
Abstract
Dementia is more prevalent in Blacks than in Whites, likely due to a combination of environmental and biological factors. Paradoxically, clinical studies suggest an attenuation of APOE ε4 risk of dementia in African ancestry (AFR), but a dearth of neuropathological data preclude the interpretation of the biological factors underlying these findings, including the association between APOE ε4 risk and Alzheimer’s disease (AD) pathology, the most frequent cause of dementia. We investigated the interaction between African ancestry, AD-related neuropathology, APOE genotype, and functional cognition in a postmortem sample of 400 individuals with a range of AD pathology severity and lack of comorbid neuropathology from a cohort of community-dwelling, admixed Brazilians. Increasing proportions of African ancestry (AFR) correlated with a lower burden of neuritic plaques (NP). However, for individuals with a severe burden of NP and neurofibrillary tangles (NFT), AFR proportion was associated with worse Clinical Dementia Rating sum of boxes (CDR-SOB). Among APOE ε4 carriers, the association between AFR proportion and CDR-SOB disappeared. APOE local ancestry inference of a subset of 309 individuals revealed that, in APOE ε4 noncarriers, non-European APOE background correlated with lower NP burden and, also, worse cognitive outcomes than European APOE when adjusting by NP burden. Finally, APOE ε4 was associated with worse AD neuropathological burden only in a European APOE background. APOE genotype and its association with AD neuropathology and clinical pattern are highly influenced by ancestry, with AFR associated with lower NP burden and attenuated APOE ε4 risk compared to European ancestry.
Similar content being viewed by others

Introduction
Recent data from the USA suggest a prevalence of Alzheimer’s disease (AD)-type dementia (AD dementia) of 19% in non-Hispanic Blacks compared to 10% in non-Hispanic Whites, with Hispanics having a prevalence in between these estimates [1, 2]. A study from a large UK cohort also suggests that older Blacks have a higher prevalence of dementia than Whites [3]. Paradoxically, several studies suggest that apolipoprotein E ε4 allele (APOE4), considered the strongest genetic risk factor for late-onset AD, has a weaker effect in Blacks than in Whites [4, 5] or that the effect of APOE4 on AD risk is attenuated in African ancestry (AFR), especially when the APOE gene is on a local African ancestry [6,7,8]. Indeed, APOE4 allele frequency varies across populations, consistently more common in AFR than European ancestry (EUR) (12–21% vs. 6–14%, respectively) [9, 10]. Factors related to genetic ancestry architecture, specific traits, or disease-related genetic variants enriched in a particular population due to founder effects may provide biological explanations for these differences [11, 12]. However, pinpointing the biological impact of ancestry-related genetic architecture on AD risk has been challenging. Self-reporting race is a poor predictor of ancestry-related biological effects because social determinants of health influence it, i.e., environmental factors present where people live and work that impact disease risk [13,14,15,16,17,18]. Also, self-reported race is a qualitative metric, whereas genetic-based ancestry is quantitative, thus providing a better metric of admixture. More recent work in AD using genomic-based analysis of ancestry instead of self-reported race has advanced the field. However, the impact of most of this work is still limited by the lack of neuropathological confirmation [6, 19] since non-White individuals are still underrepresented in autopsy studies. Neuropathological examination is the gold standard to diagnose and score age-related neuropathological findings. Most aging individuals show multiple comorbid neuropathological changes that impact clinical outcomes. Unfortunately, antemortem diagnosis remains unavailable for most of these conditions, including TDP-43 proteinopathy, synucleinopathies, and aging-related tau astrogliopathies [20, 21]. This limitation hampers the ability to investigate ancestry-related biological differences, as opposed to differences due to social determinants of health, in AD risk or to determine whether the APOE4 risk in AD dementia is really attenuated in AFR or the lower risk of dementia is related to increased amounts of non-AD neuropathology in individuals with AFR. The latter is possible. In a previous study investigating ancestry-driven differences in risk of developing neuropathological changes commonly associated with dementia, we used a panel of ancestry-informative markers (AIMs) in a cohort of 202 autopsy cases of individuals dwelling in São Paulo, a highly admixed 12 million inhabitants city in Brazil. We found that subjects with higher proportions of AFR ancestry showed a lower prevalence of neuritic plaques (OR = 0.43, 95% CI = 0.21–0.89, p = 0.02) than individuals with EUR ancestry when adjusted for sociodemographic variables and APOE genotype. Conversely, other neuropathological alterations, such as AD-tau burden, Lewy body disease, or microvascular brain changes, showed similar prevalence among different ancestries [22].
To interrogate the correlation between proportion of AFR, AD neuropathology, clinical decline, and APOE4 risk, we have expanded our original clinicopathological cohort sixfold (1333 individuals over 50 years of age) to obtain the necessary power of analysis to investigate only cases showing evidence of AD-related neuropathological changes or a lack of neuropathological diagnosis (N = 400). We excluded individuals with other non-AD neuropathological changes to avoid confounders in the analysis. We interrogated whether the percentage of AFR correlates with functional cognitive scores in participants stratified by APOE4 status over equivalent AD-neuropathology burden. Finally, as disadvantaged social determinants of health are enriched in particular ancestry groups, biological and environmental contributions must be considered when interpreting results associated with global ancestry. To isolate a possible ancestry-related biological effect, we investigated the interaction between AD neuropathological burden, cognition, and AFR, stratifying individuals by their local ancestry within the APOE locus.
Methods
Participants
A full-body autopsy is mandatory in São Paulo city when an individual dies from undiagnosed non-traumatic death. This study, which was approved by the Internal Review Board of the University of São Paulo Medical School, included samples and data from the Biobank for Aging Studies (BAS) from the University of São Paulo Medical School (Brazil) that were collected between 2004 and 2017 [23, 24]. The BAS includes individuals who were 18 years and older at the time of death and with informants who had at least weekly contact with the deceased in the six months prior to death. Exclusion criteria for participating in the BAS cohort included inconsistent clinical data or brain tissue unsuitable for neuropathological analyses (cerebrospinal fluid pH <6.5 or acute brain lesions that required examination by the pathologist in charge for the cause of death certification). A detailed explanation of the BAS procedures can be found elsewhere [23].
Trained gerontologists perform clinical and functional assessments. After the informed consent had been signed, the most knowledgeable informant was interviewed to obtain the deceased’s clinical history using a semi-structured interview, which has shown good evidence of validity for detecting cognitive impairment by informants in postmortem settings [24, 25]. Cognitive impairment was assessed using the Clinical Dementia Rating Scale (CDR)—informant section [26]. We also used the Informant Questionnaire on Cognitive Decline in the Elderly (IQCODE) as an alternative measure of cognitive function [27].
For this study, we included participants either lacking neuropathological changes (normal controls) or those exclusively with evidence of AD-related neuropathological changes (plaques and/or neurofibrillary tangles). Therefore, individuals with non-AD neuropathological lesions i.e., any evidence of TDP-43 proteinopathy or synucleinopathy, primary tauopathy (except ARTAG and AGD, which are considered benign), or significant micro- or macrocerebrovascular pathology (criteria described in [23] and Supplementary Material) were excluded in addition to cases with incomplete clinical, neuropathological, and genetic data.
Genetic analyses and variables
APOE Dataset of genomic variants used in APOE local ancestry and coding genotypes associated with this project is available in the University of São Paulo Data Repository https://repositorio.uspdigital.usp.br/handle/item/377 DNA samples were obtained from blood or brain tissue and genotyped using Illumina OmniExpress 700k microarray or Illumina BeadXpress custom genotyping panel, as detailed in Supplementary Methods. APOE common alleles were preferably genotyped directly using allele-specific amplification [28] or after imputation of rs429358 to compose haplotypes (detailed in Supplementary Methods). Individuals were classified as either APOE4 carriers (at least one ε4 allele) or noncarriers, hereby defining the APOE4+ or APOE4− status, respectively. Global tri-hybrid continental ancestry was inferred using 47 ancestry informative markers (AIMs) with Structure 2.3.4 [29] using K = 3. The panel is a subset from a previously described panel [22], which combined HapMap, Human Genome Diversity Project (HGDP), and New York Cancer Project (NYCP) as parental populations that were used to calibrate our inference (see Supplementary Methods). Global ancestry was analyzed in two ways: dichotomously, using a 2% cutoff for AFR (first quartile of the AFR distribution) [22]; and as a continuous variable, in increments of 10% AFR proportions indicating the presence of the African component in admixed individuals.
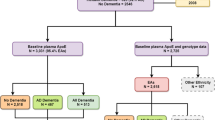
In the 309 individuals with available genotype microarray data, local ancestry inference (LAI) using large reference panels that included Brazilians and Brazilian parental populations were used to determine local ancestry of each APOE allele, as African, European, and Native American [30] (detailed in Supplementary Methods). For analysis involving local APOE ancestry, the 309 individuals were first classified into APOE4+ (at least one ε4 allele, n = 74, group A) and APOE4− (only ε3 and/or ε2 alleles, n = 235, group B). Given the predominance of European alleles, the APOE4+ group was further divided into four groups: European APOE4+ (group A1, n = 31, including homozygotes), mixed ancestry with one European APOE4+ and one non-European APOE4− allele (“Mixed APOE4+ 1” group A2, n = 3), mixed ancestry with one non-European APOE4+ and any European APOE4− allele (“Mixed APOE4+ 2” group A3, n = 23) and non-European APOE4+ (group A4, n = 17, including homozygotes). The APOE4− was further divided into three groups: European APOE4− (group B1, n = 138), mixed ancestry APOE4− (group B2, n = 73), and non-European APOE4− (group B3, n = 24). Figure 1 and Supplementary Table 1 provide all counts of individuals per APOE genotypes and local ancestries. Non-European was defined in the study as a combination of African and Native American ancestries, since the latter is rarer (Supplementary Table 2).

While groups A1, A4, B1, and B3 contain individuals with a single local ancestry at APOE locus, groups A2, A3, and B2 contain individuals with dual ancestry at the APOE locus (mixed). Group A has APOE4 carriers (APOE4+) and group B is composed of noncarriers (APOE4−). Local ancestries referred as EUR (European) and non-EUR (Non-European).
Neuropathological assessment
The BAS uses a 14-region immunohistochemistry panel to detect neurodegeneration using universally accepted criteria to stage and diagnose cases[23]. Neurofibrillary tangle (NFT) pathology was scored by Braak stage, encoded into four groups following the conventional categorization [31]: Braak stages 0, I/II, III/IV, and V/VI. β-amyloid plaque pathology was scored using Consortium to Establish a Registry for Alzheimer’s Disease (CERAD) for the density of neuritic plaques, scored as none, sparse, moderate, or frequent.
Postmortem interview
The clinical interview included information on age, sex, and reported race by the informant, the latest confirmed by the interviewer on a government-issued document with photo identification. The informant also reported on the deceased’s years of formal education.
Cognitive function was evaluated using the CDR scale, which is a five-point scale used to classify dementia severity in six domains: memory, orientation, judgment and problem solving, community affairs, home, hobbies, and personal care [26]. The CDR was designed to be applied to both the patient and the informant, but due to study design, only the informant part was used. As the study outcome, we used the CDR sum of boxes (CDR-SOB, range: 0–18).
Statistical analysis
We used descriptive statistics to examine the characteristics of the sample by AFR status, categorized into two groups defined by a cutoff of 2% of AFR. This cutoff was defined based on the AFR proportion present in 90% of Caucasian samples from the Human Genome Diversity and HapMap Projects in 2012 [22, 32]. We used independent groups Student’s t test for continuous variables and chi-squared or Fisher’s exact tests to describe categorical variables. Sociodemographic, cognitive, and neuropathology variables were also compared regarding AFR in individuals reported as Whites. Subsequent analysis classified individuals based on the proportion of AFR ancestry (measured as a continuous 10% increasing scale). We determined the association of AD-neuropathology burden (Braak stages and CERAD scores) with AFR using ordinal logistic regression models adjusted for age, sex, and education. We further adjusted this model for APOE4 status (APOE4+ vs. APOE4−). Variance inflation factor (VIF) values did not indicate multicollinearity between Braak stages and CERAD scores in our sample.
We investigated the association between AFR and cognition, independent of AD-neuropathology burden, using the CDR-SOB as a continuous outcome and linear regression models adjusted for Braak stages and CERAD scores. These models were adjusted for age, sex, education, and APOE4 status.
Next, we examined whether AFR was an effect modifier in the relationship between AD-neuropathology burden and CDR-SOB scores by creating interaction terms of AFR with Braak stages and CERAD scores. Moreover, for the interaction analyses, we performed sensitivity analyses considering AFR as a binary variable defined by the 2% cutoff. Since we hypothesized that APOE4 could modify the previous interactions, we tested the hypothesis of a triple interaction between AFR, AD-neuropathology, and APOE4. Further, we stratified the previous interaction analyses by APOE4 status.
Finally, we investigated the association between CDR-SOB and the local ancestry of APOE using linear regression models adjusted for age, sex, and education. As indicated in the tables, AD-neuropathology scores were used as outcomes or CDR-SOB covariates, and models were adjusted for AFR. Groups based on local APOE ancestry (Fig. 1) were used both in APOE4− individuals to test local ancestry effects (group B1 vs. B2 + B3; B1 vs. B3, see Results) and between APOE4+ vs. APOE4− individuals of the same local ancestry (groups A1 vs. B1 and A4 vs. B3, respectively, see Results) to test allele-specific effects for each context. We also tested the associations with cognitive function as the outcome using the IQCODE instead of the CDR-SOB to confirm our findings’ robustness. All analyses used Stata 15 (StataCorp, College Station, TX). The alpha level was set at 0.05, and all tests were two-tailed.
Results
Demographics
The analysis included 400 participants with a mean age of 72.0 ± 12.1 years old. 50% were women, the mean education attainment was 4.7 ± 3.9 years, and 27% of the participants had at least one APOE4 allele. Participants were reported as White (69%), Brown (18%), and Black (12%). Genomic-based ancestry analysis revealed that 75% of participants had ≥2% of AFR ancestry, a group that contains a significant proportion of White (65%), most Brown, and all Black individuals. Of note, few individuals had >80% AFR even among those reported as Black, highlighting the admixed composition of this cohort. In univariate analyses, the ≥2% AFR group had similar age and sex distribution but a lower educational level than the <2% AFR group (Table 1). The ≥2% AFR group had a greater proportion of individuals with a lower plaque burden. However, we detected no differences in CDR score close to death, APOE4 status, or neurofibrillary tangles burden between the two groups. (Table 1). Similar results were found when we repeated these analyses in individuals reported as Whites (Supplementary Table 1). The average AFR proportions within individuals with declared White, Brown, and Black ethnicity groups were 11%, 36%, and 61%, respectively, demonstrating a broad range of admixture across reported race/ethnicities (Supplementary Fig. 1 and Supplementary Table 2).
African ancestry and AD pathology
We replicated the analysis of our 2013 paper [22] in this larger cohort with 400 subjects with pure AD neuropathology or lacking significant neuropathological changes and obtained similar results (Supplementary Table 3). Participants with ≥2% AFR had lower CERAD scores than those with <2%AFR (OR = 0.58, 95% CI = 0.35; 0.96, p = 0.03). As before, Braak stage showed no association with an ancestry group.
African ancestry, AD pathology, and cognitive outcomes
Using this larger cohort, we obtained increased analysis power to interrogate whether the increasing proportion of AFR modifies the association between AD-neuropathology and cognitive abilities. We found no correlation between AFR and functional cognitive abilities (CDR-SOB and IQCODE as the outcomes) (Table 2 and Supplementary Table 4).
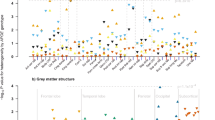
We found significant interactions between AFR and AD-neuropathology (p value for AFR interaction with CERAD = 0.007; and Braak = 0.002) (Fig. 2A, B, and Supplementary Table 5). This suggests that, among individuals with severe AD neuropathology, the higher the AFR proportion, the worse the CDR-SOB scores are, even after adjustment for age, sex, education, and APOE4 status. In sensitivity analysis, using AFR defined by the 2% cutoff, only the interaction between AFR and CERAD was significant (p = 0.005). The interaction between AFR and Braaak was no longer significant, possibly due to a lack of power (p = 0.13) (Supplementary Fig. 2).

Linear regression models of African ancestry and Clinical Dementia Rating Sum of Boxes (CDR-SOB) considering an interaction term between African ancestry and neuritic plaques evaluated by the CERAD score (A, C, E), or neurofibrillary tangle burden evaluated by the Braak & Braak stage (B, D, F). A neuritic plaque burden in all individuals [Black diamond: None or sparse (n = 303); Gray triangle: Moderate (n = 49); Black circle: Frequent (n = 48)]; (B) neurofibrillary tangle burden in all individuals [Black diamond: 0-II (n = 263); Gray triangle: III-IV (n = 99); Black circle: V-VI (n = 38)]; (C) neuritic plaques in APOE4− individuals [Black diamond: None or sparse plaques (n = 239); Gray triangle: Moderate plaques (n = 31); Black circle: Frequent plaques (n = 22)]; (D) neurofibrillary tangles in APOE4− individuals [Black diamond: Braak 0-II (n = 206); Gray triangle: Braak III-IV (n = 64); Black circle: Braak V-VI (n = 22)]; (E) neuritic plaques in APOE4+ individuals [Black diamond: None or sparse plaques (n = 64)]; Gray triangle: Moderate plaques (n = 18); Black circle: Frequent plaques (n = 26); and (F) neurofibrillary tangles in APOE4 + individuals [Black diamond: Braak 0-II (n = 57); Gray triangle: Braak III-IV (n = 35); Black circle: Braak V-VI (n = 16)]. P values for the interaction terms included in linear regression models adjusted for age, sex, education, and APOE4 status (A, B). Neuritic plaques were evaluated by the Consortium to Establish a Registry for Alzheimer’s disease (CERAD) score, and neurofibrillary tangles were evaluated by the Braak staining system.
To further examine the impact of APOE4 in the association between cognitive abilities and AD-pathology according to AFR proportion, we tested and found a significant triple interaction between AFR plus APOE4 status with CERAD score (p = 0.04), but not with Braak stages (p = 0.77). Thus, we stratified individuals by APOE4 status to interrogate, “Does the proportion of AFR impact the CDR-SOB scores independently of AD neuropathological burden as observed with the whole cohort without stratification?” Among APOE4− individuals, the results remained similar, meaning that the higher the AFR proportion, the worse the CDR-SB scores are in individuals with a higher burden of AD-neuropathology. However, the interactions lost significance in individuals APOE4+ (Fig. 2C–F). We found similar results when we used the IQCODE as the outcome, except for a loss of significance in the interaction between Braak scores and AFR in APOE4− (Supplementary Fig. 3).
Local APOE4 ancestry
It is essential to recognize the importance of disconnecting global and local genomic ancestries regarding effect sizes in admixed populations. To further investigate a possible biological role of European vs. non-European APOE alleles in AD-neuropathology scores and cognitive abilities (CDR-SOB), we re-run regressions in a subgroup of 309 individuals stratified by their APOE status (APOE4+ and APOE4−) and local ancestry (EUR vs. non-EUR), either adjusting or not for global ancestry (Fig. 1).
First, we tested the APOE4− group (Table 3) because we only observed worse CDR-SOB scores associated with a higher global AFR proportion in this group (Fig. 2C, D). Compared to individuals with local EUR APOE4- genotypes (homozygous for local ancestry), those with local non-EUR APOE4− genotypes had lower CERAD scores independent of the adjustment for global AFR (Table 3), in line with results obtained when considering global ancestry only. Despite the lower odds of accumulating neuritic plaques, the CDR-SOB scores were worse in the local non-EUR APOE4− groups when adjusting only for the CERAD scores, meaning that once plaques accumulate, the functional outcome seems to be worse in non-EUR APOE4− individuals (mixed plus non-EUR APOE4− alleles, see Fig. 1), exactly as observed in the global ancestry only analyses. This association lost statistical significance after correcting for global AFR proportion, although the trend remains (p = 0.059). Similar findings were found when we used the IQCODE as the cognitive outcome (Supplementary Table 6).
As we hypothesize that the APOE4 allele has an attenuated effect in non-EUR ancestry, we compared the effect magnitude in APOE4− vs. APOE4+ in individuals with local EUR in APOE separately from individuals with non-EUR APOE (see Fig. 1 groups). We excluded individuals with a mix of EUR and non-EUR APOE alleles for this analysis. Table 4A shows the results for individuals with EUR APOE (Table 4A, APOE4+ vs. APOE4−, Fig. 1 groups A1 vs. B1). As expected, EUR APOE4+ individuals had higher Braak stages than EUR APOE4−, even after adjusting for global ancestry; interestingly, the CDR-SOB scores were similar for both groups, even after adjusting for the burden of AD-pathology.
Next, we tested the local non-EUR APOE4+ individuals (Table 4B, Non-European APOE4+ vs. APOE4−, Fig. 1 groups A4 vs. B3). As opposed to individuals EUR at the APOE locus, we did not find associations of local ancestry with AD-pathology (nor with cognitive scores). Results did not change after adjustment for global ancestry. Results from Table 4 support the hypothesis that the effect of APOE4+ on neuropathological AD burden is attenuated in non-EURs when using corresponding local ancestry APOE4− individuals as references. We found similar results when we performed sensitivity analyses using the IQCODE as the cognitive outcome (Supplementary Table 7).
Discussion
Several studies point to race-based differences in risk and expression of dementia, likely due to a combined contribution of ancestry-based genetic factors and social determinants of health [1, 2]. Studies with comprehensive neuropathological and DNA-based ancestry assessments in large cohorts with admixed individuals have the potential to help disentangle the nature vs. nurture contributions to these differences. This study with 400 subjects who either lack neuropathological findings or had a broad range of AD neuropathological burden in the absence of other significant neuropathological changes drawn from an admixed cohort of 1,333 individuals showed that (1) AFR correlates with a lower burden of neuritic plaques, (2) among APOE4− individuals with a severe burden of neuritic plaques and tau neurofibrillary tangles, the higher the AFR proportion, the worse the functional cognitive scores, a difference that persists even upon stratification by local APOE ancestry, (3) among APOE4+ individuals with similar loads of AD pathology, functional cognitive scores are similar regardless of the AFR proportion, and (4) APOE4 carriers shows worse neuropathological and functional outcomes than noncarriers, but only in individuals with local EUR APOE and not in individuals with local non-EUR APOE.
These results validate and expand our previous study [22] that showed that AFR correlates with a lower burden of neuritic plaques even after adjusting for several factors, including APOE status. Furthermore, this study innovates by adding quantitative rather than discrete measures of AFR and providing a more in-depth analysis of the role of APOE in AFR. A finding of an interaction among AFR, CERAD scores for neuritic plaques, and APOE genotypes inspired us to interrogate whether APOE4 conferred a similar risk to individuals of AFR compared to EUR ancestry.
Among APOE4− individuals with a severe burden of neuritic plaques and neurofibrillary tangles, the higher the AFR proportion, the worse the functional cognitive scores. This observation mainly persisted upon stratification by local APOE ancestry after adjusting for neuritic plaques burden, independent of global ancestry status, even though the CERAD outcome continued to present the opposite effect (less severity in AFR). Paradoxically, we found no association between the proportion of AFR and AD metrics in the APOE4+ group. Further analysis comparing the magnitude effect of APOE4+ vs. APOE4− in neuropathological and functional outcomes in local EUR vs. non-EUR APOE groups showed a negative impact of APOE4+ (worse AD neuropathological metrics than in APOE4− individuals) in EUR only. These combined results corroborate the hypothesis of an attenuated effect of non-EUR APOE4+ in AD neuropathology.
The literature shows a higher prevalence of dementia in Blacks than in Whites [33], but most of these studies analyzed cohorts lacking neuropathological assessment and/or DNA-based ancestry determination. Thus, non-AD neuropathological changes, such as cerebrovascular changes, a known contributor to cognitive decline [34] and more prevalent in non-EUR [35], make it difficult to interrogate the relationship of risk factors to AD neuropathological changes. Our study suggests that a higher burden of AD neuropathology is not likely to explain this difference in cognitive scores. Moreover, since our cohort lacks noticeable non-AD neuropathological changes, it is also unlikely that comorbid neuropathological changes explain the differences in cognitive outcomes. Despite our best efforts to eliminate other confounders: using a cohort of individuals dwelling in the same city and adjusting the models for education, a proxy of social determinants of health, we cannot exclude that a combination of social factors contributed to a worse cognitive reserve in individuals with increasing AFR proportion, which is contributing for the worse cognitive scores [36,37,38]. A study from Cuba shows worse cognitive scores in individuals with a high AFR proportion only before adjusting for socioeconomic factors [39]. Although this study is not directly comparable to ours (no neuropathology assessment and dichotomous classification of AFR), it shows how social determinants of health enriched in specific populations may impact cognition. In addition to sociodemographic factors, APOE2 (ε2 allele) and APOE3 (ε3 allele) effects on cognition may differ across ancestries. APOE2 is generally considered to have a protective effect against AD in EUR ancestry, but less is known in non-EUR ancestry. Weaker APOE2 effect size was reported recently in non-EUR local ancestry context [8]. In a multi-racial cohort of New York City, APOE ε2/ε3 genotype was associated with an 8x increased risk of dementia of AD-type in African-Americans (self-declared race). However, it was associated with reduced risk in Whites [40]. Unfortunately, APOE genotypes ε2/ε2 and ε2/ε3 are less common genotypes, which challenges robust association studies due to sample size limitations, particularly in detailed neuropathology-based studies in population-representative samples such as ours. Further studies should investigate if a poor protective effect of APOE ε2 in non-EUR contributes to the worse functional cognitive scores in this group or if the ε3 allele itself has a different effect size in AFR (less protective).
The most intriguing observation of this study is the attenuation of the relationship between higher AFR proportion and worse CDR-SOB scores among APOE4+ and the attenuation of AD neuropathology burden in APOE4+ vs. APOE4− in individuals with non-EUR APOE background. Including local ancestry analysis is critical in admixed population studies because global ancestry is inferred, grouping a small number of ancestry-informative markers. Thus the local ancestry of a given gene may be different from the global ancestry estimates (i.e. EUR/EUR or EUR/non-EUR local ancestry in an individual with a predominant non-EUR global estimate and vice-versa).
The literature also suggests a possible biological attenuation of risk for AD-related cognitive decline among APOE4 carriers of AFR vs. EUR ancestry. In a comparison performed by Rajabli and colleagues [6] between African American and Puerto Rican AD cases and controls (no neuropathological confirmation for any group), APOE presented a differential effect based on AFR in admixed individuals. Although APOE4 is a significant risk allele for AD in both populations, odds ratio was 1.3–3.5-fold higher in EUR backgrounds [6]. Blue and colleagues showed that APOE2 and APOE4 had weaker effects (although in the same direction) in Caribbean Hispanics clinical AD (AD dementia, no neuropathological assessment) cohorts compared with a cohort of EUR with dementia of AD-type [8]. Notably, as expected, APOE4 homozygosity was the main contributor to the AD hazard ratio. Still, AFR local APOE decreased the hazard ratio by 28% [8]. Another study suggests a similar effect of APOE4 in AFR and EUR (global ancestry), but unfortunately, this study lacked neuropathological assessments [11].
Interestingly in the same study, the effect of APOE4 is attenuated in the subgroup of Dominicans, the closest in ancestry composition to our Brazilian cohort. Furthermore, a study from New York found that a higher risk of dementia among African Americans and Hispanics was not related to APOE4 [41]. Individuals with the APOE4 allele get an advantage in high-pathogen and energy-limited contexts by experiencing reduced innate inflammation and maintaining higher lipid levels [38, 42]. The proportion of APOE4 in cognitively normal AFR individuals is higher than in other populations [43]. Complex interactions between cognitive outcomes and cardiovascular phenotypes such as triglyceride levels [44], arterial thromboembolism, aneurism, and obesity [45] may contribute to attenuated APOE4 effect in individuals with AFR ancestral ancestry.
APOE4 mRNA expression levels are higher in EUR than in AFR allele [46], which could explain the larger effect-size. Interestingly, a recent single-cell expression study suggested that frontal cortex cells of AD patients significantly overexpress APOE4 in EUR local APOE ancestries than in AFR local ancestries [46]. This observation corroborates the previous findings and offers a local ancestry-specific APOE expression regulation hypothesis and favoring the existence of a polygenic modulation of APOE net penetrance that can be proxied by global ancestry in admixed individuals. A recent study on rare APOE missense variants modifying common e3 and e4 association signals raises the possibility that apoE4 protein has a different molecular function (i.e., misfunction) in different ancestries [47]. Moreover, for the interaction analyses Finally, haplotypic structure of population-specific rare and common variant combinations may underlie the attenuation of APOE4 deleterious effect in AFR. Indeed, relevant functional haplotypes may include neighboring genes such as TOMM40, also associated with AD [48], pointing that ancestry-specific effects from neighboring genes may be driving our findings [6]. Local ancestry was also significantly associated with known AD-related loci such as ABCA7 and CD33, and loci without previous association with AD such as CYP4B1, DAB1, MYSM1, and others, always controlling for APOE genotypes [49].
This study has several strengths, including a community-dwelling sample from an admixed population, neuropathological assessment, exclusion of individuals with non-AD neuropathological changes, DNA-based ancestry determination, and known APOE background. However, it is important to point out its limitations. Despite having one of the largest cliniconeuropathological series with admixed individuals, the number of individuals with APOE4+ genotypes is small, especially with a non-EUR background. Also, we run multiple tests. These factors increase the chances of error type I or II. Nevertheless, our results align with the literature on clinical samples. Also, we used semi-quantitative rather than quantitative neuropathological assessment and two different methods to input APOE genotype as the collection spans several years. However, quality control comparisons showed a similar result with any of the methods.
In conclusion, our work corroborates the need to increase the number of admixed populations in AD research. It suggests that neuropathology, clinical outcomes, and APOE genotyping differ with different ancestry backgrounds. The association between increased AFR proportion and worse functional cognitive scores was lost in APOE4 + , supporting the hypothesis that APOE4 risk in AD is attenuated in individuals with AFR ancestry compared to EUR ancestry.
References
Steenland K, Goldstein FC, Levey A, Wharton W. A meta-analysis of Alzheimer’s disease incidence and prevalence comparing African-Americans and Caucasians. J Alzheimers Dis. 2016;50:71–6.
Rajan KB, Weuve J, Barnes LL, McAninch EA, Wilson RS, Evans DA Population estimate of people with clinical Alzheimer’s disease and mild cognitive impairment in the United States (2020-2060). Alzheimers Dement. 2021;17:1966–75.
Pham TM, Petersen I, Walters K, Raine R, Manthorpe J, Mukadam N, et al. Trends in dementia diagnosis rates in UK ethnic groups: analysis of UK primary care data. Clin Epidemiol. 2018;10:949–60.
Murrell JR, Price B, Lane KA, Baiyewu O, Gureje O, Ogunniyi A, et al. Association of apolipoprotein E genotype and Alzheimer disease in African Americans. Arch Neurol. 2006;63:431–4.
Chin AL, Negash S, Hamilton R. Diversity and disparity in dementia: the impact of ethnoracial differences in Alzheimer disease. Alzheimer Dis Assoc Disord. 2011;25:187–95.
Rajabli F, Feliciano BE, Celis K, Hamilton-Nelson KL, Whitehead PL, Adams LD, et al. Ancestral origin of ApoE epsilon4 Alzheimer disease risk in Puerto Rican and African American populations. PLoS Genet. 2018;14:e1007791.
Farrer LA, Cupples LA, Haines JL, Hyman B, Kukull WA, Mayeux R, et al. Effects of age, sex, and ethnicity on the association between apolipoprotein E genotype and Alzheimer disease. A meta-analysis. APOE and Alzheimer Disease Meta Analysis Consortium. JAMA. 1997;278:1349–56.
Blue EE, Horimoto A, Mukherjee S, Wijsman EM, Thornton TA. Local ancestry at APOE modifies Alzheimer’s disease risk in Caribbean Hispanics. Alzheimers Dement. 2019;15:1524–32.
Phan L, Jin Y, Zhang H, Qiang W, Shekhtman E, Shao D, et al. ALFA: Allele Frequency Aggregator: National Center for Biotechnology Information, U.S. National Library of Medicine. 2020 www.ncbi.nlm.nih.gov/snp/docs/gsr/alfa/.
Abondio P, Sazzini M, Garagnani P, Boattini A, Monti D, Franceschi C, et al. The genetic variability of APOE in different human populations and its implications for longevity. Genes. 2019;10:222.
Granot-Hershkovitz E, Tarraf W, Kurniansyah N, Daviglus M, Isasi CR, Kaplan R, et al. APOE alleles’ association with cognitive function differs across Hispanic/Latino groups and genetic ancestry in the study of Latinos-investigation of neurocognitive aging (HCHS/SOL). Alzheimers Dement. 2021;17:466–74.
Marca-Ysabel MV, Rajabli F, Cornejo-Olivas M, Whitehead PG, Hofmann NK, Illanes Manrique MZ, et al. Dissecting the role of Amerindian genetic ancestry and the ApoE epsilon4 allele on Alzheimer disease in an admixed Peruvian population. Neurobiol Aging. 2021;101:e11–e15.
Yaffe K, Falvey C, Harris TB, Newman A, Satterfield S, Koster A, et al. Effect of socioeconomic disparities on incidence of dementia among biracial older adults: prospective study. BMJ 2013;347:f7051.
Tang MX, Cross P, Andrews H, Jacobs DM, Small S, Bell K, et al. Incidence of AD in African-Americans, Caribbean Hispanics, and Caucasians in northern Manhattan. Neurology. 2001;56:49–56.
Perkins P, Annegers JF, Doody RS, Cooke N, Aday L, Vernon SW. Incidence and prevalence of dementia in a multiethnic cohort of municipal retirees. Neurology. 1997;49:44–50.
Peterson RL, George KM, Gilsanz P, Ackley S, Mayeda ER, Glymour MM, et al. Racial/Ethnic Disparities in Young Adulthood and Midlife Cardiovascular Risk Factors and Late-life Cognitive Domains: The Kaiser Healthy Aging and Diverse Life Experiences (KHANDLE) Study. Alzheimer Dis Assoc Disord. 2021;35:99–105.
Babulal GM, Quiroz YT, Albensi BC, Arenaza-Urquijo E, Astell AJ, Babiloni C, et al. Perspectives on ethnic and racial disparities in Alzheimer’s disease and related dementias: Update and areas of immediate need. Alzheimers Dement. 2019;15:292–312.
Levine DA, Gross AL, Briceno EM, Tilton N, Kabeto MU, Hingtgen SM, et al. Association between blood pressure and later-life cognition among black and white individuals. JAMA Neurol. 2020;77:810–9.
Kunkle BW, Schmidt M, Klein HU, Naj AC, Hamilton-Nelson KL, Larson EB, et al. Novel Alzheimer Disease Risk Loci and Pathways in African American Individuals Using the African Genome Resources Panel: A Meta-analysis. JAMA Neurol. 2021;78:102–13.
Suemoto CK, Leite REP, Ferretti-Rebustini REL, Rodriguez RD, Nitrini R, Pasqualucci CA, et al. Neuropathological lesions in the very old: results from a large Brazilian autopsy study. Brain Pathol. 2019;29:771–81.
Karanth S, Nelson PT, Katsumata Y, Kryscio RJ, Schmitt FA, Fardo DW, et al. Prevalence and Clinical Phenotype of Quadruple Misfolded Proteins in Older Adults. JAMA Neurol. 2020;77:1299–307.
Schlesinger D, Grinberg LT, Alba JG, Naslavsky MS, Licinio L, Farfel JM, et al. African ancestry protects against Alzheimer’s disease-related neuropathology. Mol Psychiatry. 2013;18:79–85.
Suemoto CK, Ferretti-Rebustini RE, Rodriguez RD, Leite RE, Soterio L, Brucki SM, et al. Neuropathological diagnoses and clinical correlates in older adults in Brazil: A cross-sectional study. PLoS Med. 2017;14:e1002267.
Ferretti REL, Damin AE, Brucki SMD, Morillo LS, Perroco TR, Campora F, et al. Post-Mortem diagnosis of dementia by informant interview. Dement Neuropsychol. 2010;4:138–44.
Ferretti-Rebustini REL, Grinberg LT, Rebustini F, Suemoto CK, Leite REP, rodriguez RD, et al. Construct validity of the Clinical Dementia Rating Scale to assess the level of cognitive decline by informants. Alzheimer’s Dement [Internet]. 2021;17:e053956.
Morris JC. The Clinical Dementia Rating (CDR): current version and scoring rules. Neurology 1993;43:2412–4.
Jorm AF. The Informant Questionnaire on cognitive decline in the elderly (IQCODE): a review. Int Psychogeriatr. 2004;16:275–93.
Calero O, Hortiguela R, Bullido MJ, Calero M. Apolipoprotein E genotyping method by real time PCR, a fast and cost-effective alternative to the TaqMan and FRET assays. J Neurosci Methods. 2009;183:238–40.
Falush D, Stephens M, Pritchard JK. Inference of population structure using multilocus genotype data: dominant markers and null alleles. Mol Ecol Notes. 2007;7:574–8.
Borda V, Alvim I, Mendes M, Silva-Carvalho C, Soares-Souza GB, Leal TP, et al. The genetic structure and adaptation of Andean highlanders and Amazonians are influenced by the interplay between geography and culture. Proc Natl Acad Sci USA 2020;117:32557–65.
Braak H, Braak E. Neuropathological stageing of Alzheimer-related changes. Acta Neuropathologica. 1991;82:239–59.
International HapMap C. The International HapMap Project. Nature 2003;426:789–96.
Moon H, Badana ANS, Hwang SY, Sears JS, Haley WE. Dementia Prevalence in Older Adults: Variation by Race/Ethnicity and Immigrant Status. Am J Geriatr Psychiatry. 2019;27:241–50.
Kapasi A, DeCarli C, Schneider JA. Impact of multiple pathologies on the threshold for clinically overt dementia. Acta Neuropathol. 2017;134:171–86.
Sacco RL, Boden-Albala B, Gan R, Chen X, Kargman DE, Shea S, et al. Stroke incidence among white, black, and Hispanic residents of an urban community: the Northern Manhattan Stroke Study. Am J Epidemiol. 1998;147:259–68.
Borrell LN, Elhawary JR, Fuentes-Afflick E, Witonsky J, Bhakta N, Wu AHB, et al. Race and Genetic Ancestry in Medicine - A Time for Reckoning with Racism. N. Engl J Med. 2021;384:474–80.
Hollister BM, Farber-Eger E, Aldrich MC, Crawford DC. A Social Determinant of Health May Modify Genetic Associations for Blood Pressure: Evidence From a SNP by Education Interaction in an African American Population. Front Genet. 2019;10:428.
Yassine HN, Finch CE. APOE alleles and diet in brain aging and Alzheimer’s disease. Front Aging Neurosci. 2020;12:150.
Llibre-Guerra JJ, Li Y, Allen IE, Llibre-Guerra JC, Rodriguez Salgado AM, Penalver AI, et al. Race, genetic admixture and cognitive performance in the Cuban population. J Gerontol A Biol Sci Med Sci. 2021;77:331–8.
Maestre G, Ottman R, Stern Y, Gurland B, Chun M, Tang MX, et al. Apolipoprotein E and Alzheimer’s disease: ethnic variation in genotypic risks. ANNALSOF NEUROLOGY. 1995;37:254–9.
Tang MX, Stern Y, Marder K, Bell K, Gurland B, Lantigua R, et al. The APOE-epsilon4 allele and the risk of Alzheimer disease among African Americans, whites, and Hispanics. JAMA. 1998;279:751–5.
Garcia AR, Finch C, Gatz M, Kraft T, Eid Rodriguez D, Cummings D, et al. APOE4 is associated with elevated blood lipids and lower levels of innate immune biomarkers in a tropical Amerindian subsistence population. Elife. 2021;10:e68231.
Wang YY, Ge YJ, Tan CC, Cao XP, Tan L, Xu W. The proportion of APOE4 carriers among non-demented individuals: a pooled analysis of 389,000 community-dwellers. J Alzheimers Dis. 2021;81:1331–9.
Kuo CL, Pilling LC, Atkins JL, Kuchel GA, Melzer D. ApoE e2 and aging-related outcomes in 379,000 UK Biobank participants. Aging (Albany NY). 2020;12:12222–33.
Lumsden AL, Mulugeta A, Zhou A, Hypponen E. Apolipoprotein E (APOE) genotype-associated disease risks: a phenome-wide, registry-based, case-control study utilising the UK Biobank. EBioMedicine. 2020;59:102954.
Griswold AJ, Celis K, Bussies PL, Rajabli F, Whitehead PL, Hamilton-Nelson KL, et al. Increased APOE epsilon4 expression is associated with the difference in Alzheimer’s disease risk from diverse ancestral backgrounds. Alzheimers Dement. 2021;17:1179–88.
Le Guen Y, Belloy ME, Grenier-Boley B, de Rojas I, Castillo-Morales A, Jansen I, et al. Association of Rare APOE Missense Variants V236E and R251G With Risk of Alzheimer Disease. JAMA Neurol. 2022;79:652–63.
Roses AD, Lutz MW, Saunders AM, Goldgaber D, Saul R, Sundseth SS, et al. African-American TOMM40'523-APOE haplotypes are admixture of West African and Caucasian alleles. Alzheimers Dement. 2014;10:592–601.e2.
Hohman TJ, Cooke-Bailey JN, Reitz C, Jun G, Naj A, Beecham GW, et al. Global and local ancestry in African-Americans: Implications for Alzheimer’s disease risk. Alzheimers Dement. 2016;12:233–43.
Acknowledgements
We are grateful to the families who donated brains to the Biobank of Aging Studies of the University of Sao Paulo and the Sao Paulo Autopsy Service for the partnership. This work received funding from Sao Paulo Research Foundation (grant numbers 06/55318-1, 09/09134-4, 13/08028-1, 14/50931-3 16/24326-0; 18/16626-0) Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq) (466763/2014-0, 465355/2014-5, 403502/2020-9), Alzheimer Association and National Institute of Health (K24AG053435), FAPEMIG (00314-16). Part of the genetic data was generated with funds from NIH R01AG17917.
Author information
Authors and Affiliations
Contributions
MSN and CKS were equal first authors. Concept and design: MSN, CKS, MZ, LTG. Acquisition, analysis, or interpretation of data: MSN, CKS, LAB, MOS, REFR, RDR, REPL, NMA, VB, ETS, WJF, CAP, RN, KY, MZ, LTG. Drafting of the manuscript: MSN, CKS, LTG. Critical revision of the manuscript for important intellectual content: LAB, MOS, REFR, RDR, REPL, NMA, VB, ETS, WJF, CAP, RN, KY, MZ. Statistical analysis: MSN, CKS. Obtained funding: WJF, CAP, RN, MZ, LTG. Supervision: MZ, LTG.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Naslavsky, M.S., Suemoto, C.K., Brito, L.A. et al. Global and local ancestry modulate APOE association with Alzheimer’s neuropathology and cognitive outcomes in an admixed sample. Mol Psychiatry 27, 4800–4808 (2022). https://doi.org/10.1038/s41380-022-01729-x
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41380-022-01729-x
This article is cited by
-
Is Alzheimer disease a disease?
Nature Reviews Neurology (2024)
-
Association between APOE-ε4 allele and cognitive function is mediated by Alzheimer’s disease pathology: a population-based autopsy study in an admixed sample
Acta Neuropathologica Communications (2023)
-
Plasma apolipoprotein E levels, isoform composition, and dimer profile in relation to plasma lipids in racially diverse patients with Alzheimer’s disease and mild cognitive impairment
Alzheimer's Research & Therapy (2023)
-
Alzheimer’s drug trials plagued by lack of racial diversity
Nature (2023)
-
Causal effects on complex traits are similar for common variants across segments of different continental ancestries within admixed individuals
Nature Genetics (2023)
