
Concentric and Eccentric Remodelling of the Left Ventricle and Its Association to Function in the Male Athletes Heart: An Exploratory Study
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Design
2.3. Procedures
2.3.1. Anthropometric and Electrocardiography
2.3.2. Echocardiography
2.3.3. Conventional Echocardiography
2.3.4. Two-Dimensional Speckle Tracking Echocardiography
2.3.5. Temporal Speckle Tracking Echocardiography
2.4. Statistical Analysis
2.5. Laboratory 2DSTE Intra-Observer Reproducibility
3. Results
3.1. Demographics
3.2. Conventional Echocardiography
3.3. Two-Dimensional Speckle Tracking Echocardiography
3.4. Temporal Speckle Tracking Echocardiography
4. Discussion
4.1. Conventional Echocardiography
4.2. Two-Dimensional Speckle Tracking Echocardiography
4.3. Temporal Speckle Tracking Echocardiography
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Prior, D.L.; La Gerche, A. The athlete’s heart. Heart 2012, 98, 947–955. [Google Scholar] [CrossRef] [PubMed]
- Beaudry, R.; Haykowsky, M.J.; Baggish, A.; La Gerche, A. A Modern Definition of the Athlete’s Heart—For Research and the Clinic. Cardiol. Clin. 2016, 34, 507–514. [Google Scholar] [CrossRef] [PubMed]
- Brown, B.; Somauroo, J.; Green, D.J.; Wilson, M.; Drezner, J.; George, K.; Oxborough, D. The complex phenotype of the Athlete’s heart: Implications for preparticipation screening. Exerc. Sport Sci. Rev. 2017, 45, 96–104. [Google Scholar] [CrossRef]
- Finocchiaro, G.; Dhutia, H.; D’Silva, A.; Malhotra, A.; Steriotis, A.; Millar, L.; Prakash, K.; Narain, R.; Papadakis, M.; Sharma, R.; et al. Effect of Sex and Sporting Discipline on LV Adaptation to Exercise. JACC Cardiovasc. Imaging 2017, 10, 965–972. [Google Scholar] [CrossRef] [PubMed]
- Utomi, V.; Oxborough, D.; Whyte, G.P.; Somauroo, J.; Sharma, S.; Shave, R.; Atkinson, G.; George, K. Systematic review and meta-analysis of training mode, imaging modality and body size influences on the morphology and function of the male athlete’s heart. Heart 2013, 99, 1727–1733. [Google Scholar] [CrossRef]
- Utomi, V.; Oxborough, D.; Ashley, E.; Lord, R.; Fletcher, S.; Stembridge, M.; Shave, R.; Hoffman, M.D.; Whyte, G.; Somauroo, J.; et al. Predominance of normal left ventricular geometry in the male ‘athlete’s heart’. Heart 2014, 100, 1264–1271. [Google Scholar] [CrossRef]
- Brown, B.; Millar, L.; Somauroo, J.; George, K.; Sharma, S.; La Gerche, A.; Forsythe, L.; Oxborough, D. Left ventricular remodeling in elite and sub-elite road cyclists. Scand. J. Med. Sci. Sport. 2020, 30, 1132–1139. [Google Scholar] [CrossRef] [Green Version]
- Forsythe, L.; MacIver, D.H.; Johnson, C.; George, K.; Somauroo, J.; Papadakis, M.; Brown, B.; Qasem, M.; Oxborough, D. The relationship between left ventricular structure and function in the elite rugby football league athlete as determined by conventional echocardiography and myocardial strain imaging. Int. J. Cardiol. 2018, 261, 211–217. [Google Scholar] [CrossRef]
- Spence, A.L.; Naylor, L.H.; Carter, H.H.; Buck, C.L.; Dembo, L.; Murray, C.P.; Watson, P.; Oxborough, D.; George, K.P.; Green, D.J. A prospective randomised longitudinal MRI study of left ventricular adaptation to endurance and resistance exercise training in humans. J. Physiol. 2011, 589, 5443–5452. [Google Scholar] [CrossRef] [Green Version]
- Mont, L.; Pelliccia, A.; Sharma, S.; Biffi, A.; Borjesson, M.; Terradellas, J.B.; Carré, F.; Guasch, E.; Heidbuchel, H.; La Gerche, A.; et al. Pre-participation cardiovascular evaluation for athletic participants to prevent sudden death: Position paper from the EHRA and the EACPR, branches of the ESC. Endorsed by APHRS, HRS, and SOLAECE. Eur. J. Prev. Cardiol. 2017, 24, 41–69. [Google Scholar] [CrossRef] [Green Version]
- Pelliccia, A.; Caselli, S.; Sharma, S.; Basso, C.; Bax, J.J.; Corrado, D.; D’Andrea, A.; D’Ascenzi, F.; Di Paolo, F.M.; Edvardsen, T.; et al. European Association of Preventive Cardiology (EAPC) and European Association of Cardiovascular Imaging (EACVI) joint position statement: Recommendations for the indication and interpretation of cardiovascular imaging in the evaluation of the athlete’s heart. Eur. Heart J. 2018, 39, 1949–1969. [Google Scholar] [CrossRef] [PubMed]
- Augustine, D.X.; Howard, L. Left Ventricular Hypertrophy in Athletes: Differentiating Physiology From Pathology. Curr. Treat. Options Cardiovasc. Med. 2018, 20, 96. [Google Scholar] [CrossRef] [PubMed]
- Millar, L.M.; Fanton, Z.; Finocchiaro, G.; Sanchez-Fernandez, G.; Dhutia, H.; Malhotra, A.; Merghani, A.; Papadakis, M.; Behr, E.R.; Bunce, N.; et al. Differentiation between athlete’s heart and dilated cardiomyopathy in athletic individuals. Heart 2020, 106, 1059–1065. [Google Scholar] [CrossRef] [PubMed]
- Abergel, E.; Chatellier, G.; Hagege, A.; Oblak, A.; Linhart, A.; Ducardonnet, A.; Menard, J. Serial left ventricular adaptations in world-class professional cyclists: Implications for disease screening and follow-up. J. Am. Coll. Cardiol. 2004, 44, 144–149. [Google Scholar] [CrossRef] [Green Version]
- Elliott, P.M.; Anastasakis, A.; Borger, M.A.; Borggrefe, M.; Cecchi, F.; Charron, P.; Hagege, A.A.; Lafont, A.; Limongelli, G.; Mahrholdt, H.; et al. 2014 ESC Guidelines on diagnosis and management of hypertrophic cardiomyopathy: The Task Force for the Diagnosis and Management of Hypertrophic Cardiomyopathy of the European Society of Cardiology (ESC). Eur. Heart J. 2014, 35, 2733–2779. [Google Scholar] [CrossRef]
- Forsythe, L.; George, K.; Oxborough, D. Speckle Tracking Echocardiography for the Assessment of the Athlete’s Heart: Is It Ready for Daily Practice? Curr. Treat. Options Cardiovasc. Med. 2018, 20, 83. [Google Scholar] [CrossRef] [Green Version]
- D’Ascenzi, F.; Caselli, S.; Solari, M.; Pelliccia, A.; Cameli, M.; Focardi, M.; Padeletti, M.; Corrado, D.; Bonifazi, M.; Mondillo, S. Novel echocardiographic techniques for the evaluation of athletes’ heart: A focus on speckle-tracking echocardiography. Eur. J. Prev. Cardiol. 2016, 23, 437–446. [Google Scholar] [CrossRef]
- D’Andrea, A.; Sperlongano, S.; Russo, V.; D’Ascenzi, F.; Benfari, G.; Renon, F.; Palermi, S.; Ilardi, F.; Giallauria, F.; Limongelli, G.; et al. The role of multimodality imaging in athlete’s heart diagnosis: Current status and future directions. J. Clin. Med. 2021, 10, 5126. [Google Scholar] [CrossRef]
- Beaumont, A.; Grace, F.; Richards, J.; Hough, J.; Oxborough, D.; Sculthorpe, N. Left Ventricular Speckle Tracking-Derived Cardiac Strain and Cardiac Twist Mechanics in Athletes: A Systematic Review and Meta-Analysis of Controlled Studies. Sport. Med. 2017, 47, 1145–1170. [Google Scholar] [CrossRef] [Green Version]
- Butz, T.; Van Buuren, F.; Mellwig, K.-P.; Langer, C.; Plehn, G.; Meissner, A.; Trappe, H.-J.; Horstkotte, D.; Faber, L. Two-dimensional strain analysis of the global and regional myocardial function for the differentiation of pathologic and physiologic left ventricular hypertrophy: A study in athletes and in patients with hypertrophic cardiomyopathy. Int. J. Cardiovasc. Imaging 2011, 27, 91–100. [Google Scholar] [CrossRef]
- Kansal, M.M.; Lester, S.J.; Surapaneni, P.; Sengupta, P.P.; Appleton, C.P.; Ommen, S.R.; Ressler, S.W.; Hurst, R.T. Usefulness of two-dimensional and speckle tracking echocardiography in ‘gray zone’ left ventricular hypertrophy to differentiate professional football player’s heart from hypertrophic cardiomyopathy. Am. J. Cardiol. 2011, 108, 1322–1326. [Google Scholar] [CrossRef]
- Richand, V.; Lafitte, S.; Reant, P.; Serri, K.; Lafitte, M.; Brette, S.; Kerouani, A.; Chalabi, H.; Dos Santos, P.; Douard, H.; et al. An Ultrasound Speckle Tracking (Two-Dimensional Strain) Analysis of Myocardial Deformation in Professional Soccer Players Compared with Healthy Subjects and Hypertrophic Cardiomyopathy. Am. J. Cardiol. 2007, 100, 128–132. [Google Scholar] [CrossRef] [PubMed]
- Pacileo, G.; Baldini, L.; Limongelli, G.; Di Salvo, G.; Iacomino, M.; Capogrosso, C.; Rea, A.; D’Andrea, A.; Russo, M.G.; Calabrò, R. Prolonged left ventricular twist in cardiomyopathies: A potential link between systolic and diastolic dysfunction. Eur. J. Echocardiogr. 2011, 12, 841–849. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harkness, A.; Ring, L.; Augustine, D.X.; Oxborough, D.; Robinson, S.; Sharma, V. Normal reference intervals for cardiac dimensions and function for use in echocardiographic practice: A guideline from the British Society of Echocardiography. Echo Res. Pract. 2020, 7, G1–G18. [Google Scholar] [CrossRef]
- Sharma, S.; Drezner, J.A.; Baggish, A.; Papadakis, M.; Wilson, M.G.; Prutkin, J.M.; La Gerche, A.; Ackerman, M.J.; Börjesson, M.; Salerno, J.C.; et al. International recommendations for electrocardiographic interpretation in athletes. Eur. Heart J. 2018, 39, 1466–1480. [Google Scholar] [CrossRef] [PubMed]
- Robinson, S.; Rana, B.; Oxborough, D.; Steeds, R.; Monaghan, M.; Stout, M.; Pearce, K.; Harkness, A.; Ring, L.; Paton, M.; et al. A practical guideline for performing a comprehensive transthoracic echocardiogram in adults: The British Society of Echocardiography minimum dataset. Echo Res. Pract. 2020, 7, G59–G93. [Google Scholar] [CrossRef] [PubMed]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mor-Avi, V.; Lang, R.M.; Badano, L.P.; Belohlavek, M.; Cardim, N.M.; Derumeaux, G.; Galderisi, M.; Marwick, T.; Nagueh, S.F.; Sengupta, P.P.; et al. Current and evolving echocardiographic techniques for the quantitative evaluation of cardiac mechanics: ASE/EAE consensus statement on methodology and indications: Endorsed by the Japanese Society of Echocardiography. J. Am. Soc. Echocardiogr. 2011, 24, 277–313. [Google Scholar] [CrossRef]
- Johnson, C.; Kuyt, K.; Oxborough, D.; Stout, M. Practical tips and tricks in measuring strain, strain rate and twist for the left and right ventricles. Echo Res. Pract. 2019, 6, R87–R98. [Google Scholar] [CrossRef] [Green Version]
- MacIver, D.H.; Townsend, M. A novel mechanism of heart failure with normal ejection fraction. Heart 2008, 94, 446–449. [Google Scholar] [CrossRef]
- D’Andrea, A.; The Echocardiography Study Group of the Italian Society of Cardiology; Radmilovic, J.; Carbone, A.; Mandoli, G.E.; Santoro, C.; Evola, V.; Bandera, F.; D’Ascenzi, F.; Bossone, E.; et al. Speckle tracking evaluation in endurance athletes: The “optimal” myocardial work. Int. J. Cardiovasc. Imaging 2020, 36, 1679–1688. [Google Scholar] [CrossRef] [PubMed]
- Baggish, A.L.; Battle, R.W.; Beaver, T.A.; Border, W.L.; Douglas, P.S.; Kramer, C.M.; Martinez, M.W.; Mercandetti, J.H.; Phelan, D.; Singh, T.K.; et al. Recommendations on the Use of Multimodality Cardiovascular Imaging in Young Adult Competitive Athletes: A Report from the American Society of Echocardiography in Collaboration with the Society of Cardiovascular Computed Tomography and the Society for Cardiovascular Magnetic Resonance. J. Am. Soc. Echocardiogr. 2020, 33, 523–549. [Google Scholar] [CrossRef] [PubMed]
- Cappelli, F.; Toncelli, L.; Cappelli, B.; De Luca, A.; Stefani, L.; Maffulli, N.; Galanti, G. Adaptative or maladaptative hypertrophy, different spatial distribution of myocardial contraction. Clin. Physiol. Funct. Imaging 2010, 30, 6–12. [Google Scholar] [CrossRef]
- Schnell, F.; Matelot, D.; Daudin, M.; Kervio, G.; Mabo, P.; Carré, F.; Donal, E. Mechanical Dispersion by Strain Echocardiography: A Novel Tool to Diagnose Hypertrophic Cardiomyopathy in Athletes. J. Am. Soc. Echocardiogr. 2017, 30, 251–261. [Google Scholar] [CrossRef] [PubMed]
- Buckberg, G.; Hoffman, J.I.; Mahajan, A.; Saleh, S.; Coghlan, C. Cardiac Mechanics Revisited: The relationship of cardiac architecture to ventricular function. Circulation 2008, 118, 2571–2587. [Google Scholar] [CrossRef] [Green Version]
- Fukuta, H.; Little, W.C. The Cardiac Cycle and the Physiologic Basis of Left Ventricular Contraction, Ejection, Relaxation, and Filling. Heart Fail. Clin. 2008, 4, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Nagueh, S.F.; Smiseth, O.A.; Appleton, C.P.; Byrd, B.F., 3rd; Dokainish, H.; Edvardsen, T.; Flachskampf, F.A.; Gillebert, T.C.; Klein, A.L.; Lancellotti, P.; et al. Recommendations for the Evaluation of Left Ventricular Diastolic Function by Echocardiography: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2016, 29, 277–314. [Google Scholar] [CrossRef] [Green Version]
- Kovács, A.; Apor, A.; Nagy, A.; Vágó, H.; Tóth, A.; Kováts, T.; Sax, B.; Széplaki, G.; Becker, D.; Merkely, B. Left ventricular untwisting in athlete’s heart: Key role in early diastolic filling? Int. J. Sport. Med. 2014, 35, 259–264. [Google Scholar] [CrossRef] [Green Version]
- Rowland, T. Echocardiography and circulatory response to progressive endurance exercise. Sport. Med. 2008, 38, 541–551. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Concentric (n = 15; Median (Range)) | Eccentric (n = 15; Median (Range)) | Normal (n = 15; Median (Range)) | |
|---|---|---|---|
| Age (y) | 24 (19–34) | 24 (19–34) | 25 (19–34) |
| Height (m) | 1.82 (1.71–1.94) | 1.82 (1.74–1.89) | 1.82 (1.72–1.90) |
| Body Mass (kg) | 76 (64–105) | 76 (67–99) | 76 (69–99) |
| Body Surface Area (m2) | 1.99 (1.74–2.30) | 1.96 (1.83–2.19) | 1.95 (1.86–2.25) |
| Training Days per Week (days/week) | 6 (5–7) | 6 (5–7) | 6 (5–7) |
| Training Hours per Week (hours/week) | 20 (8–40) | 15 (6–40) | 17 (9–40) |
| Heart Rate (beats/min) | 55 (40–67) | 50 (39–65) | 52 (38–95) |
| Concentric (Median (Range)) | Eccentric (Median (Range)) | Normal (Median (Range)) | |
|---|---|---|---|
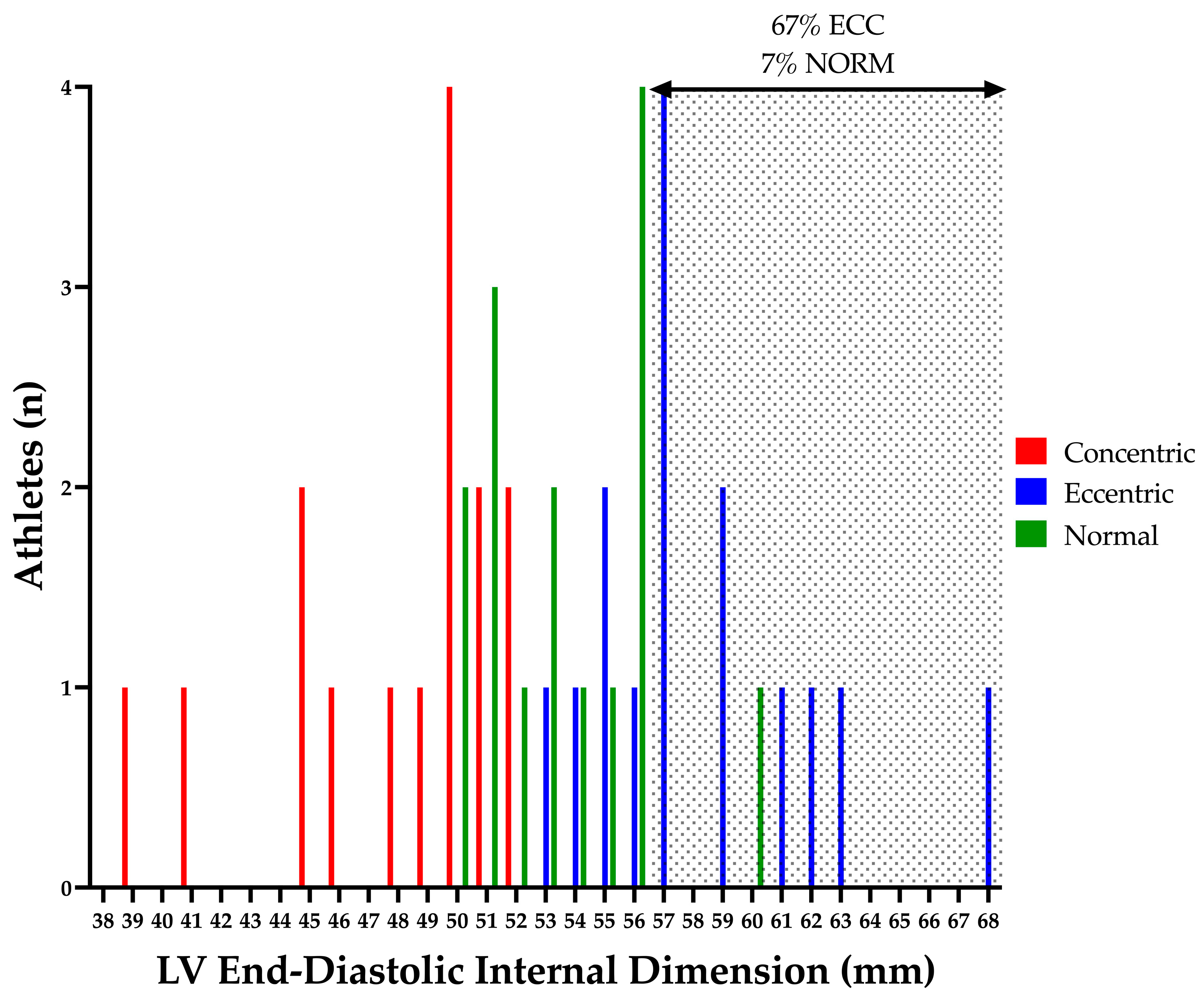
| LVIDd (mm) | 50 (39–52) ‡† | 57 (53–68) ‡* | 53 (50–60) †* |
| LVIDdi (BSA; mm/m2) | 25 (19–29) ‡† | 29 (26–34) ‡* | 27 (23–30) †* |
| LVIDdi0.5 (BSA^0.5; mm/m2^0.5) | 34 (27–39) ‡† | 40 (39–48) ‡* | 38 (34–42) †* |
| LVIDs (mm) | 33 (30–38) ‡† | 37 (33–48) ‡ | 37 (33–40) † |
| LVIDsi (BSA; mm/m2) | 17 (15–19) ‡† | 19 (18–24) ‡ | 18 (16–21) † |
| LVIDsi0.5 (BSA^0.5; mm/m2^0.5) | 24 (21–26) ‡† | 27 (24–34) ‡ | 26 (24–28) † |
| LV Mass (g) | 207 (105–233) ‡ | 226 (212–365) ‡* | 191 (154–213) * |
| LV Massi (BSA; g/m2) | 100 (50–127) ‡ | 116 (110–183) ‡* | 99 (74–107) * |
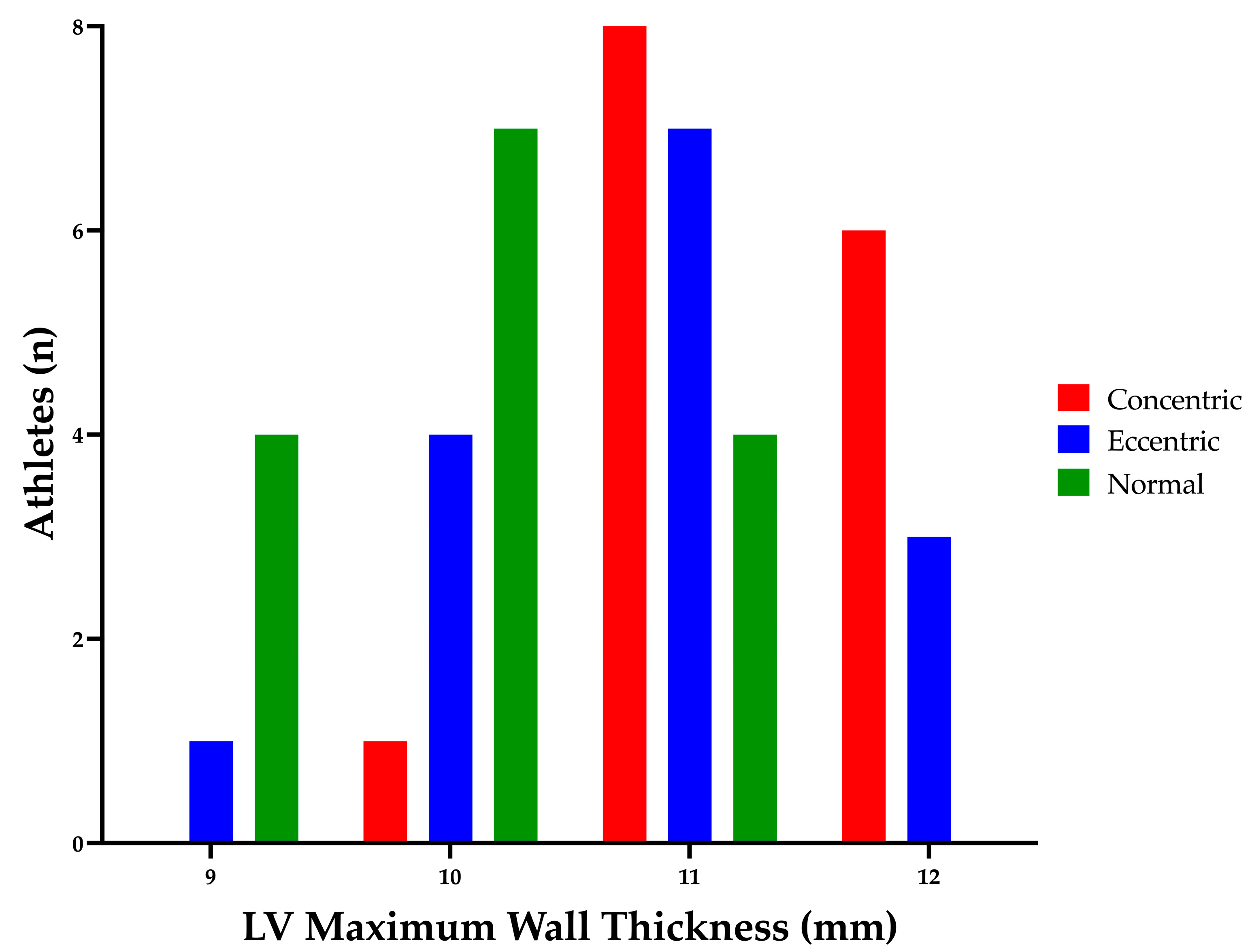
| Mean Wall Thickness (mm) | 10 (9–12) † | 10 (9–11) * | 9 (8–10) †* |
| Max Wall Thickness (mm) | 11 (10–12) † | 11 (9–12) * | 10 (9–11) †* |
| RWT (ratio) | 0.46 (0.42–0.51) ‡† | 0.36 (0.27–0.40) ‡ | 0.36 (0.28–0.41) † |
| LVEDV (mL) | 138 (79–201) | 153 (125–198) | 152 (125–192) |
| LVEDVi (BSA; mL/m2) | 71 (43–99) | 79 (57–99) | 80 (56–100) |
| LVEDVi1.5 (BSA^1.5; mm/m2^1.5) | 51 (32–69) | 55 (39–72) | 58 (37–72) |
| LVESV (mL) | 52 (20–105) | 68 (38–90) | 65 (50–90) |
| LVESVi (BSA; mL/m2) | 25 (11–51) | 34 (20–48) | 34 (24–46) |
| LVESVi1.5 (BSA^1.5; mm/m2^1.5) | 17 (8–36) † | 24 (15–35) | 25 (16–33) † |
| Stroke Volume (mL) | 87 (59–114) | 94 (65–111) | 90 (70–107) |
| Cardiac Output (L/min) | 4.7 (2.8–6.8) | 4.6 (2.9–5.6) | 4.6 (3.3–7.0) |
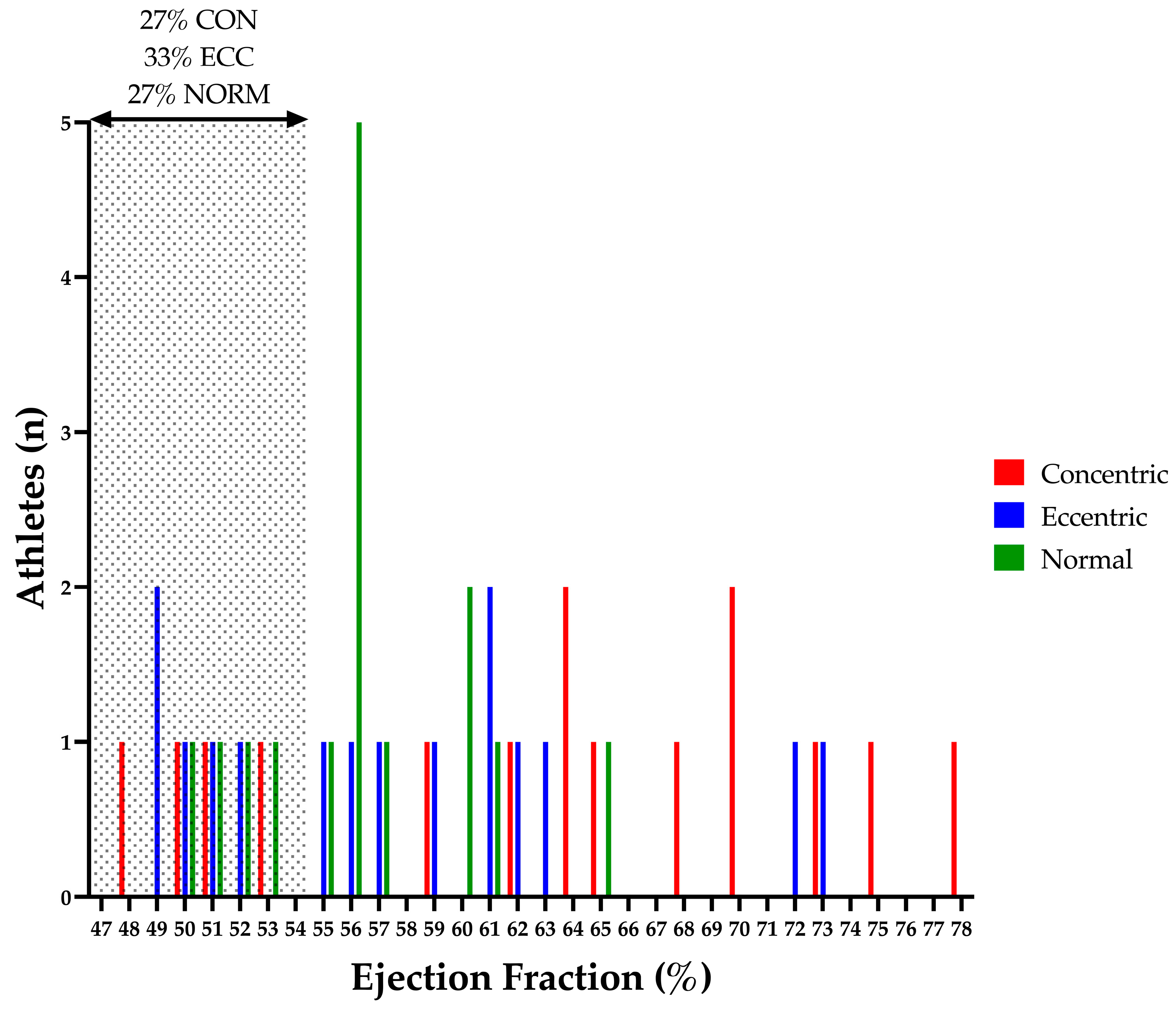
| Ejection Fraction (%) | 64 (48–78) † | 57 (49–73) | 56 (50–65) † |
| Concentric (Median (Range)) | Eccentric (Median (Range)) | Normal (Median (Range)) | |
|---|---|---|---|
| MV E (m/s) | 0.77 (0.53–1.05) | 0.74 (0.49–1.02) | 0.73 (0.54–0.91) |
| MV A (m/s) | 0.40 (0.20–0.58) | 0.35 (0.23–0.55) | 0.44 (0.24–0.63) |
| E:A (ratio) | 1.88 (1.15–5.25) | 2.06 (1.32–3.40) | 1.86 (0.86–3.17) |
| Septal S’ (cm/s) | 9 (7–11) | 8 (7–10) | 9 (8–11) |
| Septal E’ (cm/s) | 11 (8–17) | 11 (9–14) | 12 (9–16) |
| Septal A’ (cm/s) | 7 (5–10) | 7 (5–10) | 7 (5–9) |
| Lateral S’ (cm/s) | 11 (8–17 | 11 (7–18) | 12 (9–14) |
| Lateral E’ (cm/s) | 19 (10–25) | 17 (13–22) | 19 (10–26) |
| Lateral A’ (cm/s) | 7 (4–15) | 7 (4–13) | 6 (5–8) |
| Average S’ (cm/s) | 10 (8–14) | 10 (8–13) | 10 (9–13) |
| Average E’ (cm/s) | 16 (10–20) | 14 (11–18) | 16 (11–21) |
| Average A’ (cm/s) | 7 (5–12) | 7 (5–10) | 7 (5–9) |
| Average E:E’ (ratio) | 4.8 (3.4–8.1) | 5.5 (3.6–6.2) | 4.6 (3.6–7.3) |
| LVOT Velocity (m/s) | 1.05 (0.67–1.68) | 1.13 (0.84–1.5) | 1.1 (0.78–1.22) |
| LVOT VTI (cm) | 21.9 (14.6–32.1) | 22.8 (18.0–32.2) | 22.5 (16.2–25.9) |
| Aortic Velocity (m/s) | 1.24 (1.15–1.78) | 1.28 (1.04–1.73) | 1.26 (1.04–1.45) |
| Concentric (Median (Range)) | Eccentric (Median (Range)) | Normal (Median (Range)) | |
|---|---|---|---|
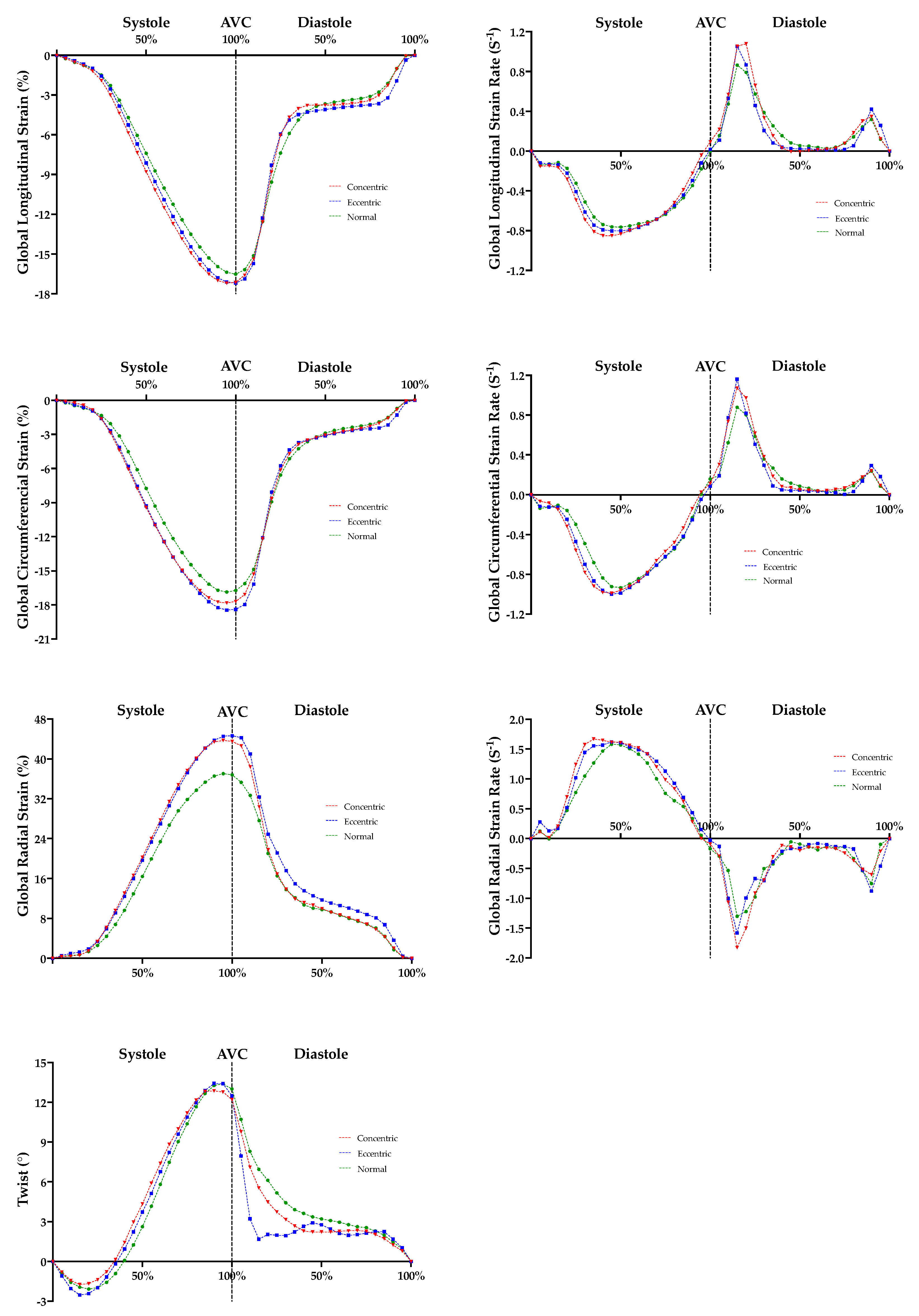
| GLS (%) | −16.9 (−14.9–20.6) | −17.9 (−13.0–22.1) | −16.9 (−12.8–19.4) |
| GLSr S (s−1) | −0.91 (−0.77–1.04) | −0.85 (−0.70–1.07) | −0.80 (−0.73–1.09) |
| GLSr E (s−1) | 1.32 (0.79–1.86) | 1.21 (0.70–1.63) | 1.29 (0.49–1.56) |
| GLSr A (s−1) | 0.53 (0.37–0.66) | 0.47 (0.28–0.95) | 0.41 (0.28–0.71) |
| GCS (%) | −18.1 (−13.6–24.5) | −18.7 (−15.6–22.4) | −18.0 (−13.5–19.7) |
| GCSr S (s−1) | −1.02 (−0.80–1.41) | −1.09 (−0.87–1.26) | −0.97 (−0.73–1.22) |
| GCSr E (s−1) | 1.45 (0.74–1.90) | 1.43 (0.90–1.82) | 1.28 (0.87–1.88) |
| GCSr A (s−1) | 0.37 (0.10–0.61) | 0.42 (0.18–0.75) | 0.35 (0.22–0.47) |
| GRS (%) | 42.2 (30.3–70.5) | 50.0 (39.2–60.0) | 40.6 (29.9–57.0) |
| GRSr S (s−1) | 2.00 (1.45–2.77) | 2.19 (1.62–2.89) | 2.05 (1.47–3.03) |
| GRSr E (s−1) | −2.62 (−1.79–4.32) | −2.99 (−2.09–3.99) | −2.69 (−1.63–4.92) |
| GRSr A (s−1) | −1.08 (−0.64–1.83) | −1.18 (−0.62–2.21) | −1.14 (−0.67–2.24) |
| Twist (°) | 14.9 (3.7–25.3) | 12.5 (6.3–20.8) | 13.2 (8.8–24.2) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Johnson, C.; Sculthorpe, N.; George, K.; Stout, M.; Procter, W.; Cooper, R.M.; Oxborough, D. Concentric and Eccentric Remodelling of the Left Ventricle and Its Association to Function in the Male Athletes Heart: An Exploratory Study. J. Cardiovasc. Dev. Dis. 2023, 10, 269. https://doi.org/10.3390/jcdd10070269
Johnson C, Sculthorpe N, George K, Stout M, Procter W, Cooper RM, Oxborough D. Concentric and Eccentric Remodelling of the Left Ventricle and Its Association to Function in the Male Athletes Heart: An Exploratory Study. Journal of Cardiovascular Development and Disease. 2023; 10(7):269. https://doi.org/10.3390/jcdd10070269
Chicago/Turabian StyleJohnson, Christopher, Nicholas Sculthorpe, Keith George, Martin Stout, William Procter, Robert M. Cooper, and David Oxborough. 2023. "Concentric and Eccentric Remodelling of the Left Ventricle and Its Association to Function in the Male Athletes Heart: An Exploratory Study" Journal of Cardiovascular Development and Disease 10, no. 7: 269. https://doi.org/10.3390/jcdd10070269