
Abstract
There are insufficient data in managing patients at high risk of deterioration. We aimed to investigate that national early warning score (NEWS) could predict severe outcomes in patients identified by a rapid response system (RRS), focusing on the patient’s age. We conducted a retrospective cohort study from June 2019 to December 2020. Outcomes were unplanned intensive care unit (ICU) admission, ICU mortality, and in-hospital mortality. We analyzed the predictive ability of NEWS using receiver operating characteristics (ROC) curve and the effect of NEWS parameters using multivariable logistic regression. A total of 2,814 RRS activations were obtained. The predictive ability of NEWS for unplanned ICU admission and in-hospital mortality was fair but was poor for ICU mortality. The predictive ability of NEWS showed no differences between patients aged 80 years or older and under 80 years. However, body temperature affected in-hospital mortality for patients aged 80 years or older, and the inverse effect on unplanned ICU admission was observed. The NEWS showed fair predictive ability for unplanned ICU admission and in-hospital mortality among patients identified by the RRS. The different presentations of patients 80 years or older should be considered in implementing the RRS.
Similar content being viewed by others

Introduction
The United Nations defines a super-aged society as a society where 20% of the total population is 65 years or older1. Population worldwide is rapidly aging and, by 2050, more than 20% of the world’s population is expected to be 65 years or older2,3. Including South Korea, one of the world’s fastest aging societies, many countries transformed into a super-aged society4,5. Following the current trends, the management of the elderly population is emerging as an important social issue6. Elderly patients have various comorbidities, and often cognitive functions become impaired7,8. Also, managing elderly patients who require hospitalization is challenging9,10,11. Consequently, early recognition of the patient’s deterioration becomes a crucial part of successful treatment for elderly hospitalized patients12.
A rapid response system (RRS) is a preventive system for the early detection of hospitalized patients at high risk of deterioration13. Various early warning scoring system was used in the implementation of the RRS14,15. The National early warning score (NEWS), created in 2012 by the Royal College of Physicians of London standardizing the assessment of acute illness severity, is one of the early warning scoring systems used to implement RRS16,17. Several studies have demonstrated that NEWS effectively detects patients at high risk of deterioration relating to unexpected intensive care unit (ICU) admission and in-hospital mortality18. However, in the resource-limited environment such as rural areas of the super-aged society, prioritization of management may be required among patients identified by the RRS19. Nonetheless, there was insufficient information that clinicians can use as a reference in their management.
To the best of our knowledge, the usefulness of NEWS was unknown in the management of elderly patients identified by RRS. We hypothesized that NEWS could be used for predicting severe outcomes in managing hospitalized elderly patients at high risk of deterioration. Therefore, the purpose of this study was to investigate the predictive ability of NEWS for severe outcomes in patients identified by the RRS, focusing on the patient’s age.
Results
Baseline characteristics of the study population
A total of 2,814 RRS activations from 851 patients were recorded, at an average of 3.3 RRS activations per patient. The mean ± standard deviation (SD) age of all patients was 72.6 ± 14.2, and the proportion of men was 60.2%. The mean ± SD age was 65.1 ± 12.6 for patients 80 years or older and 85.3 ± 4.2 for patients under 80 years, respectively. Baseline characteristics according to age group are depicted in Table 1. In patients under 80 years, the proportions of males, high body mass index (BMI), high systolic blood pressure score, and high heart rate score were higher than patients 80 years or older. For disease classification, differences in diagnosed disease distributions by age group were statistically significant except for gastrointestinal diseases. Pulmonary disease was the most common diagnosis in both groups, while the cardiovascular disease was the least diagnosed in patients under 80 years, and neurological disease was the least diagnosed in patients 80 years or older. Regarding severe outcomes, the proportion of unplanned ICU admissions (10.9% vs. 10.6%, p = 0.887) did not differ between the age groups, but proportions of ICU (1.3% vs. 2.9%, p = 0.005) and in-hospital mortality (47.5% vs. 40.2%, p < 0.001) were higher in patients 80 years or older.
Predicting severe outcomes using NEWS
Efficiency NEWS curves for severe outcomes by age group are shown in Supplementary Figure S1. The predictive ability of NEWS for unplanned ICU admission was slightly significantly efficient in patients 80 years or older, but there were no significant differences in the ability to predict ICU and in-hospital mortality. In the ROC curves, the predictive ability of NEWS for unplanned ICU admission (area under the receiver operating characteristic curve [AUROC] 0.650, 95% confidence interval [CI] 0.619–0.680) and in-hospital mortality (AUROC 0.661, 95% CI 0.641–0.680) was fair but was poor for ICU mortality (AUROC 0.566, 95% CI 0.489–0.643). There was no statistically significant difference between patients under 80 years and patients 80 years or older in the comparison of the predictive ability of NEWS for unplanned ICU admission (AUROC 0.639 [95% CI 0.601–0.677] vs. 0.666 [0.614–0.718], p = 0.409), for ICU mortality admission (AUROC 0.560 [95% CI 0.444–0.675] vs. 0.582 [0.478–0.687], p = 0.777), and for in-hospital mortality admission (AUROC 0.666 [95% CI 0.642–0.691] vs. 0.648 [0.615–0.680], p = 0.365) (Fig. 1). In patients 80 years or older, the NEWS cut-off values were 9 for unplanned ICU admission, 10 for ICU mortality, and 9 for in-hospital mortality, respectively. Sensitivity and specificity for severe outcomes according to NEWS are described in Table 2.

Receiver operating characteristic curves of the National early warning score for severe outcomes by age group. Dots indicate thresholds of National early warning score for the highest accuracy. NEWS National early warning score, ICU intensive care unit, AUROC area under the receiver operating characteristic curve, Se sensitivity, Sp specificity.
Effects of NEWS parameters on severe outcomes
In the multivariable logistic regression analysis, body temperature was significantly related to unplanned ICU admission in patients under 80 years (odds ratio [OR] 1.57, 95% CI 1.22–2.00, p < 0.001), but not in patients 80 years or older (OR 0.78, 95% CI 0.49–1.21, p = 0.295) (Fig. 2). However, body temperature had an inverse relationship with in-hospital mortality. The results of sensitivity analyses using raw NEWS parameters are shown in Table 3.

Effects of National early warning score parameters on severe outcomes by age group. ICU intensive care unit, OR odds ratio, CI confidence interval.
In subgroup analyses for patients 80 years or older, the AUROC of NEWS for unplanned ICU admission was significantly higher in patients with non-pulmonary diseases, high BMI, genitourinary disease, and neurological disease (Supplementary Table S1). In contrast, the AUROC of NEWS for in-hospital mortality was significantly higher in male, low BMI, and cancer patients. Among patients under 80 years, significant differences existed in gastrointestinal, neurological, and cancer subgroups for predicting unplanned ICU admission and BMI and genitourinary subgroups for predicting in-hospital mortality (Supplementary Table S2).
Discussion
Our study found that NEWS had a fair predictive ability for unplanned ICU admission and in-hospital mortality among the patients identified by the RRS. There were no differences in the ability of NEWS for predicting unplanned ICU admission and in-hospital mortality between patients 80 years or older and patients under 80 years. However, the overall prediction accuracy for ICU mortality was low in both age groups, possibly due to the small ICU mortality cases.
NEWS is widely used as a reference score for RRS, and patients with NEWS seven or higher are considered at high risk of deterioration15,20. Smith et al. reported that NEWS outperformed other early warning scores for predicting cardiac arrest, unplanned ICU admission, and death within 24 h21. Liu et al. and Smith et al. also showed that NEWS had significant discriminative power for identifying in-hospital mortality22,23. However, little is known about indicators that predict severe outcomes in patients identified as high risk through NEWS. Our findings could provide references for managing patients identified by the RRS.
To the best of our knowledge, no previous studies have suggested additional cut-off values of the NEWS for predicting severe outcomes among elderly patients identified by the RRS. The cut-off of the NEWS discriminating high risk patients is well established24,25. However, in elderly populations, a large number of patients can be classified as high risk26. It is also challenging to perform intensive management for all these patients in resource-limited situations27. Therefore, additional screening criteria are necessary to assess which patients require immediate intensive care. We estimated cut-off values in high risk patients that can predict unplanned ICU admission and in-hospital mortality. The cut-off value for unplanned ICU admission was higher in patients 80 years or older. In this regard, transfer to ICU should be carefully considered in very elderly patients identified by the RRS.
Among NEWS parameters, respiratory rate, SpO2, and heart rate affected unplanned ICU admission, while all parameters affected in-hospital mortality. In particular, body temperature did not affect unplanned ICU admission in patients 80 years or older. Thermoregulation and immune function are lower in elderly populations, which can cause an afebrile condition in people with severe infection28,29. Consequently, body temperature may not affect unplanned ICU admission. On the other hand, body temperature had a significant effect on in-hospital mortality. In very elderly patients, body temperature changes may lead to adverse outcomes, such as in-hospital mortality. Therefore, in implementing RRS, body temperature in patients 80 years or older may need to be interpreted carefully.
In subgroup of patients with low BMI, the predictive ability of NEWS was poor for unplanned ICU admission but good for in-hospital mortality. Low BMI is associated with decreased health conditions, such as malnutrition and cachexia, relating to poor disease prognosis30. Among high risk patients with low BMI, NEWS may predict a long-term prognosis than a sudden deterioration. The predictive ability of NEWS for unplanned ICU admission was poor in patients 80 years or older with pulmonary diseases. A previous study reported the concern about a decreased ability of NEWS in patients with chronic hypoxemia31. In addition, there was an attempt to supplement respiratory parameters, such as NEWS2, which adds hypercapnic respiratory failure assessment to NEWS32. Therefore, a multi-dimensional approach will be required in patients 80 years or older with pulmonary diseases. Meanwhile, the predictive ability of NEWS for in-hospital mortality was superior for men. It may be due to gender differences in various diseases33,34. Mechanisms related to these differences, such as oxidative stress, cannot be measured with NEWS35. Gender differences in the prediction of severe outcomes should be evaluated in future studies.
The limitation of our study is that our findings were derived from a single-center-based retrospective cohort in South Korea. Each country has its health care system. Therefore, the results of this study may not be widely generalizable. In addition, a relatively small number of patients participated during the mid-term period. Therefore, potential selection bias should be considered in the interpretation of our findings. However, as we mentioned earlier, this study was based on a nationwide RRS pilot program. Besides, the hospital where this study was conducted is located in the state with the highest number of elderly patients in South Korea. Further validation is required after the RRS program is officially launched.
Nevertheless, our study has several strengths. A large number of patients 80 years or older participated in this study, enabling it to serve as a reference for hospitalized patient care for a growing number of aging societies. Healthcare resources can be strained due to external factors such as the coronavirus-19 (COVID-19) pandemic, and our findings can help clinicians prioritize high risk patients who need immediate intensive care. We believe that accurately applied intensive care can help prevent a pandemic-induced collapse of a healthcare system. Finally, cut-off values and important parameters for NEWS were presented. Besides, we found characteristics that NEWS performed with high accuracy in patients 80 year or older; thus, clinicians can apply NEWS when making treatment or care decisions for very elderly patients.
In conclusion, the NEWS showed fair predictive ability for unplanned ICU admission and in-hospital mortality among patients identified by RRS. Clinicians should consider the different presentations of patients 80 years or older at high risk of deterioration. More studies are required on the management of elderly patients at high risk of deterioration.
Methods
Study population
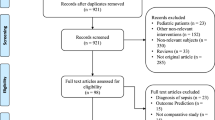
A single-center-based, retrospective, consecutive cohort study was conducted at Hallym University Chuncheon Sacred Heart Hospital, a teaching hospital, from June 2019 to December 2020. In this hospital, the RRS pilot program was operated by the Korean government36. When a patient’s NEWS was recorded seven or higher, the detected patient was classified as a high risk. After that, a member of the rapid response team visited the patients and intervened in their management. The RRS activations for the same patients detected at different times were regarded as separate cases. For all hospitalized patients, the NEWS was measured and recorded automatically using an electronic health-record-based system. We retrospectively reviewed all data of RRS activations, and 3,163 RRS activations from 935 patients were obtained. Of the 3,163 activations, we excluded 14 activated after ICU admission, 10 activated for patients < 18 years, and 325 with missing data. Therefore, 2,814 RRS activations from 851 patients were included in the final analysis.
Ethics declarations
This retrospective cohort study was conducted in accordance with the Helsinki declaration and approved by the Institutional Review Board (IRB) of the Hallym University Chuncheon Sacred Heart Hospital (IRB number: 2021-02-007). The need for written informed consent was waived and confirmed by the IRB of the Hallym University Chuncheon Sacred Heart Hospital (IRB number: 2021-02-007) because this was a retrospective cohort study.
National early warning score
The NEWS was used as a reference value for RRS activation. The cut-off value of NEWS for activating RRS was seven. The NEWS consists of seven physiological parameters, and the total score is calculated by summing scores for each parameter (Supplementary Table S3)37. The physiologic NEWS parameters were respiratory rate, systolic blood pressure, level of consciousness, supplemental oxygen, heart rate, saturation of percutaneous oxygen (SpO2), and body temperature. These items were scored from 0 to 3 points each, except SpO2 ranged from 0 to 2 points.
Severe outcomes
We regarded unplanned ICU admission, ICU mortality, and in-hospital mortality as severe outcomes. Unplanned ICU admission, the main outcome of this study, was defined as abrupt transfer to the ICU within 24 h after the RRS activation. Secondary outcomes were ICU and in-hospital mortality, defined as death events within 24 h after ICU admission and within the hospitalized period, respectively. Cases of death in the ICU were also included in both ICU and in-hospital mortality. All incidents were identified automatically using the hospital’s electronic medical records.
Other measurements
BMI was defined as body weight divided by height squared (kg/m2). The reason for hospital admission consisted of cardiovascular, pulmonary, gastrointestinal, genitourinary, neurological diseases, and cancer. We used international disease classifications at admission for defining the disease classification38. Diseases not included in the above six categories, such as severe sepsis, were classified as other diseases.
Statistical analyses
All statistical analyses were performed using R version 4.0.3 (R core Team 2020; R Foundation for Statistical Computing, Vienna, Austria). We analyzed patients identified by the RRS according to the patient’s age. Among the NEWS parameters, continuous variables were categorized according to their scores and expressed as numbers (percentages). The p-value for comparing baseline characteristics was analyzed using Pearson’s chi-square test, except for the level of consciousness, which was analyzed using Fisher’s exact test. For assessing the predictive ability of the NEWS, a receiver operating characteristic (ROC) curve was drawn using the ‘pROC’ package for R. The 95% CI for the AUROC and p-values were calculated using Delong’s test. Sensitivity and specificity were calculated using 2000 stratified bootstrap replicates. The NEWS cut-off values for severe outcomes were calculated using the Youden index39.
We further analyzed the effect of NEWS parameters on severe outcomes using multivariable logistic regression analysis. Each parameter was adjusted for other parameters and the reason for hospital admission. Scored NEWS values were used for the main analysis, and sensitivity analyses were performed using the raw NEWS values. Because its observed values were low, the level of consciousness was excluded from the analysis.
Subgroup analyses were performed on sex, BMI, and the reason for hospital admission by age groups. The BMI subgroup was divided by the median. Subgroup analysis for ICU mortality was not performed due to the low number of ICU mortality cases. An additional subgroup analysis was performed with patients under 80 years. For all analyses in this study, p-values < 0.05 were considered statistically significant.
Data availability
Our datasets are available from the corresponding author on reasonable request.
Abbreviations
- NEWS:
-
National early warning score
- ICU:
-
Intensive care unit
- RRS:
-
Rapid response system
- SpO2:
-
Saturation of percutaneous oxygen
- BMI:
-
Body mass index
- ROC:
-
Receiver operating characteristic
- CI:
-
Confidence interval
- AUROC:
-
Area under the receiver operating characteristic curve
- OR:
-
Odds ratio
- SD:
-
Standard deviation
- COVID-19:
-
Coronavirus-19
References
Park, S., Yang, M.-J., Ha, S.-N. & Lee, J.-S. Effective anti-aging strategies in an era of super-aging. J. Menopausal Med. 20(3), 85 (2014).
The Organisation for Economic Co-operation and Development. Ageing and demographic change. https://www.oecd.org/economy/ageing-inclusive-growth/. Assessed 24 August 2021.
World Health Organization. Global health and aging. https://www.who.int/ageing/publications/global_health.pdf. Assessed 24 August 2021.
Kim, K. W. & Kim, O. S. Super Aging in South Korea unstoppable but mitigatable: A sub-national scale population projection for best policy planning. Spat. Demography. 8(2), 155–173 (2020).
World Health Organization. Ageing. https://www.who.int/health-topics/ageing#tab=tab_1. Assessed 24 August 2021.
Christensen, K., Doblhammer, G., Rau, R. & Vaupel, J. W. Ageing populations: The challenges ahead. The lancet. 374(9696), 1196–1208 (2009).
Hazra, N. C., Rudisill, C. & Gulliford, M. C. Determinants of health care costs in the senior elderly: Age, comorbidity, impairment, or proximity to death?. Eur. J. Health Econ. 19(6), 831–842 (2018).
Fu, C., Li, Z. & Mao, Z. Association between social activities and cognitive function among the elderly in China: A cross-sectional study. Int. J. Environ. Res. Public Health. 15, 2 (2018).
Roberts, H. C., Lim, S. E. R., Cox, N. J. & Ibrahim, K. The challenge of managing undernutrition in older people with frailty. Nutrients 11, 4 (2019).
Ananthakrishnan, A. N., Donaldson, T., Lasch, K. & Yajnik, V. Management of inflammatory bowel disease in the elderly patient: Challenges and opportunities. Inflamm. Bowel Dis. 23(6), 882–893 (2017).
Filippatos, T. D., Makri, A., Elisaf, M. S. & Liamis, G. Hyponatremia in the elderly: Challenges and solutions. Clin. Interv. Aging 12, 1957 (2017).
Lette, M. et al. Improving early detection initiatives: A qualitative study exploring perspectives of older people and professionals. BMC Geriatr. 17(1), 1–13 (2017).
Sakai, T. & DeVita, M. A. Rapid response system. J. Anesth. 23(3), 403–408 (2009).
Ludikhuize, J. et al. Standardized measurement of the modified early warning score results in enhanced implementation of a rapid response system: A quasi-experimental study. Resuscitation 85(5), 676–682 (2014).
Ehara, J. et al. The effectiveness of a national early warning score as a triage tool for activating a rapid response system in an outpatient setting: A retrospective cohort study. Medicine 98, 52 (2019).
McGinley, A. & Pearse, R. M. A national early warning score for acutely ill patients (British Medical Journal Publishing Group, 2012).
Dziadzko, M. A. et al. Multicenter derivation and validation of an early warning score for acute respiratory failure or death in the hospital. Crit. Care 22(1), 1–12 (2018).
Lee, Y. S. et al. Evaluation of the efficacy of the national early warning score in predicting in-hospital mortality via the risk stratification. J. Crit. Care 47, 222–226 (2018).
Mathews, K. S. et al. Effect of emergency department and intensive care unit occupancy on admission decisions and outcomes for critically ill patients. Crit. Care Med. 46(5), 720 (2018).
Subbe, C. P., Duller, B. & Bellomo, R. Effect of an automated notification system for deteriorating ward patients on clinical outcomes. Crit. Care 21(1), 1–9 (2017).
Smith, G. B., Prytherch, D. R., Meredith, P., Schmidt, P. E. & Featherstone, P. I. The ability of the National Early Warning Score (NEWS) to discriminate patients at risk of early cardiac arrest, unanticipated intensive care unit admission, and death. Resuscitation 84(4), 465–470 (2013).
Liu, V. X. et al. Comparison of early warning scoring systems for hospitalized patients with and without infection at risk for in-hospital mortality and transfer to the intensive care unit. JAMA Netw. Open 3(5), e205191–e205191 (2020).
Pimentel, M. A. et al. A comparison of the ability of the National Early Warning Score and the National Early Warning Score 2 to identify patients at risk of in-hospital mortality: A multi-centre database study. Resuscitation 134, 147–156 (2019).
Spångfors, M., Bunkenborg, G., Molt, M. & Samuelson, K. The National Early Warning Score predicts mortality in hospital ward patients with deviating vital signs: A retrospective medical record review study. J. Clin. Nurs. 28(7–8), 1216–1222 (2019).
Farenden, S., Gamble, D. & Welch, J. Impact of implementation of the National Early Warning Score on patients and staff. Br. J. Hosp. Med. (Lond). 78(3), 132–136 (2017).
Tirkkonen, J., Setälä, P. & Hoppu, S. Characteristics and outcome of rapid response team patients ≥75 years old: A prospective observational cohort study. Scand. J. Trauma Resusc. Emerg. Med. 25(1), 77 (2017).
Schultz, M. J. et al. Current challenges in the management of sepsis in ICUs in resource-poor settings and suggestions for the future. Intensive Care Med. 43(5), 612–624 (2017).
Blatteis, C. M. Age-dependent changes in temperature regulation—a mini review. Gerontology 58(4), 289–295 (2012).
Montecino-Rodriguez, E., Berent-Maoz, B. & Dorshkind, K. Causes, consequences, and reversal of immune system aging. J. Clin. Invest. 123(3), 958–965 (2013).
Norman, K., Pichard, C., Lochs, H. & Pirlich, M. Prognostic impact of disease-related malnutrition. Clin. Nutr. 27(1), 5–15 (2008).
Eccles, S. R., Subbe, C., Hancock, D. & Thomson, N. CREWS: Improving specificity whilst maintaining sensitivity of the National Early Warning Score in patients with chronic hypoxaemia. Resuscitation 85(1), 109–111 (2014).
Williams, B. The National Early Warning Score 2 (NEWS2) in patients with hypercapnic respiratory failure. Clin. Med. 19(1), 94 (2019).
Regitz-Zagrosek, V. & Kararigas, G. Mechanistic pathways of sex differences in cardiovascular disease. Physiol Rev. 97(1), 1–37 (2017).
Ngo, S. T., Steyn, F. J. & McCombe, P. A. Gender differences in autoimmune disease. Front. Neuroendocrinol. 35(3), 347–369 (2014).
Kander, M. C., Cui, Y. & Liu, Z. Gender difference in oxidative stress: A new look at the mechanisms for cardiovascular diseases. J. Cell Mol. Med. 21(5), 1024–1032 (2017).
Lee, B. Y. & Hong, S.-B. Rapid response systems in Korea. Acute Crit. care. 34(2), 108 (2019).
The Royal College of Emergency Physicians. Position Statement. National Early Warning Score (NEWS) for Adult Patients Attending Emergency Departments. https://www.rcem.ac.uk/docs/News/CEM10125-Position%20statement%20-%20NEWS%20for%20adult%20patients%20attending%20EDs%20-%20June%202016.pdf. Assessed 24 August 2021.
World Health Organization. ICD-11 for Mortality and Morbidity Statistics. https://icd.who.int/browse11/l-m/en. Assessed 24 August 2021.
Fluss, R., Faraggi, D. & Reiser, B. Estimation of the Youden Index and its associated cutoff point. Biometr. J. 47(4), 458–472 (2005).
Acknowledgements
The authors have no acknowledgments.
Author information
Authors and Affiliations
Contributions
Conceptualization: C.Y.L., M.L. Formal analysis, and Writing-original draft: S.H.K. Review and editing: H.S.C., E.S.J., H.C., H.L., S.L. Supervision, and validation: Y.K. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Kim, S.H., Choi, H.S., Jin, E.S. et al. Predicting severe outcomes using national early warning score (NEWS) in patients identified by a rapid response system: a retrospective cohort study. Sci Rep 11, 18021 (2021). https://doi.org/10.1038/s41598-021-97121-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-021-97121-w
This article is cited by
-
Improved inpatient deterioration detection in general wards by using time-series vital signs
Scientific Reports (2022)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
