

Abstract
Objective. Interleukin 34 (IL-34) is a recently discovered cytokine that binds macrophage colony-stimulating factor (M-CSF) receptor. Rheumatoid arthritis (RA) is characterized by increased osteoclastogenesis. To identify the significance of IL-34 in RA, the IL-34 concentration was measured in serum and synovial fluid (SF).
Methods. IL-34 concentrations were measured in serum from patients with RA (n = 113), patients with osteoarthritis (OA; n = 56), and controls (n = 36), and in SF isolated from patients with RA (n = 36) or OA (n = 24). Correlations between serum IL-34 levels and clinical features in RA were assessed. The levels of IL-1β, IL-6, IL-17α, interferon-γ-induced protein 10, receptor activator of nuclear factor κB ligand (RANKL), and Dickkopf-1 were also measured.
Results. Patients with RA had a higher mean serum level of IL-34 than did patients with OA and controls (188.0 ± 550.3, 36.6 ± 38.0, and 49.1 ± 78.5 pg/ml, respectively). Similarly, SF IL-34 concentration was higher in patients with RA than in those with OA. IL-34 levels were positively associated with IL-6 levels in serum from patients with RA and OA. SF IL-34 concentration correlated significantly with IL-6 and RANKL levels only in RA. The serum level of IL-34 was not correlated with systemic osteoporosis and radiographic joint damage in RA. IL-34 levels in the serum from patients with RA were positively correlated with rheumatoid factor and anticyclic citrullinated peptide antibody titers (r = 0.282 and 0.491, respectively).
Conclusion. Circulating IL-34 levels in RA correlated with autoantibody production. Further investigations of localized and systemic effects of IL-34 are warranted to elucidate RA pathogenesis.
Rheumatoid arthritis (RA) is a chronic inflammatory polyarthritis characterized by synovial hyperplasia resulting in progressive structural damage in adjacent cartilage and bone, functional disability, and reduced quality of life. Activated osteoclasts are considered key players in RA pathophysiology by contributing to focal bone erosion, and periarticular and generalized bone loss1,2. Perturbation of the inflammatory cytokines causes an imbalance between osteoblast and osteoclast activities, resulting in accentuated bone resorption.
Experiments have identified receptor activator of nuclear factor-κB ligand (RANKL) and macrophage colony-stimulating factor (M-CSF) as crucial players in osteoclast differentiation and function. M-CSF (also called CSF-1) is an osteoblast/stromal cell product. Administration of recombinant human M-CSF completely cures impaired bone resorption in the osteopetrotic op/op mouse, which has a severe deficiency in osteoclast function3. RANKL is also an indispensable factor for osteoclast differentiation, activation, and survival. In addition to being expressed by osteoblasts, RANKL is produced abundantly by infiltrating T cells and synoviocytes in patients with RA4,5,6, and its receptor, RANK, is expressed by osteoclasts and their precursors. RANKL binding to its receptor RANK promotes the activation and survival of mature osteoclasts, which have bone-resorbing capacity7.
Lin, et al8 used recombinant cDNA to identify a novel cytokine from an embryonic kidney cell line, which they designated interleukin 34 (IL-34). They showed that the receptor of IL-34 is a known receptor, the M-CSF receptor, and is expressed on the cell surface of human monocytes. IL-34 was shown to exhibit the same efficacy as M-CSF in stimulating colony formation of macrophages in human bone marrow cells. Surprisingly, a few subsequent experiments have demonstrated that IL-34 can substitute entirely for M-CSF in RANKL-induced osteoclastogenesis9,10.
To date, little was known about the function or clinical significance of IL-34 in human diseases such as RA. A recent report by Chemel, et al11 demonstrated that IL-34 is expressed in RA synovium and that IL-34 expression could be induced by tumor necrosis factor-α (TNF-α) and IL-1β. Similar results were found by Hwang, et al12, who reported that IL-34 was expressed in the RA synovium and fibroblast-like synovial cells (FLS), and that TNF-α induced IL-34 production by RA FLS and osteoclast formation.
To ascertain the clinical role of IL-34 in human RA, we compared the level of IL-34 in serum obtained from patients with RA, patients with osteoarthritis (OA), and healthy controls. We used ELISA, after removal of rheumatoid factor (RF) with 150 μg/ml of blocking reagent (HeteroBlock), as recommended recently by Todd, et al13. We also compared the level of IL-34 in synovial fluid (SF) from patients with RA and OA. We analyzed the associations between serum IL-34 concentration and disease activity, clinical features, and other molecules involved in osteoclast activity, such as IL-17α, IL-1β, IL-6, RANKL, interferon-γ-induced protein 10 (IP-10), and Dickkopf-1 (DKK-1).
MATERIALS AND METHODS
Subjects
Serum samples were obtained from 113 consecutive patients with RA (93 women, 20 men) and 56 patients with OA (52 women, 4 men) who visited the outpatient department, Division of Rheumatology, Bucheon St. Mary’s Hospital, Catholic University of Korea, from January 2011 to April 2012. All patients who met the American College of Rheumatology (ACR) criteria for RA14 and patients who met the ACR criteria for OA15 were included in our study. Thirty-six healthy volunteers (27 women, 9 men) were included as controls. Those with elderly onset RA (EORA), defined as RA with onset age at 60 years or over, were grouped. Young onset RA (YORA) was defined as having RA symptoms between the ages of 18 and 59 years, and those patients were grouped. When disease duration was < 6 months, patients were defined as having early RA (ERA).
SF was obtained from 24 patients with OA (19 women, 5 men) and 36 patients with RA (28 women, 8 men). The analysis also included 7 paired serum and SF samples obtained from the same patients with RA at the same time. Serum and SF samples were stored at −80°C until analysis. Our study was approved by the institutional review board of Bucheon St. Mary’s Hospital (HC11TISI0067) and was performed in accordance with the Helsinki II Declaration. All patients were informed and gave their written consent.
Measurement of cytokines and chemokine in serum and SF
The concentrations were measured by Luminex multiple bead technology (Milliplex Human Cytokine/Chemokine kit, Millipore Corporation; Bio-Plex, Bio-rad Laboratories) according to the instructions provided by the manufacturer. The Bio-Plex Human Cytokine panel includes IL-17α, IL-1β, IL-6, IP-10, and the Milliplex Human Cytokine/Chemokine panel includes RANKL. According to the manufacturer, the interassay coefficient of variation (CV) is 5.8% to 15.9% and the intraassay CV is 4.6% to 10.5%. DKK-1 and IL-34 levels were measured using a commercial sandwich ELISA kit (R&D Systems). The intraassay CV was 3.3% to 4.2% and the interassay CV was 4.6% to 7.6%. To eliminate the influence of RF on cytokine/chemokine levels in the Luminex assay and ELISA, all sera and SF samples were precleared using a commercial reagent to block heterophilic antibodies (HeteroBlock; Omega Biologicals Inc.).
Clinical data and measurement of inflammatory markers
All patients were followed up to obtain clinical data: age, sex, disease duration, erythrocyte sedimentation rate (ESR), C-reactive protein (CRP) level, anticyclic citrullinated peptide (anti-CCP) antibody, and RF titer. RF titer was measured using a particle-enhanced immunoturbidimetric assay; a level > 15 U/ml was considered positive. Anti-CCP antibody titer was measured using a chemiluminescent microparticle immunoassay (ARCHITECT anti-CCP), a second-generation test for anti-CCP assay; a level > 5 U/ml was considered positive, as suggested by the manufacturer. ESR was evaluated using the Westergren method; values ≤ 15 mm/h for men and ≤ 20 mm/h for women were considered normal. CRP level was measured using an immunonephelometry method; values > 5 mg/l were considered positive. The 28-joint count Disease Activity Score (DAS28) was calculated as described16. Disease activity status of remission (REM), low disease activity (LDA), moderate disease activity (MDA), and high disease activity (HDA) were also determined using DAS28. REM was defined as DAS 28 < 2.6, LDA as 2.6 ≤ DAS28 ≤ 3.2, MDA as 3.2 < DAS28 < 5.1, HDA as 5.1 ≤ DAS2817. The extent of joint damage, as indicated by joint space narrowing and erosion, was assessed by the Sharp score18. Seventeen joint areas in each hand were scored for erosion and 18 joint areas in each hand were scored for joint space narrowing. Erosion scores range from 0 to 170 and joint space narrowing scores range from 0 to 144. The total Sharp Score (TSS) was calculated as the sum of the erosion and joint space narrowing scores, with a range of 0 to 31418.
Bone mineral density (BMD) measurement
BMD was measured in the lumbar (L-spine) and right total proximal femur, neck, upper neck, and trochanter by dual energy x-ray absorptiometry (DEXA; LUNAR, GE Medical Systems). To avoid selection bias, it was recommended that all of the RA subjects have BMD measured at the time informed consent was acquired. BMD measurement was performed on 62 patients (54.9%) with RA. The others refused the examination for various reasons, including its cost. L-spine BMD was measured in L1 through L4 with an anterior-posterior view. BMD values are expressed as g/cm2, the Z score, and the T score. In postmenopausal women and men age ≥ 50 years, the World Health Organization diagnosis T score criteria were applied to BMD measurement by central DEXA at the lumbar spine and femoral neck19. In premenopausal women and men < 50 years of age, osteoporosis is defined using the International Society for Clinical Densitometry recommendation, with Z scores of −2.0 or lower.
Statistical analysis
The results are presented as mean ± SD or number (percent). In the figures, each value for a cytokine or chemokine in the serum or SF is represented as a dot plot with mean (bar). Differences between groups in the serum levels of cytokines/chemokines were analyzed using the Kruskal-Wallis test followed by posthoc analysis using the Mann-Whitney U test. The Mann-Whitney U test was used to analyze the cytokine/chemokine levels in RA and OA SF. To assess the Gaussian distribution and the equality of variance, the Shapiro-Wilk test and Levene test were used, respectively. IL-34 level in serum and SF in all groups showed non-normal distribution (Shapiro-Wilk test p < 0.0001). Qualitative data were compared using the chi-square test. Potential correlations between variables were examined using Spearman’s rank correlation. A multivariate linear regression analysis was used to assess association between the serum level of IL-34 and clinical variables (age, mean prednisolone dose for previous 1 month, disease duration, the use of anti-TNF agents, DAS28, RF, and anti-CCP antibody titers). To increase precision on the key variables, a backward elimination selection process was used, wherein potential confounders with p > 0.020 were dropped from the model20. Statistical software (SPSS version 16.0; SPSS Inc.) was used for the statistical analyses. All the p values were 2-tailed and p < 0.05 were considered significant.
RESULTS
Serum and SF levels of IL-34 in RA, OA, and healthy controls
The mean ages of the patients with RA and OA, and healthy controls were similar (54.0, 56.5, and 53.3 yrs, respectively), and the mean RA disease duration was 65.3 ± 71.2 months (range 0–288 months). The baseline clinical and laboratory features are presented in Table 1. Eighty-four percent of patients with RA were seropositive for either RF (78.8%) or anti-CCP (71.6%) antibodies. In this cohort, 26 patients (23.0%) had ERA (disease duration < 6 mos), and 19 patients (16.8%) had EORA (disease onset age ≥ 60 yrs). Twenty-nine percent of patients with RA had osteoporosis in their L-spine or femoral neck. The mean TSS of the patients with RA was 37.0 ± 33.9. The mean prednisolone dose administered in patients with RA was < 5 mg/day.
Clinical and laboratory features in 205 subjects. Clinical characteristics are presented as mean ± SD or number (percentage).
Elevated IL-34 levels in serum and SF of patients for RA
The mean serum IL-34 levels were 49.1 ± 78.5 pg/ml, 36.6 ± 38.0 pg/ml, and 188.0 ± 550.3 pg/ml in healthy controls and OA and RA patients, respectively. Serum IL-34 concentration was significantly higher in patients with RA than in those with OA and controls (p = 0.011; Figure 1A). IL-34 in SF was measured in 24 patients with OA and in 36 patients with RA of similar mean age (61.1 ± 10.2 vs 55.7 ± 17.2, p = 0.294). SF IL-34 level was higher in patients with RA than in OA (151.6 ± 342.5 vs 21.3 ± 15.1, p < 0.001; Figure 1B). In patients with RA, IL-34 concentrations did not differ significantly between serum and SF (p = 0.641; Figure 1C). IL-34 was measured in 7 matched serum and SF samples from patients with RA. As shown in Figure 1D, IL-34 levels were similar in the serum and SF of these patients (p = 0.255).

Serum and synovial fluid (SF) values of interleukin 34 (IL-34) according to clinical features in rheumatoid arthritis (RA). A. Serum concentrations of IL-34 were measured in healthy controls (HC; n = 36) and in patients with osteoarthritis (OA; n = 56) and RA (n = 113). IL-34 serum level was significantly higher in patients with RA than in patients with OA. B. SF concentration of IL-34 was higher in RA (n = 36) than in OA (n = 24). C. IL-34 concentrations did not differ between RA serum and RA SF. D. IL-34 levels in serum and SF samples in 7 patients with RA were measured simultaneously. Symbols represent individual samples and horizontal bars represent the mean of all samples within a group (A–C). E. Patients with RA were categorized into groups according to RA disease duration [early RA (ERA) and established RA]. The mean serum level of IL-34 in patients with established RA is higher than that found in ERA. F. The scatter plot indicates the serum IL-34 level and lowest T score in patients with RA divided into 2 groups based on the presence of osteoporosis.
Higher serum level of IL-34 in established RA
The patients with RA were categorized into an ERA (n = 26) and established RA (n = 87) group according to disease duration (< 6 mos vs ≥ 6 mos). The serum concentration of IL-34 differs significantly between the 2 groups (143.5 ± 174.8 pg/ml and 201.3 ± 620.2 pg/ml in ERA and established RA, respectively; Figure 1E). As it is widely identified that the clinical presentation of EORA patients differs from that of YORA21, we determined whether there exists a significant difference between the groups. Although the mean serum level of IL-34 tended to be higher in the EORA group than in the YORA group (464.3 ± 845.0 pg/ml and 132.13 ± 455.7 pg/ml in EORA and YORA, respectively, p = 0.111), the difference was not significant. Then patients with RA were divided into 4 groups according to the DAS28 score (REM, LDA, MDA, and HDA), and the IL-34 serum concentrations were compared between groups. The mean serum IL-34 concentrations were similar in the 4 groups (data not shown). Systemic bone loss is a characteristic feature of RA and inflammation contributes mainly to the bone loss and increases fracture risk in patients with RA22. To determine whether serum IL-34 is involved in generalized bone loss in RA, serum concentrations of the cytokine were compared between patients with RA stratified by BMD (non-osteoporosis vs osteoporosis). Mean serum IL-34 level in patients with RA who have osteoporosis seemed to be higher than in those without osteoporosis (457.0 ± 875.4 and 65.6 ± 80.5 pg/ml, respectively, p = 0.004). But there was no significant association between IL-34 value and lowest T score in each patient. In the patients with osteoporosis, IL-34 expression showed negative correlation with T score (Figure 1F). There was weak or no direct association between the presence of osteoporosis and IL-34 value in patients with RA.
Association between IL-34 concentration and osteoclastogenesis-associated cytokine/chemokine levels
Table 2 illustrates the associations between the levels of IL-34 and cytokines/chemokines involved in osteoclastogenesis. Serum IL-34 concentrations correlated significantly with serum IL-6 levels in both RA and OA patients (γ = 0.270 and 0.547, respectively), whereas no correlations were observed in controls. In SF from patients with RA, IL-34 correlated significantly with IL-6 and RANKL levels (γ = 0.482 and 0.635, respectively). By contrast, IL-34 level did not correlate significantly with the cytokine/chemokine levels in SF of patients with OA.
Correlation analysis for serum and synovial fluid (SF) interleukin-34 (IL-34) level and osteoclastogenesis-associated cytokines/chemokines.
Association between serum IL-34 concentration and clinical features in patients with RA
The associations between clinical features and IL-34 serum concentration in patients with RA are presented in Table 3. The DAS28, ESR, CRP level, BMD, and TSS did not correlate with serum IL-34 levels in patients with RA. The hallmarks of structural damage in RA, such as bone erosion and joint space narrowing, are the consequence of the local inflammatory process, and the structural damage seen in radiographs progresses over time, even if the RA disease activity is low. Therefore, further analyses of serum IL-34 levels were restricted to patients with ERA, but similar results were found (data not shown). Taken together, these data indicated that the serum IL-34 level does not reflect inflammatory status in patients with RA. The serum IL-34 concentrations in patients with RA correlated only with RF (r = 0.282, p = 0.004) and anti-CCP antibody (r = 0.491, p < 0.001) titers (Table 3).
Correlation analysis for serum interleukin 34 (IL-34) and clinical data in patients with RA.
Correlation between serum IL-34 and RF and anti-CCP antibody titers in patients with RA
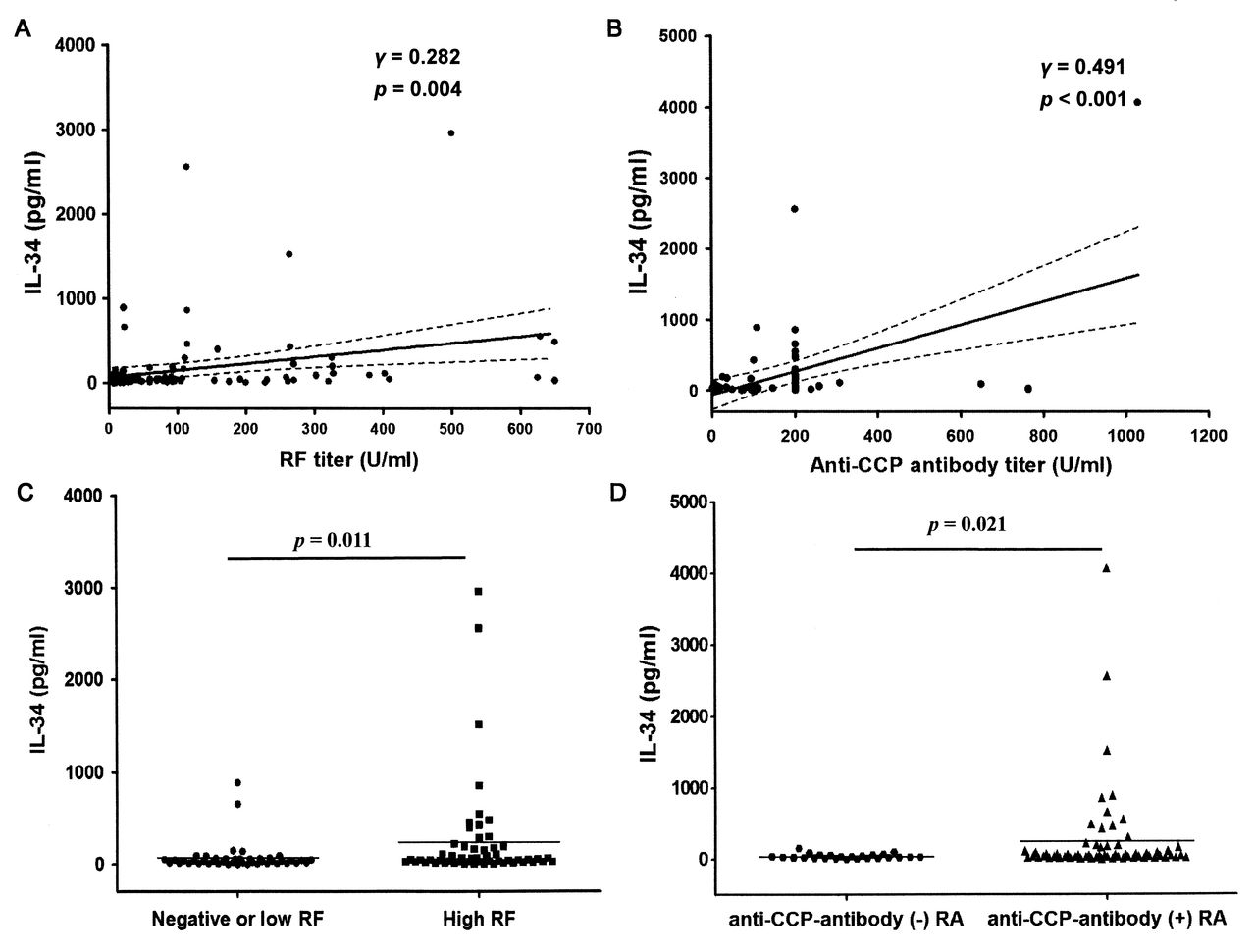
Because serum IL-34 concentration in patients with RA correlated significantly with RF (Figure 2A) and anti-CCP antibody (Figure 2B) titers, the patients with RA were categorized according to RF status [negative or positive with a low titer (< 50 IU/ml) vs positive with a high titer (≥ 50 IU/ml)] and anti-CCP antibody titer (negative or positive). IL-34 level was significantly higher in RA patients with a high RF titer than in those with a low RF titer and in those negative for RF (244.6 ± 555.3 pg/ml vs 72.8 ± 155.8 pg/ml, p = 0.011; Figure 2C). Similarly, IL-34 serum concentration was also significantly higher in anti-CCP antibody–positive patients with RA than in anti-CCP antibody–negative patients (248.8 ± 633.1 pg/ml vs 38.4 ± 34.3, p = 0.021; Figure 2D). Twenty-six patients (23.0%) in the RA group exhibited extraarticular manifestations (EAM) including sicca symptoms (n = 21), rheumatoid nodules (n = 2), pulmonary findings (n = 2), and Raynaud phenomenon (n = 1). Serum IL-34 levels did not differ significantly between patients with RA who exhibited EAM and those who did not (data not shown).
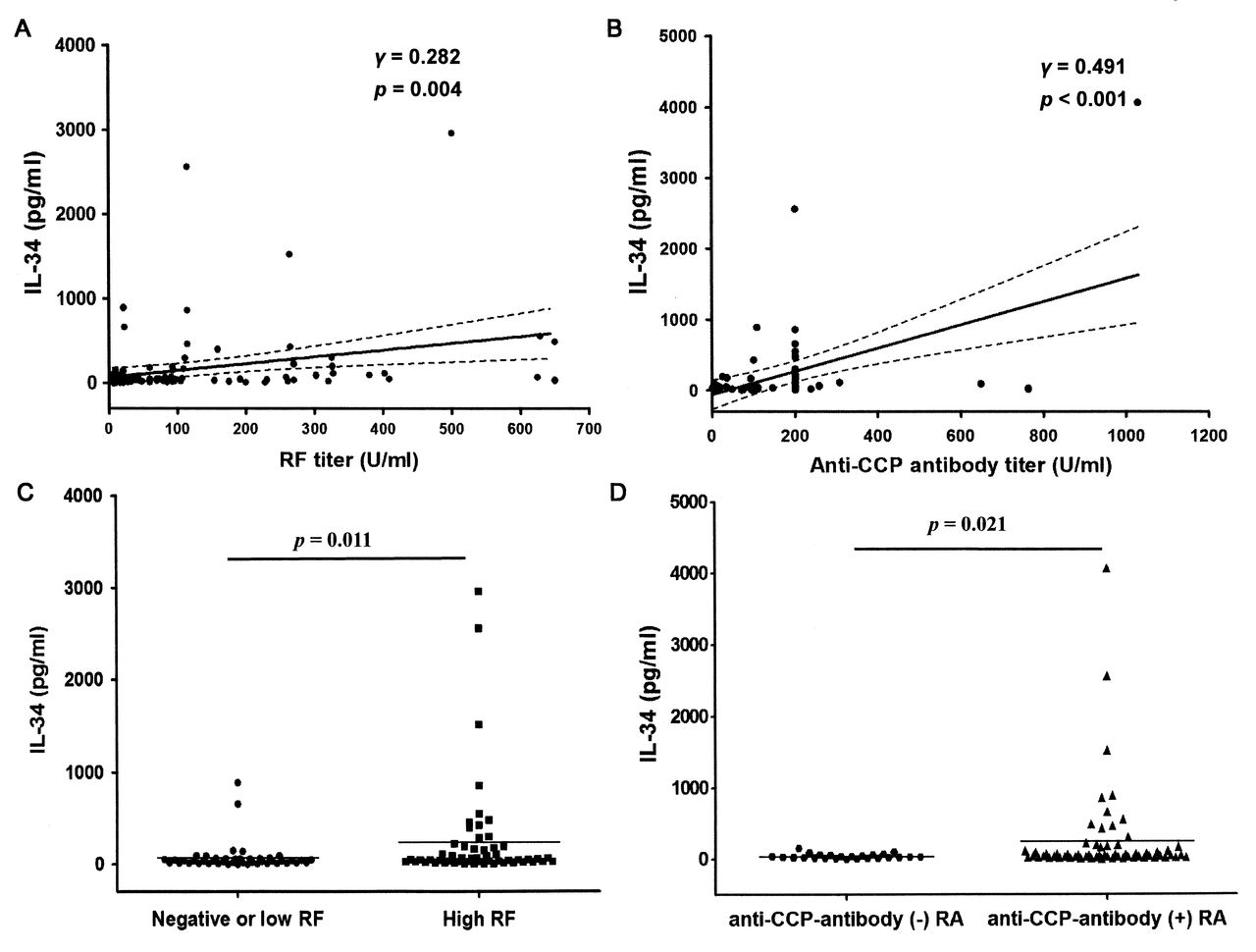
Correlations between serum interleukin 34 (IL-34) levels and rheumatoid factor (RF) and anticyclic citrullinated peptide (anti-CCP) antibody titers in patients with rheumatoid arthritis (RA). A. The serum IL-34 levels of patients with RA correlated significantly with RF titer (n = 100). B. There was a positive correlation between the serum IL-34 levels and anti-CCP antibody titer (n = 58). The statistically significant correlation coefficient (r) and p values are shown. Linear plots of IL-34 for RF or anti-CCP antibody titers are presented with calculated 95% CI (dashed line). C. IL-34 serum levels in RA patients with a high RF titer were significantly higher than in those with a low RF titer or negative for RF. D. Anti-CCP antibody–positive patients with RA showed higher serum concentrations of IL-34 than did anti-CCP antibody–negative patients. Symbols represent individual samples and horizontal bars represent the mean of all samples within a group.
Clinical correlates of serum IL-34 values
Table 4 shows the results of the multivariate linear regression analyses conducted to estimate the influence of potential clinical variables on serum levels of IL-34, while adjusting for sex. Multivariate linear regression identified age and RF titer as independent risk factors for serum IL-34 values. Mean prednisolone dose for the last month, DAS28, disease duration, and the use of anti-TNF agents were included in the model to control for potential confounding. They were found to be insignificant. The anti-CCP antibody titer was significantly positively correlated only with the serum level of IL-34. Other confounders were all revealed to be insignificant by multivariate analysis.
Multivariate linear regression analysis: correlation between clinical variables and rheumatoid factor (RF)/anticyclic citrullinated peptide (anti-CCP) antibody titers, adjusted for sex.
DISCUSSION
In our study, serum IL-34 levels were significantly higher in patients with RA than in patients with OA and controls. The concentration of IL-34 in SF was also higher in patients with RA than in patients with OA. This supports the idea that IL-34 is implicated in RA pathogenesis. Our findings showed similar IL-34 serum levels and SF levels in patients with RA, suggesting that cytokines play pathophysiological roles in RA by at least partially affecting systemic features of the disease. Indeed, our multivariate regression analysis identified serum IL-34 concentrations in patients with RA as being significantly correlated with RF and anti-CCP antibody titers. In contrast, RA disease activity, extent of radiographic damage, and systemic osteoporosis did not show any correlation with IL-34 values in the patients with RA. Taken together, these findings suggest a link between IL-34 and RA pathogenesis, in particular with regard to RA-specific autoantibody production.
Although IL-34 promotes osteoclastogenesis in in vitro experiments9, it is difficult to conclude that IL-34 has an indispensable osteoclastogenic property, at least in RA. In fact, IL-34−/− mice do not display overt malformation in bone23,24, whereas the mice that lack CSF-1 (CSF-1op/op) and those that lack CSF-1R display an osteopetrotic phenotype25,26. Therefore, there may be inevitably functional similarities and differences between IL-34 and CSF-1. Foucher, et al27 suggested the immunosuppressive effects of IL-34. They showed that IL-34 induces differentiation of human monocytes into M2 macrophages that exert immunosuppressive capacity, and that was in an M-CSF– independent manner. By contrast, it was previously reported that IL-34 expression in RA synovium is significantly associated with synovitis severity, suggesting the possible contribution of IL-34 to inflammation and bone erosion in RA11. That result could be discordant with ours. We carefully inferred that the increased expression of IL-34 in RA synovium with more severe inflammation could represent the counterbalance of the cytokine. That assumption could explain the lack of association between IL-34 and systemic osteoporosis, as well as local structural changes in patients with RA shown in our study. Therefore, further research is warranted to identify the biological roles of IL-34 in human RA.
In addition, time of day dependency should be considered in our study. We showed that the level of IL-34 in RA was significantly correlated with IL-6 concentration in both serum and SF. Keller, et al28 reported ex vivo data on mice that demonstrated the endogenous oscillation of serum IL-6 levels over time. It could be postulated that the circadian clock, rather than IL-6 itself, may play a pivotal role in endogenous expression of IL-34 in humans. Further, one report showed a disturbed circadian rhythm in patients with RA, compared to control patients with OA29. Therefore, the longitudinal repeated measure of IL-34 in each patient with RA could give us more reliable information on the biological effects of IL-34 regarding the disease activity or prognosis in human RA.
A limitation of our study is the lack of information on serum levels of 25(OH)-vitamin D3 in humans. Nakamichi, et al30, recently reported that 1α,25(OH)2D3 induced osteoclastogenesis in CSF-1op/op mice by enhanced expression of IL-34 in bone and spleen through a vitamin D receptor-mediated mechanism. Therefore, it could be extrapolated that 25(OH)-vitamin D3 levels may be a confounding bias in determining serum levels of IL-34 in humans. Although the etiology and pathology of RA remain elusive, anti-CCP antibody and RF have been revealed to be associated with the disease course31,32. In autoantibody production, B cells are the primary source. T follicular helper cells, a special subset of CD4+ T cells, assist B cells33,34. In our study, serum levels of IL-34 in RA were significantly correlated with RF and anti-CCP antibody titers. However, IL-34 was originally described as a cytokine that specifically promotes the survival and differentiation of CD14+ monocytes in peripheral blood mononuclear cells, not T or B cells8. Until now, there has been no evidence that suggests any direct link between T or B lymphocytes and IL-34. Therefore, to reveal the mechanism underlying the relationship between IL-34 and autoantibody titers, further research is needed.
Our study found that IL-34 serum and SF levels are significantly higher in patients with RA than in patients with OA and controls. The IL-34 level was associated with autoantibody production in patients with RA, but did not reflect disease activity, joint damage severity, and systemic osteoporosis. Further investigations of the localized and systemic effects of IL-34 are warranted to elucidate the potent pathophysiological roles of IL-34 in RA.
- Accepted for publication July 10, 2013.








{kind=link}
{kind=link}