
Abstract
The mysterious death of Mr. Alexander Litvinenko who was most possibly poisoned by Polonium-210 (210Po) in November 2006 in London attracted the attention of the public to the kinetics, dosimetry and the risk of this high radiotoxic isotope in the human body. In the present paper, the urinary excretion of seven persons who were possibly exposed to traces of 210Po was monitored. The values measured in the GSF Radioanalytical Laboratory are in the range of natural background concentration. To assess the effective dose received by those persons, the time-dependence of the organ equivalent dose and the effective dose after acute ingestion and inhalation of 210Po were calculated using the biokinetic model for polonium (Po) recommended by the International Commission on Radiological Protection (ICRP) and the one recently published by Leggett and Eckerman (L&E). The daily urinary excretion to effective dose conversion factors for ingestion and inhalation were evaluated based on the ICRP and L&E models for members of the public. The ingestion (inhalation) effective dose per unit intake integrated over one day is 1.7 × 10−8 (1.4 × 10−7) Sv Bq−1, 2.0 × 10−7 (9.6 × 10−7) Sv Bq−1 over 10 days, 5.2 × 10−7 (2.0 × 10−6) Sv Bq−1 over 30 days and 1.0 × 10−6 (3.0 × 10−6) Sv Bq−1 over 100 days. The daily urinary excretions after acute ingestion (inhalation) of 1 Bq of 210Po are 1.1 × 10−3 (1.0 × 10−4) on day 1, 2.0 × 10−3 (1.9 × 10−4) on day 10, 1.3 × 10−3 (1.7 × 10−4) on day 30 and 3.6 × 10−4 (8.3 × 10−5) Bq d−1 on day 100, respectively. The resulting committed effective doses range from 2.1 × 10−3 to 1.7 × 10−2 mSv by an assumption of ingestion and from 5.5 × 10−2 to 4.5 × 10−1 mSv by inhalation. For the case of Mr. Litvinenko, the mean organ absorbed dose as a function of time was calculated using both the above stated models. The red bone marrow, the kidneys and the liver were considered as the critical organs. Assuming a value of lethal absorbed dose of 5 Gy to the bone marrow, 6 Gy to the kidneys and 8 Gy to the liver, the amount of 210Po which Mr. Litvinenko might have ingested is therefore estimated to range from 27 to 1,408 MBq, i.e 0.2–8.5 μg, depending on the modality of intake and on different assumptions about blood absorption.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Polonium-210 (210Po) is a natural radionuclide which decays to 206Pb, emitting alpha particles with energy of 5.3044 (100%) and 4.5166 MeV (0.00122%) [1]. The half-life of 210Po is 138.376 days [1], which corresponds to a specific activity of 1.66 × 1014 Bq g−1. High amounts of pure 210Po activity can be produced by three ways: the activation of 209Bi (natural abundance 100%) with thermal neutrons (cross section σ = 0.034 barn), the separation from 222Rn daughter nuclides emanated from 226Ra, and the separation from Pb–Bi alloy coolants of some fast neutron reactors.
210Po is a decay daughter of 210Pb in 238U decay chain of the uranium series; it occurs in the uranium ores and exists ubiquitously in the environment. According to the United Nations Scientific Committee on the Effects of Atomic Radiation (UNSCEAR) [2], the concentration of 210Po in air is reported to be from 10 to 80 μBq m−3 with a reference value of 50 μBq m−3; the annual intake of the public ranges from 18 Bq in South America to 220 Bq in Asia with a reference value of 58 Bq. Through inhalation and diet 210Po is accumulated in the human body, its concentration in human tissues is 200 mBq kg−1 in lungs, 600 mBq kg−1 in liver, 600 mBq kg−1 in kidneys, 100 mBq kg−1 in muscle and other tissues, and 2,400 mBq kg−1 in bone. However, these body contents are reference values, they vary between individuals. The presence of 210Po in tobacco greatly increases the intake of this radionuclide by smokers. Recently, Desideri et al. [3] reported that in Italy smokers who smoke 20 cigarettes per day inhale, on average, 79.5 mBq of 210Po daily; those smokers concomitantly inhale the same amount of radioactivity from 210Pb. The measured 210Po concentration in lung parenchyma of smokers is about three times that of non-smokers [4]. Hill reported a higher content of 210Po in kidneys, liver, lungs, and gonads for smokers compared to non-smokers [5].
With regard to daily excretion, Glöbel et al. [6] reported in 1966 the measurements in one German subject to be in the range of 40.7–351.5 mBq in feces and 2.2–37 mBq in urine. Naumann et al. [7] reported daily urinary excretion ranging from 2.8 (detection limit of 2 mBq l−1 with urinary excretion of 1.4 l d−1) to 9.9 mBq d−1 in Berlin area. Dalheimer et al. [8] recently reported a daily urinary excretion median value of 3.5 mBq d−1 for non-smokers and 6.6 mBq d−1 for smokers. In Brazil, the reported values of 210Po excretion in urine were 5.2 mBq l−1 for non-smokers and 9.8 mBq l−1 for smokers [9, 10]. In Saudi Arabia, the measured values range from 1.5 to 10 mBq l−1 for non-smokers and 3.3 to 15.9 mBq l−1 for smokers [11].
According to the model recommended by the International Commission on Radiological Protection (ICRP), about 10–50% of ingested 210Po is absorbed by the intestine and flows into the bloodstream and mostly deposits in the liver, kidneys, spleen, red bone marrow and other tissues [12]. To distinguish between ingestion of the organic and inorganic forms of polonium, ICRP recommended an f 1 value of 0.1 for workers and 0.5 for members of the public [12]. For intake by inhalation, ICRP recommended an f 1 value of 0.1 for workers and members of the public inhaling the material of Type F (fast absorption into blood) and M (moderate absorption into blood) [13, 14], an f 1 value of 0.01 was used for members of the public inhaling the material of Type S (slow absorption into blood) [14]. The effective dose coefficients of 210Po for adult members of the public recommended by ICRP are 1.2 × 10−6 Sv Bq−1 for ingestion calculated with an f 1 value of 0.5, and 3.3 × 10−6 Sv Bq−1 for inhalation assuming a material of Type M with an f 1 value of 0.1 [14].
As reported in the media, Mr. Alexander Litvinenko died 23 days (the 23rd of November 2006 was included) after he was possibly poisoned by 210Po. In this context, the organ absorbed doses in the days following, say from days 1 to 30, after acute intake of 210Po are important for intake lethal dose estimation. The equivalent dose and effective dose coefficients are needed for the effective dose and the risk assessments of other probably contaminated members of the public.
In the present work, the daily urinary and fecal excretions, the time-dependence of the equivalent dose and the effective dose from 1 to 1,000 days after acute ingestion and inhalation of 1 Bq of 210Po were calculated using the biokinetic model for polonium recommended by ICRP [12] and the model recently developed by Leggett and Eckerman (L&E) [15]. These modeled excretions and dose coefficients can be used for the estimate of intake and the risk assessment, provided that the 210Po urinary or other excreta data are available from the people who were potentially contaminated in this 210Po accident. The GSF Radioanalytical Laboratory measured urine samples of seven German subjects who were suspected to have been exposed to traces of 210Po in the aftermath of the poisoning of Mr. Litvinenko. Those measured results and the calculated conversion factors of the daily urinary excretion to effective dose are applied to assess the effective dose for those persons. In order to estimate the possible intake of 210Po and organ dose for Mr. Litvinenko, the mean organ absorbed dose was calculated applying the two above-mentioned models. The results obtained using ICRP and L&E models are compared and critically discussed.
Materials and methods
Experimental measurement of urinary excretion of 210Po
Seven persons (5 male and 2 female) aged from 23 to 48 years from Germany provided their 24-h-urine samples in December 2006. Among those persons only one was a smoker. Information on the suspected day of exposure to 210Po was also acquired. Samples were measured between 6 and 12 days after the possible exposure. The complete 24-h-urine samples were transferred into appropriate glass beakers. The sampling containers were washed twice with 20 ml 9 M HCl. The washing solutions were added to the samples. About 160 mBq 208Po yield tracer and 1 g ascorbic acid per liter urine were added. Polonium was deposited onto copper discs (20 h, 20°C). The urine was discarded and the discs were rinsed with water and isopropanole. The polonium isotopes were determined by alpha spectrometry with Canberra PIPS detectors in vacuum chambers. The spectra were evaluated with Eurisys Interwinner Software. The analytical procedure was last validated by participating in the IAEA proficiency test IAEA-CU-2007-09 on the determination of 210Po in water.
Biokinetic model of 210Po
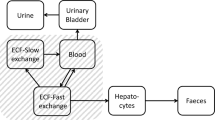
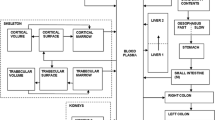
The ICRP and L&E systemic biokinetic models of polonium [12, 15], coupled with the gastrointestinal tract model of ICRP Publication 30 [16] and the respiratory tract model of ICRP Publication 66 [17], were used to calculate the retentions of 210Po in organs or tissues after incorporation. In the ICRP model, a fraction of 30, 10, 5, 10, and 45% of polonium entering into the systemic circulation is deposited in the liver, kidneys, spleen, red marrow and the rest of the body, respectively. It is retained in those organs with a half-life of 50 days. A ratio of 1:2 between the urinary and fecal excretions is assumed for systemic polonium [12]. Recently, an improved, physiologically realistic systemic biokinetic model for polonium in humans was constructed by Leggett and Eckerman based on the data identified to most likely represent the typical behavior of polonium in laboratory animals and human subjects [15]. In contrast to the current ICRP model, the new proposed model enables one to predict the excretion of polonium in human hair and sweat. In addition, a compartment representing the bone surface was integrated into the model of polonium. The urinary excretion pathway is more physiologically realistic than the current ICRP model. Therefore, the new model is expected to provide a more reliable estimation of the intake and the effective dose from the measured urinary excretion data.
Dose calculation of 210Po after ingestion and inhalation
The average organ absorbed dose, D T , in an organ or a tissue T, due to nuclear transformations, U S , of a radionuclide in various source organs S, is calculated applying the methodology developed by the Medical Internal Radiation Dose (MIRD) Committee [18]: \( D_{T} = {\sum\limits_s { \ifmmode\expandafter\tilde\else\expandafter\sim \fi{A}_{S} \times S{\left( {T \leftarrow S} \right)}} }, \) where \( \ifmmode\expandafter\tilde\else\expandafter\sim \fi{A}_{S} \) is the time-integrated, or cumulated activity, and is equal to the number of transformations U S in S; S(T ← S) is the absorbed dose in T per unit cumulated activity in S. The equivalent dose, H T , is given by summing the product of U S and the specific effective energy [SEE(T ← S)] over all source organs, S [19]. In the values of the specific effective energy each type of radiation is weighted by a given radiation weighting factor, which accounts for the different effectiveness in inducing late effects.
The U S of the radionuclide in the source organ or tissue was obtained by integrating the retention function, which was modeled by the SAAM II program (University of Washington, Seattle, WA). The values of S(T ← S) and SEE(T ← S) were calculated by using the SEECAL program [20]. The effective dose, E, was calculated by the sum of the product of the equivalent dose, H T and the corresponding tissue weighting factor, w T , over 12 organs and tissues (T) and the product between the equivalent dose of the so called remainder tissue, H rem, and its weighting factor, w rem [19, 21]. The equivalent dose of the colon, H colon, was calculated as 0.57 × H ULI + 0.43 × H LLI, where H ULI and H LLI are the equivalent doses in the walls of the upper large intestine (ULI) and the lower large intestine (LLI), respectively [19]. The dose of thymus is taken as a surrogate for the oesophagus, in absence of a dosimetric model for the oesophagus [12]. For the lungs, the apportionment factors for target cells in different lung regions recommended by ICRP were used [17].
Results and discussion
Firstly, the measured 210Po urinary excretion is presented. Secondly, the time-dependent organ equivalent dose, effective dose, organ absorbed dose and daily excretion in urine and in feces, in hair and sweat after acute ingestion and inhalation of 210Po are shown. The average values of body content and daily excretion of 210Po for the normal unexposed public are estimated. Finally, the effective doses for the possibly contaminated seven subjects are predicted. The amount of 210Po Mr. Litvinenko probably ingested are estimated and discussed based on different assumptions.
Measured 210Po urinary excretion
Figure 1 shows one alpha spectrum of the samples. The 208Po tracer contained some 209Po impurities. However, this did not interfere with the determination of 210Po. In Table 1, the 210Po activities (±1 combined standard uncertainty) of seven 24-h-urine samples are shown. Daily urinary excretion ranged from 3.3 to 26.4 mBq d−1, with a mean value of 11.3 mBq d−1. All these values are in the range of natural levels, and below the reported level of 30 mBq d−1 set by the Health Protection Agency (HPA) [22].

Alpha spectrum of 208/209/210Po isolated from one 24-h-urine sample. 209Po is an impurity of the 208Po tracer
210Po organ equivalent dose and effective dose after acute intake
The equivalent and effective doses per unit intake for members of the public and for workers after acute ingestion and inhalation using both the ICRP and L&E models are presented in Fig. 2. The time-dependent equivalent and effective doses incline to a constant value after 300 days of acute intake. The effective dose coefficient for inhalation is generally higher than for ingestion. The organ equivalent doses of public are higher than that of workers because the f 1 value of 0.5 recommended for the members of the public is higher than the value of 0.1 for workers.

Time-dependence of organ equivalent dose and effective dose coefficient after acute ingestion and inhalation for members of the public and the workers by using the systemic models recommended by ICRP [12] and the model developed recently by Leggett and Eckerman (L&E) [15], combining the gastrointestinal tract and the human respiratory tract models [16, 17]. The line legend symbols, which are shown in the figure, are applicable for the others. The title of “ICRP Public/Workers Ingestion/Inhalation” represents the ICRP model for members of the public/the workers by ingestion/inhalation
By inhalation, the total deposition of inhaled aerosols in the whole respiratory tract for workers is 1.7 times higher than that of the public. However, for workers, about 74% of the total inhaled aerosols are assumed to be deposited in the extrathoracic (ET) region, which gives less contribution to the resulting dose coefficient, in comparison to the public, for which only 32% is assumed to be deposited in ET region. The deposition in the alveolar–interstitial (AI) region of the lungs for public is two times higher than that for the workers [17]. Therefore, the dose coefficient of the lungs is higher for the public. This higher equivalent dose in lungs makes a slightly higher effective dose for the public.
For most organs, e.g. kidneys, liver, red marrow and spleen, the organ equivalent dose calculated using the ICRP model is generally higher than that by the L&E model. By inhalation, the lung doses are the main contribution to the effective dose and they are almost identical between the two models. Anyway, the effective doses by the two models show a smaller discrepancy than the change in organ equivalent doses. For members of the public, the effective dose coefficients range from 1.7 × 10−8 Sv Bq−1 on the first day, 2.0 × 10−7 Sv Bq−1 on the 10th day, 5.2 × 10−7 Sv Bq−1 on the 30th day, to a constant value of 1.2 × 10−6 Sv Bq−1 in the later days for acute ingestion; and 1.4 × 10−7, 9.6 × 10−7, 2.0 × 10−6, 3.3 × 10−6 Sv Bq−1 for acute inhalation on the same mentioned days with the ICRP model, respectively.
210Po mean organ absorbed dose after acute intake
In order to assess deterministic effects of exposure to 210Po, organ absorbed dose was also calculated. The time-dependence of the organ absorbed dose after acute intake of 210Po is shown in Fig. 3. Because 210Po is an alpha emitter (negligible contribution to dose from gamma ray), the organ absorbed doses are 20 times smaller than the corresponding values of the organ equivalent dose since a radiation weighting factor of 20 for alpha particles is applied in calculating the organ equivalent dose. The highest organ absorbed doses are in the kidneys after intake for ingestion, and in the lungs after inhalation. Doses to members of the public are generally higher than for workers; the L&E model gives lower estimates than the ICRP model. The dose absorbed by the red marrow per unit ingestion (inhalation), calculated using the ICRP model for members of the public, is 1.5 × 10−3 (1.4 × 10−4) Gy MBq−1 at 1 day after incorporation, 2.2 × 10−2 (2.1 × 10−3) Gy MBq−1 at 10 days, 5.7 × 10−2 (6.0 × 10−3) Gy MBq−1 at 30 days, and 1.1 × 10−1 (1.5 × 10−2) Gy MBq−1 at 100 days, respectively.

Time-dependence of mean organ absorbed dose after acute ingestion and inhalation for members of the public and the workers by using the systemic models recommended by ICRP [12] and the model developed recently by Leggett and Eckerman (L&E) [15], combining the gastrointestinal tract and the human respiratory tract models [16, 17]. The line legend symbols, which are shown in the figure, are applicable for the others. The title of “ICRP Public/Workers Ingestion/Inhalation” represents the ICRP model for members of the public/the workers by ingestion/inhalation
210Po daily excretion in urine and in feces after acute intake
The predicted daily excretions in urine and in feces, by using both models, are shown in Fig. 4. The lower intestinal absorption, assumed for the workers, results in a higher value in their fecal excretions. For both the public and the workers, the daily urinary and fecal excretions by ingestion are much higher than that by inhalation. By means of the L&E model, the excretion of 210Po in human hair and sweat could be used to estimate the intake and the level of 210Po in the human body, provided that the measured amount of 210Po in hair is available. However, it is not obvious to assess the intake and level of 210Po in the body from hair measurements because their results are highly dependent on modality of sample collection and because the model does not discriminate between excretion into sweat and hair. In the first few days after incorporation, the amount of 210Po excreted in urine is markedly higher than that in hair and sweat (of a factor up to 25 times). This factor is predicted to be smaller at later times, reaching about the value of 1 approximately 100 days after intake.

Daily urinary and fecal excretions for members of the public and the workers after acute ingestion and inhalation of 1 Bq of 210Po by using the systemic models recommended by ICRP [12] and the model developed recently by Leggett and Eckerman [15], coupled with the gastrointestinal tract and the human respiratory tract models [16, 17]
By using the ICRP model, the predicted daily urinary excretions of 210Po for members of the public are 1.1 × 10−3 Bq d−1 on the first day, 2.0 × 10−3 Bq d−1 on the 10th day, 1.3 × 10−3 Bq d−1 on the 30th day and 3.6 × 10−4 Bq d−1 on the 100th day after acute ingestion of 1 Bq of 210Po; and 1.0 × 10−4, 1.9 × 10−4, 1.7 × 10−4 and 8.3 × 10−5 Bq d−1 on same mentioned days after acute inhalation, respectively.
210Po dose conversion factor of daily urinary excretion to effective dose
To enable an easy calculation of the effective dose for the persons whose urinary excretion were measured, the daily urinary excretion to effective dose conversion factor were calculated based on the ICRP and L&E models. They are tabulated in Table 2. There are two kinds of conversion factors presented in Table 2, namely, E/U and E’/U, where E is the effective dose coefficient, as defined and recommended by ICRP; E’ is the effective dose by the time T after intakes. In the earlier days, the factor E/U is larger than E’/U, however, after 300 days from intake, those two factors reach the same value. For example, if one has inhaled 1 Bq of 210Po, according to the ICRP model for members of the public, the resulting effective dose E’ is 1.4 × 10−7 by T = 1 day, 2.0 × 10−6 by T = 30 days and 3.3 × 10−6 Sv Bq−1 by T = 50 years. The effective dose E’ released at the time of urine collection can be estimated. It represents approximately the lower limits of dose released by 210Po in the earlier days. Since measurements were generally conducted few days after sampling, the results of the activity measurements in urine needed to be corrected for radioactive decay in order to obtain the actual activity value at the day of urine collection.
210Po body content and urinary and fecal excretion for normal unexposed people
According to the average concentration of 210Po in the foodstuffs and in the air reported by UNSCEAR [2], the normal unexposed person ingests 0.16 Bq and inhales 1 mBq of 210Po each day. Applying the ICRP model for members of the public, the content of 210Po in human body is predicted to be about 1.1 Bq. It is estimated that about 4 mBq in urine and 0.15 Bq in feces could be found daily. These results are in excellent agreement with the experimental values reported in the literature [6–11, 22, 23].
Internal dose assessment for the monitored subjects
Although the measured excreted activities were comparable to the natural levels, and below the threshold set by the HPA to identify individuals probably exposed to 210Po from the London incident [22], effective doses were nonetheless calculated under the pessimistic assumption that the measured activities were actually due to an acute intake on the day of suspected exposure to 210Po. In Table 1 the values of committed effective dose E (over 50 years) and E′ (till the day of sample collection) are presented as estimated from the results of the measurements in urine. The intakes of inhalation and ingestion were assumed separately. As samples were collected only few days after the suspected exposure, the estimate of the effective dose E′ is much lower than the value of E. Considering the values of E as conservative estimates of the exposures of the monitored subjects, it can be seen that the resulting effective doses range from 2.1 × 10−3 to 1.7 × 10−2 mSv by ingestion, and from 5.5 × 10−2 to 4.5 × 10−1 mSv by inhalation. Even under the very restrictive and pessimistic assumptions used for these evaluations, the dose received would be considered to represent the natural background radiation dose contributed from 210Po.
Estimating 210Po intake for Mr. Alexander Litvinenko
As reported in the media, Mr. Litvinenko was most possibly poisoned on 1 November 2006 and died 23 days later on 23 November at 21:21 o’clock. From the available information, it is possible to assume that polonium was administered orally, and that multiple organ failure, probably connected with bone marrow syndrome, was responsible for the death of Mr. Litvinenko.
As Harrison et al. [24] pointed out, animal studies showed that multiple organ damages were the cause of deaths within few weeks from intake of 210Po. The results of the biokinetic modeling presented above indicated that kidneys, liver and red marrow could be the critical organs, being among the organs with the highest absorbed dose coefficients. According to the data presented by Harrison et al. [24], the lethal dose LD50 may be estimated as about 3–4 Gy for the bone marrow syndrome, 6 Gy for acute kidneys damage and 8 Gy for acute liver damage. An LD100 of 5 Gy for red marrow syndrome is also given. Those values were calculated for internal irradiation from 210Po, taking into account relative biological effectiveness (RBE) of alpha particles and dose protraction. The absorbed dose of 5 Gy to red marrow, 6 Gy to kidneys and 8 Gy to liver were applied as a basis on the organ lethal dose in this work to estimate the possible intake of 210Po by Mr. Litvinenko.
The organ absorbed dose coefficients were calculated for day 23 after ingestion (the day of 23 November was included as full day in the calculations) in the present work. The resulting dose coefficients are 4.6 × 10−2 (1.8 × 10−2) Gy MBq−1 for red bone marrow, 2.2 × 10−1 (1.3 × 10−1) Gy MBq−1 for kidneys, 1.1 × 10−1 (8.5 × 10−2) Gy MBq−1 for liver with ICRP (L&E) model, assuming an f 1 value of 0.5; and 9.2 × 10−3 (3.6 × 10−3) Gy MBq−1 for red bone marrow, 4.4 × 10−2 (2.6 × 10−2) Gy Bq−1 for kidneys, 2.3 × 10−2 (1.7 × 10−2) Gy MBq−1 for liver assuming an f 1 value of 0.1.
The estimation of possible intake of 210Po is summarized in Table 3. Both of the ICRP and L&E models were used. According to different f 1 values of 0.5 and 0.1, the estimated amounts of 210Po range from 27 to 1,408 MBq, corresponding to 0.2 to 8.5 μg. Moreover, the organ absorbed doses, calculated after an incorporation of estimated amount of 210Po assuming the red bone marrow as a critical organ with an absorbed dose of 5 Gy, are presented in Table 4. In their paper, Harrison et al. [24] concluded that 0.1–0.3 GBq or more absorbed to blood of an adult male is likely to be fatal within 1 month. This range would correspond to an intake of 200–600 MBq assuming 50% absorption to blood and to 1–3 GBq assuming 10% absorption to blood, respectively. These values are consistent with the estimates obtained in the present work.
Conclusions
In this work, the time-dependent organ equivalent dose, effective dose and daily excretion in urine and in feces after an acute intake of 210Po are calculated by applying the models of polonium recommended by ICRP and the new model developed recently by Leggett and Eckerman. The conversion factors from the daily urinary excretion to the effective dose were evaluated. Moreover, the 24-h-urine samples of seven persons who were possibly contaminated were measured in the GSF Radioanalytical Laboratory. Their measured excretions resulted within the natural level of the excretion rate of 210Po, and below the threshold limit value of 30 mBq d−1 recommended by the HPA to identify individuals probably exposed to 210Po from the London incident. The effective dose was estimated for those seven persons using their measured urinary excretion and the calculated conversion factors. They were in the range of 2.1 × 10−3 to 1.7 × 10−2 mSv assuming an intake by ingestion, and 5.5 × 10−2 to 4.5 × 10−1 mSv by inhalation. They are much lower than the mean effective dose of 2.4 mSv to the population in the federal republic of Germany during the year 2005 [25]. From the fact that the measured results were within the natural level of the excretion rate of 210Po, it is concluded that no additional 210Po intake can be detected. Thus, no excess health effects related to the toxicity of 210Po are expected for those monitored subjects besides the background exposure to the natural level of 210Po. In addition, the time-dependent mean organ absorbed dose was calculated with the ICRP and L&E models. Based on these calculated organ absorbed doses, and different assumptions on lethal absorbed doses for red bone marrow, kidneys, liver, and on blood absorption, the minimum estimated amount of 210Po which led to the death of Mr. Alexander Litvinenko in November 2006 in London is estimated to range from 27 to 1,408 MBq, about 0.2 to 8.5 μg, if only 210Po was used as a poison.
References
Firestone RB (1996) Table of isotopes, 8th CD-ROM edn. Wiley, New York
United Nations (2000) Sources and effects of ionizing radiation: 2000 report to the general assembly, with scientific annexes, vol 1, Annex B. United Nations Scientific Committee on the Effects of Atomic Radiation, United Nations, New York
Desideri D, Meli MA, Feduzi L, Roselli C (2007) 210Po and 210Pb inhalation by cigarette smoking in Italy. Health Phys 92:58–63
Rajewsky B, Stahlhofen W (1966) Polonium-210 activity in the lungs of cigarette smokers. Nature 209:1312–1313
Hill CR (1965) Polonium-210 in man. Nature 208:423–428
Glöbel B, Muth H, Oberhausen E (1966) Aufnahme und Ausscheidung der natürlichen Radionuklide 210Pb und 210Po durch den Menschen. Strahlentherapie 131:218–226
Naumann M, Hänisch K, Hartmann M (1998) Levels of natural radionuclides in human excreta in the Berlin area. Radiat Prot Dosim 79:197–200
Dalheimer A, König K, Noßke D, Schäfer I (2007) Der Hamburger Poloniumfall aus sicht der Inkorporations-Überwachung. In: Bayer A, Faleschini H, Krüger S, Strobl Chr (Bandherausgeber) Vorkehrungen und Massnahmen bei Radiologischen Ereignissen. 5. Seminar des Arbeitskreises Notfallschutz. Augsburg, 25. bis 27. April 2007. Bericht Nr. FS-07–142-AKN. Publikationsreihe Fortschritte im Strahlenschutz. Fachverband für Strahlenschutz e.V., TÜV Media GmbH, Köln, pp 82–88
Lipsztein JL, Melo DR, Sousa W, Dias da Cunha KM, Azeredo AMG, Julião L, Santos M (2003) Norm workers: a challenge for internal dosimetry programmes. Radiat Prot Dosim 105:317–320
Santos PL, Gouvea RC, Dutra IR (1994) Concentrations of 210Pb and 210Po in hair and urine of workers, of the uranium mine at Pocos de Caldas (Brazil) Sci Total Environ 148:61–65
Al-Arifi MN, Alkarfy KM, Al-Suwayeh SA, Aleissa KA, Shabana EI, Al-Dhuwaili AA, Al-Hassan MI (2006) Levels of 210Po in blood, urine and hair of some Saudi smokers. J Radioanal Nucl Chem 269:115–118
ICRP (1993) Age-dependent doses to members of the public from intake of radionuclides: Part 2 ingestion dose coefficients. Annals of ICRP 23 (3/4). Pergamon, Oxford
ICRP (1994) Dose coefficients for intakes of radionuclides by workers. Annals of ICRP 24 (4). Pergamon, Oxford
ICRP (1996) Age-dependent doses to members of the public from intake of radionuclides: Part 5 compilation of ingestion and inhalation dose coefficients. Annals of ICRP 26 (1). Pergamon, Oxford
Leggett RW, Eckerman KF (2001) A systemic biokinetic model for polonium. Sci Total Environ 275:109–125
ICRP (1979) Limits on intakes of radionuclides for workers. Part 1. Annals of the ICRP 2 (3–4). Pergamon, Oxford
ICRP (1994) Human respiratory tract model for radiological protection. Annals of the ICRP 24 (1–3). Pergamon, Oxford
Loevinger R, Berman M (1976) A revised schema for calculating the absorbed dose from biologically distributed radionuclides. MIRD Pamphlet No. 1, Revised. Society of Nuclear Medicine, New York
ICRP (1995) Age-dependent doses to members of the public from intake of radionuclides: Part 4 inhalation dose coefficients. Annals of the ICRP 25 (3–4). Pergamon, Oxford
Cristy M, Eckerman KF (1993) SEECAL: program to calculate age-dependent specific effective energies. ORNL/TM-12351, Oak Ridge National Laboratory, Oak Ridge
ICRP (1991) 1990 Recommendations of the International Commission on Radiological Protection. Annals of the ICRP 21 (1–3). Pergamon, Oxford
HPA (2007) Assessment of doses from measurements of Polonium-210 in urine, Health Protection Agency. http://www.hpa.org.uk/polonium/Dose_Assessment.pdf. Cited 15 March 2007
Spencer H, Holtzman RB, Kramer L, Ilcewicz FH (1977) Metabolic balances of 210Pb and 210Po at natural levels. Radiat Res 69:166–184
Harrison J, Leggett R, Lloyd D, Phipps A, Scott B (2007) Polonium-210 as a poison. J Radiol Prot 27:17–40
BMU (2006) Umweltradioaktivität und Strahlenbelastung Jahresbericht 2005. Bundesministerium für Umwelt, Naturschutz und Reaktorsicherheit, Bonn
Acknowledgments
We thank the Research Centre Jülich for providing us rapidly with 208Po tracer. We thank Ms. V. Tschöpp and Mr. R. Lindner for performing the radiochemical analysis. Special thanks are due to Dr. Linda Walsh for linguistically reading the manuscript.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License ( https://creativecommons.org/licenses/by-nc/2.0 ), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
Li, W.B., Gerstmann, U., Giussani, A. et al. Internal dose assessment of 210Po using biokinetic modeling and urinary excretion measurement. Radiat Environ Biophys 47, 101–110 (2008). https://doi.org/10.1007/s00411-007-0133-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00411-007-0133-0