
Abstract
Introduction
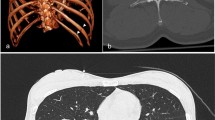
Management of major trauma patients with evidence of polytrauma involves the use of immediate whole-body CT (WBCT). Identification of patients appropriate for immediate WBCT remains challenging. Our study aimed to assess for improvement in patient selection for WBCT over time as a major trauma centre (MTC).
Methods
We conducted a retrospective study of patients who presented to our MTC during distinct two-month periods, one in 2013 and the other in 2017. Patients over 18 years of age who presented primarily following blunt trauma and activated a major trauma call were included. All patients underwent either immediate WBCT or standard ATLS workup. Those undergoing WBCT had the results of their scan recorded as positive or negative.
Results
A total of 516 patients were included, 232 from 2 months in 2013 and 284 from 2 months in 2017. There was no significant difference in the proportion of patients undergoing WBCT (61.6% vs 59.5%), selective CT (31.9% vs 32.4%) or no CT (6.5% vs 8.1%) between the cohorts. There was no improvement in the rate of negative WBCT observed between 2013 and 2017 (47.6% vs 39.6%, p = 0.17).
Conclusion
There was no improvement in patient selection for WBCT following trauma at our institution over a three-year period. Optimal patient selection presents an ongoing clinical challenge, with 39–47% of patients undergoing a scan demonstrating no injuries.



Similar content being viewed by others


References
American College of Surgeons Committee on Trauma (2012) Advanced trauma life support program for doctors, 9th edn. American College of Surgeons, Chicago
Leidner B, Adiels M, Aspelin P et al (1998) Standardized CT examination of the multitraumatized patient. Eur Radiol 8:1630–1638. https://doi.org/10.1007/s003300050601
Surendran A, Mori A, Varma DK, Gruen RL (2014) Systematic review of the benefits and harms of whole-body computed tomography in the early management of multitrauma patients: are we getting the whole picture? J Trauma Acute Care Surg 76:1122–1130. https://doi.org/10.1097/TA.0000000000000178
Sierink JC, Saltzherr TP, Reitsma JB et al (2012) Systematic review and meta-analysis of immediate total-body computed tomography compared with selective radiological imaging of injured patients. Br J Surg 99:52–58. https://doi.org/10.1002/bjs.7760
Healy DA, Hegarty A, Feeley I et al (2014) Systematic review and meta-analysis of routine total body CT compared with selective CT in trauma patients. Emerg Med J 31:101–108. https://doi.org/10.1136/emermed-2012-201892
Gordic S, Alkadhi H, Hodel S et al (2015) Whole-body CT-based imaging algorithm for multiple trauma patients: radiation dose and time to diagnosis. Br J Radiol 88:20140616. https://doi.org/10.1259/bjr.20140616
Ionising radiation: dose comparisons–GOV.UK. https://www.gov.uk/government/publications/ionising-radiation-dose-comparisons/ionising-radiation-dose-comparisons
Sierink JC, Treskes K, Edwards MJR et al (2016) Immediate total-body CT scanning versus conventional imaging and selective CT scanning in patients with severe trauma (REACT-2): a randomised controlled trial. Lancet 388:673–683. https://doi.org/10.1016/S0140-6736(16)30932-1
Linder F, Mani K, Juhlin C, Eklöf H (2016) Routine whole body CT of high energy trauma patients leads to excessive radiation exposure. Scand J Trauma Resusc Emerg Med 24:7. https://doi.org/10.1186/s13049-016-0199-2
Shannon L, Peachey T, Skipper N et al (2015) Comparison of clinically suspected injuries with injuries detected at whole-body CT in suspected multi-trauma victims. Clin Radiol 70:1205–1211. https://doi.org/10.1016/j.crad.2015.06.084
Major trauma centre|St George’s Healthcare services. https://www.stgeorges.nhs.uk/service/emergency-department/major-trauma-centre/
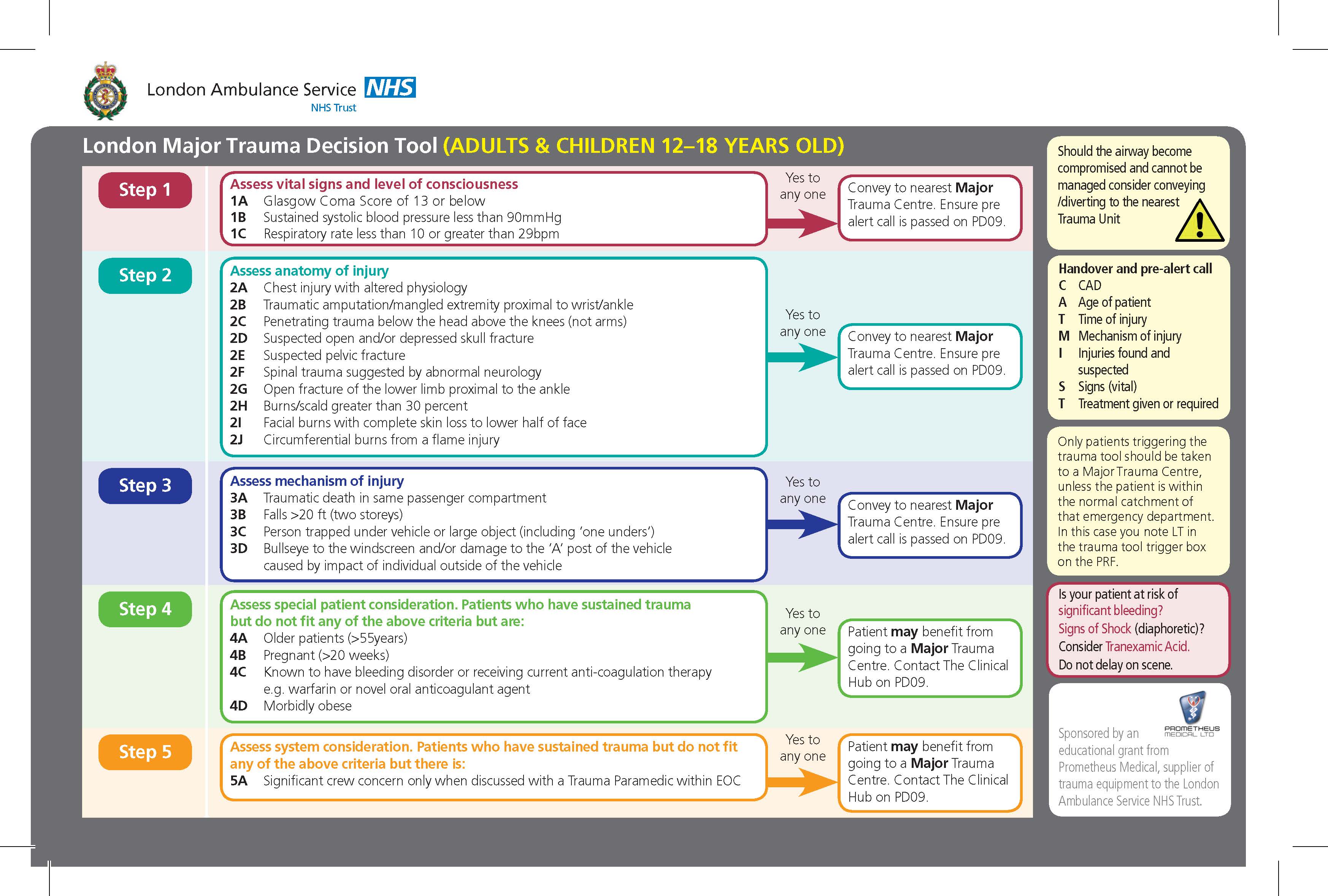
London Ambulance Service–London Major Trauma Decisions Tool (Adults & Children 12-18 years old). http://www.c4ts.qmul.ac.uk/downloads/trauma-triage-london-adult.jpg
Venugopal K, Kinghorn AF, Emordi CE et al (2012) An evaluation of the use of whole-body computed tomography in trauma patients at a United Kingdom trauma centre. Eur J Emerg Med 19:193–195. https://doi.org/10.1097/MEJ.0b013e32834ada14
Bingol O, Ayrık C, Kose A et al (2015) Retrospective analysis of whole-body multislice computed tomography findings taken in trauma patients. Turk J Emerg Med 15:116–121. https://doi.org/10.1016/j.tjem.2015.11.004
Brenner DJ, Elliston CD (2004) Estimated radiation risks potentially associated with full-body CT screening. Radiology 232:735–738. https://doi.org/10.1148/radiol.2323031095
Lawson CM, Daley BJ, Ormsby CB, Enderson B (2011) Missed injuries in the era of the trauma scan. J Trauma Inj Infect Crit Care 70:452–458. https://doi.org/10.1097/TA.0b013e3182028d71
Ptak T, Rhea JT, Novelline RA (2003) Radiation dose is reduced with a single-pass whole-body multi-detector row CT trauma protocol compared with a conventional segmented method: initial experience. Radiology 229:902–905. https://doi.org/10.1148/radiol.2293021651
Ptak T, Rhea JT, Novelline RA (2001) Experience with a continuous, single-pass whole-body multidetector CT protocol for trauma: the three-minute multiple trauma CT scan. Emerg Radiol 8:250–256. https://doi.org/10.1007/PL00011915
Geyer LL, Körner M, Harrieder A et al (2016) Dose reduction in 64-row whole-body CT in multiple trauma: an optimized CT protocol with iterative image reconstruction on a gemstone-based scintillator. Br J Radiol 89:20160003. https://doi.org/10.1259/bjr.20160003
Padole A, Ali Khawaja RD, Kalra MK, Singh S (2015) CT radiation dose and iterative reconstruction techniques. Am J Roentgenol 204:W384–W392. https://doi.org/10.2214/AJR.14.13241
Standards of practice and guidance for trauma radiology in severely injured patients Standards of practice and guidance for trauma radiology in severely injured patients, 2nd edn
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
P. Beak, B. Gabbott and M. Williamson declare that they have no conflict of interest to disclose. CB Hing reports personal fees from Elsevier, grants from ORUK, grants from Arthrex, grants from Stryker, grants from NIHR, outside the submitted work.
Ethical approval
This article does not contain any studies with human participants performed by any of the authors.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

{kind=link}
Cite this article
Beak, P., Gabbott, B., Williamson, M. et al. Four years of experience as a major trauma centre results in no improvement in patient selection for whole-body CT scans following blunt trauma. Eur J Orthop Surg Traumatol 30, 473–477 (2020). https://doi.org/10.1007/s00590-019-02592-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00590-019-02592-3