
JOURNAL OF ORTHOPAEDICS AND CLINICAL RESEARCH
Poliomyelitis - Related Deformities Successfully Treated with Reconstructing and Lengthening Lower Limb Surgeries and Followed up 11 Years: Challenging Approaches in a Limited - Resources Country
Abdulmouain Zrek1*, Khaled Harmouch2, Tamim Alsuliman3, Marah Mansour4 and Samer Murad5
1Senior Consultant, Department of Orthopedic Surgery, Alrazi Governmental hospital, Syrian Ministry of Health, Aleppo, Syrian Arab Republic
2Near East University Faculty of Medicine- Near East Boulevard, ZIP: 99138 Nicosia, TRNC Mersin 10, Turkey
3Hematology and Cell Therapy Department, Saint-Antoine Hospital, AP-HP, Sorbonne University, Paris, France
4Faculty of Medicine,Tartous University, Tartous, Syrian Arab Republic
5Orthopedic Surgeon, Department of Orthopedic Surgery, Alrazi Governmental hospital, Syrian Ministry of Health, Aleppo, Syrian Arab Republic
*Corresponding Author: Zrek A, MD, Senior Consultant, Department of Orthopedic Surgery, Alrazi Governmental hospital, Syrian Ministry of Health, Aleppo, Syrian Arab Republic.
| ReceivedMay 12, 2022 | RevisedMay 20, 2022 | AcceptedMay 25, 2022 | PublishedJul 20, 2022 |
Abstract
Poliomyelitis is a viral infection that may lead to paralysis or death. Paralysis can lead to skeletal and joint deformities. Typical manifestations include equinoscavus and tibial shortening. We report a polio case presented with right equinus foot, clawing in the right great toe, and shortening in the right tibia.
Keywords
External Fixation, Foot Deformities, Limb-length Discrepancy, Poliomyelitis, Surgical Techniques
Clinical Message
Many Polio cases that were infected before 1999 are still presenting with a variety of post-polio squealer in Syria. Surgeons still manage these complications following advanced and up-to-date surgical techniques in a limited-resource country.
Background
Poliomyelitis or Polio is an acute infection caused by variant strains of poliovirus.
It can affect the respiratory, gastrointestinal, and central nervous systems [1]. In the majorityof cases, the infection is asymptomatic; however, symptoms may include headache, sore throat, nausea, vomiting, severe muscle weakness, muscle contracture, and flaccid paralysis. Paralysis usually affects the lower limb more than the upper limb. Patients may complain of muscle weakness associated with pain and decreased or absent reflexes [2]. Muscle weakness and contractures may lead to abnormal limb development and limb-length discrepancy [3].
Deformities are managed according to the stage, severity, and extent of paralysis and may require multiple corrective surgeries. In Syria, cases with old polio infection are still encountered with a variety of post-polio complications. Herein, we report a case of a 24- year old patient who presented with multiple polio-related musculoskeletal deformities. We also illustrate in detail the surgical work and the techniques applied to manage this case efficiently.
Case Presentation
A 24-year-old female presented to the Department of Orthopedic Surgery complaining of low back pain and motion restrictions due to limb weakness, foot deformities, and lower limb-length discrepancy. Clinical examination revealed polio-related deformities of the right lower limb and tiptoe gait with equines foot. It also demonstrated a 4 cm shorter right limb with apparent right leg dystrophy, in comparison to the left one at the level of mid-gastrocnemius. Flexor muscle movement was better than the extensors. Clawing in the right great toe, equines foot, and plantar flexion deformity caused by the imbalance between extensors and flexors of the foot and ankle were also observed (Figure 1).

Figure 1: Foot deformities caused by poliomyelitis, foot equines and bowing, and clawing of the great toe.
No further deformities were noted. Spina bifida, Marie Tooth disease, and other familial histories were excluded. Three consecutive surgeries were performed over five years to correct the foot deformities and lengthen the lower limb by 3 centimeters. During the first surgery, in February 2006, correcting the foot and the great toe deformities were accomplished. The tibialisposterior tendon was transferred from its insertion at the dorsal foot, specifically the cuboid bone, across the interoseous membrane to rectify the equine foot and the bending while retaining the muscular strength of the foot and ankle extension. The Jones surgical procedure was used: arthrodesis and toe k-wire fixation were used to repair the great toe's inter-phalangeal joint. The long extensor of the great toe was transferred from its insertion to the first metatarsal neck through a formed canal, and the tendon was sutured on itself to rectify the clawing of the great toe, placing it in a functional position and retainingmuscular strength while in motion (Figure 2).

Figure 2: Surgical incisions for transferring of the posterior tibialis tendon to the dorsum of the foot and attachment to the lower foot button and Jones procedure: arthrodesis of the inter-phalangeal joint of the great toe and fixation with two Kirschner wires and extensor halluces longus transfer to the first metatarsal neck.
In August 2008, the second procedure entailed the placement of the axial dynamic external fixator on the medial side of the tibialis (Figure 3).

Figure 3: Image of the lower limb on the day after the second surgery, showing the dynamic axial external fixator.
Cutting 2cm from the middle of the fibula and fixing the distal portion with a cortical screw to avoid syndesmosis sliding. The proximal portion of the tibia cortex was osteotomies to establish an appropriate region for lower limb lengthening (Figure 4).
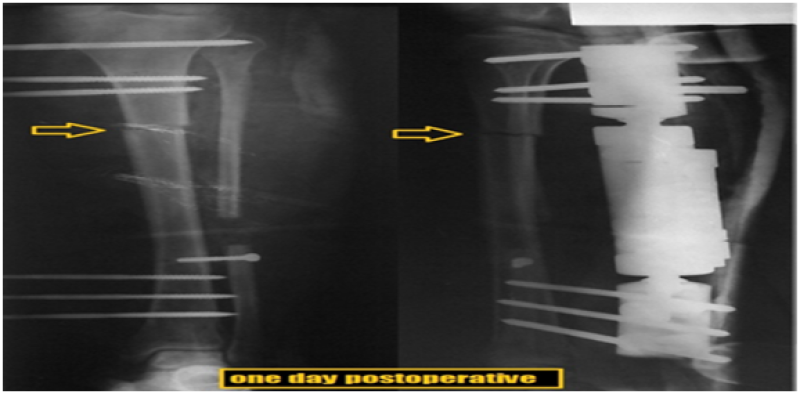
Figure 4: A radiograph of the leg bone on the day after lengthening surgery.
The Achilles tendon was lengthened percutaneous using three small incisions and a temporary splint. During follow-up, the selected region for tibia osteotomy seemed to be inappropriate for sufficient callus formation and led to delayed consolidation (Figure 5) which necessitated a 6-week limb brace putting (Figure 6).
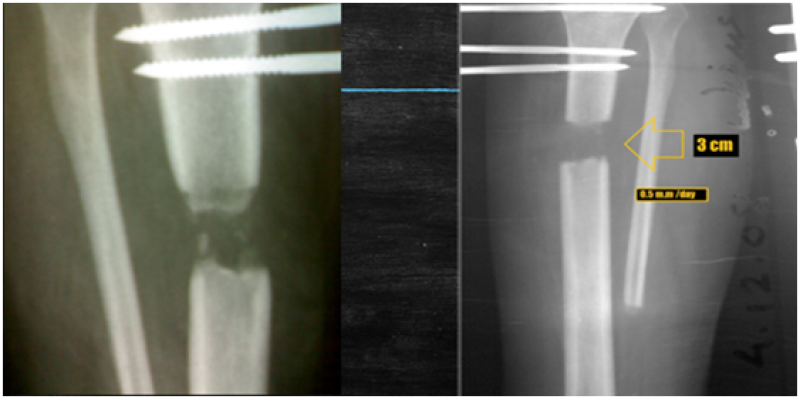
Figure 5: A radiograph at the end of the lengthening and weakness of the extension callus formed.

Figure 6: A radiograph after removing the dynamic axial external fixator and placing the limb in a plaster cast above the knee.
After the removal of the axial dynamic external fixator and the cortical screw, the third surgery was performed in January 2010. The lengthening region of the proximal portion of the tibia was fixed with an intramedullary nail, and grafted with an iliac cancellous bone graft to maintain successful engraftment without damaging the callus. The lengthening amount and callus formation were preserved. Complete engraftment and callus formation were completed in the spring of 2010 (Figure 7).

Figure 7: X-ray showing the complete fusion of the lengthening site two months after the third surgery, and fixation of the tibia with an intramedullary nail with grafting of the site of lengthening through the skin.
Eleven years Follow-up revealed equal leg-length on both sides. Muscular strength, excellent plantar flexion and dorsalmotion in the right foot, a functional great toe, and excellent ability of prolonged walking were also recorded (Figure 8).

Figure 8: The final clinical form of the foot in the plantar position and the lower limbs in the standing position.
Discussion and Conclusion
In the 1980s, the number of annual paralytic cases due to polio was >350,000. Since then, the international vaccination campaigns have been successful in nearly eradicating the virus worldwide. In 2016, there were only 42 active cases [4]. In Syria, polio was totally eliminated in 1999. However, in 2013, 25 new polio cases were reported [5]. In Syria, Patients infected with polio before 1999 are still encountered in daily practice with a variety of limb deformities. Polio foot and ankle deformities include equines foot, claw hallux, and contracted tendon [6]. Leg deformities include limb-length discrepancy [3]. Correction of these deformities requires multiple surgeries. Our patient underwent 3 consecutive surgeries. During the first surgery, the equines foot and claw hallux were corrected, and a plantigrade foot was obtained. In the second surgery, the limb-length discrepancy and contracted tendon were lengthened concomitantly. The Ilizarov apparatus is typically used for tibia lengthening [7]. However, in our case, the axial dynamic external fixator was selected (Figure3). Tibia lengthening may be associated with several complications, including delayed consolidations, pin tract infections, and axial deviations [8]. The occurrence of delayed consolidations is attributed to many factors, including the osteotomy technique, fixation stability, and delayed bone healing due to co-existent muscular atrophy and bone hypoplasia [7]. In our case, tibial lengthening was complicated by delayed consolidations of the callus. This necessitated another surgery. It is also thought that the osteotomy site, at the upper third of the tibia shaft, was not ideal for sufficient callus formation. According to the literature, one approach to managing delayed consolidations is through the transition from external fixation to internal fixation [9]. Internal fixation was performed by removing the axial dynamic external fixator, fixing the lengthening region with an intramedullary nail, and inserting a bone graft into the distraction callus. The Iliac crest was used for bone graft as it is proven to be an excellent grafting option [10]. The above-mentioned surgeries can usually be completed in less than 2 years. The harsh circumstances in Syria limited the performance of these surgeries within the expected timeline and led to an unanticipated delay. After 11 years of follow-up, the maximal tibia lengthening has been reached Figure8. In conclusion, post-polio squealer remains a significant challenge in some countries, and extensive consultations should be considered to establish the finest management. Cases with post-polio sequelae exhibit significant challenges in Syria. Despite the extreme shortage of medical resources in the country, corrective, multi-step and selective surgeries are still performed and excellent outcomes are obtained.
References
1. Herring JA. Tachdjian's Pediatric Orthopaedics: From the Texas Scottish Rite Hospital for Children E-Book. Elsevier Health Sciences. 2020;27.
2. Bennett JE, Dolin R, Blaser MJ. Mandell, douglas, and bennett's principles and practice of infectious diseases E-book. Elsevier Health Sciences. 2019;8.
3. Emara KM, Khames A. Functional outcome after lengthening with and without deformity correction in polio patients. IntOrthop. 2008;32(3):403-7. PubMed | CrossRef
4. Roser M, Ritchie H, Ortiz-Ospina E. Internet. Our World in Data.2021.
5. Tajaldin B, Almilaji K, Langton P, Sparrow A. Defining polio: closing the gap in global surveillance. Ann Glob Health. 2015;81(3):386-95. CrossRef
6. Joseph B, Watts H. Polio revisited: reviving knowledge and skills to meet the challenge of resurgence. J Child Orthop. 2015;9(5):325-38. PubMed | CrossRef
7. Song HR, Myrboh V, Oh CW, Lee ST, Lee SH. Tibial lengthening and concomitant foot deformity correction in 14 patients with permanent deformity after poliomyelitis. ActaOrthop. 2005;76(2):261-9. PubMed | CrossRef
8. Paley D. Problems, obstacles, and complications of limb lengthening by the Ilizarov technique. ClinOrthopRelat Res. 1990;250:81-104. PubMed
9. Wu CC, Chen WJ. Tibial lengthening: technique for speedy lengthening by external fixation and secondary internal fixation. Journal of Trauma and Acute Care Surgery. 2003;54(6):1159-65. PubMed | CrossRef
10. Khan SN, Tomin E, Lane JM.Clinical applications of bone graft substitutes. OrthopClin North Am. 2000;31(3):389-98. PubMed | CrossRef
Abdulmouain Zrek1*, Khaled Harmouch2, Tamim Alsuliman3, Marah Mansour4 and Samer Murad5
1Senior Consultant, Department of Orthopedic Surgery, Alrazi Governmental hospital, Syrian Ministry of Health, Aleppo, Syrian Arab Republic
2Near East University Faculty of Medicine- Near East Boulevard, ZIP: 99138 Nicosia, TRNC Mersin 10, Turkey
3Hematology and Cell Therapy Department, Saint-Antoine Hospital, AP-HP, Sorbonne University, Paris, France
4Faculty of Medicine,Tartous University, Tartous, Syrian Arab Republic
5Orthopedic Surgeon, Department of Orthopedic Surgery, Alrazi Governmental hospital, Syrian Ministry of Health, Aleppo, Syrian Arab Republic
*Corresponding Author: Zrek A, MD, Senior Consultant, Department of Orthopedic Surgery, Alrazi Governmental hospital, Syrian Ministry of Health, Aleppo, Syrian Arab Republic.
Copyright© 2022 by Zrek A, et al. All rights reserved. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Zrek A, Harmouch K, Alsuliman T, Mansour M, Murad S. Poliomyelitis - Related Deformities Successfully Treated with Reconstructing and Lengthening Lower Limb Surgeries and Followed up 11 years: Challenging Approaches in a Limited - Resources Country. J Orth Clin Res. 2022;1(1):1-8. DOI: https://doi.org/10.37191/Mapsci-JOCR-1(1)-001