Morgenstern, J. Canadian Association of Radiologists Guidance on Contrast-Associated Acute Kidney Injury, First10EM, June 8, 2022. Available at:
https://doi.org/10.51684/FIRS.128056
Many years ago, I wrote a review of the 2012 Canadian Association of Radiologists consensus guidelines for the prevention of contrast-induced nephropathy (now called contrast-assocaited acute kidney injury), which I am only realizing now that I never published to the blog. (Owen 2014) I think there were some significant problems with that guideline (such as the fact that CIN is just assumed to exist), but it actually had some very reasonable guidance, which has unfortunately been almost universally ignored. They acknowledged that “in patients who are acutely ill, delays in imaging while awaiting SCr level results may adversely affect patient care.” Furthermore, the patients at risk can almost all be identified by risk factors, rather than waiting for bloodwork. Therefore, they state that we should not delay imaging in emergency department patients to see a creatinine. That is good advice, and has apparently been the official guidance in Canada throughout my entire career, and yet it has not been followed in any hospital that I have ever worked in.
We now have an updated version of this guideline, which although imperfect, should still improve care for most emergency department patients (if implemented):
The paper
Macdonald DB, Hurrell C, Costa AF, McInnes MDF, O’Malley ME, Barrett B, Brown PA, Clark EG, Hadjivassiliou A, Kirkpatrick IDC, Rempel JL, Jeon PM, Hiremath S. Canadian Association of Radiologists Guidance on Contrast Associated Acute Kidney Injury. Can Assoc Radiol J. 2022 May 24:8465371221083970. doi: 10.1177/08465371221083970. Epub ahead of print. PMID: 35608223 [free full text]
Does contrast really hurt kidneys?
Many prior guidelines have started with the assumption that contrast causes kidney injury, so it is a major win that this guideline starts with a discussion of the underlying evidence for this essential question. They acknowledge that a control group is essential when studying this question, and that our historical practice is entirely based on uncontrolled studies. Studies that have control groups “demonstrate that the incidence of AKI associated with contrast-enhanced CT scans is no higher than the incidence of AKI associated with unenhanced CT scans.” (This evidence is discussed in detail in the main CIN post.) They discuss some important limitations to this data, such as the limited number of patients with severely reduced kidney function, and the limitations of propensity matching, all of which I agree with. They state that the evidence cannot be interpreted to state that CIN is a myth, and that there is “currently insufficient evidence to claim that there is zero risk.” I agree with this statement, but we also need to acknowledge that there is insufficient evidence to claim that there is any risk at all. There is clearly uncertainty remaining in this data, but given that every controlled study shows no harm, the bulk of the evidence suggests that this is not a clinically relevant entity. Overall, I agree with their ultimate conclusion that “the role of contrast as the cause of AKI remains unproven and the risk of contrast as a cause of AKI is likely very low.”
Is blood work required before IV contrast?
For urgent scans, they give us a very clear answer: NO.
“Any patient requiring diagnosis for urgent and/or life threatening diagnosis should not have their scan delayed for the purposes of screening.”
“When the patient is in an emergent presentation (such as suspected acute stroke, pulmonary embolism, acute aortic syndrome, bowel ischemia or perforation, and other conditions), an indicated contrast-enhanced imaging study should proceed without delay. Do not delay for eGFR and do not withhold contrast that is necessary for an accurate diagnosis of the emergent pathology.”
For emergency department patients requiring contrast for less urgent conditions, they provide the very reasonable but practically vague guidance to “weigh the benefits of a contrast-enhanced CT versus the very small, theoretical risk of a transient AKI.” Although they do not come out and say it clearly, considering that we see no risk of AKI in all the high quality research available, this really boils down to the question of whether a contrast scan is necessary. Obviously, we should not be ordering scans that are unnecessary. However, if there is any benefit from a contrast CT, the benefit will always outweigh the harms, as the harms are theoretical, and in the worst case scenario very very rare.
Again, I will emphasize that these guidelines are very clear that we should not even be considering this issue in the resuscitation bay. “When a patient is facing a life-threatening illness, indicated examinations with [iodinated contrast medium] should not be withheld for fear of CA-AKI.”
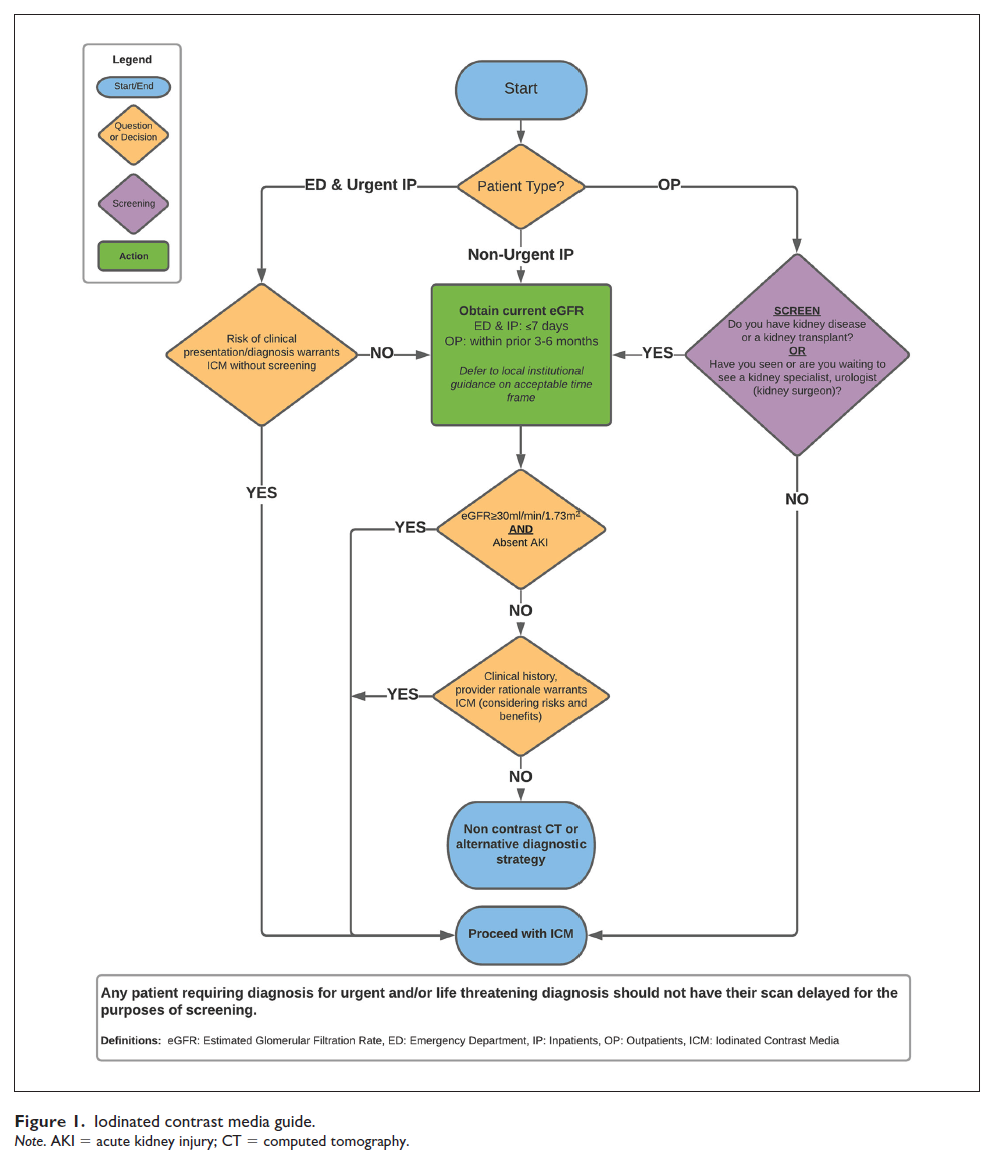
If you have a stable patient and there is absolutely no risk of delaying the CT, then the guidelines suggest screening for an eGFR. They note that “only those with severe CKD (eGFR ≤30 mL/min/1.73 m2), and those with preexisting AKI are at risk of CA-AKI.” So the vast majority of patients will still be able to receive contrast. However, the most important step in this guideline is the step after you find a patient with an eGFR <30 or acute kidney injury. At that point, they suggest considering whether you require IV contrast to make the diagnosis, and if you do need IV contrast to proceed with the scan, regardless of the results of the blood test.
Pause to think about that for a moment. Regardless of the results of the bloodwork, if you think contrast is necessary, you give contrast. What is the most fundamental rule in medicine? Don’t order a test if it is not going to change your management. Their algorithm suggests ordering bloodwork, and then proceeding with the same course of action whatever the results.
So although their guidance is reasonable, they have it in the wrong order. You shouldn’t be considering the need for IV contrast after looking at blood work results. You should be considering the need right when you order the test. If the contrast is needed, you do the scan with contrast. If the contrast is not necessary, don’t order a contrast CT. (If you are truly unsure about the benefit of contrast, then it is perfectly reasonable to consider the eGFR, but that is a relatively rare scenario in emergency medicine.)
Ultimately, their recommendations essentially mirror the brilliant algorithm proposed by Josh Farkas:
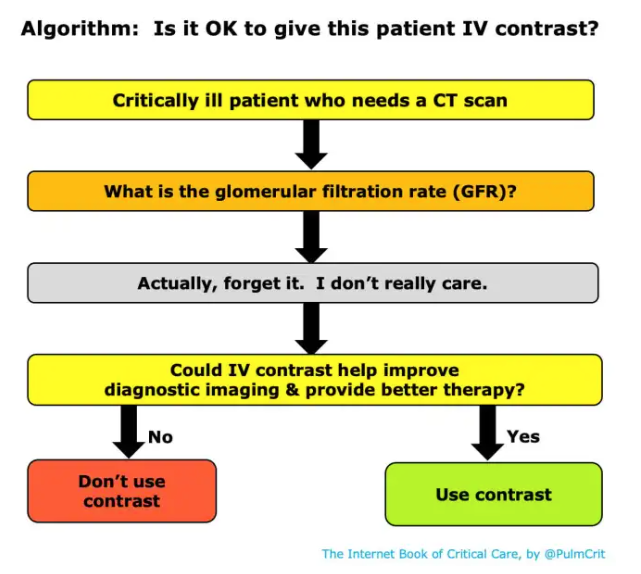
If you need contrast to make an important diagnosis, you should order the test, no matter what the blood work says. Knowing that, you shouldn’t wait for blood before ordering the test, because that is just delaying the diagnosis, and potentially harming your patient.
Their actual algorithm looks a little different, but again I would emphasis that if you know that you need the contrast scan to make the diagnosis, the guideline recommends getting the scan whatever the blood work shows. Therefore, it makes absolutely no sense to delay that scan waiting for bloodwork. Doing so only increases the risk from a delayed diagnosis.
Blood work doesn’t help in acute kidney injury
A common scenario that we will encounter in emergency medicine is acute kidney injury. However, the eGFR (and serum creatinine) is unreliable in the setting of acute kidney injury, so we can’t use bloodwork to risk stratify these patients. Waiting for bloodwork to assess for AKI therefore doesn’t make any sense.
These authors acknowledge that there are no studies demonstrating an increased risk in this group of patients, but there is a paucity of evidence and a theoretical risk, so caution is recommended. However, “in these patients, the potential risk of developing CA-AKI must again be weighed against the risk from delayed or missed diagnoses by avoiding ICM.”
In most patients, the clear harm from delayed diagnosis is clearly going to outweigh the theoretical, unproven harm of contrast.
We can’t prevent kidney injury
The other rationale occasionally given for ordering blood work prior to performing a contrast CT is that we might be able to provide some treatment to prevent kidney injury. Numerous options have been suggested over the years, with simple IV fluids and n-acetylcysteine being the most popular. According to the best evidence available, none of these treatment modalities work. (I think this might be because we are trying to prevent a condition that doesn’t really exist.) We should not be providing IV fluids with the sole purpose of trying to prevent kidney injury from IV contrast medium. (Nijssen 2017) As there are no effective prophylactic regimens, prophylaxis is not a valid reason to require blood work prior to performing a contrast CT.
Remember, there is harm from avoiding contrast
Prior guidelines have spent a lot of time focusing on the risk of contrast, but paid inadequate attention to the risks incurred by avoiding or delaying scans because of fears of post-contrast kidney injury. This group does a good job reminding us that both sides of the coin must be considered (and that the risks of contrast are exceedingly low, so that the benefits will almost always win.)
The significant harms of our current system are often ignored. Avoiding necessary scans is clearly harmful, and so is delaying time-sensitive scans. However, the harms don’t stop there. Unscientific rules requiring blood work before contrast have tremendous downstream consequences, resulting in inefficiency and delays throughout the emergency department, tying up beds, and delaying care for patients in the waiting room. All of those harms need to be considered and compared to the completely unproven, theoretical harms of contrast.
Bottom line
These guidelines provide a reasonable summary of the evidence around IV contrast and kidney injury.
If a CT is urgent, you should never delay the CT out of consideration for renal function.
Contrast is still recommended in patients with severe chronic kidney disease or acute kidney injury if the contrast is required to make an important diagnosis and there is not a reasonable alternative diagnostic test. Therefore, if you know that a contrast CT is the only reasonable test, and you are going to order it no matter what the blood work shows, you should not delay the CT just to see the blood work results. Doing so can only hurt your patient.
The only context that blood work is reasonable prior to CT in the emergency department is if there is a reasonable alternative diagnostic test, and the delay caused by adding blood work will not result in any harm.
Other FOAMed
Does contrast cause kidney injury? The evidence
The AMACING Trial: Prehydration to Prevent Contrast Induced Nephropathy (CIN)?
The AMACING trial on The Bottom Line
Rebellion21: Kidneys and Contrast
Contrast Nephropathy, myth thereof
References
Owen RJ, Hiremath S, Myers A, Fraser-Hill M, Barrett BJ. Canadian Association of Radiologists consensus guidelines for the prevention of contrast-induced nephropathy: update 2012. Can Assoc Radiol J. 2014 May;65(2):96-105. doi: 10.1016/j.carj.2012.11.002. Epub 2014 Feb 20. PMID: 24559602
Macdonald DB, Hurrell C, Costa AF, McInnes MDF, O’Malley ME, Barrett B, Brown PA, Clark EG, Hadjivassiliou A, Kirkpatrick IDC, Rempel JL, Jeon PM, Hiremath S. Canadian Association of Radiologists Guidance on Contrast Associated Acute Kidney Injury. Can Assoc Radiol J. 2022 May 24:8465371221083970. doi: 10.1177/08465371221083970. Epub ahead of print. PMID: 35608223
Nijssen EC, Rennenberg RJ, Nelemans PJ, Essers BA, Janssen MM, Vermeeren MA, Ommen VV, Wildberger JE. Prophylactic hydration to protect renal function from intravascular iodinated contrast material in patients at high risk of contrast-induced nephropathy (AMACING): a prospective, randomised, phase 3, controlled, open-label, non-inferiority trial. Lancet. 2017 Apr 1;389(10076):1312-1322. doi: 10.1016/S0140-6736(17)30057-0. Epub 2017 Feb 21. PMID: 28233565