

Although cases of coronary artery aneurysm formation and myocardial infarction due to dissection in patients with polyarteritis nodosa (PAN) have been reported1,2, there are no reports evaluating widespread coronary arteritis accompanied by myocardial damage using cardiac magnetic resonance imaging (cMRI). We performed cMRI on a young man with widespread coronary arteritis resulting from PAN, and evaluated the changes in myocardial involvement after 3 months.
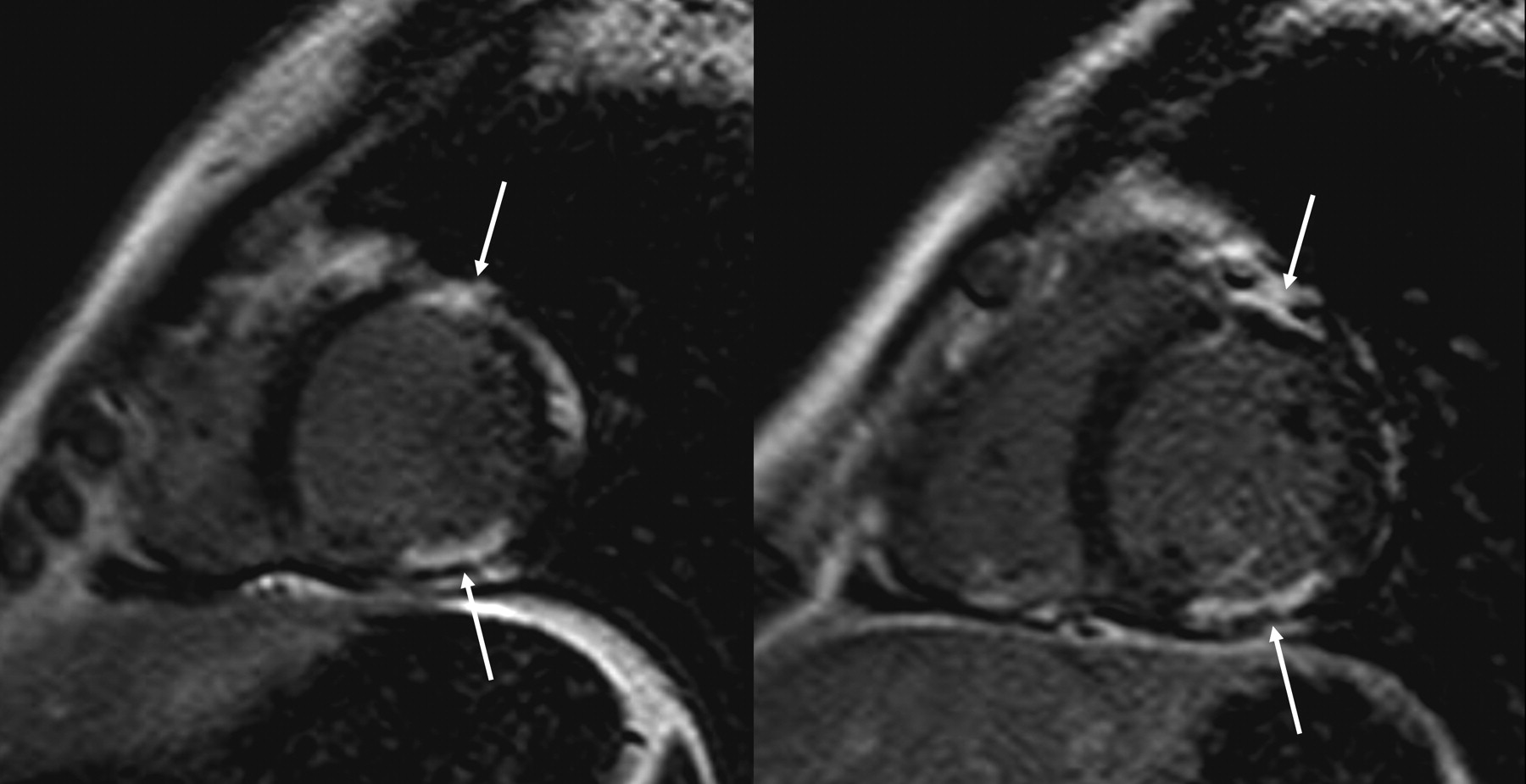
This case involved a 35-year-old male who, in July 2009, noted unintentional weight loss (4 kg in 1 month), fever, and joint pain. Toward the end of August, he presented for examination after noticing paresthesia and myalgia in both lower extremities and discomfort in the chest unrelated to physical exertion. There was nothing remarkable in medical histories of the patient or family. There were no irregular vital signs but there was muscular tenderness in both lower extremities. Electrocardiogram revealed slightly elevated ST in II, III, and aVF leads. Laboratory examination showed leukocytosis (11,000/μl), elevated C-reactive protein (11.42 mg/dl), and elevated creatine kinase (CPK 170 U/l, CPK-MB 35.9), but no evidence of renal or hepatic dysfunction. No obvious infectious foci could be identified. Tests for antinuclear antibody, HBsAg, hepatitis C virus antibody, syphilis rapid plasma reagin, cryoglobulin, and immune complex were negative, and myeloperoxidase-antineutrophil cytoplasmic antibodies (ANCA) and proteinase 3-ANCA levels were < 10 EU/ml. A chest radiograph revealed no abnormalities. Echocardiography examination revealed posterior-wall and inferior-wall hypokinesis, and ejection fraction was 63%. On cMRI, a delayed-enhanced (DE) image showed linear enhancements in the subendocardial layer, suggesting myocardial infarctions (Figure 1). A coronary angiography examination showed widespread stenosis in multiple peripheral blood vessels and vascular wall abnormalities, and the patient was diagnosed as having coronary arteritis (Figure 2). He was also diagnosed with PAN based on paresthesia and myalgia in bilateral lower extremities, weight loss, and angiography findings. Moreover, 3 of the American College of Rheumatology diagnostic criteria3 for PAN were confirmed. He was started on 60 mg prednisone and 100 mg cyclophosphamide orally per day. Inflammatory response was suppressed and the symptoms disappeared.

Delayed-enhanced cardiac MRI showed linear enhancements in mainly subendocardial layer of anterior and inferior wall (arrows), suggesting myocardial infarctions.

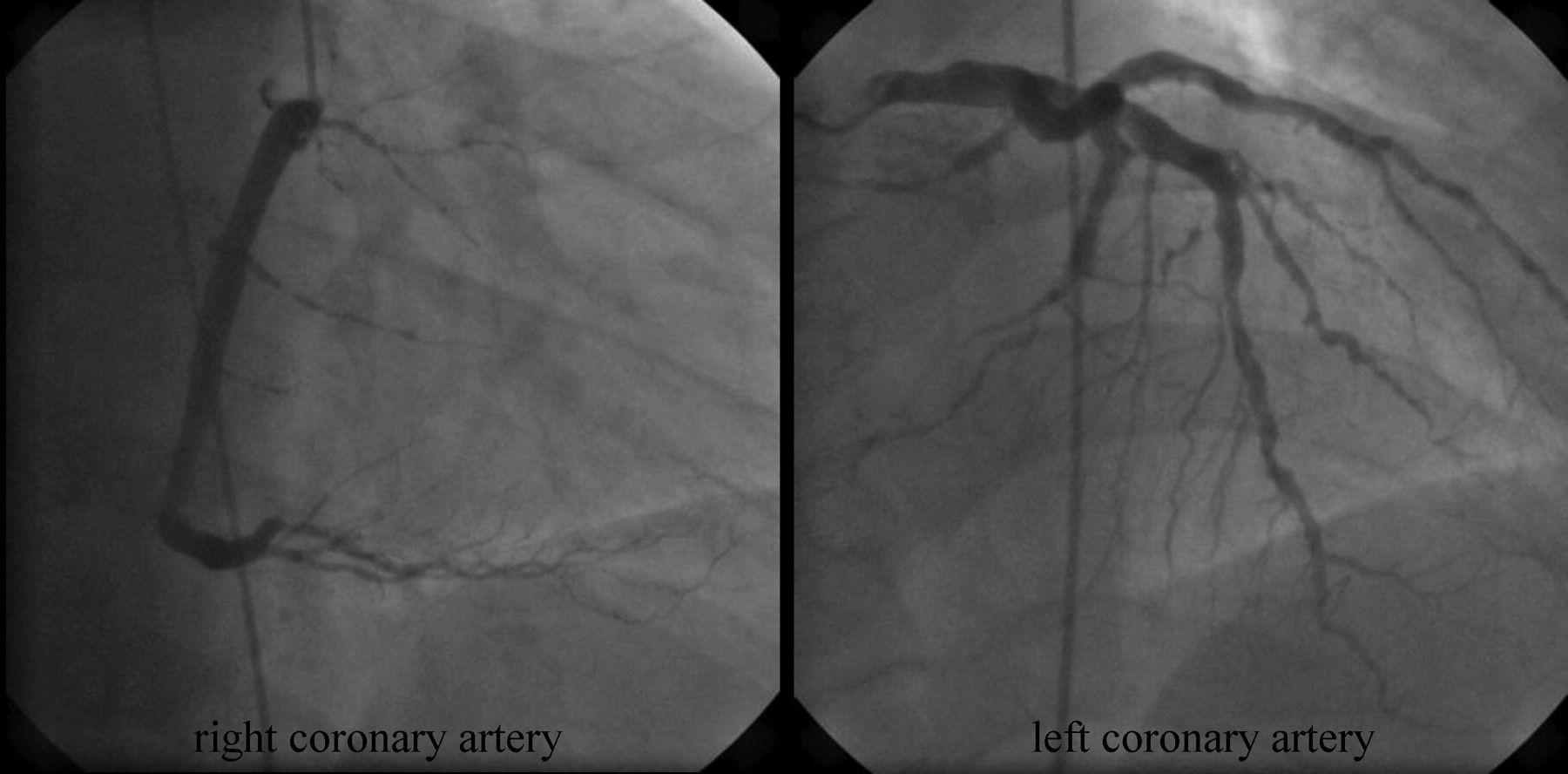
Coronary angiogram of right and left coronary arteries. In the distal branches of all coronary arteries, diffuse lesions with corkscrew-like appearance were present. These findings were compatible with coronary arteritis.
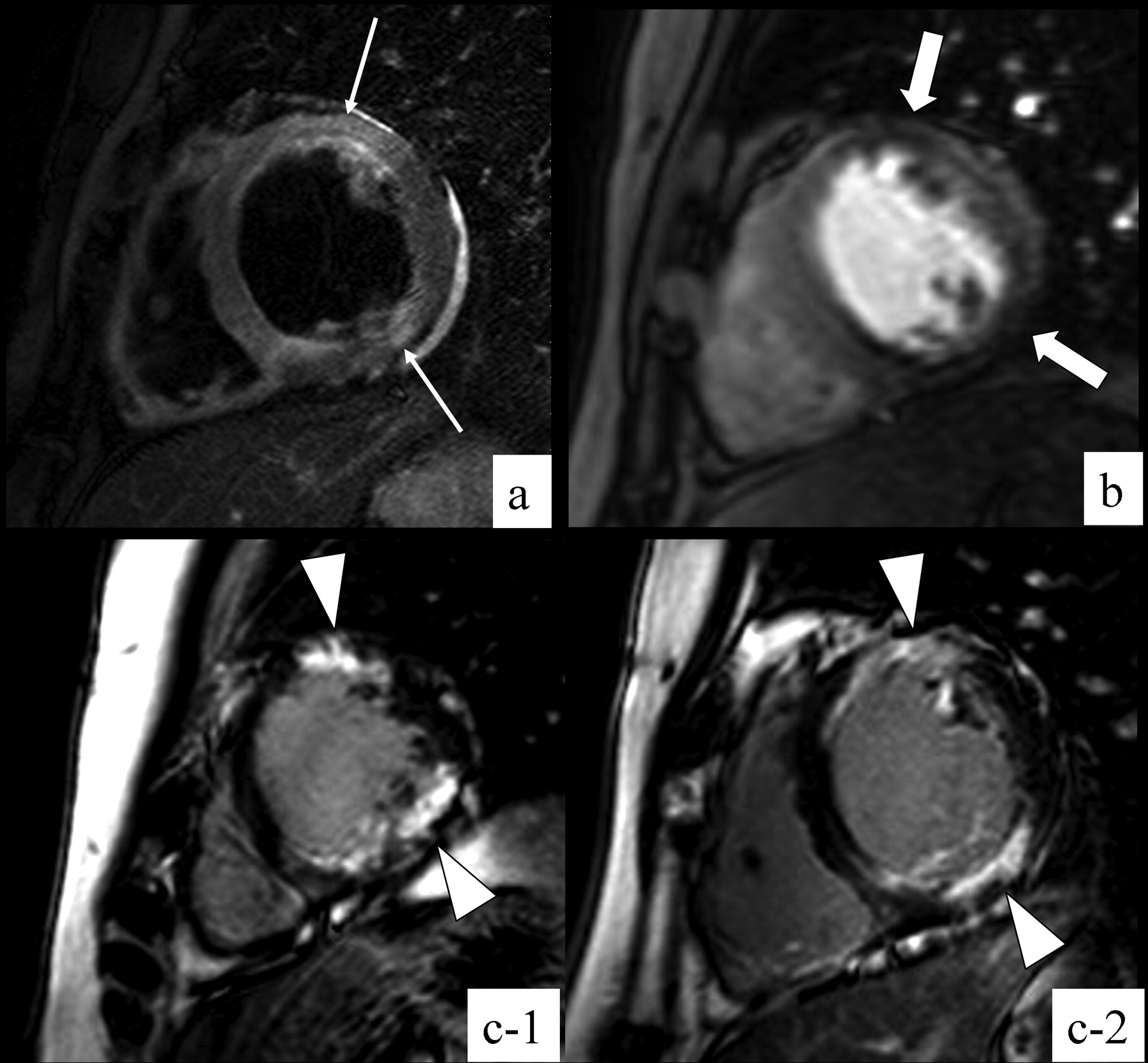
An ensuing electrocardiogram showed T-wave inversions in II, III, and aVF leads. However, in a cMRI after 3 months, high signal intensity, indicating edema, was shown on the “black-blood” T2-weighted inversion-recovery MRI (Figure 3A). A stress perfusion MRI (Figure 3B) showed nonsegmental circumferential perfusion defects (arrows) suggesting microvascular impairment. The DE image (Figure 3, C1, C2) showed multiple curvilinear enhancements with border irregularities in the subendocardial and middle layers, which had increased in size. A gray zone was also observed adjacent to the strongly enhanced lesions. These findings of cMRI suggest the possibility of progression in myocardial involvement, regardless of PAN activity. In terms of PAN, despite alleviating the observed inflammation and dissipation of symptoms, cardiac involvement may progress, an important consideration to keep in mind.
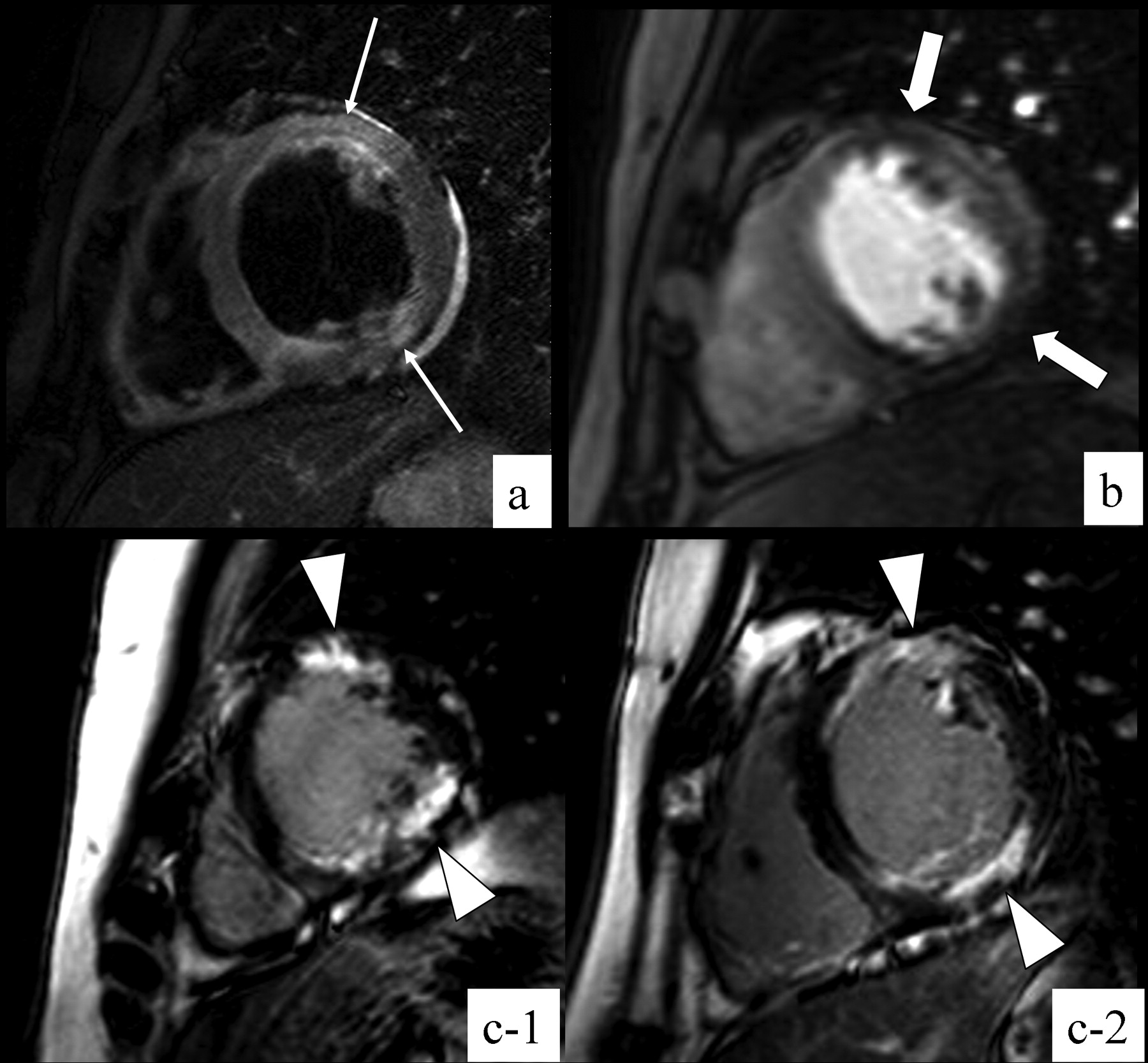
Followup cardiac MRI. A. Black-blood T2-weighted image: high-intensity lesions were seen in anterior and inferior wall (arrows), indicating edema. B. Pharmacological stress perfusion MRI showed perfusion defects (thick arrows). Rest perfusion MRI showed no defects (not shown). These findings suggested myocardial ischemia. C1, C2. Delayed-enhanced MRI showed multiple curvilinear enhancements in subendocardial and middle layer of anterior and inferior wall (arrowheads). Compared with previous study, delayed-enhanced lesion has grown. The border of the lesions became extremely irregular, and a gray zone was also seen adjacent to strongly-enhanced lesions.
Cardiac MRI can be useful as a far less invasive method of evaluating myocardial damage in patients with PAN.








{kind=link}
{kind=link}
{kind=link}