Microparticles Carrying Sonic Hedgehog Are Increased in Humans with Peripheral Artery Disease

 , ,
, ,
Abstract
:1. Introduction
2. Results
3. Discussion
4. Materials and Methods
4.1. Patients
4.2. Analysis of Collateral Vessels
4.3. MP Analysis
4.4. Plasma Collection, MP Depletion of Plasma, and Determination of Shh Protein Concentration
4.5. Statistical Analysis
Author Contributions
Funding
Conflicts of Interest
References
- Agouni, A.; Mostefai, H.A.; Porro, C.; Carusio, N.; Favre, J.; Richard, V.; Henrion, D.; Martinez, M.C.; Andriantsitohaina, R. Sonic hedgehog carried by microparticles corrects endothelial injury through nitric oxide release. FASEB J. 2007, 21, 2735–2741. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katoh, Y.; Katoh, M. Hedgehog target genes: Mechanisms of carcinogenesis induced by aberrant hedgehog signaling activation. Curr. Mol. Med. 2009, 9, 873–886. [Google Scholar] [CrossRef] [PubMed]
- Pola, R.; Ling, L.E.; Silver, M.; Corbley, M.J.; Kearney, M.; Blake Pepinsky, R.; Shapiro, R.; Taylor, F.R.; Baker, D.P.; Asahara, T.; et al. The morphogen Sonic hedgehog is an indirect angiogenic agent upregulating two families of angiogenic growth factors. Nat. Med. 2001, 7, 706–711. [Google Scholar] [CrossRef]
- Qin, Y.; He, Y.H.; Hou, N.; Zhang, G.S.; Cai, Y.; Zhang, G.P.; Xiao, Q.; He, L.S.; Li, S.J.; Yi, Q.; et al. Sonic hedgehog improves ischemia-induced neovascularization by enhancing endothelial progenitor cell function in type 1 diabetes. Mol. Cell Endocrinol. 2016, 423, 30–39. [Google Scholar] [CrossRef] [PubMed]
- Passman, J.N.; Dong, X.R.; Wu, S.P.; Maguire, C.T.; Hogan, K.A.; Bautch, V.L.; Majesky, M.W. A sonic hedgehog signaling domain in the arterial adventitia supports resident Sca1+ smooth muscle progenitor cells. Proc. Natl. Acad. Sci. USA 2008, 105, 9349–9354. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piccioni, A.; Gaetani, E.; Palladino, M.; Gatto, I.; Smith, R.C.; Neri, V.; Marcantoni, M.; Giarretta, I.; Silver, M.; Straino, S.; et al. Sonic hedgehog gene therapy increases the ability of the dystrophic skeletal muscle to regenerate after injury. Gene Ther. 2014, 21, 413–421. [Google Scholar] [CrossRef] [PubMed]
- Palladino, M.; Gatto, I.; Neri, V.; Straino, S.; Silver, M.; Tritarelli, A.; Piccioni, A.; Smith, R.C.; Gaetani, E.; Losordo, D.W.; et al. Pleiotropic beneficial effects of sonic hedgehog gene therapy in an experimental model of peripheral limb ischemia. Mol. Ther. 2011, 19, 658–666. [Google Scholar] [CrossRef] [PubMed]
- Martinez, M.C.; Tesse, A.; Zobairi, F.; Andriantsitohaina, R. Shed membrane microparticles from circulating and vascular cells in regulating vascular function. Am. J. Physiol. Heart Circ. Physiol. 2005, 288, H1004–H1009. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taraboletti, G.; D’Ascenzo, S.; Borsotti, P.; Giavazzi, R.; Pavan, A.; Dolo, V. Shedding of the matrix metalloproteinases MMP-2, MMP-9, and MT1-MMP as membrane vesicle-associated components by endothelial cells. Am. J. Pathol. 2002, 160, 673–680. [Google Scholar] [CrossRef]
- Benameur, T.; Soleti, R.; Porro, C.; Andriantsitohaina, R.; Martinez, M.C. Microparticles carrying Sonic hedgehog favor neovascularization through the activation of nitric oxide pathway in mice. PLoS ONE 2010, 5, e12688. [Google Scholar] [CrossRef] [PubMed]
- Golomb, B.A.; Dang, T.T.; Criqui, M.H. Peripheral arterial disease: Morbidity and mortality implications. Circulation 2006, 114, 688–699. [Google Scholar] [CrossRef]
- Pola, R.; Ling, L.E.; Aprahamian, T.R.; Barban, E.; Bosch-Marce, M.; Curry, C.; Corbley, M.; Kearney, M.; Isner, J.M.; Losordo, D.W. Postnatal recapitulation of embryonic hedgehog pathway in response to skeletal muscle ischemia. Circulation 2003, 108, 479–485. [Google Scholar] [CrossRef]
- Kusano, K.F.; Allendoerfer, K.L.; Munger, W.; Pola, R.; Bosch-Marce, M.; Kirchmair, R.; Yoon, Y.S.; Curry, C.; Silver, M.; Kearney, M.; et al. Sonic hedgehog induces arteriogenesis in diabetic vasa nervorum and restores function in diabetic neuropathy. Arterioscler. Thromb. Vasc. Biol. 2004, 24, 2102–2107. [Google Scholar] [CrossRef]
- Kusano, K.F.; Pola, R.; Murayama, T.; Curry, C.; Kawamoto, A.; Iwakura, A.; Shintani, S.; Ii, M.; Asai, J.; Tkebuchava, T.; et al. Sonic hedgehog myocardial gene therapy: Tissue repair through transient reconstitution of embryonic signaling. Nat. Med. 2005, 11, 1197–1204. [Google Scholar] [CrossRef]
- Benameur, T.; Andriantsitohaina, R.; Martinez, M.C. Therapeutic potential of plasma membrane-derived microparticles. Pharmacol. Rep. 2009, 61, 49–57. [Google Scholar] [CrossRef]
- Bijlsma, M.F.; Groot, A.P.; Oduro, J.P.; Franken, R.J.; Schoenmakers, S.H.; Peppelenbosch, M.P.; Spek, C.A. Hypoxia induces a hedgehog response mediated by HIF-1α. J. Cell Mol. Med. 2009, 13, 2053–2060. [Google Scholar] [CrossRef]
- Caradu, C.; Guy, A.; James, C.; Reynaud, A.; Gadeau, A.P.; Renault, M.A. Endogenous Sonic Hedgehog limits inflammation and angiogenesis in the ischaemic skeletal muscle of mice. Cardiovasc. Res. 2018, 114, 759–770. [Google Scholar] [CrossRef]
- Tanaka, T.; Arai, M.; Minemura, S.; Oyamada, A.; Saito, K.; Jiang, X.; Tsuboi, M.; Sazuka, S.; Maruoka, D.; Matsumura, T.; et al. Expression level of sonic hedgehog correlated with the speed of gastric mucosa regeneration in artificial gastric ulcers. J. Gastroenterol. Hepatol. 2014, 29, 736–741. [Google Scholar] [CrossRef]
- Song, K.; Rao, N.J.; Chen, M.L.; Huang, Z.J.; Cao, Y.G. Enhanced bone regeneration with sequential delivery of basic fibroblast growth factor and sonic hedgehog. Injury 2011, 42, 796–802. [Google Scholar] [CrossRef]
- Johnson, N.R.; Wang, Y. Controlled delivery of sonic hedgehog morphogen and its potential for cardiac repair. PLoS ONE 2013, 8, e63075. [Google Scholar] [CrossRef]
- Soleti, R.; Benameur, T.; Porro, C.; Panaro, M.A.; Andriantsitohaina, R.; Martinez, M.C. Microparticles harboring Sonic Hedgehog promote angiogenesis through the upregulation of adhesion proteins and proangiogenic factors. Carcinogenesis 2009, 30, 580–588. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marrachelli, V.G.; Mastronardi, M.L.; Sarr, M.; Soleti, R.; Leonetti, D.; Martinez, M.C.; Andriantsitohaina, R. Sonic hedgehog carried by microparticles corrects angiotensin II-induced hypertension and endothelial dysfunction in mice. PLoS ONE 2013, 8, e72861. [Google Scholar] [CrossRef] [PubMed]
- Paulis, L.; Fauconnier, J.; Cazorla, O.; Thireau, J.; Soleti, R.; Vidal, B.; Ouille, A.; Bartholome, M.; Bideaux, P.; Roubille, F.; et al. Activation of Sonic hedgehog signaling in ventricular cardiomyocytes exerts cardioprotection against ischemia reperfusion injuries. Sci. Rep. 2015, 5, 7983. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crawford, J.R.; Trial, J.; Nambi, V.; Hoogeveen, R.C.; Taffet, G.E.; Entman, M.L. Plasma Levels of Endothelial Microparticles Bearing Monomeric C-reactive Protein are Increased in Peripheral Artery Disease. J. Cardiovasc. Transl. Res. 2016, 9, 184–193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burdess, A.; Michelsen, A.E.; Brosstad, F.; Fox, K.A.; Newby, D.E.; Nimmo, A.F. Platelet activation in patients with peripheral vascular disease: Reproducibility and comparability of platelet markers. Thromb. Res. 2012, 129, 50–55. [Google Scholar] [CrossRef] [PubMed]
- Suggested standards for reports dealing with lower extremity ischemia. Prepared by the Ad Hoc Committee on Reporting Standards, Society for Vascular Surgery/North American Chapter, International Society for Cardiovascular Surgery. J. Vasc. Surg. 1986, 4, 80–94. Available online: https://www.ncbi.nlm.nih.gov/pubmed/3723692 (accessed on 29 November 2018). [CrossRef]
- Suh, H.P.; Kim, Y.; Suh, Y.; Hong, J. Multidetector Computed Tomography (CT) Analysis of 168 Cases in Diabetic Patients with Total Superficial Femoral Artery Occlusion: Is It Safe to Use an Anterolateral Thigh Flap without CT Angiography in Diabetic Patients? J. Reconstr. Microsurg. 2018, 34, 65–70. [Google Scholar] [CrossRef] [PubMed]
- Coumans, F.A.W.; Brisson, A.R.; Buzas, E.I.; Dignat-George, F.; Drees, E.E.E.; El-Andaloussi, S.; Emanueli, C.; Gasecka, A.; Hendrix, A.; Hill, A.F.; et al. Methodological Guidelines to Study Extracellular Vesicles. Circ. Res. 2017, 120, 1632–1648. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | PAD | Controls | p | |
|---|---|---|---|---|
| Years of age (mean ± SD) | 71.4 ± 9.4 | 70.3 ± 8.2 | n.s. | |
| Males, n (%) | 37 (74.0) | 27 (54.0) | <0.05 | |
| Smokers, n (%) | 17 (34.0) | 7 (14.0) | <0.01 | |
| Diabetes, n (%) | 22 (44.0) | 17 (34.0) | n.s. | |
| Dyslipidemia, n (%) | 36 (72.0) | 30 (60.0) | n.s. | |
| Hypertension, n (%) | 40 (80.0) | 40 (80.0) | n.s. | |
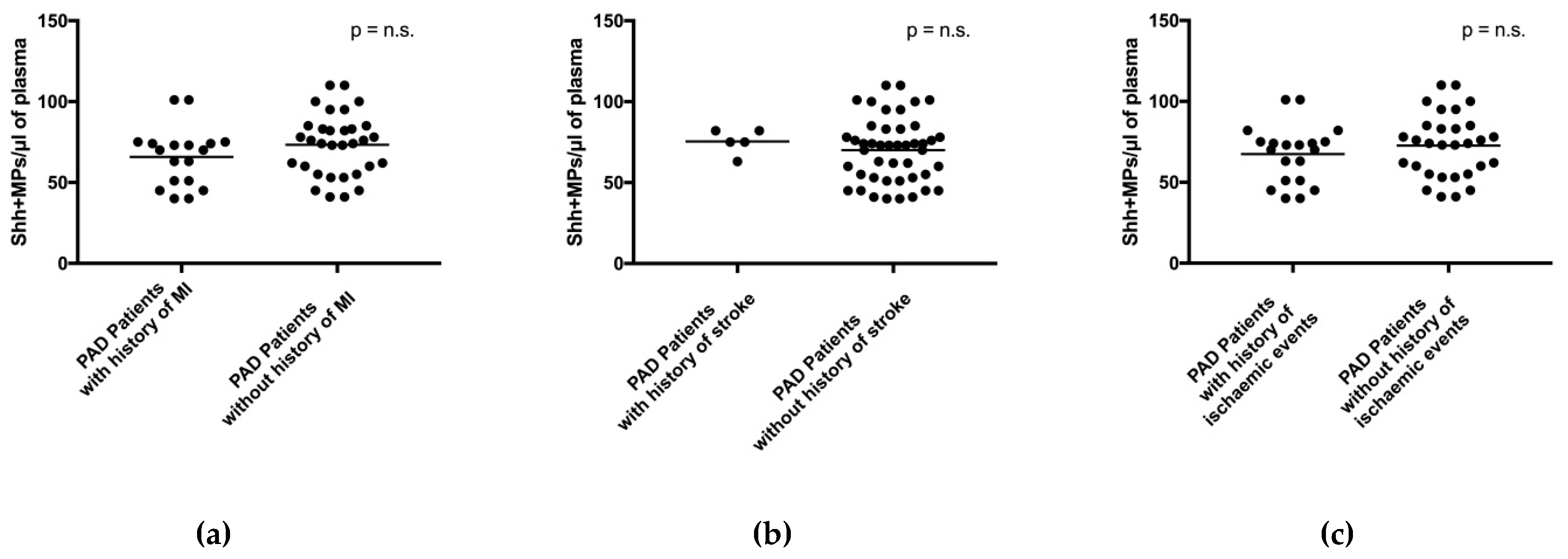
| Previous MI, n (%) | 21 (42.0) | 4 (8.0) | <0.01 | |
| Previous Stroke, n (%) | 6 (12.0) | 0 (0.0) | <0.01 | |
| Therapy | SAPT, n (%) | 33 (66.0) | 24 (48.0) | 0.04 |
| DAPT, n (%) | 9 (18.0) | 0 (0.0) | <0.01 | |
| Statins, n (%) | 36 (72.0) | 28 (56.0) | n.s. | |
| ACE inhibitors/ARB, n (%) | 27 (54.0) | 26 (52.0) | n.s. | |
| Beta-blockers, n (%) | 23 (46.0) | 19 (38.0) | n.s. | |
| Type of MPs | PAD | Controls | p |
|---|---|---|---|
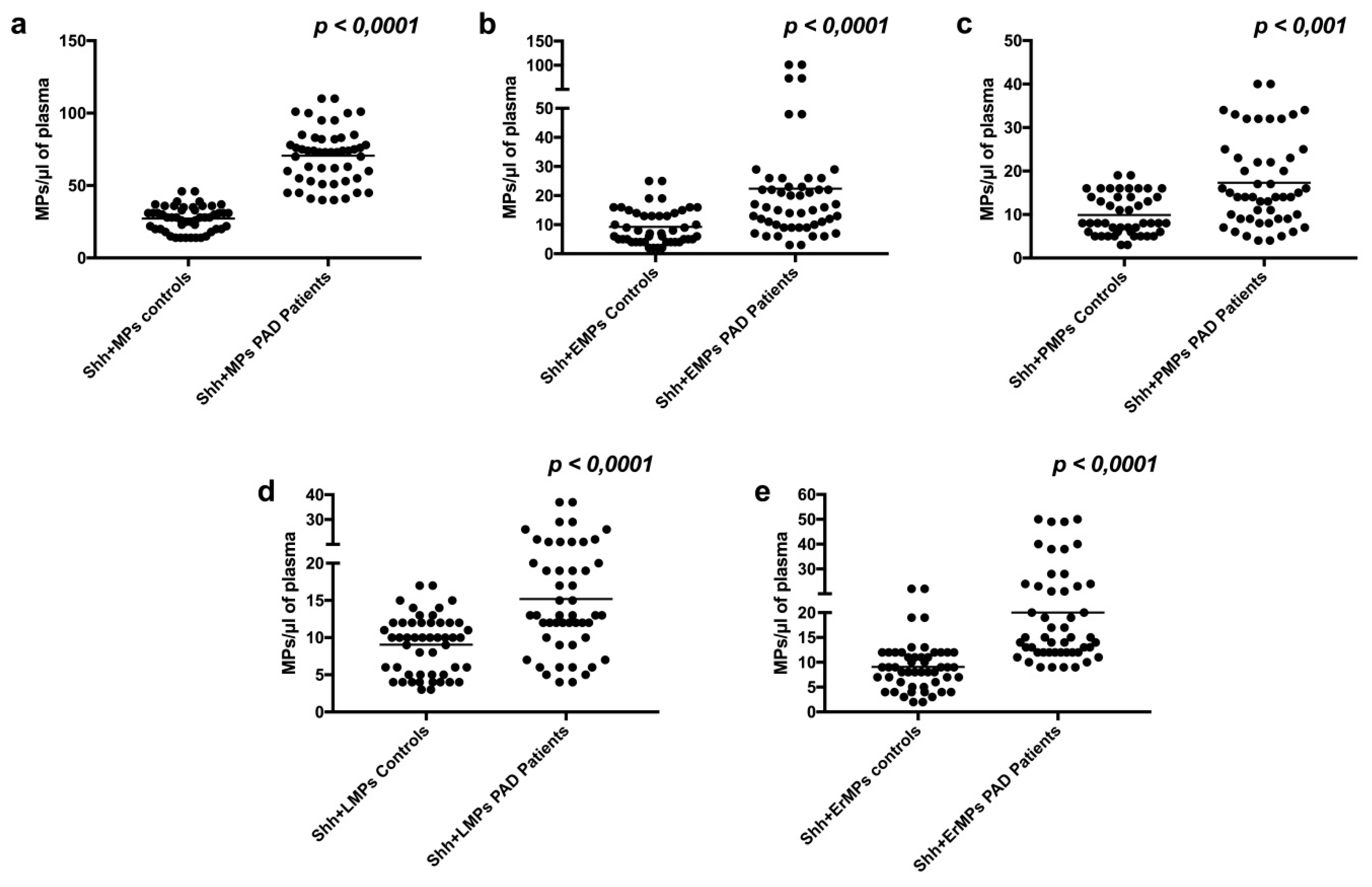
| Shh + MPs/μL (mean ± SD) | 70.5 ± 19.0 | 27.2 ± 8.5 | p < 0.001 |
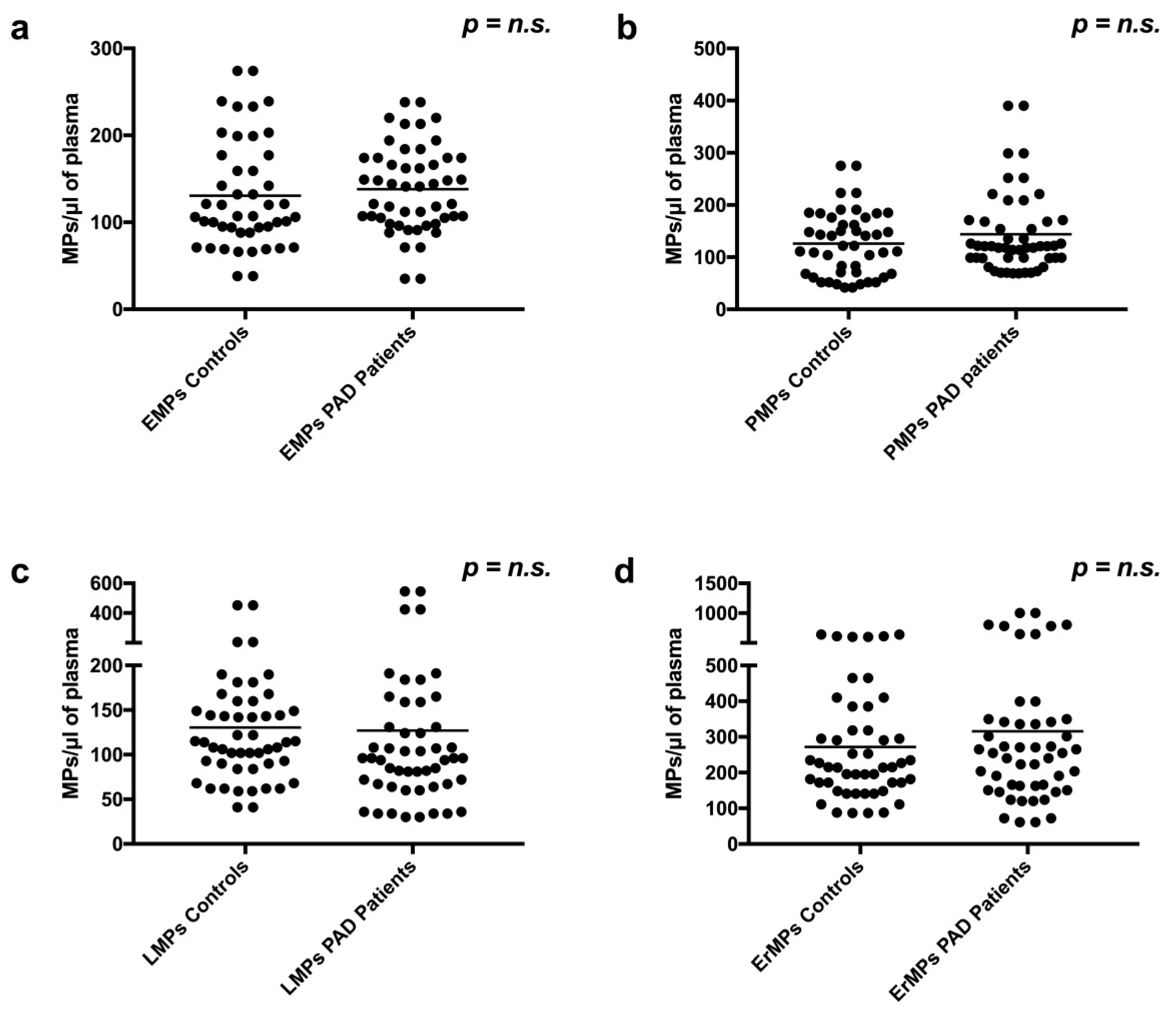
| EMPs/μL (mean ± SD) | 138.2 ± 49.2 | 130.6 ± 62.2 | n.s |
| Shh + EMPs/μL (mean ± SD) | 22.3 ± 21.8 | 9.2 ± 6.0 | p < 0.001 |
| PMPs/μL (mean ± SD) | 143.9 ± 77.1 | 126.1 ± 61.6 | n.s |
| Shh + PMPs/μL (mean ± SD) | 17.3 ± 10.1 | 9.9 ± 4.6 | p < 0.001 |
| LMPs/μL (mean ± SD) | 126.9 ± 116.6 | 130.5 ± 79.0 | 0.09 |
| Shh + LMPs/μL (mean ± SD) | 15.2 ± 7.9 | 9.0 ± 3.9 | p < 0.001 |
| ErMPs/µL (mean ± SD) | 315.5 ± 238.7 | 271.6 ± 159.5 | n.s. |
| Shh + ErMPs/µL (mean ± SD) | 20.0 ± 11.8 | 9.8 ± 4.6 | p < 0.001 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Giarretta, I.; Gatto, I.; Marcantoni, M.; Lupi, G.; Tonello, D.; Gaetani, E.; Pitocco, D.; Iezzi, R.; Truma, A.; Porfidia, A.; et al. Microparticles Carrying Sonic Hedgehog Are Increased in Humans with Peripheral Artery Disease. Int. J. Mol. Sci. 2018, 19, 3954. https://doi.org/10.3390/ijms19123954
Giarretta I, Gatto I, Marcantoni M, Lupi G, Tonello D, Gaetani E, Pitocco D, Iezzi R, Truma A, Porfidia A, et al. Microparticles Carrying Sonic Hedgehog Are Increased in Humans with Peripheral Artery Disease. International Journal of Molecular Sciences. 2018; 19(12):3954. https://doi.org/10.3390/ijms19123954
Chicago/Turabian StyleGiarretta, Igor, Ilaria Gatto, Margherita Marcantoni, Giulia Lupi, Diego Tonello, Eleonora Gaetani, Dario Pitocco, Roberto Iezzi, Addolorata Truma, Angelo Porfidia, and et al. 2018. "Microparticles Carrying Sonic Hedgehog Are Increased in Humans with Peripheral Artery Disease" International Journal of Molecular Sciences 19, no. 12: 3954. https://doi.org/10.3390/ijms19123954