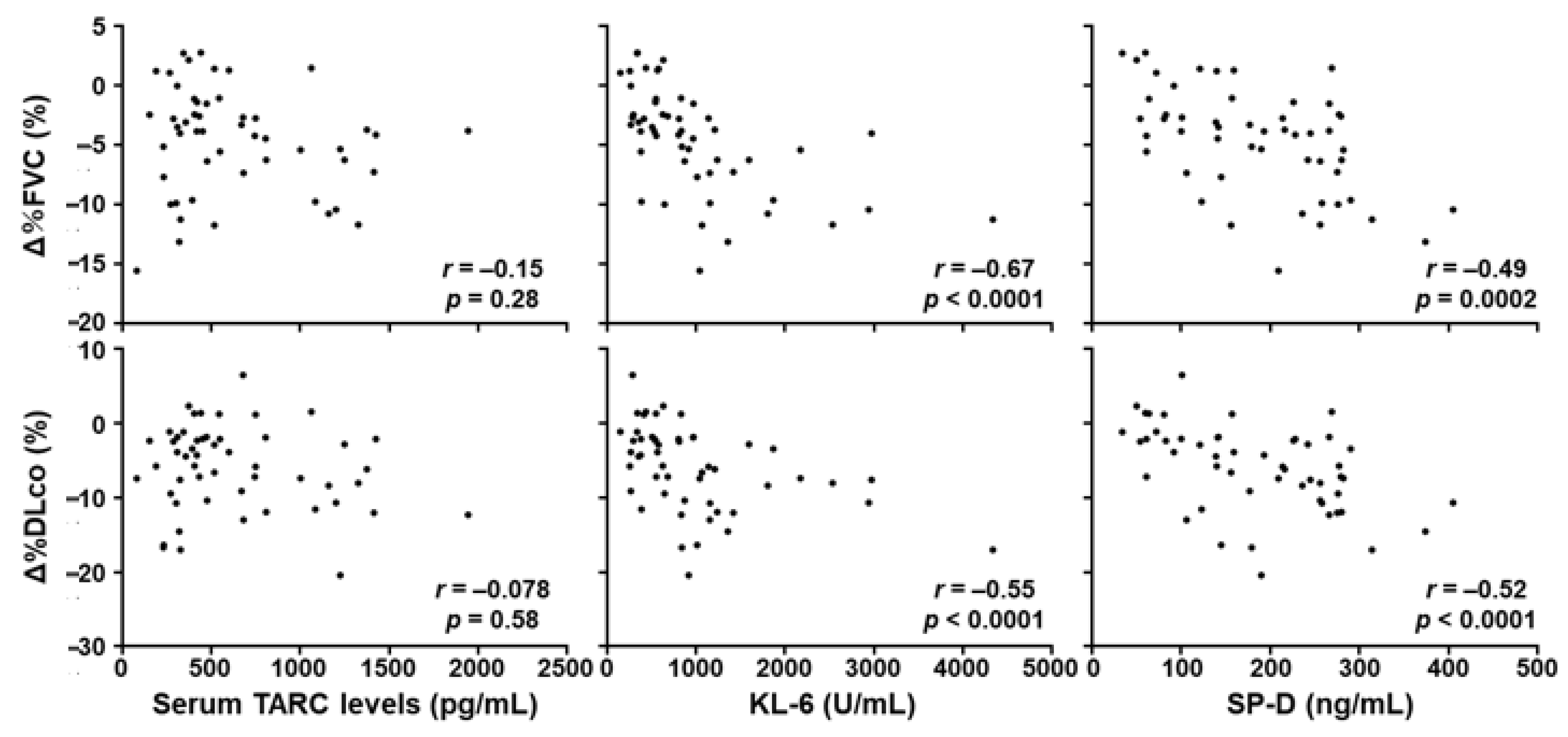
3.5. Correlation of Serum TARC Levels at the First Visit and the Progression of SSc-ILD during the Follow-up Period
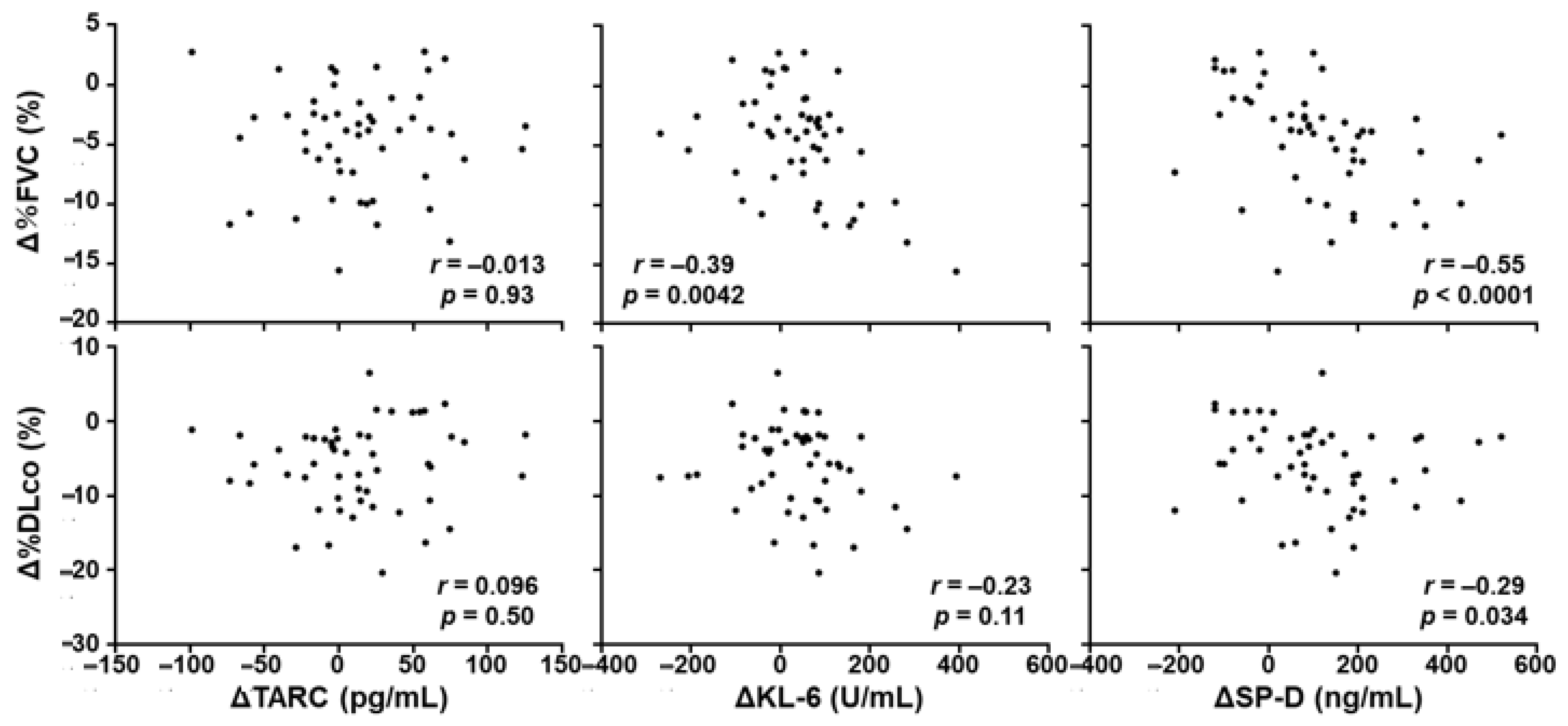
3.6. Correlation between the Change of Serum TARC Levels and the Progression of SSc-ILD during the Follow-up Period
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Gabrielli, A.; Avvedimento, E.V.; Krieg, T. Scleroderma. N. Engl. J. Med. 2009, 360, 1989–2003. [Google Scholar] [CrossRef] [PubMed]
- Yoshizaki, A. Pathogenic roles of B lymphocytes in systemic sclerosis. Immunol. Lett. 2018, 195, 76–82. [Google Scholar] [CrossRef] [PubMed]
- Yoshizaki, A.; Yanaba, K.; Iwata, Y.; Komura, K.; Ogawa, A.; Muroi, E.; Ogawa, F.; Takenaka, M.; Shimizu, K.; Hasegawa, M.; et al. Elevated serum interleukin-27 levels in patients with systemic sclerosis: Association with T cell, B cell and fibroblast activation. Ann. Rheum. Dis. 2011, 70, 194–200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuzumi, A.; Yoshizaki, A.; Toyama, S.; Fukasawa, T.; Ebata, S.; Nakamura, K.; Yamashita, T.; Saigusa, R.; Miura, S.; Hirabayashi, M.; et al. Serum interleukin-34 levels in patients with systemic sclerosis: Clinical association with interstitial lung disease. J. Dermatol. 2018, 45, 1216–1220. [Google Scholar] [CrossRef]
- Kalogerou, A.; Gelou, E.; Mountantonakis, S.; Settas, L.; Zafiriou, E.; Sakkas, L. Early T cell activation in the skin from patients with systemic sclerosis. Ann. Rheum. Dis. 2005, 64, 233–1235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoshizaki, A.; Yanaba, K.; Iwata, Y.; Komura, K.; Ogawa, A.; Akiyama, Y.; Muroi, E.; Hara, T.; Ogawa, F.; Takenaka, M.; et al. Cell Adhesion Molecules Regulate Fibrotic Process via Th1/Th2/Th17 Cell Balance in a Bleomycin-Induced Scleroderma Model. J. Immunol. 2010, 185, 2502–2515. [Google Scholar] [CrossRef] [Green Version]
- Salmon-Ehr, V.; Serpier, H.; Nawrocki, B.; Gillery, P.; Clavel, C.; Kalis, B.; Birembaut, P.; Maquart, F.X. Expression of interleukin-4 in scleroderma skin specimens and scleroderma fibroblast cultures. Potential role in fibrosis. Arch. Dermatol. 1996, 132, 802–806. [Google Scholar] [CrossRef]
- Fuschiotti, P.; Medsger, T.A.; Morel, P.A. Effector CD8+ T cells in systemic sclerosis patients produce abnormally high levels of interleukin-13 associated with increased skin fibrosis. Arthritis Rheum. 2009, 60, 1119–1128. [Google Scholar] [CrossRef]
- Hügle, T.; O’Reilly, S.; Simpson, R.; Kraaij, M.D.; Bigley, V.; Collin, M.; Krippner-Heidenreich, A.; van Laar, J.M. Tumor necrosis factor-costimulated T lymphocytes from patients with systemic sclerosis trigger collagen production in fibroblasts. Arthritis Rheum. 2013, 65, 481–491. [Google Scholar] [CrossRef]
- O’Reilly, S.; Hügle, T.; van Laar, J.M. T cells in systemic sclerosis: A reappraisal. Rheumatology 2012, 51, 1540–1549. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rincón, M.; Anguita, J.; Nakamura, T.; Fikrig, E.; Flavell, R.A. Interleukin (IL)-6 directs the differentiation of IL-4-producing CD4+ T Cells. J. Exp. Med. 1997, 185, 461–470. [Google Scholar] [CrossRef] [Green Version]
- Khan, K.; Xu, S.; Nihtyanova, S.; Derrett-Smith, E.; Abraham, D.; Denton, C.P.; Ong, V.H. Clinical and pathological significance of interleukin 6 overexpression in systemic sclerosis. Ann. Rheum. Dis. 2012, 71, 1235–1242. [Google Scholar] [CrossRef]
- Greenblatt, M.B.; Sargent, J.L.; Farina, G.; Tsang, K.; Lafyatis, R.; Glimcher, L.; Whitfield, M.L.; Aliprantis, A.O. Interspecies Comparison of Human and Murine Scleroderma Reveals IL-13 and CCL2 as Disease Subset-Specific Targets. Am. J. Pathol. 2012, 180, 1080–1094. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, M.; Baron, M.; Pedroza, C.; Salazar, G.A.; Ying, J.; Charles, J.; Agarwal, S.K.; Hudson, M.; Pope, J.; Zhou, X.; et al. CCL2 in the Circulation Predicts Long-Term Progression of Interstitial Lung Disease in Patients With Early Systemic Sclerosis: Data From Two Independent Cohorts. Arthritis Rheum. 2017, 69, 1871–1878. [Google Scholar] [CrossRef] [Green Version]
- Mor, A.; Salto, M.S.; Katav, A.; Barashi, N.; Edelshtein, V.; Manetti, M.; Levi, Y.; George, J.; Matucci-Cerinic, M. Blockade of CCL24 with a monoclonal antibody ameliorates experimental dermal and pulmonary fibrosis. Ann. Rheum. Dis. 2019, 78, 1260–1268. [Google Scholar] [CrossRef] [PubMed]
- Imai, T.; Yoshida, T.; Baba, M.; Nishimura, M.; Kakizaki, M.; Yoshie, O. Molecular cloning of a novel T cell-directed CC chemokine expressed in thymus by signal sequence trap using Epstein-Barr virus vector. J. Biol. Chem. 1996, 271, 21514–21521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Imai, T.; Baba, M.; Nishimura, M.; Kakizaki, M.; Takagi, S.; Yoshie, O. The T cell-directed CC chemokine TARC is a highly specific biological ligand for CC chemokine receptor 4. J. Biol. Chem. 1997, 272, 15036–15042. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saeki, H.; Tamaki, K. Thymus and activation regulated chemokine (TARC)/CCL17 and skin diseases. J. Dermatol. Sci. 2006, 43, 75–84. [Google Scholar] [CrossRef]
- Kakinuma, T.; Wakugawa, M.; Nakamura, K.; Hino, H.; Matsushima, K.; Tamaki, K. High level of thymus and activation-regulated chemokine in blister fluid and sera of patients with bullous pemphigoid. Br. J. Dermatol. 2003, 148, 203–210. [Google Scholar] [CrossRef]
- Kakinuma, T.; Sugaya, M.; Nakamura, K.; Kaneko, F.; Wakugawa, M.; Matsushima, K.; Tamaki, K. Thymus and activation-regulated chemokine (TARC/CCL17) in mycosis fungoides: Serum TARC levels reflect the disease activity of mycosis fungoides. J. Am. Acad. Dermatol. 2003, 48, 23–30. [Google Scholar] [CrossRef]
- Vestergaard, C.; Bang, K.; Gesser, B.; Yoneyama, H.; Matsushima, K.; Larsen, C.G. A Th2 chemokine, TARC, produced by keratinocytes may recruit CLA+CCR4+ lymphocytes into lesional atopic dermatitis skin. J. Investig. Dermatol. 2000, 115, 640–646. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kakinuma, T.; Nakamura, K.; Wakugawa, M.; Mitsui, H.; Tada, Y.; Saeki, H.; Torii, H.; Asahina, A.; Onai, N.; Matsushima, K.; et al. Thymus and activation-regulated chemokine in atopic dermatitis: Serum thymus and activation-regulated chemokine level is closely related with disease activity. J. Allergy Clin. Immunol. 2001, 107, 535–541. [Google Scholar] [CrossRef]
- Ryu, J.H.; Colby, T.V.; Hartman, T.E.; Vassallo, R. Smoking-related interstitial lung diseases: A concise review. Eur. Respir. J. 2001, 17, 122–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fischer, A.; du Bois, R. Interstitial lung disease in connective tissue disorders. Lancet 2012, 380, 689–698. [Google Scholar] [CrossRef]
- Yamane, H.; Ochi, N.; Yamagishi, T.; Honda, Y.; Takeyama, M.; Takigawa, N. Circulating thymus and activation-regulated chemokine/CC chemokine ligand 17 is a strong candidate diagnostic marker for interstitial lung disease in patients with malignant tumors: A result from a pilot study. Ther. Clin. Risk Manag. 2015, 11, 949–959. [Google Scholar] [CrossRef] [Green Version]
- Yamane, H.; Ochi, N.; Nagasaki, Y.; Yamagishi, T.; Honda, Y.; Nozomu Nakagawa, N.; Takeyama, M.; Nakanishi, H.; Takigawa, N. Drug-induced interstitial lung disease in the treatment of malignant lymphoma as a potential diagnostic marker: A comparison of serum Krebs von Lungen-6 and thymus and activation-regulated chemokine/CC chemokine ligand 17. Ther. Clin. Risk Manag. 2018, 14, 1457–1465. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kawashima, T.; Tada, Y.; Asano, Y.; Yazawa, N.; Tomita, M.; Tamaki, Z.; Kubo, M.; Ihn, H.; Sugaya, M.; Kadono, T.; et al. Serum TARC/CCL17 levels are increased in dermatomyositis associated with interstitial lung disease. J. Dermatol. Sci. 2010, 60, 52–54. [Google Scholar] [CrossRef]
- Fujii, H.; Shimada, Y.; Hasegawa, M.; Takehara, K.; Sato, S. Serum levels of a Th1 chemoattractant IP-10 and Th2 chemoattractants, TARC and MDC, are elevated in patients with systemic sclerosis. J. Dermatol. Sci. 2004, 35, 43–51. [Google Scholar] [CrossRef] [PubMed]
- Boin, F.; De Fanis, U.; Bartlett, S.J.; Wigley, F.M.; Rosen, A.; Casolaro, V. T Cell Polarization Identifies Distinct Clinical Phenotypes in Scleroderma Lung Disease. Arthritis Rheum. 2008, 58, 1165–1174. [Google Scholar] [CrossRef]
- Schmidt, K.; Martinez-Gamboa, L.; Meier, S.; Witt, C.; Meisel, C.; Hanitsch, L.G.; Becker, M.O.; Huscher, D.; Burmester, G.R.; Riemekasten, R. Bronchoalveoloar lavage fluid cytokines and chemokines as markers and predictors for the outcome of interstitial lung disease in systemic sclerosis patients. Arthritis Res. Ther. 2009, 11, R111. [Google Scholar] [CrossRef] [Green Version]
- Valenzi, E.; Bulik, M.; Tabib, T.; Morse, C.; Sembrat, J.; Bittar, T.H.; Rojas, M.; Lafyatis, R. Single-cell analysis reveals fibroblast heterogeneity and myofibroblasts in systemic sclerosis-associated interstitial lung disease. Ann. Rheum. Dis. 2019, 78, 1379–1387. [Google Scholar] [CrossRef] [PubMed]
- Matsushita, T.; Hasegawa, M.; Hamaguchi, Y.; Takehara, K.; Sato, S. Longitudinal analysis of serum cytokine concentrations in systemic sclerosis: Association of interleukin 12 elevation with spontaneous regression of skin sclerosis. J. Rheumatol. 2006, 33, 275–284. [Google Scholar] [PubMed]
- Van den Hoogen, F.; Khanna, D.; Fransen, J.; Johnson, S.R.; Baron, M.; Tyndall, A.; Matucci-Cerinic, M.; Naden, R.P.; Medsger, T.A., Jr.; Carreira, P.E.; et al. 2013 classification criteria for systemic sclerosis: An American college of rheumatology/European league against rheumatism collaborative initiative. Ann. Rheum. Dis. 2013, 72, 1747–1755. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- LeRoy, E.C.; Black, C.; Fleischmajer, R.; Jablonska, S.; Krieg, T.; Medsger, T.A., Jr.; Rowell, N.; Wollheim, F. Scleroderma (systemic sclerosis): Classification, subsets and pathogenesis. J. Rheumatol. 1988, 15, 202–205. [Google Scholar]
- Clements, P.J.; Lachenbruch, P.A.; Seibold, J.R.; Zee, B.; Steen, V.D.; Brennan, P.; Silman, A.J.; Allegar, N.; Varga, J.; Massa, M. Skin thickness score in systemic sclerosis: An assessment of interobserver variability in 3 independent studies. J. Rheumatol. 1993, 20, 1892–1896. [Google Scholar]
- Takahashi, T.; Asano, Y.; Yamashita, T.; Nakamura, K.; Saigusa, R.; Miura, S.; Ichimura, Y.; Toyama, T.; Hirabayashi, M.; Taniguchi, T.; et al. A potential contribution of psoriasin to vascular and epithelial abnormalities and inflammation in systemic sclerosis. J. Eur. Acad. Dermatol. Venereol. 2018, 32, 291–297. [Google Scholar] [CrossRef]
- Sato, S.; Nagaoka, T.; Hasegawa, M.; Nishijima, C.; Takehara, K. Elevated serum KL-6 levels in patients with systemic sclerosis: Association with the severity of pulmonary fibrosis. Dermatology 2000, 200, 196–201. [Google Scholar] [CrossRef]
- Yanaba, K.; Hasegawa, M.; Hamaguchi, Y.; Fujimoto, M.; Takehara, K.; Sato, S. Longitudinal analysis of serum KL-6 levels in patients with systemic sclerosis: Association with the activity of pulmonary fibrosis. Clin. Exp. Rheumatol. 2003, 21, 429–436. [Google Scholar]
- Yanaba, K.; Hasegawa, M.; Takehara, K.; Sato, S. Comparative study of serum surfactant protein-D and KL-6 concentrations in patients with systemic sclerosis as markers for monitoring the activity of pulmonary fibrosis. J. Rheumatol. 2004, 31, 1112–1120. [Google Scholar]
- Asano, Y.; Ihn, H.; Yamane, K.; Yazawa, N.; Kubo, M.; Fujimoto, M.; Tamaki, K. Clinical significance of surfactant protein D as a serum marker for evaluating pulmonary fibrosis in patients with systemic sclerosis. Arthritis Rheum. 2001, 44, 1363–1369. [Google Scholar] [CrossRef]
- Cottin, V.; Brown, K.K. Interstitial lung disease associated with systemic sclerosis (SSc-ILD). Respir. Res. 2019, 18, 13. [Google Scholar] [CrossRef]
- Crestani, B.; Seta, N.; Palazzo, E.; Rolland, C.; Venembre, P.; Dehoux, M.; Boutten, A.; Soler, P.; Dombret, M.C.; Kahn, M.F. Interleukin-8 and neutrophils in systemic sclerosis with lung involvement. Am. J. Respir. Crit. Care Med. 1994, 150, 1363–1367. [Google Scholar] [CrossRef]
- Sakamoto, N.; Kakugawa, T.; Hara, A.; Nakashima, S.; Yura, H.; Harada, T.; Ishimoto, H.; Yatera, K.; Kuwatsuka, Y.; Hara, T.; et al. Association of elevated α-defensin levels with interstitial pneumonia in patients with systemic sclerosis. Respir. Res. 2015, 16, 148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Luigi, L.; Sgrò, P.; Duranti, G.; Sabatini, S.; Caporossi, D.; Del Galdo, F.; Dimauro, I.; Antinozzi, C. Sildenafil Reduces Expression and Release of IL-6 and IL-8 Induced by Reactive Oxygen Species in Systemic Sclerosis Fibroblasts. Int. J. Mol. Sci. 2020, 21, 3161. [Google Scholar] [CrossRef] [PubMed]
- Kameda, M.; Otsuka, M.; Chiba, H.; Kuronuma, K.; Hasegawa, T.; Takahashi, H.; Takahashi, H. CXCL9, CXCL10, and CXCL11; biomarkers of pulmonary inflammation associated with autoimmunity in patients with collagen vascular diseases-associated interstitial lung disease and interstitial pneumonia with autoimmune features. PLoS ONE 2020, 15, e0241719. [Google Scholar] [CrossRef] [PubMed]
- Crescioli, C.; Corinaldesi, C.; Riccieri, V.; Raparelli, V.; Vasile, M.; Del Galdo, F.; Valesini, G.; Lenzi, A.; Basili, S.; Antinozzi, C. Association of circulating CXCL10 and CXCL11 with systemic sclerosis. Ann. Rheum. Dis. 2018, 77, 1845–1846. [Google Scholar] [CrossRef] [PubMed] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinical and Laboratory Features | Serum TARC Levels | ||
|---|---|---|---|
| Elevated (n = 20) | Normal (n = 54) | p values | |
| Sex, number of women/men | 18/2 | 48/6 | >0.999 |
| Age, mean years ± SD | 51.6 ± 15.5 | 48.9 ± 17.0 | 0.601 |
| Disease duration, mean years ± SD | 3.0 ± 2.7 | 3.4 ± 4.7 | 0.647 |
| Disease pattern, No. of dcSSc/lcSSc | 19/1 | 36/18 | 0.015 * |
| MRSS, mean points ± SD | 12.5 ± 7.7 | 11.5 ± 8.2 | 0.480 |
| Autoantibodies | |||
| Anti-topoisomerase I | 75% (15/20) | 80% (43/54) | 0.753 |
| Anticentromere | 10% (2/20) | 30% (16/54) | 0.126 |
| Anti-RNA polymerase III | 5% (1/20) | 9% (5/54) | >0.999 |
| Organ involvement | |||
| Lung | |||
| ILD | 90% (18/20) | 63% (34/54) | 0.025 * |
| FVC, mean % predicted ± SD | 85.2 ± 15.3 | 89.3 ± 18.3 | 0.504 |
| DLco, mean % predicted ± SD | 74.4 ± 23.2 | 80.0 ± 20.0 | 0.299 |
| Pulmonary hypertension | 0% (0/20) | 7% (4/54) | 0.569 |
| Esophagus | 85% (17/20) | 69% (38/54) | 0.245 |
| Kidneys | 5% (1/20) | 2% (1/54) | 0.470 |
| Cutaneous symptoms | |||
| Raynaud’s phenomenon | 95% (19/20) | 91% (49/54) | >0.999 |
| Nail fold bleeding | 60% (12/20) | 61% (33/54) | >0.999 |
| Telangiectasia | 30% (6/20) | 56% (30/54) | 0.068 |
| Pitting scars | 45% (9/20) | 50% (27/54) | 0.796 |
| Digital ulcers | 25% (5/20) | 39% (21/54) | 0.411 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kuzumi, A.; Yoshizaki, A.; Ebata, S.; Fukasawa, T.; Yoshizaki-Ogawa, A.; Asano, Y.; Oba, K.; Sato, S. Serum TARC Levels in Patients with Systemic Sclerosis: Clinical Association with Interstitial Lung Disease. J. Clin. Med. 2021, 10, 660. https://doi.org/10.3390/jcm10040660
Kuzumi A, Yoshizaki A, Ebata S, Fukasawa T, Yoshizaki-Ogawa A, Asano Y, Oba K, Sato S. Serum TARC Levels in Patients with Systemic Sclerosis: Clinical Association with Interstitial Lung Disease. Journal of Clinical Medicine. 2021; 10(4):660. https://doi.org/10.3390/jcm10040660
Chicago/Turabian StyleKuzumi, Ai, Ayumi Yoshizaki, Satoshi Ebata, Takemichi Fukasawa, Asako Yoshizaki-Ogawa, Yoshihide Asano, Koji Oba, and Shinichi Sato. 2021. "Serum TARC Levels in Patients with Systemic Sclerosis: Clinical Association with Interstitial Lung Disease" Journal of Clinical Medicine 10, no. 4: 660. https://doi.org/10.3390/jcm10040660