
Abstract
Purpose
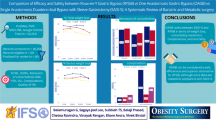
Compare primary single anastomosis duodeno-ileal bypass with sleeve gastrectomy (SADI-S) and two-stage SADI after sleeve gastrectomy (SG) in terms of weight loss, reduction/remission of comorbidities, and morbidity.
Methods
Retrospective study including 179 patients treated laparoscopically between 2016 and 2020. A 50Fr bougie was used for the SG in the primary SADI-S (group 1) and 36/40Fr for the two-stage procedure (group 2). The duodeno-ileal anastomosis was performed at 250 cm from the ileocecal valve and at least 2 cm after the pylorus.
Results
Mean age was 44.1 years old, and there were 148 women and 31 men. There were 67 (37.4%) patients in group 1 and 112 (62.6%) in group 2, with 67% completing the 4-year follow-up. Mean preoperative body mass index (BMI) was 51.1 kg/m2 and 44.6 kg/m2 for groups 1 and 2, respectively. Preoperative comorbidities were obstructive sleep apnea, hypertension, type 2 diabetes, and dyslipidemia in 103 (57.5%), 93 (52%), 65 (36.3%), and 58 (32.4%) of cases. At 4 years postoperatively, excess weight loss (EWL) was 67.5% in group 1 and 67% in group 2 (p = 0.1005). Both groups had good comorbidity remission rates. Early postoperative morbidity rate was 10.4% in group 1 and 3.6% in group 2. In group1, there were mostly postoperative intra-abdominal hematomas managed conservatively (n = 4). Two revisional surgeries were needed for duodeno-ileal anastomosis leaks. Postoperative gastroesophageal reflux disease (GERD), daily diarrhea, vitamin, and protein levels were similar in both groups.
Conclusion
Both types of strategies are efficient at short and mid-term outcomes. Preoperative criteria will inform surgeon decision between a primary and a two-stage strategy.
Graphical Abstract






Similar content being viewed by others


Data Availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
References
McKenna D, Selzer D, Burchett M, et al. Revisional bariatric surgery is more effective for improving obesity-related co-morbidities than it is for reinducing major weight loss. Surg Obes Relat Dis. 2014;10:654–9.
Yan J, Cohen R, Aminian A. Reoperative bariatric surgery for treatment of type 2 diabetes mellitus. Surg Obes Relat Dis. 2017;13:1412–21.
Aleassa EM, Hassan M, Hayes K, et al. Effect of revisional bariatric surgery on type 2 diabetes mellitus. Surg Endosc. 2019;33:2642–8.
Sánchez-Pernaute A, Herrera MAR, Pérez-Aguirre ME, et al. Single anastomosis duodeno-ileal bypass with sleeve gastrectomy (SADI-S) One to three-year follow-up. Obes Surg. 2010;20:1720–6.
Lazzati A. Epidemiology of the surgical management of obesity. J Visc Surg. 2023;160:S3-6.
Franken RJ, Sluiter NR, Franken J, et al. Treatment options for weight regain or insufficient weight loss after sleeve gastrectomy: a systematic review and meta-analysis. Obes Surg. 2022;32:2035–46.
Braghetto I, Csendes A, Lanzarini E. Is laparoscopic sleeve gastrectomy an acceptable primary bariatric procedure in obese patients? Early and 5-year postoperative results. Surg Laparosc Endosc Percutan Tech. 2012;22:479–86.
Brethauer SA, Kothari S, Sudan R, et al. Systematic review on reoperative bariatric surgery: American Society for Metabolic and Bariatric Surgery Revision Task Force. Surg Obes Relat Dis. 2014;10:952–72.
Ma P, Reddy S, Higa KD. Revisional bariatric/metabolic surgery: what dictates its Indications? Curr Atheroscler Rep. 2016;18:42.
Lazzati A, Bechet S, Jouma S, et al. Revision surgery after sleeve gastrectomy: a nationwide study with 10 years of follow-up. Surg Obes Relat Dis. 2020;16:1497–504.
O’Brien PE, Hindle A, Brennan L, et al. Long-term outcomes after bariatric surgery: a systematic review and meta-analysis of weight loss at 10 or more years for all bariatric procedures and a single-centre review of 20-year outcomes after adjustable gastric banding. Obes Surg. 2019;29:3–14.
Fischer L, Hildebrandt C, Bruckner T, et al. Excessive weight loss after sleeve gastrectomy: a systematic review. Obes Surg. 2012;22:721–31.
Pędziwiatr M, Małczak P, Wierdak M, et al. Revisional gastric bypass is inferior to primary gastric bypass in terms of short- and long-term outcomes—systematic review and meta-analysis. Obes Surg. 2018;28:2083–91.
Biertho L, Thériault C, Bouvet L, et al. Second-stage duodenal switch for sleeve gastrectomy failure: a matched controlled trial. Surg Obes Relat Dis. 2018;14:1570–9.
Surve A, Cottam D, Belnap L, et al. Long-term (> 6 Years) outcomes of duodenal switch (DS) versus single-anastomosis duodeno-ileostomy with sleeve gastrectomy (SADI-S): a matched cohort study. Obes Surg. 2021;31:5117–26.
Gebellí JP, Lazzara C, de Gordejuela AGR, et al. Duodenal switch vs. single-anastomosis duodenal switch (SADI-S) for the treatment of grade IV obesity: 5-year outcomes of a multicenter prospective cohort comparative study. Obes Surg. 2022;32:3839–46.
Topart P, Becouarn G. The single anastomosis duodenal switch modifications: a review of the current literature on outcomes. Surg Obes Relat Dis. 2017;13:1306–12.
Bashah M, Aleter A, Baazaoui J, et al. Single Anastomosis duodeno-ileostomy (SADI-S) versus one anastomosis gastric bypass (OAGB-MGB) as revisional procedures for patients with weight recidivism after sleeve gastrectomy: a comparative analysis of efficacy and outcomes. Obes Surg. 2020;30:4715–23.
Zaveri H, Surve A, Cottam D, et al. Mid-term 4-year outcomes with single anastomosis duodenal-ileal bypass with sleeve gastrectomy surgery at a single US center. Obes Surg. 2018;28:3062–72.
Surve A, Cottam D, Medlin W, et al. Long-term outcomes of primary single-anastomosis duodeno-ileal bypass with sleeve gastrectomy (SADI-S). Surg Obes Relat Dis. 2020;16:1638–46.
Verhoeff K, Mocanu V, Zalasky A, et al. Evaluation of metabolic outcomes following SADI-S: a systematic review and meta-analysis. Obes Surg. 2022;32:1049–63.
Mocanu V, Dang J, Ladak F, et al. Predictors and outcomes of bleed after sleeve gastrectomy: an analysis of the MBSAQIP data registry. Surg Obes Relat Dis. 2019;15:1675–81.
Rohm TV, Meier DT, Olefsky JM, et al. Inflammation in obesity, diabetes, and related disorders. Immunity. 2022;55:31–55.
Mocanu V, Wilson H, Verhoeff K, et al. Role of tranexamic acid (TXA) in preventing bleeding following sleeve gastrectomy: a systematic review and meta-analysis. Obes Surg. 2023;33:1571–9.
El Moussaoui I, Limbga A, Mehdi A. Staple line reinforcement during sleeve gastrectomy with a new type of reinforced stapler. Minerva Chir. 2018;73:127–32.
Ghosh SK, Roy S, Chekan E, et al. A narrative of intraoperative staple line leaks and bleeds during bariatric surgery. Obes Surg. 2016;26:1601–6.
Sánchez-Pernaute A, Herrera MÁR, Ferré NP, et al. Long-term results of single-anastomosis duodeno-ileal bypass with sleeve gastrectomy (SADI-S). Obes Surg. 2022;32:682–9.
Acknowledgements
The authors would like to thank Miguel Chagnon, Statistics Consultation Service, University of Montreal and Kathleen Beaumont for editing and manuscript review.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical Approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent does not apply to this retrospective review of a prospectively collected database.
Conflict of Interest
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Key points
• SADI-S showed good weight loss at 4 years PO as a primary or two-stage surgery.
• Primary/two-stage SADI-S is efficient for resolution/remission of comorbidities.
• Primary SADI-S is possible for BMI 50-60 and well-controlled comorbidities.
• Two-stage SADI-S is indicated for non-responders to SG or for BMI above 60.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Deffain, A., Denis, R., Pescarus, R. et al. Single Anastomosis Duodeno-Ileal bypass (SADI-S) as Primary or Two-Stage Surgery: Mid-Term Outcomes of a Single Canadian Bariatric Center. OBES SURG 34, 1207–1216 (2024). https://doi.org/10.1007/s11695-024-07095-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-024-07095-7