Analysis of Epidemiological Characteristics of Scarlet Fever in Zhejiang Province, China, 2004–2018

Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Source
2.2. Study Area
2.3. Statistical Methods
2.4. Ethical Statement
3. Results
3.1. General Characteristics of Scarlet Fever
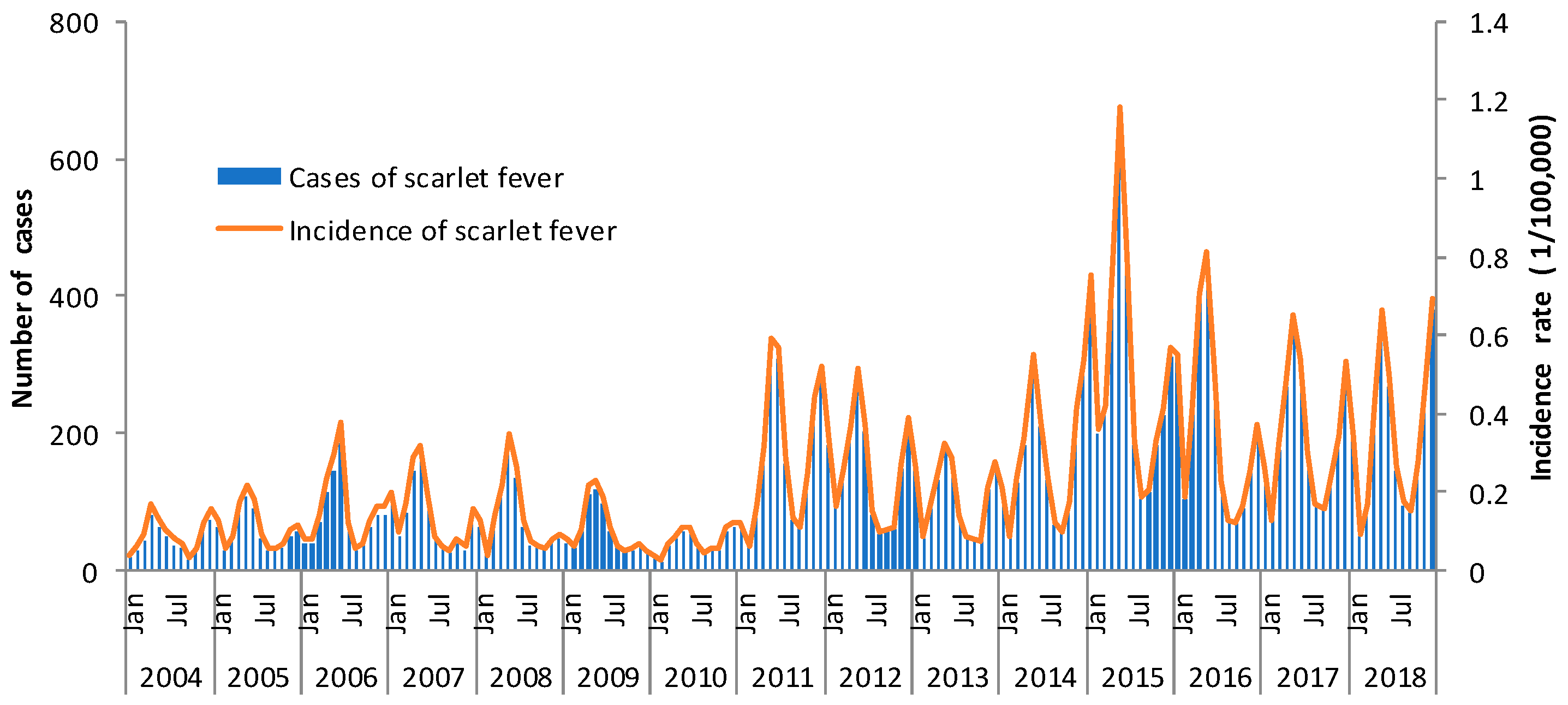
3.2. Temporal Distribution
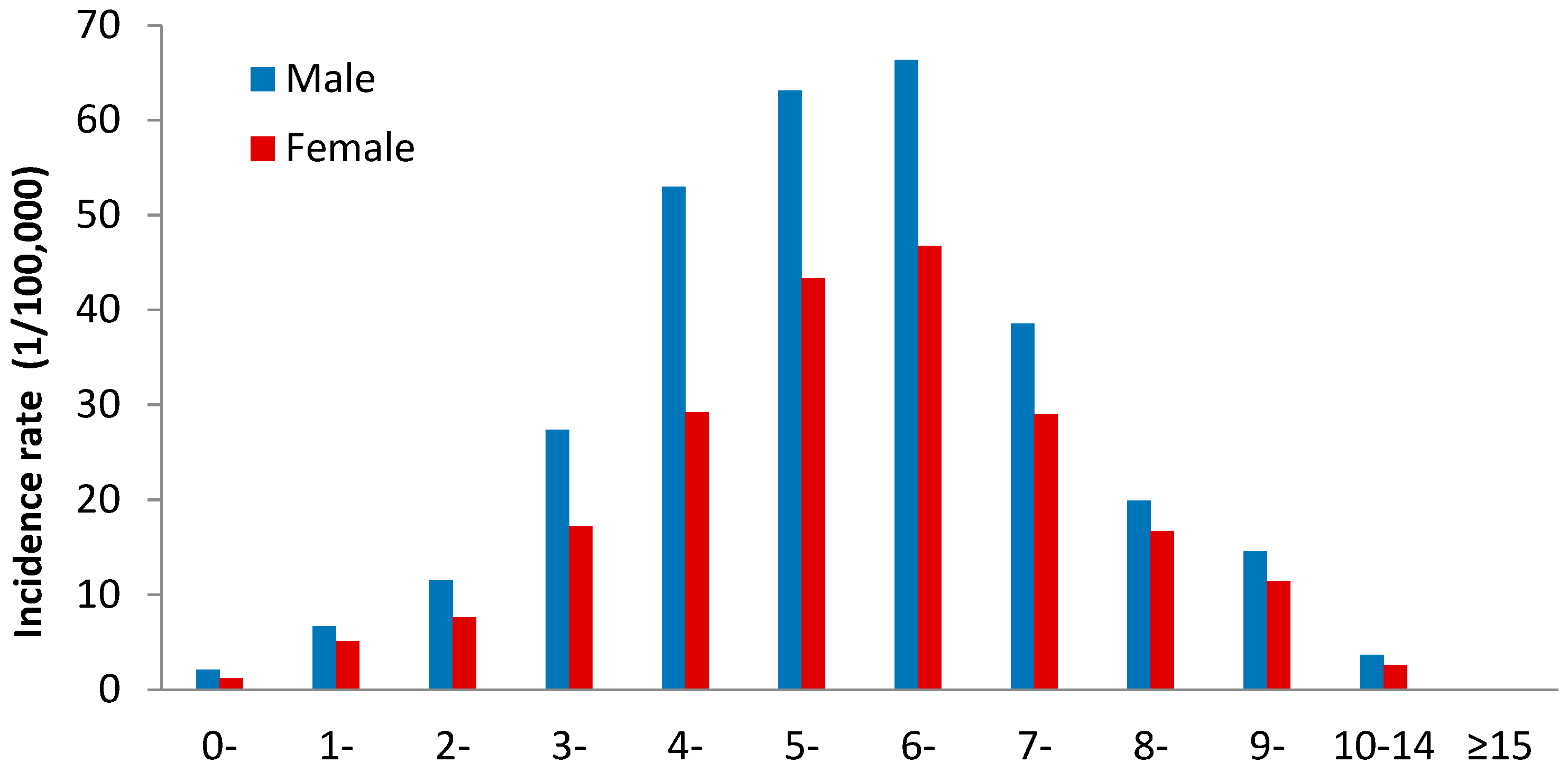
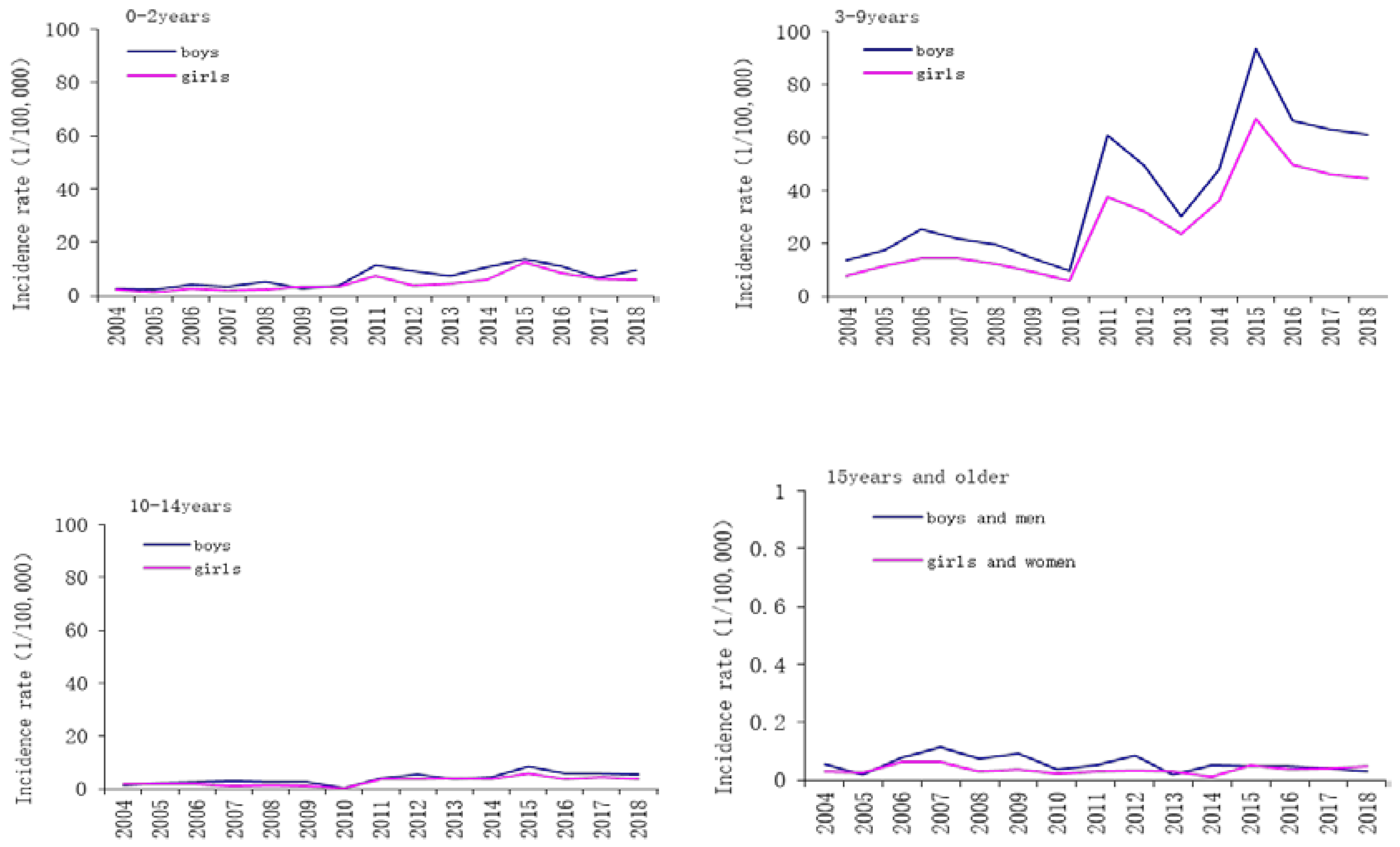
3.3. Population Distribution
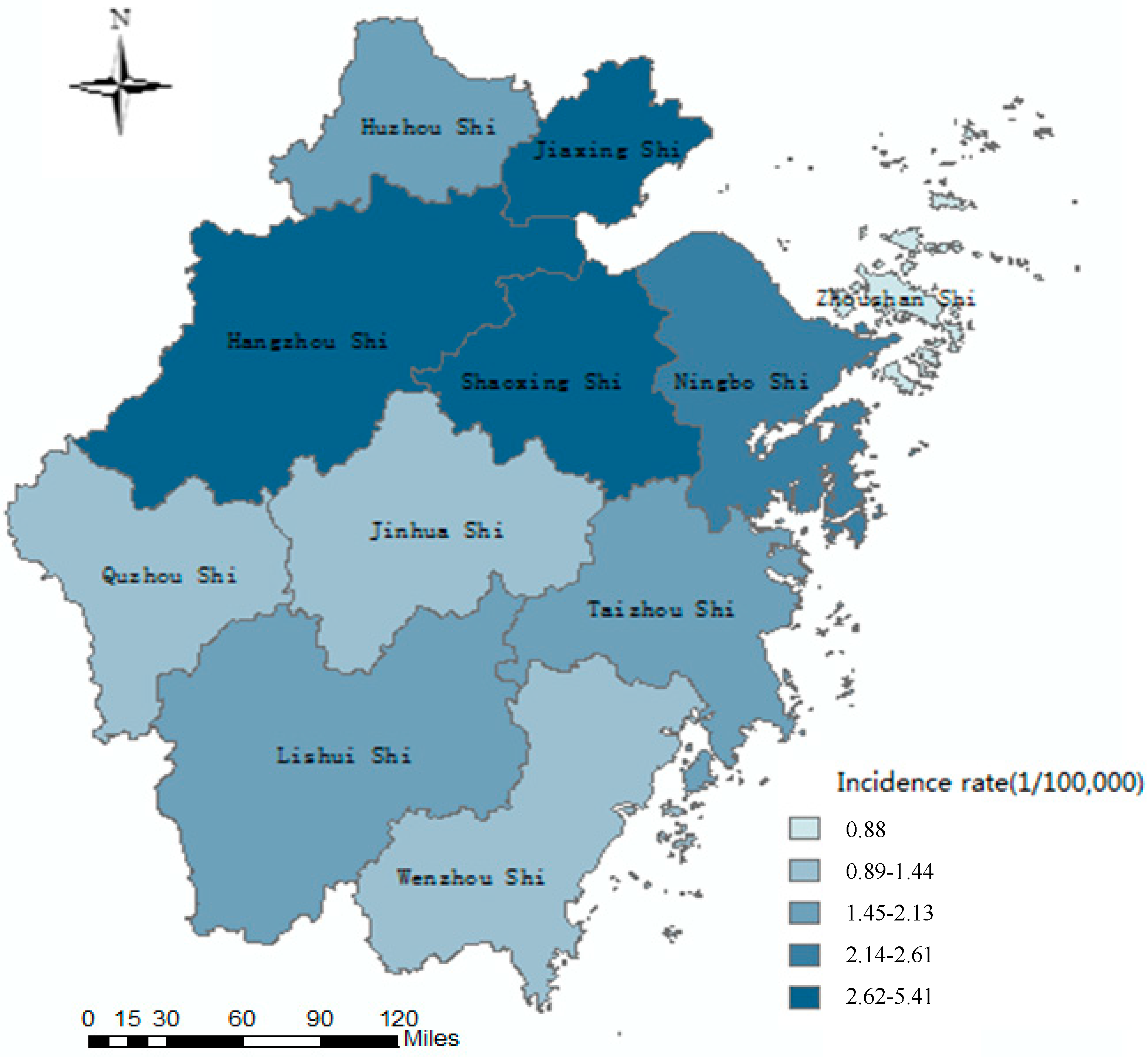
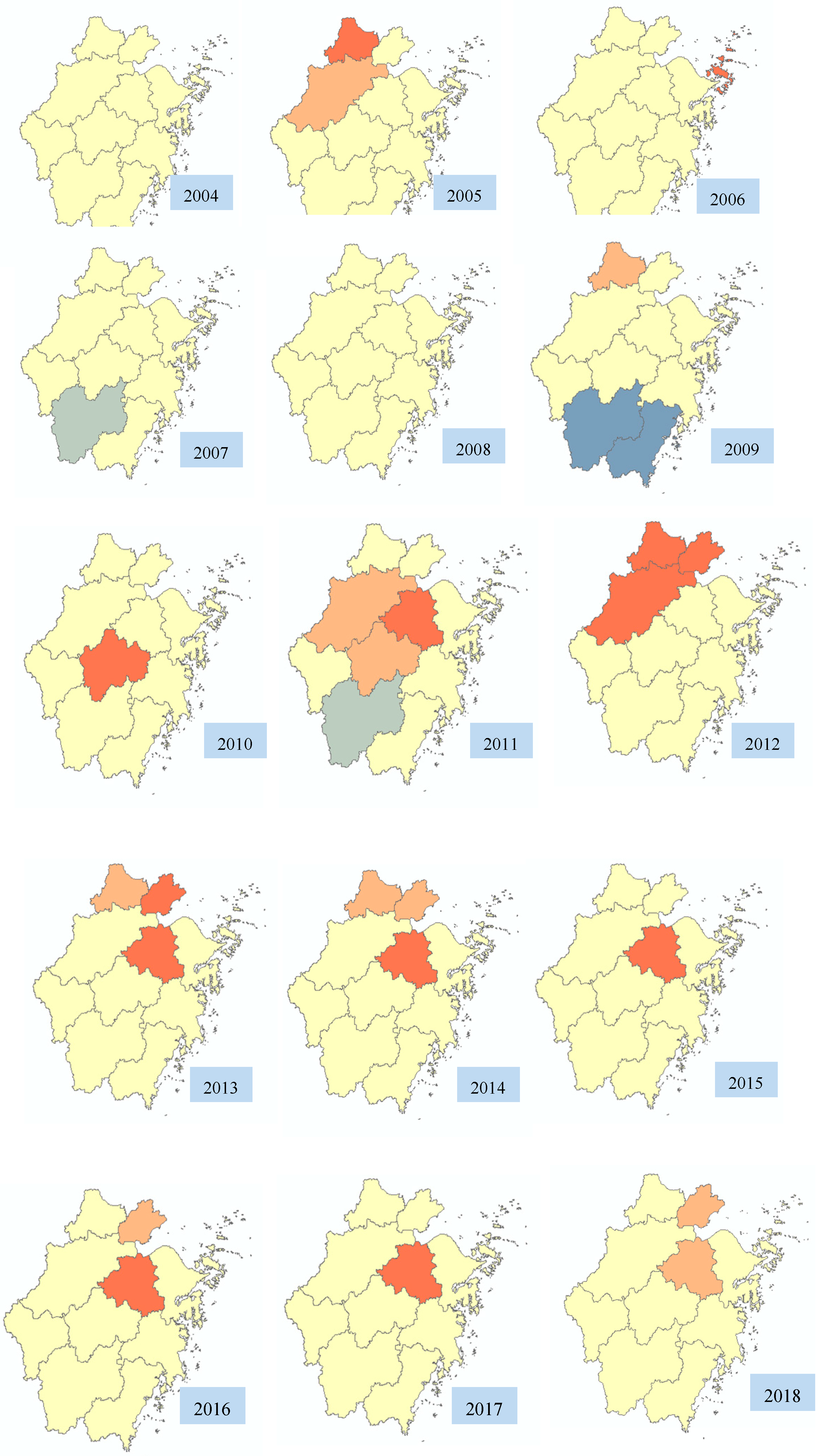
3.4. Spatial Distribution
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Mahara, G.; Chhetri, J.K.; Guo, X. Increasing prevalence of scarlet fever in China. BMJ 2016, 353, i2689. [Google Scholar] [CrossRef]
- Yang, S.G.; Dong, H.J.; Li, F.R.; Xie, S.Y.; Cao, H.C.; Xia, S.C.; Yu, Z.; Li, L.J. Report and analysis of a scarlet fever outbreak among adults through food-borne transmission in China. J. Infect. 2007, 55, 419–424. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Q.; Liu, W.D.; Ma, W.; Shi, Y.Y.; Wu, Y.; Li, Y.; Liang, S.Y.; Zhu, Y.F.; Zhou, M.H. Spatiotemporal epidemiology of scarlet fever in Jiangsu Province, China, 2005–2015. BMC Infect. Dis. 2017, 17, 596. [Google Scholar] [CrossRef] [PubMed]
- Tyrrell, G.J.; Fathima, S.; Kakulphimp, J.; Bell, C. Increasing Rates of Invasive Group A Streptococcal Disease in Alberta, Canada; 2003–2017. Open Forum Infect. Dis. 2018, 5, 177. [Google Scholar] [CrossRef] [PubMed]
- Feenry, K.T.; Dowse, G.K.; Keil, A.D.; Mackaay, C.; McLellan, D. Epidemiological features and control of an outbreak of scarlet fever in a Perth primary school. Commun. Dis. Intell. Q. Rep. 2005, 29, 386–390. [Google Scholar]
- Hoek, M.; Dalling, J.; Thompson, S.; King, S.; Bell, A.; Evans, M.; Cotterill, S.; Lewis, D. Scarlet fever outbreak in two nurseries in southwest England. Euro Surveill. 2006, 11, E060302-5. [Google Scholar] [CrossRef]
- Staszewska-Jakubik, E.; Czarkowski, M.P.; Kondej, B. Scarlet fever in Poland in 2014. Przegl. Epidemiol. 2016, 70, 195–202. [Google Scholar]
- Hsieh, Y.C.; Huang, Y.C. Scarlet fever outbreak in Hong Kong, 2011. J. Microbiol. Immunol. Infect. 2011, 44, 409–411. [Google Scholar] [CrossRef] [Green Version]
- Park, D.W.; Kim, S.H.; Park, J.W.; Kim, M.J.; Cho, S.J.; Park, H.J.; Jung, S.H.; Seo, M.H.; Lee, Y.S.; Kim, B.H.; et al. Incidence and Characteristics of Scarlet Fever, South Korea, 2008–2015. Emerg. Infect. Dis. 2017, 23, 658–661. [Google Scholar] [CrossRef]
- Tang, J.H.; Tseng, T.J.; Chan, T.C. Detecting spatio-temporal hotspots of scarlet fever in Taiwan with spatio-temporal Gi* statistic. PLoS ONE 2019, 14, e0215434. [Google Scholar] [CrossRef]
- Liu, Y.H.; Chan, T.C.; Yap, L.W.; Luo, Y.P.; Xu, W.J.; Qin, S.W.; Zhao, N.; Yu, Z.; Geng, X.; Liu, S.L. Resurgence of scarlet fever in China: A 13-year population-based surveillance study. Lancet Infect. Dis. 2018, 18, 903–912. [Google Scholar] [CrossRef]
- Lu, Q.B.; Ding, Z.Y.; Wu, C.; Wu, H.C.; Lin, J.F. Analysis of Epidemiological Characteristics of Notifiable Diseases Reported in Children Aged 0–14 Years from 2008 to 2017 in Zhejiang Province, China. Int. J. Environ. Res. Public Health 2019, 16, 168. [Google Scholar] [CrossRef] [PubMed]
- Luk, E.Y.; Lo, J.Y.; Li, A.Z.; Lau, M.C.; Cheung, T.K.; Wong, A.Y.; Wong, M.M.; Wong, C.W.; Chuang, S.K.; Tsang, T. Scarlet fever epidemic, Hong Kong, 2011. Emerg. Infect. Dis. 2012, 18, 1658–1661. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Wang, Y.; Jin, S.; Wu, Z.; Chin, D.P.; Koplan, J.P.; Wilson, M.E. Emergence and control of infectious diseases in China. Lancet 2008, 372, 1598–1605. [Google Scholar] [CrossRef]
- Ministry of Health of the People’s Republic of China. Diagnostic Criteria for Scarlet Fever (WS 282-2008); Ministry of Health of the People’s Republic of China: Beijing, China, 2008.
- Getis, A.; Ord, J.K. The analysis of spatial association by use of distance statistics. Geogr. Anal. 1992, 24, 189–206. [Google Scholar] [CrossRef]
- Ord, J.K.; Getis, A. Local spatial autocorrelation statistics-distributional issues and an application. Geogr. Anal. 1995, 27, 286–306. [Google Scholar] [CrossRef]
- Mahara, G.; Wang, C.; Huo, D.; Xu, Q.; Huang, F.; Tao, L.; Guo, J.; Cao, K.; Long, L.; Chhetri, J.K.; et al. Spatiotemporal pattern analysis of scarlet fever incidence in Beijing, China, 2005–2014. Int. J. Environ. Res. Public Health 2016, 13, 131. [Google Scholar] [CrossRef]
- Kim, J.H.; Cheong, H.K. Increasing number of scarlet fever cases, South Korea, 2011–2016. Emerg. Infect. Dis. 2018, 24, 172–173. [Google Scholar] [CrossRef]
- Watts, V.; Balasegaram, S.; Brown, C.S.; Mathew, S.; Mearkle, R.; Ready, D.; Saliba, V.; Lamagni, T. Increased Risk for Invasive Group A Streptococcus Disease for Household Contacts of Scarlet Fever Cases, England, 2011–2016. Emerg. Infect. Dis. 2019, 25, 529–537. [Google Scholar] [CrossRef]
- Yun, C.F.; Thoon, K.C. A 12 year outbreak of scarlet fever in Singapore. Lancet Infect. Dis. 2018, 18, 942. [Google Scholar] [CrossRef] [Green Version]
- Zheng, Y.H.; Meng, L.; Ren, X.W.; Liu, D.P.; Li, J.S.; Liu, H.X.; Gou, F.X.; Liu, X.F. Spatial aggregation analysis on scarlet fever in Gansu Province, 2013. Chin. J. Dis. Control Prev. 2015, 19, 979–982. (In Chinese) [Google Scholar]
- Duan, Y.; Yang, L.J.; Zhang, Y.J.; Huang, X.L.; Pan, G.X.; Wang, J. Effects of meteorological factors on incidence of scarlet fever during different periods in different districts of China. Sci. Total Environ. 2017, 581–582, 19–24. [Google Scholar] [CrossRef] [PubMed]
- Mahara, G.; Wang, C.; Yang, K.; Chen, S.; Guo, J.; Gao, Q.; Wang, W.; Wang, Q.; Guo, X. The Association between Environmental Factors and Scarlet Fever Incidence in Beijing Region: Using GIS and Spatial Regression Models. Int. J. Environ. Res. Public Health 2016, 13, 1083. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.C.; Lin, J.F.; Xu, X.P.; Wu, C.; Lu, Q.B.; Ding, Z.Y. An analysis on the correlations between the scarlet fever and me teorological factors with generalized additive model. Zhejiang Prev. Med. 2016, 28, 5–8. (In Chinese) [Google Scholar]
- Yang, F.; Zhong, H.J.; Hong, T.; Zhang, J.Q.; Lin, W.Q. Incidence trendency and epidemiological characteristics of scarlet fever in Guangdong Province, 1950–2011. South China J. Prev. Med. 2013, 39, 1–5. (In Chinese) [Google Scholar]
- World Health Organization. Western Pacific Region. Scarlet Fever: Factsheet of Scarlet Fever in China. Available online: http://www.wpro.who.int/china/mediacentre/factsheets/scarlet_fever/en/ (accessed on 20 July 2019).
- Public Health England, United Kingdom. Scarlet Fever: Second Year of High Activity. Available online: https://www.gov.uk/government/news/scarlet-fever-second-year-of-high-activity (accessed on 20 July 2019).
- Duan, Y.; Huang, X.L.; Wang, Y.J.; Zhang, J.Q.; Zhang, Q.; Dang, Y.W.; Wang, J. Impact of meteorological changes on the incidence of scarlet fever in Hefei City, China. Int. J. Biometeorol. 2016, 60, 1543–1550. [Google Scholar] [CrossRef] [PubMed]
- Ma, T.; Hong, L.; Lin, D.; Feng, L.J.; Zhou, L.; Ma, H.L.; Zu, R.Q.; Xie, G.X. Epidemiological charateristics of scarlet fever in Nanjing during 2006–2015. Chin. J. Hyg. Rescue 2016, 2, 223–229. (In Chinese) [Google Scholar]
- Centers for Disease Control and Prevention (CDC). Scarlet Fever: Group A Streptococcal (GAS) Disease. Available online: https://www.cdc.gov/groupastrep/index.html (accessed on 20 July 2019).
- Wong, S.S.; Yuen, K.Y. Streptococcus pyogenes and re-emergence of scarlet fever as a public health problem. Emerg. Microbes Infect. 2012, 1, e2. [Google Scholar] [CrossRef]
- Lu, J.Y.; Chen, Z.Q.; Liu, Y.H.; Liu, W.H.; Ma, Y.; Li, T.G.; Zhang, Z.B.; Yang, Z.C. Effect of meteorological factors on scarlet fever incidence in Guangzhou City, Southern China, 2006–2017. Sci. Total Environ. 2019, 663, 227–235. [Google Scholar] [CrossRef]
- Kim, J.; Kim, J.E.; Bae, J.M. Incidence of Scarlet Fever in Children in Jeju Province, Korea, 2002–2016: An Age-period-cohort Analysis. J. Prev. Med. Public Health 2019, 52, 188–194. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | 2004 | 2005 | 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | Total |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Gender | ||||||||||||||||
| Male | 331 | 406 | 602 | 551 | 530 | 407 | 278 | 1239 | 1092 | 714 | 1127 | 2159 | 1486 | 1391 | 1402 | 13,715 |
| Female | 193 | 244 | 328 | 322 | 286 | 242 | 177 | 704 | 614 | 503 | 726 | 1331 | 987 | 917 | 905 | 8479 |
| Sex Ratio | 1.72 | 1.66 | 1.84 | 1.71 | 1.85 | 1.68 | 1.57 | 1.76 | 1.78 | 1.42 | 1.55 | 1.62 | 1.51 | 1.52 | 1.55 | 1.62 |
| Age | ||||||||||||||||
| 0–2 years | 35 | 35 | 64 | 51 | 72 | 54 | 68 | 136 | 95 | 85 | 126 | 194 | 158 | 106 | 131 | 1410 |
| 3–9 years | 413 | 531 | 757 | 712 | 652 | 505 | 355 | 1692 | 1473 | 1036 | 1621 | 3117 | 2189 | 2072 | 2054 | 19,179 |
| 10–14 years | 59 | 75 | 80 | 73 | 70 | 62 | 19 | 95 | 109 | 84 | 90 | 155 | 105 | 110 | 102 | 1288 |
| ≥15 years | 17 | 9 | 29 | 37 | 22 | 28 | 13 | 20 | 29 | 12 | 16 | 24 | 21 | 20 | 20 | 317 |
| Occupation | ||||||||||||||||
| Scattered children | 120 | 153 | 171 | 174 | 245 | 164 | 157 | 384 | 315 | 254 | 355 | 636 | 500 | 473 | 413 | 4514 |
| Kindergarten children | 184 | 256 | 403 | 352 | 289 | 255 | 165 | 875 | 753 | 509 | 808 | 1650 | 1153 | 962 | 949 | 9563 |
| Students | 209 | 236 | 334 | 324 | 272 | 213 | 125 | 659 | 613 | 444 | 679 | 1187 | 806 | 864 | 929 | 7894 |
| Others | 11 | 5 | 22 | 23 | 10 | 17 | 8 | 25 | 25 | 10 | 11 | 17 | 14 | 9 | 16 | 223 |
| Year | Area | Gi Z-Score | Gi p-Value | Cluster |
|---|---|---|---|---|
| 2004 | No significant areas | - | - | - |
| 2005 | Huzhou | 2.244472 | 0.024802 | Hotspot |
| 2005 | Hangzhou | 1.920238 | 0.054828 | Hotspot |
| 2006 | Zhoushan | 2.224427 | 0.02612 | Hotspot |
| 2007 | Lishui | −1.736641 | 0.08245 | Coldspot |
| 2008 | No significant areas | - | - | - |
| 2009 | Wenzhou | −2.105993 | 0.35205 | Coldspot |
| 2009 | Lishui | −2.565872 | 0.10292 | Coldspot |
| 2009 | Huzhou | 1.870962 | 0.06135 | Hotspot |
| 2010 | Jinhua | 1.995008 | 0.046042 | Hotspot |
| 2011 | Lishui | −1.664144 | 0.096084 | Coldspot |
| 2011 | Hangzhou | 1.881472 | 0.059908 | Hotspot |
| 2011 | Shaoxing | 2.012153 | 0.044204 | Hotspot |
| 2011 | Jinhua | 1.819235 | 0.068876 | Hotspot |
| 2012 | Hangzhou | 2.138269 | 0.032495 | Hotspot |
| 2012 | Jiaxing | 2.250799 | 0.024398 | Hotspot |
| 2012 | Huzhou | 1.967822 | 0.049088 | Hotspot |
| 2013 | Shaoxing | 2.2472 | 0.024627 | Hotspot |
| 2013 | Jiaxing | 2.107303 | 0.035091 | Hotspot |
| 2013 | Huzhou | 1.703672 | 0.088442 | Hotspot |
| 2014 | Shaoxing | 2.143372 | 0.032083 | Hotspot |
| 2014 | Jiaxing | 1.677282 | 0.093487 | Hotspot |
| 2014 | Huzhou | 1.910595 | 0.056057 | Hotspot |
| 2015 | Shaoxing | 2.455428 | 0.014072 | Hotspot |
| 2016 | Shaoxing | 2.181783 | 0.029126 | Hotspot |
| 2016 | Jiaxing | 1.657274 | 0.097464 | Hotspot |
| 2017 | Shaoxing | 2.083044 | 0.037247 | Hotspot |
| 2018 | Shaoxing | 1.929722 | 0.053641 | Hotspot |
| 2018 | Jiaxing | 1.775277 | 0.075852 | Hotspot |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lu, Q.; Wu, H.; Ding, Z.; Wu, C.; Lin, J. Analysis of Epidemiological Characteristics of Scarlet Fever in Zhejiang Province, China, 2004–2018. Int. J. Environ. Res. Public Health 2019, 16, 3454. https://doi.org/10.3390/ijerph16183454
Lu Q, Wu H, Ding Z, Wu C, Lin J. Analysis of Epidemiological Characteristics of Scarlet Fever in Zhejiang Province, China, 2004–2018. International Journal of Environmental Research and Public Health. 2019; 16(18):3454. https://doi.org/10.3390/ijerph16183454
Chicago/Turabian StyleLu, Qinbao, Haocheng Wu, Zheyuan Ding, Chen Wu, and Junfen Lin. 2019. "Analysis of Epidemiological Characteristics of Scarlet Fever in Zhejiang Province, China, 2004–2018" International Journal of Environmental Research and Public Health 16, no. 18: 3454. https://doi.org/10.3390/ijerph16183454