

Abstract
Objective. Gout typically affects the peripheral joints of the appendicular skeleton and rarely involves the axial joints. The literature on axial gout is limited to case reports and case series. This preliminary study was conducted to identify the frequency and characteristics of axial gout.
Methods. Six hundred thirty medical records with ICD codes 274.0, 274.82, and 274.9 for peripheral gout were reviewed. Ninety-two patients had clinical or crystal-proven gout, of which 64 had prior computed tomography (CT) images of the spine performed for various medical reasons. These CT images were reviewed for features of axial gout, which include vertebral erosions mainly at the discovertebral junction and the facet joints, deposits of tophi, and erosions in the vertebral body, epidural space, ligamentum flavum and pars interarticularis.
Results. Nine of the 64 patients had radiographic changes suggestive of axial gout. Lumbar vertebrae were most commonly involved, with facet joint erosions being the most common finding. Isolated involvement of the sacroiliac joints was seen in 2 patients. Axial gout had been diagnosed clinically in only one patient.
Conclusion. Radiologic changes of axial gout were more common than recognized clinically, with a frequency of 14%. Since not all patients had CT images, it is possible that the frequency of axial involvement was even greater. A prospective study is needed to further define this process.
Gout typically affects the peripheral joints of the appendicular skeleton, and has been reported to rarely involve the axial joints. The incidence of gout has increased greater than 2-fold over the last 2 decades and its prevalence in postmenopausal women approaches that of men1,2.
With this increase in the incidence and prevalence of gout, it is reasonable to assume that the prevalence of axial gout has also increased. However, much of the information on axial gout is limited to case reports or case series. In 69 case reports on axial gout, chronic tophaceous gout was identified in 32 (46%)3–65. In these 69 patients, 34 (49%) had neck and/or back pain and 44 (63%) had elevated serum uric acid (SUA) concentrations. All levels of the axial skeleton were involved by gout, 33 (48%) involving the lumbar vertebrae, 20 (29%) the cervical vertebrae, 14 (20%) the thoracic vertebrae, and 6 (8.7%) the sacroiliac joints (SIJ). The presenting features of axial gout are reported to include neck stiffness3, back pain14,15, radiculopathy23,59, and severe neurologic compromise4,11,12. Axial gout can also occur without back pain5,6. SIJ gout can either be asymptomatic or present as acute sacroiliitis and/or as referred pain to the back, thigh, or hip8,66,67.
The pathology of gout involves urate deposition with resultant acute and chronic inflammation in the synovial fluid, articular cartilage, synovial membrane, and capsular and periarticular tissues68,69. The urate crystals penetrate into the subchondral bone, giving rise to erosions, cysts, and sclerotic appearance. In the SIJ large cystic erosions in the subchondral bone are considered to be more consistent with gout than irregularity and sclerosis of the joint margins70.
Plain radiographs and magnetic resonance imaging (MRI) have limited use in the identification of axial gout43,47,71,72. In all the case reports where MRI of the spine was performed, the diagnosis was not obvious and gout was confirmed by surgery29,36,42, 44,51,60,65,72. On the other hand, CT imaging of the axial skeleton is the preferred modality to identify axial gouty changes. Tophaceous deposits containing calcium are well identified by CT scan and appear as asymmetrical soft-tissue masses with surrounding density greater than that of a muscle34. Thus, in this retrospective clinical review, we chose to use CT imaging as the modality to identify the presence of axial gout.
MATERIALS AND METHODS
Patients
A medical record review of patients with peripheral gout seen at Washington Hospital Center in the years 1998–2006 was performed. All records of patients with International Classification of Diseases (ICD-9) codes 274.0 (gouty arthritis), 274.82 (tophaceous gout), and 274.9 (gout unspecified) were reviewed. Patients were included in the study if they had crystal-proven gout documented in the record or had presumptive diagnosis of gout as determined by the rheumatology consultation service, which included characteristic history of gout attacks and review of peripheral radiographs with evidence of characteristic gouty erosions. Clinical and laboratory details of the selected patients were collected, including age, sex, ethnicity, hypertension, diabetes mellitus, renal insufficiency, diuretic and aspirin therapy, SUA level, and serum creatinine.
Radiographic imaging.
Medical records were reviewed for the availability of CT images of neck/cervical region, chest/thoracic region, abdomen/lumbar region, or pelvis that were obtained for evaluation of a variety of clinical symptoms and body-cavity pathologies. Although the CT scans were obtained for various medical problems, none had been ordered to determine if axial gout was present.
The convention at our facility is to image C1-T2 for the CT neck, C6-L2 for CT chest, T9-L4 for CT abdomen, and L2-sacrum for pelvic views. Three radiologists initially reviewed these images individually, and later they also performed a second review together. The images were reviewed for changes suggestive of spinal gout in all the vertebrae and the SIJ, which include lobular juxtaarticular masses with an attenuation density greater than the surrounding muscle, and well defined intraarticular and juxtaarticular facet joint erosions with sclerotic borders and relative preservation of synovial joint spaces34.
RESULTS
Six hundred thirty medical records with ICD codes of 274.0, 274.9, and 274.82 were reviewed. In 92 patients there was documented crystal-proven gout or attacks of gouty arthritis as determined by the rheumatology consultation service. Sixty-four of the 92 had CT images of cervical, thoracic, or pelvic region alone or in combination for axial pain or other medical conditions. Spinal gout was identified in 9 of these 64 patients (14%; Table 1). All were African American, which reflects our hospital’s demographic population.
Radiographic changes suggestive of axial gout. All subjects were African American.
Seven patients (78%) had lumbar spine involvement and 3 (30%) thoracic spine involvement. None of the cervical spine images showed any changes suggestive of gout. Multiple vertebral levels were involved in 6 patients. Lumbar facet joint erosions were the most common finding (Table 1, Figure 1). The spinal processes were found to have tophi in one patient (Figure 2). Two patients had isolated SIJ changes, with tophi consistent with gout (Figure 3). Only 3 patients had back pain prompting CT scanning, and the images were interpreted as consistent with axial gout in only one.
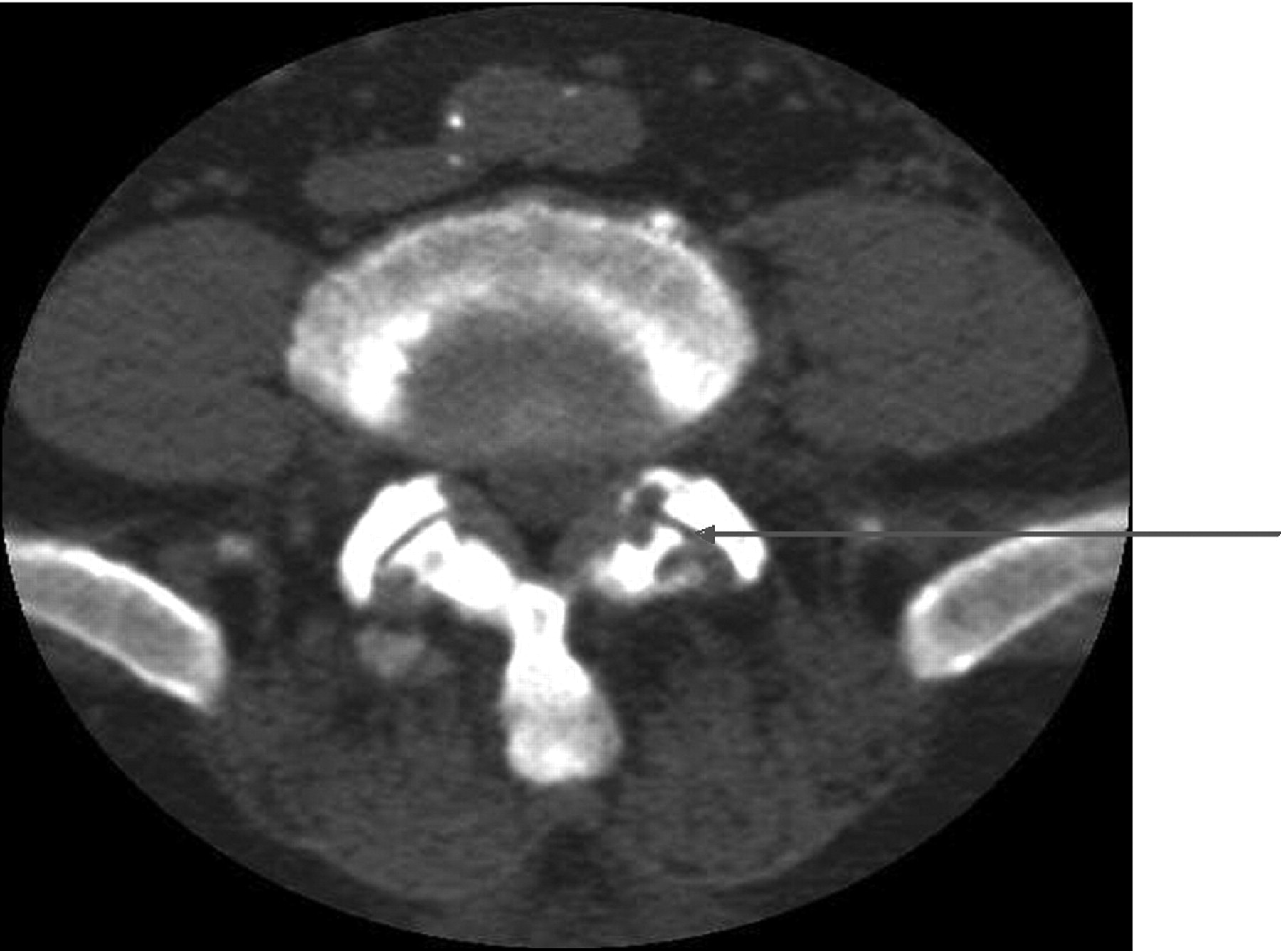
Erosive facet arthropathy associated with gouty arthritis.

Spinous process with tophus: 2 views of the same patient.

Tophus in a sacroiliac joint.
Clinical and laboratory data of the 9 patients with evidence of spinal gout and 55 patients with no features of spinal gout were compared (Table 2). We found no difference between groups in the age, SUA level, and other comorbid conditions. The mean SUA level in patients with spinal gout was 10.24 mg/dl as compared to the non-spinal gout patients at 8.36 mg/dl, which did not reach statistical significance. The results for all the vertebrae, imaged by level, are shown in Table 3. The vertebral levels with the most spinal gouty changes were L4 (12%) and L5 (9%).
Comparison of variables between spinal and non-spinal gout patients.
Vertebral levels imaged in the CT scan.
DISCUSSION
This was a study of a select population of patients with peripheral gouty arthritis who had axial CT scans available for analysis. A 14% frequency of suspected axial gout was identified. The demographic pattern showed a characteristic African American male predominance (78%). It is known that African Americans have higher incidence and prevalence of gout than Caucasians, mainly attributed to higher prevalence of hypertension and sickle cell anemia73,74. Although patients with axial gout had higher mean SUA concentrations than patients without axial gout, this was not statistically significant, but the sample size was small.
CT evidence for axial gout was more common in the lumbar spine (almost 80%) at the lower levels, i.e., L4 and L5. This is similar to cases in the literature, where 33 (approximately 45%) had lumbar vertebral involvement. However, many more of our 64 patients had lumbar CT scans than for the other spinal regions (Table 3). This predilection of spinal gout for the lumbar vertebrae is of interest. It may represent the previously observed phenomenon of monosodium urate deposition into sites of previous injury75.
None of the cervical spine images in our study revealed changes suggestive of gout, in contrast to the 20 cases of cervical spinal gout in the literature. However, our determination of cervical involvement was limited by the very small number of patients with cervical spine CT imaging. It is noteworthy that all 3 of our patients with SIJ abnormalities had renal insufficiency, but the presence of tophi in 2 supports the diagnosis of gout, rather than renal osteodystrophy.
Erosive changes in the spine can be seen in other arthritic and crystal deposition diseases such as rheumatoid arthritis, infectious arthitis, and calcium pyrophosphate dihydrate deposition disease. The distribution of the erosive changes in our series, which constituted multilevel contiguous and noncontiguous axial involvement, the absence of disc calcification, and the identification of axial tophi in the presence of peripheral gouty arthritis, makes other diagnoses less likely.
Important limitations of our study include the lack of histologic confirmation (crystal identification) of axial gout, the subjects not studied prospectively by CT scanning and clinical and laboratory evaluations, the unequal distribution of the spinal levels that were imaged leading to the lack of adequate cervical and thoracic spinal radiographs studied compared to the lumbar spinal images, and the relatively small number of patients. The radiographs were not read in a blinded fashion and there were no controls. It should be noted that axial gout was identified with reasonable but not absolute certainty based only on the presence of clinical gout and characteristic CT features, but in the absence of histologic confirmation66,76.
In our study, only 3 of the 64 cases had symptoms of back pain that prompted the CT imaging, but axial gout was diagnosed clinically in only one. The remaining 8 cases were identified by us after the review of the available CT images. These results clearly suggest that the frequency of axial gout may be much higher than previously known, that it may occur in the absence of back pain, and that physicians are not aware of the potential existence of axial involvement in gout patients. Further, the diagnosis may be missed even when CT scanning is obtained. Prospective studies are needed to determine the actual prevalence of spinal gout, and whether clinical and laboratory features correlate with spinal involvement.
Footnotes
- Accepted for publication October 9, 2008.








{kind=link}
{kind=link}
{kind=link}