
Abstract
Background
The prevalence of COVID-19 is different in studies conducted in different countries. The aim of this systematic review and meta-analysis is to estimate the pooled prevalence of COVID-19 in patients with MS.
Methods
Two independent researchers independently searched PubMed, Scopus, EMBASE, Web of Science, and google scholar along with gray literature up to April 2021. The search strategy included the MeSH and text words as (((coronavirus OR Wuhan coronavirus OR novel coronavirus OR coronavirus disease OR COVID-19 OR 2019 novel coronavirus infection OR 2019-nCOV OR severe acute respiratory syndrome coronavirus 2 OR SARS-CoV-2) AND (Multiple Sclerosis OR Sclerosis, Multiple) OR Sclerosis, Disseminated) OR Disseminated Sclerosis) OR MS (Multiple Sclerosis)) OR Multiple Sclerosis, Acute Fulminating).
Results
We found 1466 articles by literature search, and after deleting duplicates, 1029 remained. Twelve articles remained for meta-analysis. Totally, 101,462 patients were evaluated and the total number of possible/confirmed cases was 1394. Mean age ranged from 35 to 54 years. Totally, 49 patients died. The pooled prevalence of suspected COVID-19 in MS patients was 4% (95% CI: 3–4%) (I2 = 98.5%, P < 0.001). The pooled prevalence of hospitalization in infected cases was 10% (95% CI: 7–12%) (I2 = 95.6%, P < 0.001). The pooled prevalence of death in hospitalized cases was 4% (95% CI: 1–6%) (I2 = 82.4%, P < 0.001).
Conclusion
Hospitalization rate is higher among MS patients based on COVID-19 infection while the pooled infection rate is estimated as 4%.
Similar content being viewed by others

Introduction
COVID-19 (severe acute respiratory syndrome coronavirus 2 [SARSCoV-2]) disease infection is in pandemic stage and fever, dry cough, shortness of breath, hyposmia/anosmia, and hypogeusia/ageusia are among the common manifestations [1]. Concerns were raised for patients who received immunomodulatory or immunosuppressive medications such as patients with multiple sclerosis (MS) [2]. Based on mechanism of action of disease-modifying therapies (DMTs), risk of infection differs between MS cases [3]. Multiple Sclerosis International Federation (MSIF) declared that patients with MS should continue their medications during pandemic stage and in the case of positive COVID-19 tests or infection confirmation, they have to consult with the neurologist [4]. Overall, literature shows that MS patients are not at higher risk of severe infection and the rate of infection is not great [2]. Studies which were conducted in different countries reported different prevalence of COVID-19 infection in MS cases. So, we designed this systematic review and meta-analysis to estimate the pooled prevalence of COVID-19 in patients with MS.
Methods
Two independent researchers independently searched PubMed, Scopus, EMBASE, Web of Science, and google scholar along with gray literature up to April 2021.
The search strategy included the MeSH and text words as (((coronavirus OR Wuhan coronavirus OR novel coronavirus OR coronavirus disease OR COVID-19 OR 2019 novel coronavirus infection OR 2019-nCOV OR severe acute respiratory syndrome coronavirus 2 OR SARS-CoV-2) AND (Multiple Sclerosis OR Sclerosis, Multiple) OR Sclerosis, Disseminated) OR Disseminated Sclerosis) OR MS (Multiple Sclerosis)) OR Multiple Sclerosis, Acute Fulminating).
Inclusion criteria were cross-sectional studies and articles which had been published in the English language.
Exclusion criteria were cohort, case-report, and RCT studies.
We collected data regarding first author, country of origin, number of enrolled patients, number of possible/confirmed cases, mean age, F/M ratio, mean EDSS, mean duration of the disease, number of hospitalizations, ICU admissions, and death.
Risk of bias assessment
We evaluated the risk of potential bias by the Newcastle–Ottawa quality assessment scale (adapted for cross-sectional studies) [5]. It includes seven questions with the maximum total score of 10. The higher the score, the better the quality of the study.
Statistical analysis
All statistical analyses were performed using STATA (version 14.0; Stata Corp LP, College Station, TX, USA). We used random effects model.
To determine heterogeneity, inconsistency (I2) was calculated.
Results
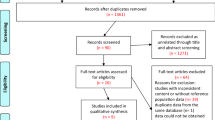
We found 1466 articles by literature search, after deleting duplicates 1029 remained. Eighteen articles remained for meta-analysis (Fig. 1).

Flow diagram summarizing the selection of eligible studies
Totally, 101,462 patients were evaluated and the total number of possible/confirmed cases was 1394.
Mean age ranged from 35 to 54 years. Totally, 49 patients died. The quality assessment score ranged between 4 and 10 (Table 1).
The pooled prevalence of suspected COVID-19 in MS patients was 4% (95% CI: 3–4%) (I2 = 98.5%, P < 0.001) (Fig. 2).

The pooled prevalence of COVID-19 in MS patients
The pooled prevalence of hospitalization in infected cases was 10% (95% CI: 7–12%) (I2 = 95.6%, P < 0.001) (Fig. 3).

The pooled prevalence of hospitalization in infected MS patients
The pooled prevalence of death in hospitalized cases was 4% (95% CI: 1–6%) (I2 = 82.4%, P < 0.001) (Fig. 4).

The pooled prevalence of death in infected MS patients
Discussion
To our knowledge, this is the first systematic review and meta-analysis of COVID-19 prevalence in MS patients.
The result of this systematic review and meta-analysis showed that the pooled prevalence of COVID-19 in MS patients is 4%. We also found that pooled hospitalization rate was 10%.
It is assumed that patients with MS are at higher risk of COVID-19 infection due to immunosuppressive or immune-modulatory agents administration while the pooled estimate and the point estimates of each study showed that the prevalence is not high in MS patients.
Conversely, the course of COVID-19 was not severe in affected cases and they had better outcome than the general population [9, 24]. Different factors such as age, disability status, immobility-related obesity, respiratory comorbidities, referring to medical center for magnetic resonance imaging, clinical visits, and laboratory examinations are considered to play role in COVID-19-related mortality and morbidity in MS patients [25].
It is reported that these patients follow quarantine rules strictly and they use masks and gloves regularly [26]. On the other hand, the first-line treatments for MS patients which are used widely are interferons (IFNs) and glatiramer acetate that are low-risk medications for MS treatment during this pandemic [25]. INFs are useful for inhibiting replication of the viruses which will be helpful for treating COVID-19 infection [27]. Anti-CD20 medications that deplete peripheral B cells are considered high-risk medications [2]. Sormani et al. found that severe infection mostly occurred in cases who were under treatment with anti-CD20 agents [28].
It is shown that patients who are under treatment with B-cell-depleting antibodies had higher risk of infection than others [9, 24].
MS patients who received B-cell-depleting agents were found to have higher rate of hospitalization in some studies [7, 9] while others believed that there is no relationship between type of medications and COVID-19 susceptibility [14].
As it is shown in Table 1, the rate of hospitalization and ICU admission was low among MS patients and four out of 570 suspected/confirmed patients died which is lower than the rate in healthy population. In Sahraian et al. study (the most number of patients) which was conducted in Iran, 4647 MS patients were evaluated, 68 were suspected/confirmed COVID-19 cases, and 17 were hospitalized while only 2 deaths were recorded [14]. The pooled estimate of hospitalization was found as 15%. In the study which was done by Ciampi et al., all suspected/confirmed cases were hospitalized but none of them died [8].
Parrotta et al. evaluated 76 suspected MS patients with COVID-19. They found 37 confirmed cases, 18 hospitalization (23.7%), and 6 (7.8%) related death [29]. Older age and progressive course of the disease were related with critical illness or death in these patients.
On the other hand, physicians are tended to hospitalize these patients more to observe MS patients carefully and do supportive care and treatments.
The results of included studies also show that the death rate was not high among infected MS patients and mortality rates were along with the general population [30, 31]. The pooled prevalence of death was 0 which ranged from 0 to 11%.
This systematic review and meta-analysis had some strengths. First, it is the first systematic review and meta-analysis. Second, we considered hospitalization and death rates.
Conclusion
Hospitalization rate is higher among MS patients based on COVID-19 while the pooled infection rate is estimated as 4%.
References
Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y et al (2020) Clinical features of patients infected with 2019 novel coronavirus in Wuhan China. Lancet 395(10223):497–506
Ghajarzadeh M, Bonavita S (2020) Are patients with multiple sclerosis (MS) at higher risk of COVID-19 infection? Neurol Sci 41(9):2315–2316
Luna G, Alping P, Burman J, Fink K, Fogdell-Hahn A, Gunnarsson M et al (2020) Infection risks among patients with multiple sclerosis treated with fingolimod, natalizumab, rituximab, and injectable therapies. JAMA Neurol 77(2):184–191
(https://www.msif.org/news/2020/02/10/thecoronavirus-and-ms-what-you-need-to-know/)
Modesti PA, Reboldi G, Cappuccio FP, Agyemang C, Remuzzi G, Rapi S et al (2016) Panethnic differences in blood pressure in Europe: a systematic review and meta-analysis. PloS one 11(1):e0147601
Ciampi E, Uribe-San-Martín R, Soler B, Fernández R, García P, Navarrete-Asenjo C, et al. (2020) COVID-19 in MS and NMOSD: A multicentric online national survey in Chile. Mult Scler Relat Disord 45:102392
Barzegar M, Mirmosayyeb O, Ghajarzadeh M, Nehzat N, Vaheb S, Shaygannejad V, et al. (2020) Mult Scler Relat Disord 45:102276
Ciampi E, Uribe-San-Martin R, Cárcamo C (2020) 2020 COVID-19 pandemic: the experience of a multiple sclerosis centre in Chile. Mult Scler Relat Disord 42:102204
Safavi F, Nourbakhsh B, Azimi AR (2020) B-cell depleting therapies may affect susceptibility to acute respiratory illness among patients with multiple sclerosis during the early COVID-19 epidemic in Iran. Mult Scler Relat Disord 43:102195
Crescenzo F, Marastoni D, Bovo C, Calabrese M (2020) Frequency and severity of COVID-19 in multiple sclerosis: a short single-site report from northern Italy. Mult Scler Relat Disord 44:102372
Dalla Costa G, Leocani L, Montalban X, Guerrero AI, Sørensen PS, Magyari M et al (2020) Real-time assessment of COVID-19 prevalence among multiple sclerosis patients: a multicenter European study. Neurol Sci 41(7):1647–1650
Moss BP, Mahajan KR, Bermel RA, Hellisz K, Hua LH, Hudec T et al (2020) <? covid19?> Multiple sclerosis management during the COVID-19 pandemic. Mult Scler J 26(10):1163–1171
Mantero V, Abate L, Balgera R, Basilico P, Salmaggi A, Cordano C (2020) Assessing the susceptibility to acute respiratory illness COVID-19-related in a cohort of multiple sclerosis patients. Mult Scler Relat Disord 46:102453
Sahraian MA, Azimi A, Navardi S, Ala S, Moghadasi AN (2020) Evaluation of the rate of COVID-19 infection, hospitalization and death among Iranian patients with multiple sclerosis. Mult Scler Relat Disord 46:102472
Vogel AC, Schmidt H, Loud S, McBurney R, Mateen FJ (2020) Impact of the COVID-19 pandemic on the health care of> 1,000 People living with multiple sclerosis: a cross-sectional study. Mult Scler Relat Disord 46:102512
Castillo Álvarez F, López Pérez MÁ, Marzo Sola ME (2020) Risk of SARS-CoV-2 infection and clinical outcomes in multiple sclerosis patients in La Rioja (Spain): Riesgo de infección por SARS-CoV-2 y resultados clínicos en pacientes con esclerosis múltiple en la Rioja (España). Med Clin (Engl Ed) 155(8):362–363
Evangelou N, Garjani A, Hunter R, Tuite-Dalton KA, Craig EM, Rodgers WJ, et al. (2020) Self-diagnosed COVID-19 in people with multiple sclerosis: a community-based cohort of the UK MS Register. J Neurol Neurosurg Psychiatry 92(1):107–109
Kovvuru S, Nalleballe K, Onteddu SR, Sharma R, Jasti M, Kapoor N et al (2021) Immunosuppression in chronic autoimmune neurological disorders during the COVID-19 pandemic. J Neurol Sci 420:117230
Reder AT, Centonze D, Naylor ML, Nagpal A, Rajbhandari R, Altincatal A et al (2021) COVID-19 in patients with multiple sclerosis: associations with disease-modifying therapies. CNS Drugs 35(3):317–330
Zabalza A, Cárdenas‐Robledo S, Tagliani P, Arrambide G, Otero‐Romero S, Carbonell‐Mirabent P, et al. (2020) COVID-19 in multiple sclerosis patients: susceptibility, severity risk factors and serological response. Eur J Neurol
Sepúlveda M, Llufriu S, Martínez-Hernández E, Català M, Artola M, Hernando A, et al. (2021) Incidence and Impact of COVID-19 in MS: A Survey From a Barcelona MS Unit. Neurol Neuroimmunol Neuroinflamm 8(2):e954
Moreno-Torres I, Meca-Lallana V, Costa-Frossard L, Oreja-Guevara C, Aguirre C, Alba Suarez E, et al (2020) editors. Risk and outcomes of COVID-19 in patients with multiple sclerosis in Madrid Spain. Multiple Sclerosis Journal: Sage Publications Ltd 1 Olivers Yard, 55 City Road, London EC1Y 1SP, England
Fernandes PM, O’Neill M, Kearns PK, Pizzo S, Watters C, Baird S et al (2020) Impact of the first COVID-19 pandemic wave on the Scottish Multiple Sclerosis Register population. Wellcome Open Res 5(276):276
Sormani MP (2020) An Italian programme for COVID-19 infection in multiple sclerosis. Lancet Neurol 19(6):481–482
Giovannoni G, Hawkes C, Lechner-Scott J, Levy M, Waubant E, Gold J (2020) The COVID-19 pandemic and the use of MS disease-modifying therapies. Mult Scler Relat Disord 39:102073
Sahraian MA, Gheini MR, Rezaeimanesh N, Ghajarzadeh M, NaserMoghadasi A (2020) Knowledge regarding COVID-19 pandemic in patients with multiple sclerosis (MS): a report from Iran. Mult Scler Relat Disord 42:102193
Totura AL, Baric RS (2012) SARS coronavirus pathogenesis: host innate immune responses and viral antagonism of interferon. Curr Opin Virol 2(3):264–275
Sormani MP, De Rossi N, Schiavetti I, Carmisciano L, Cordioli C, Moiola L et al (2021) Disease-modifying therapies and coronavirus disease 2019 severity in multiple sclerosis. Ann Neurol 89(4):780–789
Parrotta E, Kister I, Charvet L, Sammarco C, Saha V, Charlson RE, et al (2020) COVID-19 outcomes in MS: Observational study of early experience from NYU Multiple Sclerosis Comprehensive Care Center.Neurol Neuroimmunol Neuroinflamm 7(5):e835
Baud D, Qi X, Nielsen-Saines K, Musso D, Pomar L, Favre G (2020) Real estimates of mortality following COVID-19 infection. Lancet Infect Dis 20(7):773
Spychalski P, Błażyńska-Spychalska A, Kobiela J (2020) Estimating case fatality rates of COVID-19. Lancet Infect Dis 20(7):774–775
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical approval
None.
Conflict of interest
None.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Moghadasi, A.N., Mirmosayyeb, O., Barzegar, M. et al. The prevalence of COVID-19 infection in patients with multiple sclerosis (MS): a systematic review and meta-analysis. Neurol Sci 42, 3093–3099 (2021). https://doi.org/10.1007/s10072-021-05373-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10072-021-05373-1