Repeated Freezing Procedures Preserve Structural and Functional Properties of Amniotic Membrane for Application in Ophthalmology

 , ,
, , 

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Results
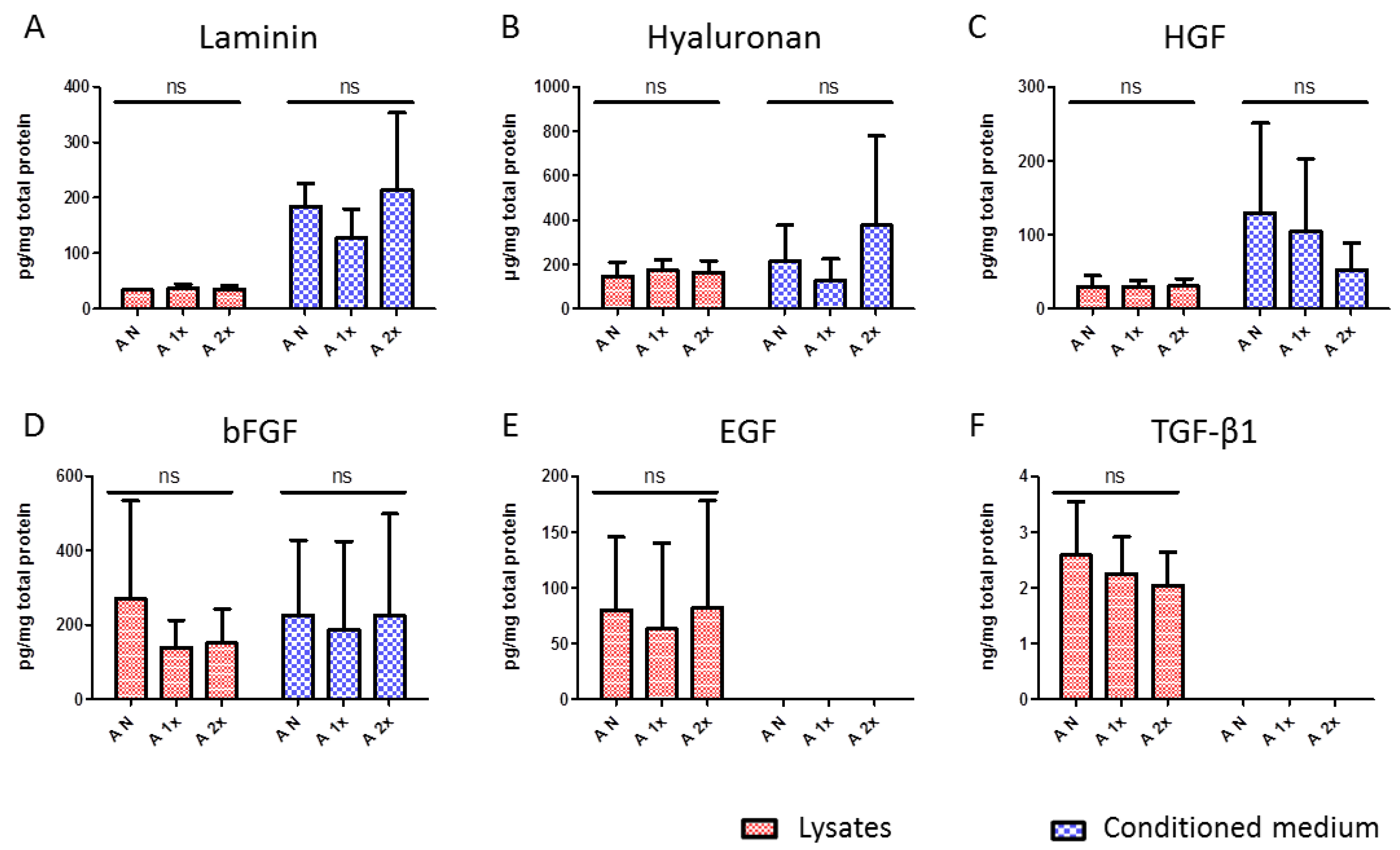
2.1. Evaluation of Content and Release Potential of Growth Factors and Extracellular Matrix Proteins of hAM
2.2. Evaluation of Morphological and Ultrastructural Changes in hAM after Multiple Freeze–Thaw Cycles
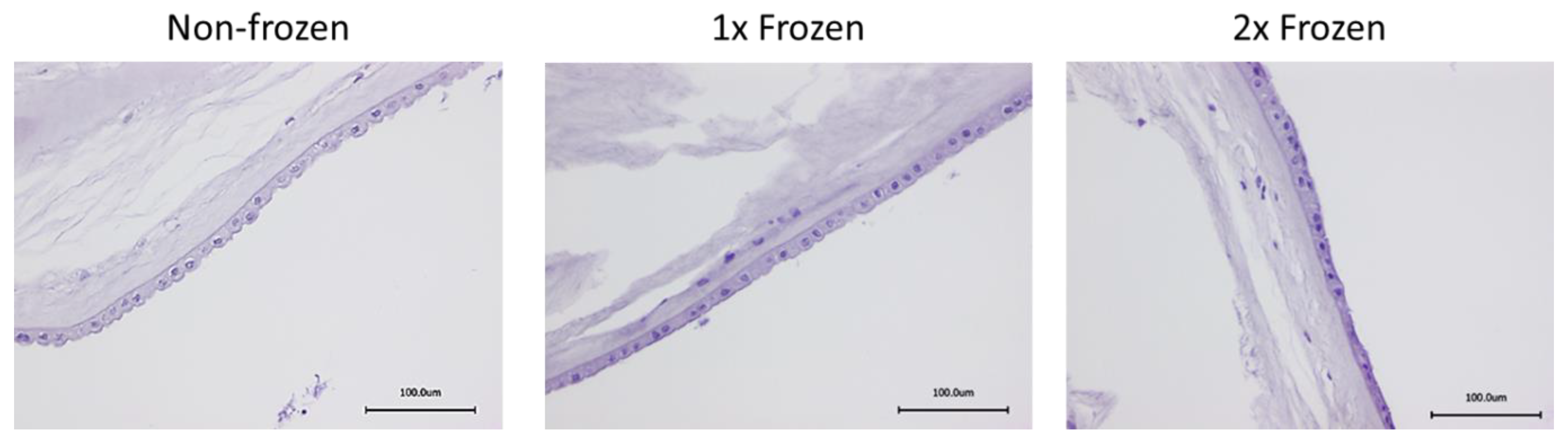
2.2.1. Histological Assessment of hAM Morphology with HE Staining
2.2.2. Analysis of Ultrastructure of hAM with SEM
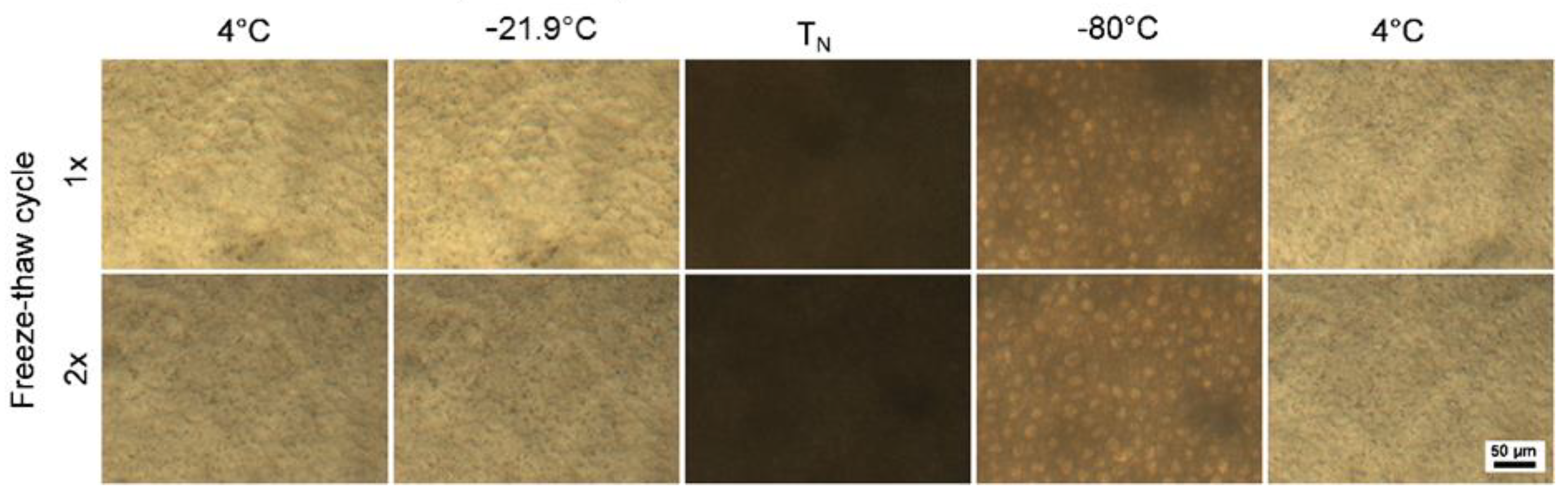
2.2.3. Cryomicroscopic Analysis of hAM Behavior at Subzero Temperatures
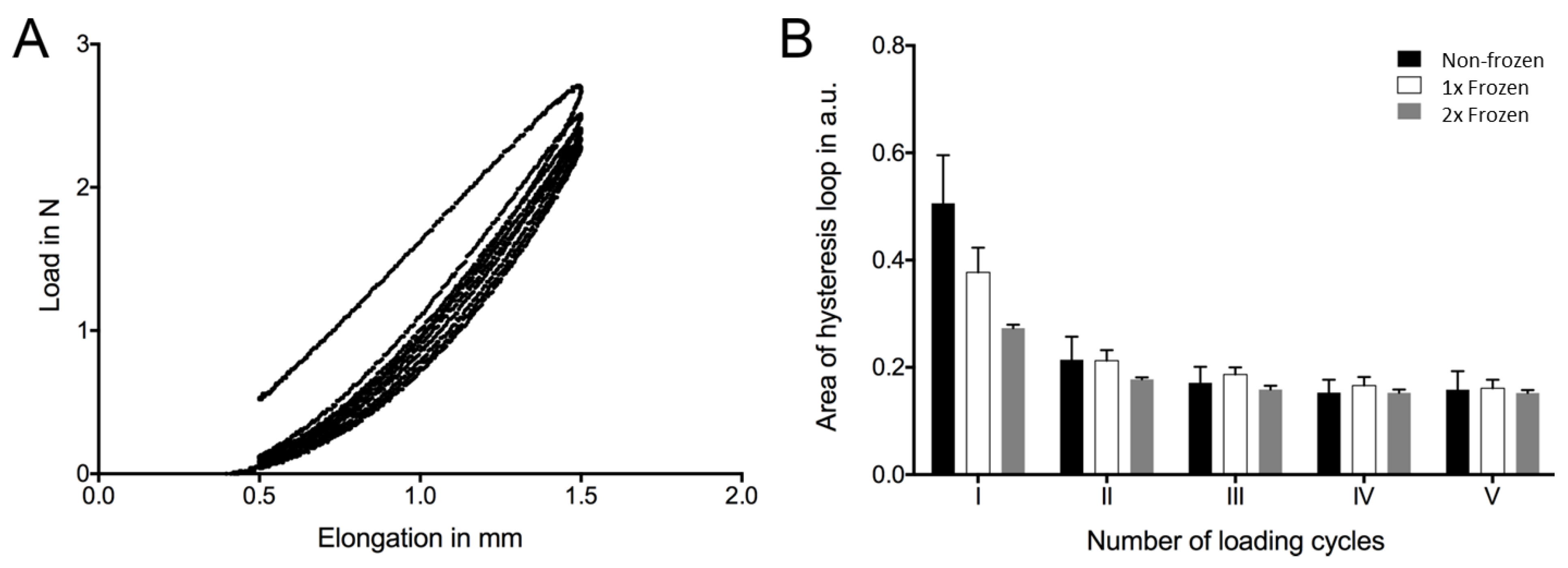
2.3. Assessment of Mechanical Properties of hAM
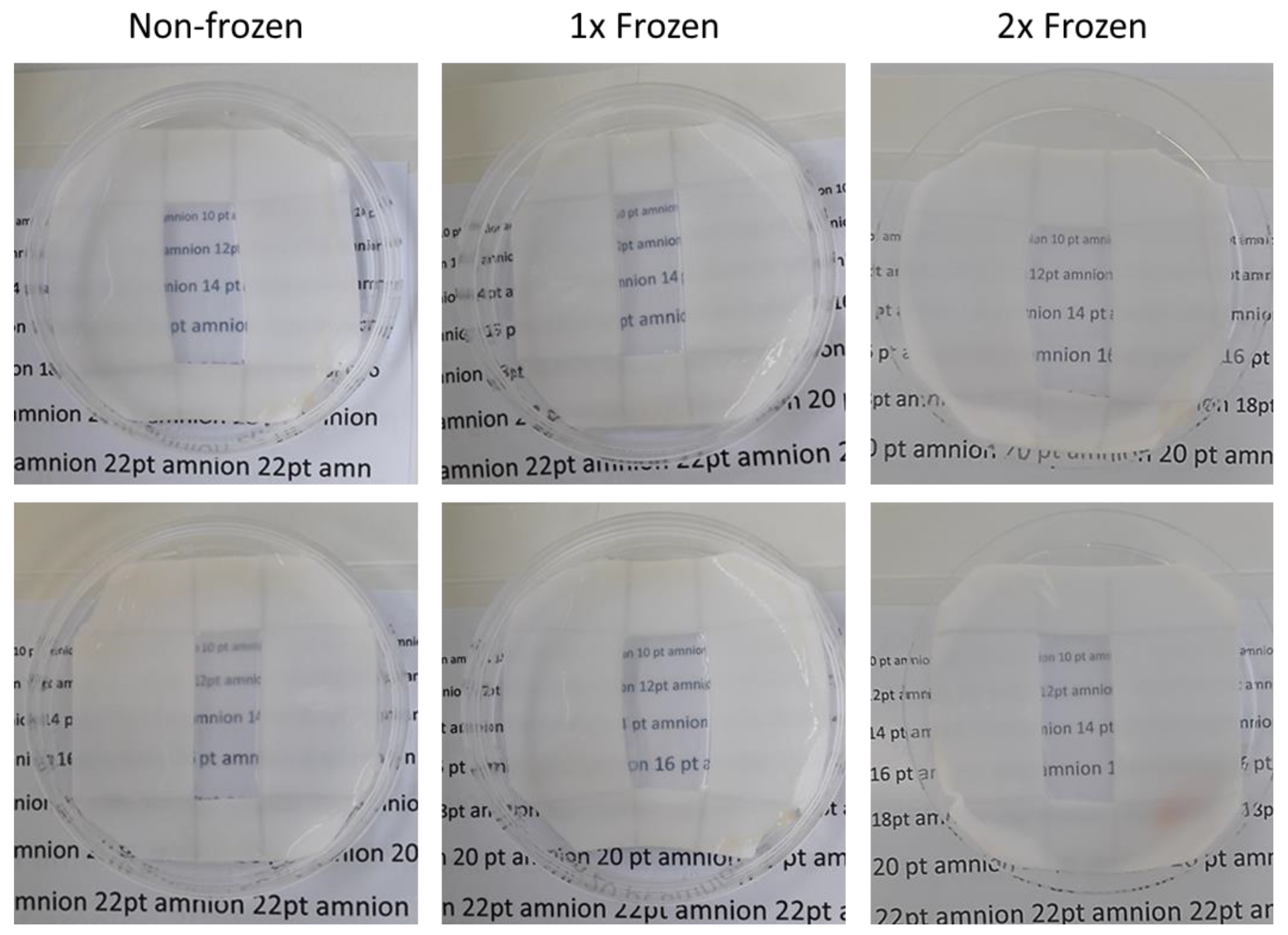
2.4. Transparency
3. Discussion
4. Materials and Methods
4.1. Experimental Design
4.2. Amniotic Membrane Preparation
4.3. Growth Factors and Extracellular Matrix Components Assessment
4.4. Morphological Evaluation
4.5. Cryomicroscopy
4.6. Scanning Electron Microscopy
4.7. Mechanical Test
4.8. Transparency Test
4.9. Data Analysis and Statistics
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Jirsova, K.; Jones, G.L. Amniotic membrane in ophthalmology: Properties, preparation, storage and indications for grafting-a review. Cell Tissue Bank 2017, 18, 193–204. [Google Scholar] [CrossRef] [PubMed]
- Kotomin, I.; Valtink, M.; Hofmann, K.; Frenzel, A.; Morawietz, H.; Werner, C.; Funk, R.H.; Engelmann, K. Sutureless fixation of amniotic membrane for therapy of ocular surface disorders. PLoS ONE 2015, 10, e0125035. [Google Scholar] [CrossRef] [PubMed]
- Le, Q.; Deng, S.X. The application of human amniotic membrane in the surgical management of limbal stem cell deficiency. Ocul. Surf. 2019, 17, 221–229. [Google Scholar] [CrossRef] [PubMed]
- Malhotra, C.; Jain, A.K. Human amniotic membrane transplantation: Different modalities of its use in ophthalmology. World J. Transpl. 2014, 4, 111–121. [Google Scholar] [CrossRef]
- Murube, J. Early clinical use of amniotic membrane in medicine and ophthalmology. Ocul. Surf. 2006, 4, 114–118. [Google Scholar] [CrossRef]
- Paolin, A.; Cogliati, E.; Trojan, D.; Griffoni, C.; Grassetto, A.; Elbadawy, H.M.; Ponzin, D. Amniotic membranes in ophthalmology: Long term data on transplantation outcomes. Cell Tissue Bank 2016, 17, 51–58. [Google Scholar] [CrossRef] [Green Version]
- Sharma, N.; Lathi, S.S.; Sehra, S.V.; Agarwal, T.; Sinha, R.; Titiyal, J.S.; Velpandian, T.; Tandon, R.; Vajpayee, R.B. Comparison of umbilical cord serum and amniotic membrane transplantation in acute ocular chemical burns. Br. J. Ophthalmol. 2015, 99, 669–673. [Google Scholar] [CrossRef] [Green Version]
- Silini, A.R.; Cargnoni, A.; Magatti, M.; Pianta, S.; Parolini, O. The Long Path of Human Placenta, and Its Derivatives, in Regenerative Medicine. Front. Bioeng. Biotechnol. 2015, 3, 162. [Google Scholar] [CrossRef]
- Pogozhykh, O.; Prokopyuk, V.; Figueiredo, C.; Pogozhykh, D. Placenta and Placental Derivatives in Regenerative Therapies: Experimental Studies, History, and Prospects. Stem Cells Int. 2018, 2018, 4837930. [Google Scholar] [CrossRef]
- Pogozhykh, O.; Prokopyuk, V.; Prokopyuk, O.; Kuleshova, L.; Goltsev, A.; Figueiredo, C.; Pogozhykh, D. Towards biobanking technologies for natural and bioengineered multicellular placental constructs. Biomaterials 2018, 185, 39–50. [Google Scholar] [CrossRef]
- Vladimir Petrovich Filatov; 1875–1956. Br. J. Ophthalmol. 1957, 41, 63–64.
- Aberasturis Cabrera, L. Local treatment of burns with placental extracts; technic of application of placental extract prepared by Filatov’s method in burns, original technic. Arch. Med. Infant 1954, 23, 123–144. [Google Scholar] [PubMed]
- Brand, I. The effect of Filatov’s placental extract on ocular tension. Klin. Monbl. Augenheilkd. Augenarztl. Fortbild. 1951, 119, 47–55. [Google Scholar] [PubMed]
- Davis, J.W. Skin transplantation with a review of 550 cases at the Johns Hopkins Hospital. Johns Hopkins Med. J. Hosp. Rep. 1910, 15, 307–396. [Google Scholar]
- Shaw, K.A.; Parada, S.A.; Gloystein, D.M.; Devine, J.G. The Science and Clinical Applications of Placental Tissues in Spine Surgery. Glob. Spine J. 2018, 8, 629–637. [Google Scholar] [CrossRef]
- Yoshizawa, R.S. Review: Public perspectives on the utilization of human placentas in scientific research and medicine. Placenta 2013, 34, 9–13. [Google Scholar] [CrossRef]
- Uhlig, C.E.; Frings, C.; Rohloff, N.; Harmsen-Aasman, C.; Schmitz, R.; Kiesel, L.; Eter, N.; Busse, H.; Alex, A.F. Long-term efficacy of glycerine-processed amniotic membrane transplantation in patients with corneal ulcer. Acta Ophthalmol. 2015, 93, e481–e487. [Google Scholar] [CrossRef] [Green Version]
- Chen, S.Y.; Han, B.; Zhu, Y.T.; Mahabole, M.; Huang, J.; Beebe, D.C.; Tseng, S.C. HC-HA/PTX3 Purified From Amniotic Membrane Promotes BMP Signaling in Limbal Niche Cells to Maintain Quiescence of Limbal Epithelial Progenitor/Stem Cells. Stem Cells 2015, 33, 3341–3355. [Google Scholar] [CrossRef]
- Riboh, J.C.; Saltzman, B.M.; Yanke, A.B.; Cole, B.J. Human Amniotic Membrane-Derived Products in Sports Medicine: Basic Science, Early Results, and Potential Clinical Applications. Am. J. Sports Med. 2016, 44, 2425–2434. [Google Scholar] [CrossRef]
- Champliaud, M.F.; Lunstrum, G.P.; Rousselle, P.; Nishiyama, T.; Keene, D.R.; Burgeson, R.E. Human amnion contains a novel laminin variant, laminin 7, which like laminin 6, covalently associates with laminin 5 to promote stable epithelial-stromal attachment. J. Cell Biol. 1996, 132, 1189–1198. [Google Scholar] [CrossRef]
- Koizumi, N.J.; Inatomi, T.J.; Sotozono, C.J.; Fullwood, N.J.; Quantock, A.J.; Kinoshita, S. Growth factor mRNA and protein in preserved human amniotic membrane. Curr. Eye Res. 2000, 20, 173–177. [Google Scholar] [CrossRef]
- Iorio, V.; Troughton, L.D.; Hamill, K.J. Laminins: Roles and Utility in Wound Repair. Adv. Wound Care (New Rochelle) 2015, 4, 250–263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akle, C.A.; Adinolfi, M.; Welsh, K.I.; Leibowitz, S.; McColl, I. Immunogenicity of human amniotic epithelial cells after transplantation into volunteers. Lancet 1981, 2, 1003–1005. [Google Scholar] [CrossRef]
- Adinolfi, M.; Akle, C.A.; McColl, I.; Fensom, A.H.; Tansley, L.; Connolly, P.; Hsi, B.L.; Faulk, W.P.; Travers, P.; Bodmer, W.F. Expression of HLA antigens, beta 2-microglobulin and enzymes by human amniotic epithelial cells. Nature 1982, 295, 325–327. [Google Scholar] [CrossRef]
- Meller, D.; Pauklin, M.; Thomasen, H.; Westekemper, H.; Steuhl, K.P. Amniotic membrane transplantation in the human eye. Dtsch. Arztebl. Int. 2011, 108, 243–248. [Google Scholar] [CrossRef] [PubMed]
- Lan, A.; Xiao, F.; Wang, Y.; Luo, Z.; Cao, Q. Efficacy of fibrin glue versus sutures for attaching conjunctival autografts in pterygium surgery: A systematic review with meta-analysis and trial sequential analysis of evidence. Oncotarget 2017, 8, 41487–41497. [Google Scholar] [CrossRef] [PubMed]
- Panda, A.; Kumar, S.; Kumar, A.; Bansal, R.; Bhartiya, S. Fibrin glue in ophthalmology. Indian J. Ophthalmol. 2009, 57, 371–379. [Google Scholar] [CrossRef]
- Romano, V.; Cruciani, M.; Conti, L.; Fontana, L. Fibrin glue versus sutures for conjunctival autografting in primary pterygium surgery. Cochrane Database Syst. Rev. 2016, 12, CD011308. [Google Scholar] [CrossRef]
- Byun, Y.S.; Kim, M.S. Superimposed fungal ulcer after fibrin glue sealant in infectious corneal ulcer. Korean J. Ophthalmol. 2011, 25, 447–450. [Google Scholar] [CrossRef] [Green Version]
- Riau, A.K.; Beuerman, R.W.; Lim, L.S.; Mehta, J.S. Preservation, sterilization and de-epithelialization of human amniotic membrane for use in ocular surface reconstruction. Biomaterials 2010, 31, 216–225. [Google Scholar] [CrossRef]
- Nakamura, T.; Sekiyama, E.; Takaoka, M.; Bentley, A.J.; Yokoi, N.; Fullwood, N.J.; Kinoshita, S. The use of trehalose-treated freeze-dried amniotic membrane for ocular surface reconstruction. Biomaterials 2008, 29, 3729–3737. [Google Scholar] [CrossRef]
- Tyszkiewicz, J.T.; Uhrynowska-Tyszkiewicz, I.A.; Kaminski, A.; Dziedzic-Goclawska, A. Amnion allografts prepared in the Central Tissue Bank in Warsaw. Ann. Transpl. 1999, 4, 85–90. [Google Scholar]
- Paolin, A.; Trojan, D.; Leonardi, A.; Mellone, S.; Volpe, A.; Orlandi, A.; Cogliati, E. Cytokine expression and ultrastructural alterations in fresh-frozen, freeze-dried and gamma-irradiated human amniotic membranes. Cell Tissue Bank 2016, 17, 399–406. [Google Scholar] [CrossRef]
- Cooke, M.; Tan, E.K.; Mandrycky, C.; He, H.; O’Connell, J.; Tseng, S.C. Comparison of cryopreserved amniotic membrane and umbilical cord tissue with dehydrated amniotic membrane/chorion tissue. J. Wound Care 2014, 23, 465–474, 476. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mahdy, R.A.; Nada, W.M.; Almasalamy, S.M.; Anany, H.A.; Almasary, A.M. A freeze-dried (lyophilized) amniotic membrane transplantation with mitomycin C and trabeculectomy for pediatric glaucoma. Cutan Ocul. Toxicol. 2010, 29, 164–170. [Google Scholar] [CrossRef] [PubMed]
- Allen, C.L.; Clare, G.; Stewart, E.A.; Branch, M.J.; McIntosh, O.D.; Dadhwal, M.; Dua, H.S.; Hopkinson, A. Augmented dried versus cryopreserved amniotic membrane as an ocular surface dressing. PLoS ONE 2013, 8, e78441. [Google Scholar] [CrossRef] [Green Version]
- Russo, A.; Bonci, P.; Bonci, P. The effects of different preservation processes on the total protein and growth factor content in a new biological product developed from human amniotic membrane. Cell Tissue Bank 2012, 13, 353–361. [Google Scholar] [CrossRef] [PubMed]
- Thomasen, H.; Pauklin, M.; Steuhl, K.P.; Meller, D. Comparison of cryopreserved and air-dried human amniotic membrane for ophthalmologic applications. Graefes Arch. Clin. Exp. Ophthalmol. 2009, 247, 1691–1700. [Google Scholar] [CrossRef]
- Chun, B.Y.; Kim, H.K.; Shin, J.P. Dried human amniotic membrane does not alleviate inflammation and fibrosis in experimental strabismus surgery. J. Ophthalmol. 2013, 2013, 369126. [Google Scholar] [CrossRef] [Green Version]
- Pogozhykh, D.; Pogozhykh, O.; Prokopyuk, V.; Kuleshova, L.; Goltsev, A.; Blasczyk, R.; Mueller, T. Influence of temperature fluctuations during cryopreservation on vital parameters, differentiation potential, and transgene expression of placental multipotent stromal cells. Stem Cell Res. Ther. 2017, 8, 66. [Google Scholar] [CrossRef] [Green Version]
- Hopkinson, A.; McIntosh, R.S.; Tighe, P.J.; James, D.K.; Dua, H.S. Amniotic membrane for ocular surface reconstruction: Donor variations and the effect of handling on TGF-beta content. Investig. Ophthalmol. Vis. Sci. 2006, 47, 4316–4322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lewis, J.K.; Bischof, J.C.; Braslavsky, I.; Brockbank, K.G.; Fahy, G.M.; Fuller, B.J.; Rabin, Y.; Tocchio, A.; Woods, E.J.; Wowk, B.G.; et al. The Grand Challenges of Organ Banking: Proceedings from the first global summit on complex tissue cryopreservation. Cryobiology 2016, 72, 169–182. [Google Scholar] [CrossRef] [PubMed]
- Caruselli, M.; Tigano, F. Effect of Filatov’s placental extracts on some immunization phenomena. G. Batteriol. Immunol. 1953, 46, 15–23. [Google Scholar] [PubMed]
- Pipino, C.; Shangaris, P.; Resca, E.; Zia, S.; Deprest, J.; Sebire, N.J.; David, A.L.; Guillot, P.V.; De Coppi, P. Placenta as a reservoir of stem cells: An underutilized resource? Br. Med. Bull. 2013, 105, 43–68. [Google Scholar] [CrossRef] [Green Version]
- Asgari, H.R.; Akbari, M.; Yazdekhasti, H.; Rajabi, Z.; Navid, S.; Aliakbari, F.; Abbasi, N.; Aval, F.S.; Shams, A.; Abbasi, M. Comparison of Human Amniotic, Chorionic, and Umbilical Cord Multipotent Mesenchymal Stem Cells Regarding Their Capacity for Differentiation Toward Female Germ Cells. Cell Reprogram 2017, 19, 44–53. [Google Scholar] [CrossRef]
- Erdem, E.; Yagmur, M.; Harbiyeli, I.; Taylan-Sekeroglu, H.; Ersoz, R. Umbilical cord blood serum therapy for the management of persistent corneal epithelial defects. Int. J. Ophthalmol. 2014, 7, 807–810. [Google Scholar]
- Mermet, I.; Pottier, N.; Sainthillier, J.M.; Malugani, C.; Cairey-Remonnay, S.; Maddens, S.; Riethmuller, D.; Tiberghien, P.; Humbert, P.; Aubin, F. Use of amniotic membrane transplantation in the treatment of venous leg ulcers. Wound Repair. Regen. 2007, 15, 459–464. [Google Scholar] [CrossRef]
- Heckmann, N.; Auran, R.; Mirzayan, R. Application of Amniotic Tissue in Orthopedic Surgery. Am. J. Orthop. (Belle Mead N.J.) 2016, 45, E421–E425. [Google Scholar]
- De Röth, A. Plastic repair of conjunctival defects with fetal membranes. Arch Ophthalmol. 1940, 23, 522–525. [Google Scholar] [CrossRef]
- Gicquel, J.J.; Dua, H.S.; Brodie, A.; Mohammed, I.; Suleman, H.; Lazutina, E.; James, D.K.; Hopkinson, A. Epidermal growth factor variations in amniotic membrane used for ex vivo tissue constructs. Tissue Eng. Part A 2009, 15, 1919–1927. [Google Scholar] [CrossRef]
- Yatim, R.M.; Kannan, T.P.; Ab Hamid, S.S. Effect of gamma radiation on the expression of mRNA growth factors in glycerol cryopreserved human amniotic membrane. Cell Tissue Bank 2016, 17, 643–651. [Google Scholar] [CrossRef] [PubMed]
- Bischoff, M.; Stachon, T.; Seitz, B.; Huber, M.; Zawada, M.; Langenbucher, A.; Szentmary, N. Growth Factor and Interleukin Concentrations in Amniotic Membrane-Conditioned Medium. Curr. Eye Res. 2017, 42, 174–180. [Google Scholar] [CrossRef] [PubMed]
- Litwiniuk, M.; Radowicka, M.; Krejner, A.; Sladowska, A.; Grzela, T. Amount and distribution of selected biologically active factors in amniotic membrane depends on the part of amnion and mode of childbirth. Can we predict properties of amnion dressing? A proof-of-concept study. Cent. Eur. J. Immunol. 2018, 43, 97–102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lopez-Valladares, M.J.; Teresa Rodriguez-Ares, M.; Tourino, R.; Gude, F.; Teresa Silva, M.; Couceiro, J. Donor age and gestational age influence on growth factor levels in human amniotic membrane. Acta Ophthalmol. 2010, 88, e211–e216. [Google Scholar] [CrossRef]
- Lei, J.; Priddy, L.B.; Lim, J.J.; Massee, M.; Koob, T.J. Identification of Extracellular Matrix Components and Biological Factors in Micronized Dehydrated Human Amnion/Chorion Membrane. Adv. Wound Care (New Rochelle) 2017, 6, 43–53. [Google Scholar] [CrossRef] [Green Version]
- Murphy, S.V.; Skardal, A.; Song, L.; Sutton, K.; Haug, R.; Mack, D.L.; Jackson, J.; Soker, S.; Atala, A. Solubilized Amnion Membrane Hyaluronic Acid Hydrogel Accelerates Full-Thickness Wound Healing. Stem Cells Transl. Med. 2017, 6, 2020–2032. [Google Scholar] [CrossRef]
- Kim, T.G.; Do Ki, K.; Lee, M.K.; So, J.W.; Chung, S.K.; Kang, J. Comparison of cytokine expression and ultrastructural alterations in fresh-frozen and dried electron beam-irradiated human amniotic membrane and chorion. Cell Tissue Bank 2019, 20, 163–172. [Google Scholar] [CrossRef]
- Ab Hamid, S.S.; Zahari, N.K.; Yusof, N.; Hassan, A. Scanning electron microscopic assessment on surface morphology of preserved human amniotic membrane after gamma sterilisation. Cell Tissue Bank 2014, 15, 15–24. [Google Scholar] [CrossRef]
- Perepelkin, N.M.; Hayward, K.; Mokoena, T.; Bentley, M.J.; Ross-Rodriguez, L.U.; Marquez-Curtis, L.; McGann, L.E.; Holovati, J.L.; Elliott, J.A. Cryopreserved amniotic membrane as transplant allograft: Viability and post-transplant outcome. Cell Tissue Bank 2016, 17, 39–50. [Google Scholar] [CrossRef]
- Pegg, D.E. The relevance of ice crystal formation for the cryopreservation of tissues and organs. Cryobiology 2010, 60, S36–S44. [Google Scholar] [CrossRef]
- Kikuchi, M.; Feng, Z.; Kosawada, T.; Sato, D.; Nakamura, T.; Umezu, M. Stress relaxation and stress-strain characteristics of porcine amniotic membrane. Biomed. Mater. Eng. 2016, 27, 603–611. [Google Scholar] [CrossRef] [PubMed]
- Faturechi, R.; Hashemi, A.; Fatouraee, N. Do mechanical properties of human fetal membrane depend on strain rate? J. Obstet. Gynaecol. Res. 2015, 41, 84–91. [Google Scholar] [CrossRef] [PubMed]
- Mutsenko, V.; Barlic, A.; Pezic, T.; Dermol-Cerne, J.; Dovgan, B.; Sydykov, B.; Wolkers, W.F.; Katkov, I.I.; Glasmacher, B.; Miklavcic, D.; et al. Me2SO- and serum-free cryopreservation of human umbilical cord mesenchymal stem cells using electroporation-assisted delivery of sugars. Cryobiology 2019, 91, 104–114. [Google Scholar] [CrossRef] [PubMed]
- Mutsenko, V.; Knaack, S.; Lauterboeck, L.; Tarusin, D.; Sydykov, B.; Cabiscol, R.; Ivnev, D.; Belikan, J.; Beck, A.; Dipresa, D.; et al. Effect of ’in air’ freezing on post-thaw recovery of Callithrix jacchus mesenchymal stromal cells and properties of 3D collagen-hydroxyapatite-scaffolds. Cryobiology 2020, 92, 215–230. [Google Scholar] [CrossRef]
- Zernetsch, H.; Repanas, A.; Rittinghaus, T.; Mueller, M.; Alfred, I.; Glasmacher, B. Electrospinning and mechanical properties of polymeric fibers using a novel gap-spinning collector. Fibers Polym. 2016, 17, 1025–1032. [Google Scholar] [CrossRef]






© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pogozhykh, O.; Hofmann, N.; Gryshkov, O.; von Kaisenberg, C.; Mueller, M.; Glasmacher, B.; Pogozhykh, D.; Börgel, M.; Blasczyk, R.; Figueiredo, C. Repeated Freezing Procedures Preserve Structural and Functional Properties of Amniotic Membrane for Application in Ophthalmology. Int. J. Mol. Sci. 2020, 21, 4029. https://doi.org/10.3390/ijms21114029
Pogozhykh O, Hofmann N, Gryshkov O, von Kaisenberg C, Mueller M, Glasmacher B, Pogozhykh D, Börgel M, Blasczyk R, Figueiredo C. Repeated Freezing Procedures Preserve Structural and Functional Properties of Amniotic Membrane for Application in Ophthalmology. International Journal of Molecular Sciences. 2020; 21(11):4029. https://doi.org/10.3390/ijms21114029
Chicago/Turabian StylePogozhykh, Olena, Nicola Hofmann, Oleksandr Gryshkov, Constantin von Kaisenberg, Marc Mueller, Birgit Glasmacher, Denys Pogozhykh, Martin Börgel, Rainer Blasczyk, and Constança Figueiredo. 2020. "Repeated Freezing Procedures Preserve Structural and Functional Properties of Amniotic Membrane for Application in Ophthalmology" International Journal of Molecular Sciences 21, no. 11: 4029. https://doi.org/10.3390/ijms21114029