By Shama Razzaq1, Tahseen Kazmi2, Amna Khalid3, Jamal Abdul Nasir3, Ahmed Saud3, Saadia Shahzad3
AFFLIATIONS:
- Department of Community Medicine, Jinnah Medical and Dental College, Karachi, Pakistan.
- Department of Community Medicine, Central Park Medical College, Lahore, Pakistan.
- Department of Community Medicine, Shalamar Medical and Dental College, Lahore, Pakistan.
ABSTRACT
Background: A handgrip dynamometer is a simple, inexpensive and quick method to assess muscle strength. Sequential decrease in handgrip strength has been shown in various studies as a strong predictor of stroke. Therefore, this study aimed to measure muscular strength and determined its association with co-morbidities to predict critical illness in a community based setting of Punjab, Pakistan.
Methods: The study participants (n=152), were recruited through convenient sampling, during a community-based survey. Muscle strength was assessed with the handgrip dynamometer and quantified according to high, average and low percentile. Chi-square test was done to assess the distribution and multinomial logistic regression analysis to identify the factors associated with them.
Results: Out of 152 participants, mean age 44.5±15.3 years, 95(62.5%) were females and 57(35.5%) males. Handgrip strength measurement showed that 38(25%) of participants had high muscle strength, 80(52.6%) average and 34(22.4%) had low muscle strength. Low muscle strength was significantly higher among females (OR: 7.9, 95% CI: 2.4-27.1) as compared to the males. In general participants having diabetes had low muscle strength (p<0.011), but in hypertensive the association was not significant (p<0.21).
Conclusion: Overall patients at risk of stroke such as diabetics had significant low muscle strength but in hypertensive the association was not significant (p<0.21). More studies with bigger sample size are required to make it a predictive marker for stroke and cardiovascular diseases. It is easy to measure and is a low-cost technique for risk scoring and risk prediction in a community-based setting at an early stage.
Keywords: Muscles; Risk; Adult; Community; Dynamometer.
The importance of muscle mass, strength, and metabolic function in the performance of exercise is a well recognized fact. Loss of muscle strength or changes in skeletal muscles may cause physical weakness and metabolic variations such as insulin resistance, hyperlipidemia and increase in blood pressure1,2.
Lower muscular fitness is emerging as a recognized determinant, in addition to previous evidence-based contributing common risk factors for non-communicable diseases (NCDs) such as low physical activity, obesity, poor diet, tobacco use, increased blood pressure, high blood sugar and increased blood cholesterol level3,4. Epidemiological studies suggest that declining muscle strength is well linked as one of the potential risk factors for cerebrovascular and cardiovascular diseases including arterial stiffness4-6.
Various studies have shown that handgrip is a reliable proxy measure of upper extremity muscle strength and declining handgrip strength has been proved to be a strong predictor of all-cause and cardiovascular mortality in a large multi-country longitudinal study i.e. Prospective Urban-Rural Epidemiology (PURE) study7-9. Therefore, handgrip strength is used as an indicator of muscular fitness, nutritional status, and walking performance and muscle mass10-12.
Moreover, adding handgrip strength (HGS) measurement to traditional office-based risk factors (age, gender, blood pressure, obesity, diabetes mellitus and smoking) in resourced limiting under-served community settings and low and middle-income countries would be beneficial where blood-based measurements are difficult to perform because HGS measurement improves the prediction of office-based risk screeningprocess9,13. Whereas, non-communicable diseases (NCDs) have been on the rise and are contributing progressively to the global and local disease burden and need to be identified and prevented early14.
Keeping in mind the rise of non-communicable diseases among the Pakistani population, the prevalence of coronary artery disease is found to be 29.6%, whereas, males and females are found at equal risk15. The situation for stroke in Pakistan is even worse since the risk factors contributing to stroke are massive and projections reported that Pakistan would be the fourth densely populated country concerning diabetic patients and every third person with 45 years of age would be hypertensive by 2020 16. Some potential risk factors associated with the declining of handgrip strength includes gender, age, body size, smoking and low physical activity have been reported in neighboring regions17.
Hence, measuring an HSG which provides a quick, reliable and budgeted procedure for measuring muscle strength may be useful for risk screening of NCDs, and has the potential to apply as a filtering technique in a clinical setting and thus must have a clinical utility9. Herein, Pakistan, there is only one study available which was carried out for finding normative data for handgrip strength among Karachi resident18. In addition, up to the best of our knowledge, there is no exploration of the factors associated with lower handgrip strength. Therefore, this study aims to assess the handgrip strength and factors associated with lower handgrip strength among adults residing at the urban squatter settlement of Lahore, Punjab.
This is a community-based cross-sectional study conducted in two selected Union Councils -120 and 122 of urban Punjab from February to March 2019. During the health camp, the eligibility criteria to recruit study participants included all adults aged 18 years and above of both genders. A total of 152 participants were recruited through a non-probability convenient sampling method.
Informed verbal and written consent was obtained from each participant. The interview was conducted using a structured questionnaire to extract the information about age, gender, present co-morbidities related to diabetes and hypertension, physical activity. That was defined as walk for 30 minutes daily, current medication history in the form of anti-hypertensive, anti-glycemic and lipid-lowering agents, tobacco use defined as current smoking and/or smokeless tobacco use and frequency of consumption of fruits and vegetables per week.
Anthropometric measurements were recorded including height and weight. Measurements of systolic and diastolic blood pressure and random blood sugar were performed according to standardized methods. Institutional Review Board (IRB) of Shalamar Medical and Dental College, Pakistan approved the study (SMDC/IRB/11-12/140).
A hand-held dynamometer could easily be used in clinical settings to measure the trunk muscle strength in patients with stroke because of its accuracy and affordability19. Analog handgrip dynamometer was used. Muscle strength was defined and measured with respect to handgrip strength by handgrip dynamometer with a protocol according to a standardized approach where a hand is placed in a vertical position and 90-degree elbow flexion and the whole procedure takes 5 minutes to be completed. The measurement is repeated two times with an interval for a while20. Participants with any physical limitations were excluded. Since there was variability in the cutoffs for defining handgrip strength therefore mean standardized score of muscle strength was used in terms of percentiles according to standard method i.e., standardized score was computed by subtracting individual value by mean scores and then divided by the standard deviation. Later, we categorized the sample into high, average and low strength based on the percentile cut-offs i.e. 25th, 50th and 75th respectively21.
Statistical analysis was carried out using SPSS. Mean± SD for continuous variable and percentage (%) were calculated for categorical variables. Chi-square test was done to assess the sample distribution according to the outcome (handgrip strength) variable and p-value less than 0.05 was considered significant. Univariate regression analysis was done and variables with p-value <0.05 in univariate analysis were kept further in multinomial regression model for further assessment. Multinomial regression analysis was done since muscle strength was characterized into three categories i.e. high, average and low muscle strength and therefore to estimate the adjusted odds ratios for associated factors of muscle strength.
A total of 152 participants with mean ±SD age of study participants i.e. 44.5 (±15.3), 95 (62.5%) of females and 57(37.5%) males. Overall, 66(43.4%) of them were currently on medications for chronic diseases. Out of the total, 52(34.2%) were consuming fruits for ≥ 3 days per week, while, 101(66.4%) of participants were consuming vegetables for more than three days per week. Participants who walk daily for thirty minutes were 66(43.4%) and those who use any kind of tobacco product currently were 25 (16.4%) (Table 1).
Table 1: Comparison of factors associated with hang grip strength study participant’s ≥18 years in urban Punjab, Pakistan.
| Characteristics | Total Participants | Muscle Strength | p– Value | ||
| High
n (%) |
Average
n (%) |
Low
n (%) |
|||
| n= 152 | 38 (25.0) | 80 (52.6) | 34 (22.4) | ||
| Gender | |||||
| Male | 57 (37.5) | 28 (73.7) | 21 (26.3) | 08 (23.5) | 0.00 ** |
| Female | 95 (62.5) | 10 (26.3) | 59 (73.8) | 26 (76.5) | |
| Age | |||||
| <40 years | 58 (38.2) | 13 (34.2) | 36 (45.0) | 09 (26.5) | 0.14 |
| ≥ 40 years | 94 (61.8) | 25 (65.8) | 44 (55.0) | 25 (73.5) | |
| Hypertensive | 54 (35.5) | 9 (23.7) | 31 (38.7) | 14 (41.2) | 0.21 |
| Diabetic | 53 (34.9) | 13 (34.2) | 21 (26.3) | 19 (55.9) | 0.01 ** |
| Physical Activity | 66 (43.4) | 21 (55.3) | 31 (38.8) | 14 (41.2) | 0.23 |
| Diastolic Blood Pressure | |||||
| Raised | 37 (24.3) | 33 (86.8) | 57 (71.3) | 25 (73.5) | 0.17 |
| Normal | 115 (75.7) | 05 (13.2) | 23 (28.7) | 09 (26.5) | |
| Systolic Blood Pressure | |||||
| Raised | 39 (25.7) | 31 (81.6) | 57 (71.3) | 25 (73.5) | 0.48 |
| Normal | 113 (74.3) | 07 (18.4) | 23 (28.7) | 09 (26.5) | |
| Blood Sugar Level | |||||
| Normal | 74 (48.7) | 17 (44.7) | 45 (56.3) | 12 (35.3) | 0.11 |
| Raised | 78 (51.3) | 21 (55.3) | 35 (43.7) | 22 (64.7) | |
| Taking Medications | 66 (43.4) | 14 (36.8) | 34 (42.5) | 18 (52.9) | 0.37 |
| Tobacco Use | 25 (16.4) | 13 (34.2) | 10 (12.5) | 02 (5.9) | 0.00 ** |
| Consumption of Fruits per Week | |||||
| < 3 days | 100 (65.8) | 24 (63.2) | 51 (63.7) | 25 (73.5) | 0.56 |
| ≥ 3 days | 52 (34.2) | 14 (36.8) | 29 (36.3) | 09 (26.5) | |
| Consumption of Vegetables per Week | |||||
| > 3 days | 101 (66.4) | 28 (73.7) | 50 (62.5) | 23 (67.6) | 0.47 |
| ≤ 3 days | 51 (33.6) | 10 (26.3) | 30 (37.5) | 11 (32.4) | |
** p-value < 0.05
Muscle strength among study participants was found as high 38(25%), average 50(52.6%) and low 34(22.4%) muscle strength while measured according to the percentile (Figure 1).
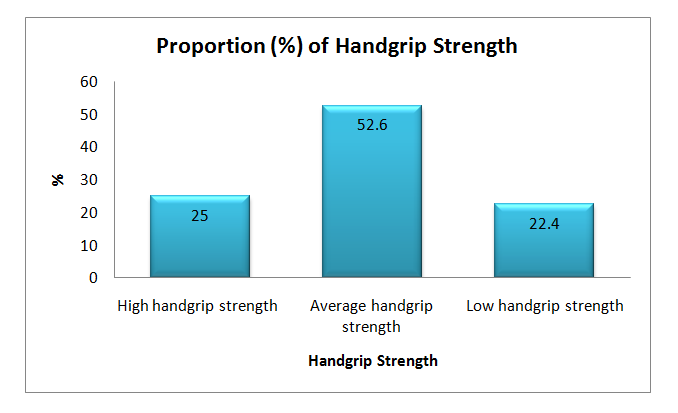
Figure 1: Proportion (%) of with handgrip strength among study participant’s ≥18 years in urban Punjab, Pakistan.
Among the total sample, 26(76.5%) of females have low muscle strength compared to only 8(23.5%) of males and had significant results as the p-value <0.001). Similarly, 28(73.7%) of males have high muscle strength as compared to 10(26.3%) of females with significant results. The difference between muscle strength of non-diabetic and diabetic participants was statistically non-significant (p-value=0.17). Those who are not hypertensive have high muscle strength compared to those who have hypertension (76.3% vs. 23.7%). In this study participants with no tobacco use 25(65.8%) have high muscle strength compared to 13(34.2%) of tobacco users (<0.05) (Table 1).
Multinomial logistic regression analysis (Table 2) for factors associated with average and low muscle strength shows females are 7.9 times more likely to have low muscle strength as compared to males and the result is statistically significant (p-value <0.001). With reference to the analogue handgrip dynamometer (Figure 2), two significant aspects were presented which were showing an original position vs. handgrip strength measurement.
Table 2: Multinomial logistic regression analysis for factors associated with hang grip strength among study participant’s ≥18 years.
|
Characteristics |
Average muscle strength |
p-Value |
Low muscle strength |
p-Value |
| OR (95% CI) | OR (95% CI) | |||
| Gender | ||||
| Male | 1 | 1 | ||
| Female | 6.4 (2.3-17.2) | 0.00 | 7.9 (2.4-27.1) | 0.00 ** |
| Age | ||||
| <40 years | 1 | 1 | ||
| ≥ 40 years | 1.3 (0.4-3.8) | 0.66 | 2.4 (0.6-9.7) | 0.19 |
| Hypertensive | 1.5 (0.5-4.9) | 0.38 | 1.1 (0.3-3.5) | 0.91 |
| Non-hypertensive | 1 | 1 | ||
| Diabetic | 1.1 (0.3-3.7) | 0.89 | 3.1 (0.7-13.2) | 0.11 |
| Non-diabetic | 1 | 1 | ||
| Physically Active | 1 | 1 | ||
| Physically Inactive | 1.5 (0.5-3.7) | 0.38 | 1.4 (0.4-4.3) | 0.51 |
| Tobacco user | 1.5 (0.4-4.9) | 0.49 | 3.2 (0.5-19.1) | 0.18 |
| Tobacco Avoidance | 1 | |||
** p-value < 0.05
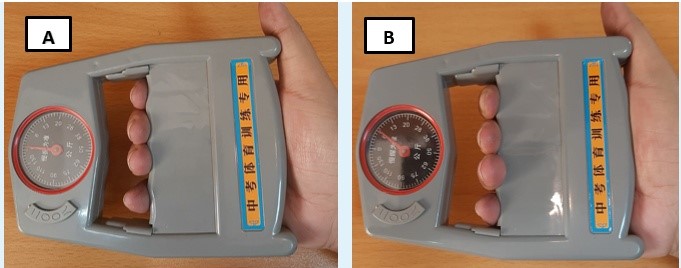
Figure 2: Analogue handgrip dynamometer (Image A: Original position; Image B: Measuring handgrip strength).
In this exploratory study, overall 80 adult participants have an average (52.6%) and low (22.4%) muscle strength and findings are comparable to those reported for Malaysian populations22. Similar findings were reported for European and American adults where weaker handgrip strength was found overall in the study population23, 24.
Since previous studies have established a correlation between muscle strength and age where it highlighted that muscle strength increases till the age of 38 years and then decreases steadily afterwards22. In our study, odds ratio of low handgrip strength is high (OR: 2.5) among participants age 40 years and above. However, the association could not be significantly established which might be due to the small sample size. A study showed a pooled data from six cohort studies reporting low handgrip strength as a potential risk factor for all-cause mortality among older age population 25.
Concerning gender, our study is showing significant association and reporting higher odds of low handgrip strength among females compared to males (OR: 6.7). These results are similar to several other previous findings. However, another study has demonstrated a comparative finding among Malaysian adults where male participants had consistently stronger handgrip measurement with an odds ratio of 1.75 times higher compared to females across all age group22. Factors underlying the difference in handgrip strength among genders were body mass index and waist circumference, which mediate the effect of handgrip strength. These factors may play role in developing cardiovascular diseases among males and females, which was evaluated in a study conducted among Korean adult population26.
Abundant evidence suggests that low handgrip strength is significantly linked with a high risk of cardiovascular diseases (CVD) and its related risk factors such as diabetes, hypertension, dyslipidemia and obesity 26,27. In our study, low strength is higher among those participants who had hypertension (OR: 1.1), diabetes (OR: 2.7) and tobacco users (OR: 3.4). In accordance with our study findings, there are other surveys conducted among Korean and Hispanic population, which is also showing that low handgrip strength is significantly related to cardiovascular risk factors and cardiovascular fitness respectively, among adults 4,26,28. However, studies have also reported that low handgrip strength is not a predictor of cardiovascular risk29. Therefore, the contrary findings among different studies appeal for further large-scale community-based research with a robust methodology.
Physical activity increases muscular functional capacity and cardio-respiratory fitness (CRF) and the latter one is an established predictor for cardiovascular disease morbidity in the future30. Similarly, in our study multinomial regression result is showing that odds of low strength is higher (OR: 1.5) among participants with no physical activity. Other robust cohort studies reporting similar findings that low physical fitness is significantly associated with low muscular strength21,30.
The strength of the study includes the participants were selected from a community, which is challenging in terms of refusals. The measurement of handgrip strength with respect to percentile is representing the meaningful result of the outcome and can be used further for applying certain interventions in a specific community. However, there are some limitations of participants selection in the study were at-risk population; hence, the results cannot be generalized to a healthy population. It is an exploratory study among people who attended the health camp and having co-morbidities so findings cannot be generalized to the whole population and cannot be conclusive. However, the findings can generate only the hypothesis, which can be explored further in future studies. Up to the best of our knowledge, this study is novel for assessing muscle strength in a community-based setting in Punjab
The participants are having either average and low muscle strength and regression analysis showed that females are at high risk of having low muscle strength. Therefore, it can be suggested that the handgrip dynamometer, an economic tool, used as a proxy measurement of upper extremity muscle strengthen a community based clinical settings. It is easy to measure and a low-cost technique for risk-scoring and risk-prediction of cardiovascular disease and cerebrovascular disease such as stroke, as evident by literature, and thus to identify high-risk people beforehand.
All authors acknowledge Department of Community Medicine, Department of Marketing and Administrative of Shalamar Medical and Dental College for the smooth rolling of this survey.
The authors have no conflicts of interest.
Institution Review Board (IRB) of Shalamar Medical and Dental College, Pakistan approved the study “Prevention of coronary artery diseases in urban slums of Lahore” with reference # SMDC/IRB/11-12/140.
Informed verbal and written consent were obtained from participants.
This study was funded through the Shahid Hussain Foundation only for the data collection process and campaign purpose. Funding source did not play any role in the design, reporting and publication of this study.
TK conceived the idea and supervised the manuscript writing. SR performed statistical analysis and wrote the initial complete manuscript. AK, AS and JAN did the literature search and contributed in data collection. TK and SS critically reviewed whole manuscript and every author has approved the final verdict of the manuscript.
- Jang SK, Kim JH, Lee Y. Effect of relative handgrip strength on cardiovascular disease among Korean adults aged 45 years and older: Results from the Korean Longitudinal Study of Aging (2006–2016). Arch Gerontol Geriatr. 2020;86:103937.
- Ji C, Zheng L, Zhang R, Wu Q, Zhao Y. Handgrip strength is positively related to blood pressure and hypertension risk: results from the National Health and nutrition examination survey. Lipids Health Dis. 2018;17(1):1-7.
- World Health Organization. Technical package for cardiovascular disease management in primary health care. Geneva, Switzerland. 2016 [Internet]. World Health Organization, 2016 [cited 2020 Jun 16]. Available from: https://www.who.int/cardiovascular_diseases/hearts/Hearts_package.pdf
- Artero EG, Lee DC, Lavie CJ, España-Romero V, Sui X, Church TS, et al Effects of muscular strength on cardiovascular risk factors and prognosis. J Cardiopulm Rehabil Prev. 2012; 32(6): 351-358.
- Cooper R, Kuh D, Cooper C, Gale CR, Lawlor DA, Matthews F, et al. Objective measures of physical capability and subsequent health: a systematic review. Age Ageing. 2010;40(1):14-23.
- Fahs CA, Heffernan KS, Ranadive S, Jae SY, Fernhall B. Muscular strength is inversely associated with aortic stiffness in young men. Med Sci Sports Exerc. 2010;42(9):1619-1624.
- Leong DP, Teo KK, Rangarajan S, Lopez-Jaramillo P, Avezum Jr A, Orlandini A, et al. Prognostic value of grip strength: findings from the Prospective Urban Rural Epidemiology (PURE) study. Lancet. 2015;386(9990):266-273.
- Wu Y, Wang W, Liu T, Zhang D. Association of grip strength with risk of all-cause mortality, cardiovascular diseases, and cancer in community-dwelling populations: a meta-analysis of prospective cohort studies. J Am Med Dir Assoc. 2017;18(6):551.e17-e35.
- Celis-Morales CA, Welsh P, Lyall DM, Steell L, Petermann F, Anderson J, et al. Associations of grip strength with cardiovascular, respiratory, and cancer outcomes and all cause mortality: prospective cohort study of half a million UK Biobank participants. BMJ. 2018 8;361:1-10.
- Willems SM, Wright DJ, Day FR, Trajanoska K, Joshi PK, Morris JA, et al. Large-scale GWAS identifies multiple loci for hand grip strength providing biological insights into muscular fitness. Nat Commun. 2017;8(1):1-2.
- Springstroh KA, Gal NJ, Ford AL, Whiting SJ, Dahl WJ. Evaluation of handgrip strength and nutritional risk of congregate nutrition program participants in Florida. J Nutr Gerontol Geriatr. 2016;35(3):193-208.
- Granic A, Jagger C, Davies K, Adamson A, Kirkwood T, Hill TR, et al. Effect of dietary patterns on muscle strength and physical performance in the very old: findings from the newcastle 85+ study. PLoS One. 2016;11(3):e0149699.
- Ueda P, Woodward M, Lu Y, Hajifathalian K, Al-Wotayan R, Aguilar-Salinas CA, et al. Laboratory-based and office-based risk scores and charts to predict 10-year risk of cardiovascular disease in 182 countries: a pooled analysis of prospective cohorts and health surveys. Lancet Diabetes Endocrinol. 2017;5(3):196-213.
- Murray CJ, Vos T, Lozano R, Naghavi M, Flaxman AD, Michaud C, et al. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2197-223.
- Jafar TH, Jafary FH, Jessani S, Chaturvedi N. Heart disease epidemic in Pakistan: women and men at equal risk. Am Heart J. 2005;150(2):221-226.
- Khealani BA, Hameed B, Mapari UU. Stroke in Pakistan. J Pak Med Assoc. 2008;58(7):400-403.
- Stenholm S, Tiainen K, Rantanen T, Sainio P, Heliövaara M, Impivaara O, et al. Long‐term determinants of muscle strength decline: prospective evidence from the 22‐year mini‐Finland follow‐up survey. J Am Geriatr Soc. 2012;60(1):77-85.
- Jawaria S. Evaluation of pakistani adult handgrip strength reference values through dynamometer. J Pak Orthop Assoc. 2017;29(04):139-144.
- Karthikbabu S, Chakrapani M. Hand-held dynamometer is a reliable tool to measure trunk muscle strength in chronic stroke. J Clin Diagn Res. 2017;11(9): YC09-YC12.
- Roberts HC, Denison HJ, Martin HJ, Patel HP, Syddall H, Cooper C, et al. A review of the measurement of grip strength in clinical and epidemiological studies: towards a standardised approach. Age Ageing. 2011;40(4):423-429.
- Timpka S, Petersson IF, Zhou C, Englund M. Muscle strength in adolescent men and risk of cardiovascular disease events and mortality in middle age: a prospective cohort study. BMC Med. 2014;12(1):62-69.
- Kamarul T, Ahmad TS, Loh W. Hand grip strength in the adult Malaysian population. J Orthop Surg. 2006;14(2):172-177.
- Petersen P, Petrick M, Connor H, Conklin D. Grip strength and hand dominance: challenging the 10% rule. Am J Occup Ther. 1989;43(7):444-447.
- Crosby CA, Wehbé MA. Hand strength: normative values. J Hand Surg Am. 1994;19(4):665-670.
- McLean RR, Shardell MD, Alley DE, Cawthon PM, Fragala MS, Harris TB, et al. Criteria for clinically relevant weakness and low lean mass and their longitudinal association with incident mobility impairment and mortality: the foundation for the National Institutes of Health (FNIH) sarcopenia project. J Gerontol A Biol Sci Med Sci. 2014;69(5):576-583.
- Lee MR, Jung SM, Kim HS, Kim YB. Association of muscle strength with cardiovascular risk in Korean adults: findings from the Korea National Health and Nutrition Examination Survey (KNHANES) VI to VII (2014–2016). Med. 2018;97(47):1-7.
- Cheung C-L, Nguyen U-SD, Au E, Tan KC, Kung AW. Association of handgrip strength with chronic diseases and multimorbidity. Age. 2013;35(3):929-941.
- Xu L, Hao YT. Effect of handgrip on coronary artery disease and myocardial infarction: a Mendelian randomization study. Sci Rep. 2017;7(1):1-5.
- Kodama S, Saito K, Tanaka S, Maki M, Yachi Y, Asumi M, et al. Cardiorespiratory fitness as a quantitative predictor of all-cause mortality and cardiovascular events in healthy men and women: a meta-analysis. JAMA. 2009;301(19):2024-2035.
- Yates T, Zaccardi F, Dhalwani NN, Davies MJ, Bakrania K, Celis-Morales CA, et al. Association of walking pace and handgrip strength with all-cause, cardiovascular, and cancer mortality: a UK Biobank observational study. Eur Heart J. 2017;38(43):3232-3240.
This is an open-access article distributed under the terms of the CreativeCommons Attribution License (CC BY) 4.0 https://creativecommons.org/licenses/by/4.0/