
Epidemiology and Transmitted HIV-1 Drug Resistance among Treatment-Naïve Individuals in Israel, 2010–2018


 , add
Show full author list
, add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Genotyping
2.3. Phylogenetic Analysis, Statistical Analysis and Ethical Approval
3. Results
3.1. Epidemiology
3.2. HIV-1 Subtypes and Resistance Mutations
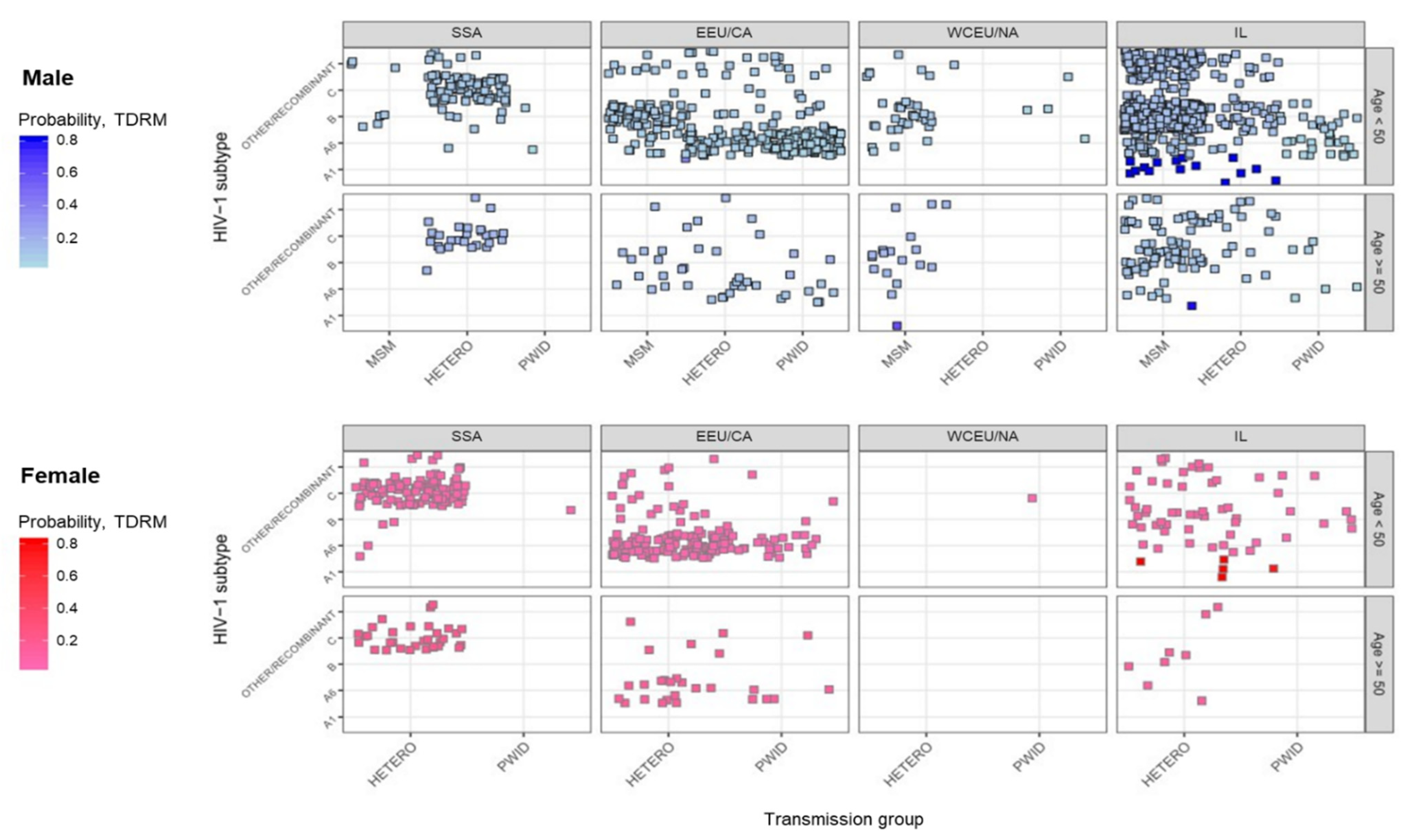
3.3. Multidimensional Mapping
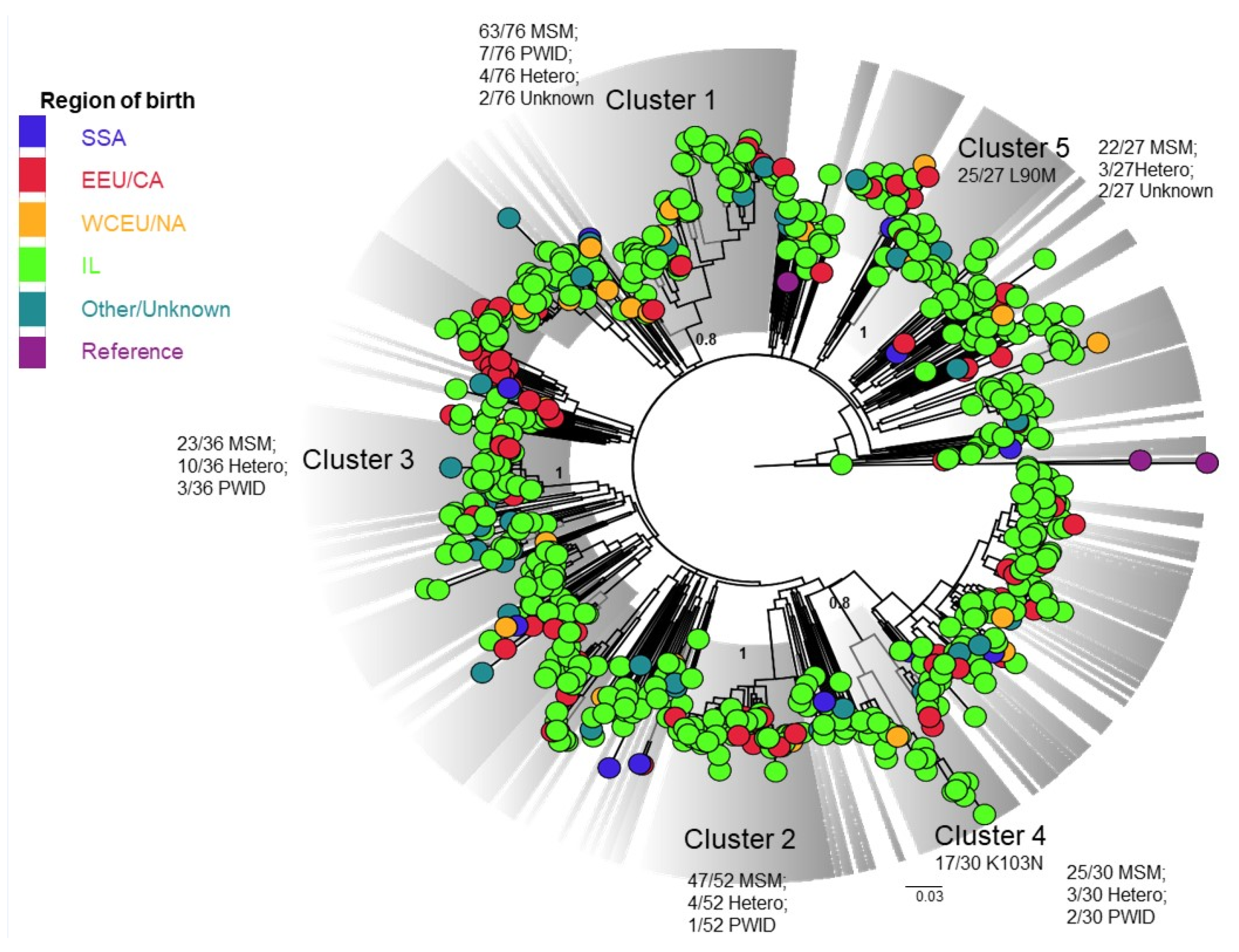
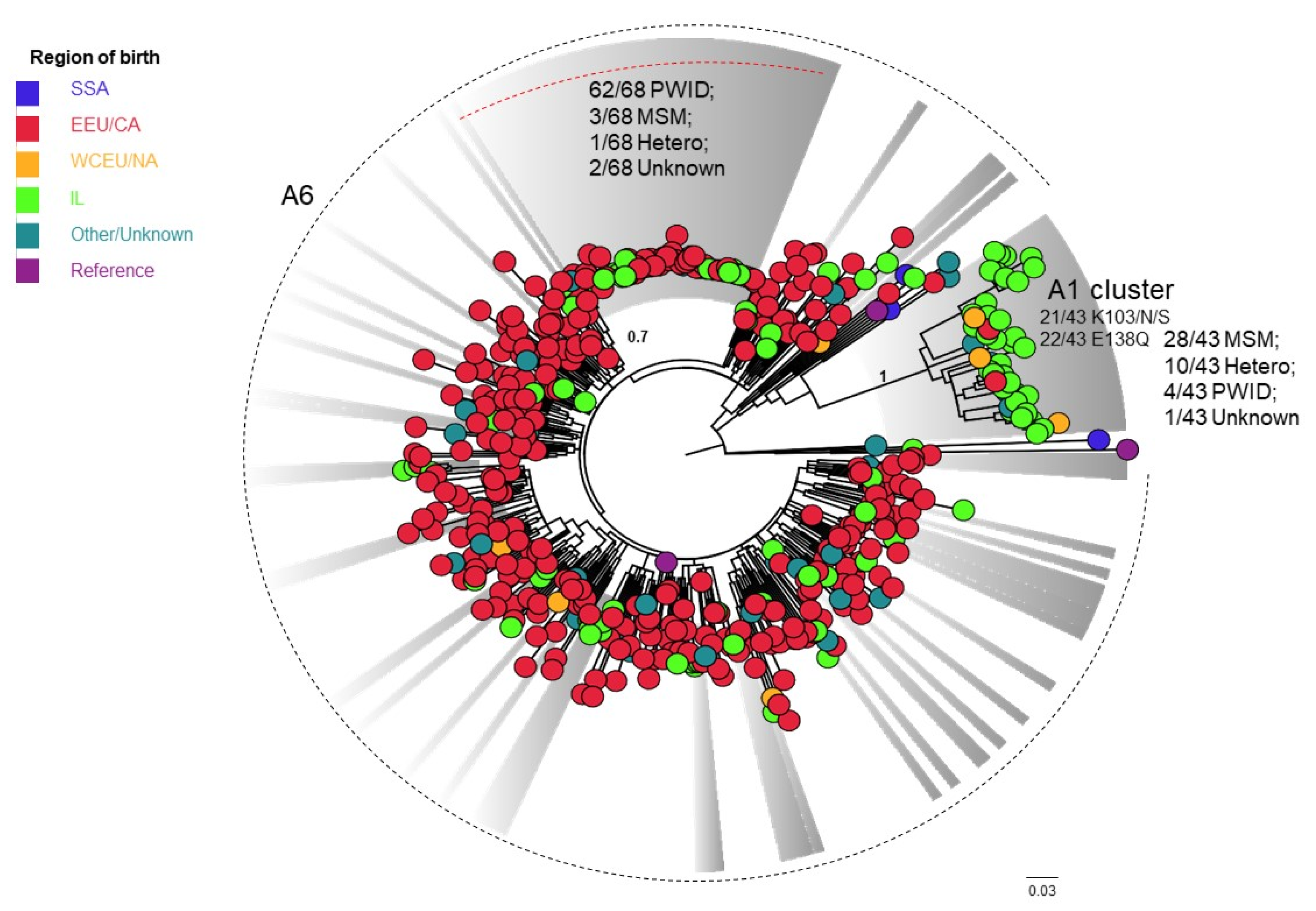
3.4. Phylogenetic Analysis
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mor, Z.; Weinstein, R.; Grotto, I.; Levin, Y.; Chemtob, D. Thirty years of HIV in Israel: Current epidemiology and future challenges. BMJ Open 2013, 3, e003078. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wagner, T.; Olshtain-Pops, K.; Wax, M.; Horwitz, O.; Shirazi, R.; Gozlan, Y.; Volnowitz, H.; Mendelson, E.; Levy, I.; Mor, O. HIV-1 infection among women in Israel, 2010–2018. BMC Infect. Dis. 2020, 20, 660. [Google Scholar] [CrossRef] [PubMed]
- Israel Seen. Israel: A Melting Pot of Cultures. 2012. Available online: https://israelseen.com/2012/05/29/israel-a-melting-pot-of-cultures (accessed on 31 December 2020).
- Jewish Virtual Library. Total Immigration to Israel by Select Country by Year (1948–Present). Available online: https://www.jewishvirtuallibrary.org/total-immigration-to-israel-by-country-per-year (accessed on 31 March 2021).
- Zuckerman, N.S.; Mor, Z.; Bucris, E.; Wax, M.; Mendelson, E.; Mor, O. Sexual intermingling of Arab and Jewish MSM in Israel: Results of a molecular epidemiology study. AIDS 2019, 33, 339–344. [Google Scholar] [CrossRef] [PubMed]
- Chemtob, D.; Grossman, Z. Epidemiology of adult and adolescent HIV infection in Israel: A country of immigration. Int. J. STD AIDS 2004, 15, 691–696. [Google Scholar] [CrossRef]
- Grossman, Z.; Avidor, B.; Mor, Z.; Chowers, M.; Levy, I.; Shahar, E.; Riesenberg, K.; Sthoeger, Z.; Maayan, S.; Shao, W.; et al. A Population-Structured HIV Epidemic in Israel: Roles of Risk and Ethnicity. PLoS ONE 2015, 10, e0135061. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Désiré, N.; Cerutti, L.; Le Hingrat, Q.; Perrier, M.; Emler, S.; Calvez, V.; Descamps, D.; Marcelin, A.-G.; Hué, S.; Visseaux, B. Characterization update of HIV-1 M subtypes diversity and proposal for subtypes A and D sub-subtypes reclassification. Retrovirology 2018, 15, 80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mendes da Silva, R.K.; Monteiro de Pina Araujo, I.I.; Venegas Maciera, K.; Gonçalves Morgado, M.; Lindenmeyer Guimarães, M. Genetic Characterization of a New HIV-1 Sub-Subtype A in Cabo Verde, Denominated A8. Viruses 2021, 13, 1093. [Google Scholar] [CrossRef] [PubMed]
- Schlösser, M.; Kartashev, V.V.; Mikkola, V.H.; Shemshura, A.; Saukhat, S.; Kolpakov, D.; Suladze, A.; Tverdokhlebova, T.; Hutt, K.; Heger, E.; et al. HIV-1 Sub-Subtype A6: Settings for Normalised Identification and Molecular Epidemiology in the Southern Federal District, Russia. Viruses 2020, 12, 475. [Google Scholar] [CrossRef] [Green Version]
- Grossman, Z.; Lorber, M.; Maayan, S.; Yacov, N.B.; Levy, I.; Averbuch, D.; Istomin, V.; Chowers, M.; Sthoeger, Z.; Ram, D.; et al. Drug-Resistant HIV Infection among Drug-Naive Patients in Israel. Clin. Infect. Dis. 2005, 40, 294–302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grossman, Z.; Avidor, B.; Girshengoren, S.; Katchman, E.; Maldarelli, F.; Turner, D. Transmission Dynamics of HIV Subtype A in Tel Aviv, Israel: Implications for HIV Spread and Eradication. Open Forum Infect. Dis. 2019, 6, ofz304. [Google Scholar] [CrossRef] [PubMed]
- Menza, T.W.; Billock, R.; Samoff, E.; Eron, J.J.; Dennis, A.M. Pretreatment integrase strand transfer inhibitor resistance in North Carolina from 2010–2016. AIDS 2017, 31, 2235–2244. [Google Scholar] [CrossRef] [PubMed]
- Bennett, D.E.; Camacho, R.J.; Otelea, D.; Kuritzkes, D.R.; Fleury, H.; Kiuchi, M.; Heneine, W.; Kantor, R.; Jordan, M.R.; Schapiro, J.M.; et al. Drug Resistance Mutations for Surveillance of Transmitted HIV-1 Drug-Resistance: 2009 Update. PLoS ONE 2009, 4, e4724. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- HIV Drug Resistance Database (HIVDB). 2021. Available online: https://hivdb.stanford.edu/ (accessed on 12 December 2021).
- Casado, J.L.; Monsalvo, M.; Fontecha, M.; Vizcarra, P.; A Rodriguez, M.; Vivancos, M.J.; Moreno, S. Dolutegravir plus rilpivirine as dual regimen in virologically suppressed HIV-1 infected patients in a clinical setting. HIV Res. Clin. Pract. 2019, 20, 64–72. [Google Scholar] [CrossRef] [PubMed]
- Moscona, R.; Ram, D.; Wax, M.; Bucris, E.; Levy, I.; Mendelson, E.; Mor, O. Comparison between next-generation and Sanger-based sequencing for the detection of transmitted drug-resistance mutations among recently infected HIV-1 patients in Israel, 2000–2014. J. Int. AIDS Soc. 2017, 20, 21846. [Google Scholar] [CrossRef] [PubMed]
- Avidor, B.; Girshengorn, S.; Matus, N.; Talio, H.; Achsanov, S.; Zeldis, I.; Fratty, I.S.; Katchman, E.; Brosh-Nissimov, T.; Hassin, D.; et al. Evaluation of a Benchtop HIV Ultradeep Pyrosequencing Drug Resistance Assay in the Clinical Laboratory. J. Clin. Microbiol. 2013, 51, 880–886. [Google Scholar] [CrossRef] [Green Version]
- Van de Laar, M.J.; Bosman, A.; Pharris, A.; Andersson, E.; Assoumou, L.; Ay, E.; Bannert, N.; Bartmeyer, B.; Brady, M.; Chaix, M.L.; et al. Piloting a surveillance system for HIV drug resistance in the European Union. Euro Surveill. 2019, 24, 1800390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The Jewish Agency for Israel. 2007. Available online: https://archive.jewishagency.org/he/historical-aliyah/content/22095 (accessed on 19 May 2021).
- Ministry of Aliyah and Integration. 2020. Available online: https://www.gov.il/en/Departments/General/aliyah_slomo (accessed on 18 May 2021).
- Emergency Care Data Set (ECDS). HIV/AIDS Surveillance in Europe 2018 Data; Emergency Care Data Set (ECDS): Stockholm, Sweden, 2019. [Google Scholar]
- Beloukas, A.; Psarris, A.; Giannelou, P.; Kostaki, E.; Hatzakis, A.; Paraskevis, D. Molecular epidemiology of HIV-1 infection in Europe: An overview. Infect. Genet. Evol. 2016, 46, 180–189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chowers, M.; Chemtob, D.; Mor, O.; Levy, I.; Elbirt, D.; Elinav, H.; Rizenberg, K.; Lorber, M.; Istomin, V.; Nemet, S.; et al. Continuum of HIV care of newly diagnosed individuals in Israel, 2011–2015: A population-based cohort study. Int. J. STD AIDS 2020, 31, 326–334. [Google Scholar] [CrossRef] [PubMed]
- Levy, I.; Maor, Y.; Mahroum, N.; Liraz, O.; Wieder, A.; Litchevski, V.; Mor, O.; Rahav, G. Data from: Missed opportunities for earlier diagnosis of HIV in patients that presented with advanced HIV disease: A retrospective cohort study. BMJ Open 2016, 6, e012721. [Google Scholar] [CrossRef] [Green Version]
- Late Presenters Working Group in COHERE in EuroCoord; Mocroft, A.; Lundgren, J.; Antinori, A.; Monforte Ad, B.J.; Bonnet, F. Late presentation for HIV care across Europe: Update from the Collaboration of Observational HIV Epidemiological Research Europe (COHERE) study, 2010 to 2013. Euro Surveill. 2015, 20, 10–2807. [Google Scholar]
- World Health Organization (WHO) Team HIV/AIDS. HIV Drug Resistance Report 2019. 2019. Available online: https://www.who.int/hiv/pub/drugresistance/hivdr-report-2019/en/ (accessed on 9 December 2021).
- Wang, Y.; de Clercq, E.; Li, G. Current and emerging non-nucleoside reverse transcriptase inhibitors (NNRTIs) for HIV-1 treatment. Expert Opin Drug Metab Toxicol. 2019, 15, 813–829. [Google Scholar] [CrossRef] [PubMed]
- Lehman, D.A.; Baeten, J.M.; McCoy, C.O.; Weis, J.F.; Peterson, D.; Mbara, G.; Donnell, D.; Thomas, K.K.; Hendrix, C.W.; Marzinke, M.A.; et al. Risk of Drug Resistance Among Persons Acquiring HIV Within a Randomized Clinical Trial of Single- or Dual-Agent Preexposure Prophylaxis. J. Infect. Dis. 2015, 211, 1211–1218. [Google Scholar] [CrossRef] [PubMed]
- Smith, S.J.; Zhao, X.Z.; Burke, T.R.; Hughes, S.H. Efficacies of Cabotegravir and Bictegravir against drug-resistant HIV-1 integrase mutants. Retrovirology 2018, 15, 37. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All (N = 3639) | 2010–2012 (N = 1264) | 2013–2015 (N = 1294) | 2016–2018 (N = 1081) | p-Value | |
|---|---|---|---|---|---|
| Age at diagnosis (years), median (IQR) (n = 3500) | 37 (30–45) | 36 (29–44) | 37 (31–45) | 38 (32–46) | <0.001 |
| Sex, n (%) | |||||
| Female | 1032 (28.4) | 361 (28.6) | 355 (27.4) | 316(29.2) | 0.025 |
| Male | 2561 (70.4) | 883 (69.9) | 922 (71.3) | 756 (69.9) | |
| Trans people | 12 (0.3) | 1 (0.1) | 5 (0.4) | 6 (0.6) | |
| Unknown | 34 (0.9) | 19 (1.5) | 12 (0.9) | 3 (0.3) | |
| Place of birth, n (%) | |||||
| Sub-Saharan Africa | 640 (17.6) | 267 (21.1) | 191 (14.8) | 182 (16.8) | <0.001 |
| Eastern Europe and Central Asia | 901 (24.8) | 266 (21) | 334 (25.8) | 301 (27.8) | |
| Israel | 1206 (33.1) | 415 (32.8) | 450 (34.8) | 341 (31.5) | |
| West/Central Europe/North America | 83 (2.3) | 23 (1.8) | 28 (2.2) | 32 (3) | |
| Other/Unknown | 809 (22.2) | 293 (23.2) | 291 (22.5) | 225 (20.8) | |
| Transmission Groups, n (%) | |||||
| Men who have sex with men | 1248 (34.3) | 432 (34.2) | 451 (34.9) | 365 (33.8) | <0.001 |
| Heterosexual contacts | 1424 (39.1) | 440 (34.8) | 504 (38.9) | 480 (44.4) | |
| Injecting drug users | 380 (10.4) | 162 (12.8) | 149 (11.5) | 69 (6.4) | |
| Unknown | 587 (16.1) | 230 (18.2) | 190 (14.7) | 167 (15.4) | |
| CD4 (cells/mm3), N (%) | N = 1899 | N = 704 (37.1) | N = 730 (38.4) | N = 465 (24.5) | |
| CD4 (cells/mm3), median (IQR) | 354 (187–544) | 351 (183–540) | 357 (193–544) | 360 (186–557) | 0.91 |
| HIV-1-RNA (Log copies/mL), N (%) | N = 2103 | N = 771 (36.7) | N = 814 (38.7) | N = 518 (24.6) | |
| HIV-1-RNA (Log copies/mL), median (IQR) | 4.7 (4.1–4.7) | 4.7 (4.0–5.2) | 4.7 (4.1–5.3) | 4.9 (4.3–5.5) | <0.001 |
| HIV-1 Subtype (n = 1957), N (%) | N = 1957 | N = 694 (35.5) | N = 741 (37.9) | N = 522 (26.7) | |
| A1 | 46 (2.4) | 15 (2.2) | 24 (3.2) | 7 (1.3) | <0.001 |
| A6 | 446 (22.8) | 156 (22.5) | 167 (22.5) | 123 (23.6) | |
| B | 860 (43.9) | 336 (48.4) | 330 (44.5) | 194 (37.2) | |
| C | 335 (17.1) | 130 (18.7) | 119 (16.1) | 86 (16.5) | |
| Other/Recombinant form | 270 (13.8) | 57 (8.2) | 101 (13.6) | 112 (21.5) | |
| TDRM by class (N = 1905), n (%) | 231 (12.1) | 70 (10.5) | 96 (13.3) | 65 (12.6) | 0.221 |
| NNRTI | 125 (6.6) | 39 (5.8) | 48 (6.6) | 38 (7.4) | 0.282 |
| NRTI | 62 (3.3) | 28 (4.2) | 19 (2.6) | 15 (2.9) | 0.188 |
| PI | 71 (3.7) | 19 (2.8) | 30 (4.1) | 22 (4.3) | 0.177 |
| HIVdrm by class (N = 1905), n (%) ECDC algorithm | 413 (21.7) | 122 (18.3) | 168 (23.2) | 123 (23.9) | 0.015 |
| NNRTI | 238 (12.5) | 72 (10.8) | 105 (14.5) | 61 (11.9) | 0.466 |
| NRTI | 118 (6.2) | 42 (6.3) | 35 (4.8) | 41 (8) | 0.3 |
| PI | 112 (5.9) | 28 (4.2) | 50 (6.9) | 34 (6.6) | 0.061 |
| Sub-Saharan Africa (N = 640) | Eastern Europe/Central Asia (N = 901) | Israel (N = 1206) | Western/Central Europe/North America (N = 83) | p-Value | |
|---|---|---|---|---|---|
| Age at diagnosis, N = 2784, (98.4%) | 605 (21.7) | 892 (32) | 1205 (43.3) | 82 (2.9) | |
| Years, Median (IQR) | 39 (32–48) | 38 (32–45) | 35 (28–43) | 43 (31–52) | <0.001 |
| ≥50, n= 426 (15.3%) | 129 (21.3) | 129 (14.1) | 146 (12.1) | 25(30.5) | <0.001 |
| <50, n = 2358 (84.7%) | 476 (78.7) | 773 (85.9) | 1059 (87.9) | 57(69.5) | |
| Sex, N = 2819 (99%) | 631(22.4) | 900 (31.9) | 1205 (42.7) | 83 (2.9) | |
| Female, n = 775 (27.5%) | 327 (51.8) | 352 (39.1) | 92 (7.6) | 4 (4.8) | <0.001 |
| Male, n = 2033 (72.1%) | 304 (48.2) | 545 (60.6) | 1106 (91.8) | 78 (94) | |
| Trans people, n = 11 (0.4%) | 0 | 3 (0.3) | 7 (0.6) | 1 (1.2) | |
| Transmission Groups, (N = 2792), n (99%) | 640 (22.9) | 901 (32.3) | 1175 (42.1) | 76(2.7) | |
| Men who have sex with men, n = 1122 (40.2%) | 11 (1.7) | 128 (14.2) | 920 (78.3) | 63 (82.9) | <0.001 |
| Heterosexual contacts, n = 1328 (47.6%) | 625 (97.7) | 513 (56.9) | 182 (15.5) | 8 (10.5) | |
| Injecting drug users, n = 342 (12.2%) | 4 (0.6) | 260 (28.9) | 73 (6.2) | 5 (6.6) | |
| HIV-1 subtype (n = 1787), n (91.6%) | 268 (15) | 490 (27.4) | 972 (54.4) | 57 (3.2) | |
| A1, n = 42 (2.4%) | 0 | 2 (0.4) | 37 (3.8) | 3 (5.3) | <0.001 |
| A6, n = 412 (23.1%) | 4 (1.5) | 328 (66.9) | 75 (7.7) | 5 (8.8) | |
| B, n = 809 (45.3%) | 16 (6) | 99 (20.2) | 659 (67.8) | 35 (61.4) | |
| C, n = 290 (16.2%) | 215 (80.2) | 23 (4.7) | 48 (4.9) | 4(7) | |
| Other/recombinant, n = 234 (13.1%) | 33 (12.3) | 38 (7.8) | 153 (15.7) | 10 (17.5) | |
| CD4 (N = 1722), n (61%) | (N = 254) | (N = 469) | (N = 953) | (N = 46) | |
| CD4 (cells/mm3) Median (IQR) | 219 (103–369) | 323 (141–540) | 400 (242–588) | 403 (267–552) | <0.001 |
| HIV-1 RNA, N = 1895, n (67.6%) | (N = 303) | (N = 525) | (N = 1010) | (N = 57) | |
| HIV-1 RNA log copies/mL, Median (IQR) | 4.7 (3.8–5.5) | 4.7 (4.1–5.3) | 4.8 (4.2–5.3) | 4.8 (4.1–5.2) | 0.132 |
| TDRM by class, N = 1741, n (%) | 32 (12.8) | 39 (8.1) | 140 (14.7) | 9 (16.4) | 0.004 |
| NNRTI | 18 (7.2) | 16 (3.3) | 82 (8.6) | 3 (5.5) | 0.003 |
| NRTI | 14 (5.6) | 18 (3.7) | 23 (2.4) | 3 (5.5) | 0.057 |
| PI | 8 (3.2) | 12 (2.5) | 44 (4.6) | 4(7.3) | 0.120 |
| HIVdrm by class, N = 1741, n (%) ECDC algorithm | 48 (19.2) | 114 (23.7) | 205 (21.5) | 17 (30.9) | 0.205 |
| NNRTI | 35 (14) | 50 (10.4) | 128 (13.4) | 7 (12.7) | 0.364 |
| NRTI | 16 (6.4) | 54 (11.2) | 30 (3.1) | 6 (10.9) | <0.001 |
| PI | 10 (4) | 25 (5.2) | 64 (6.7) | 8 (14.5) | 0.018 |
| Drug Class | Mutation | All, N = 1905 | A1, N = 46 | A6, N = 436 | B, N = 841 | C, N = 318 | Other, N = 264 | p-Value |
|---|---|---|---|---|---|---|---|---|
| PI, n (%) | L90M | 39 (2) | 2 (0.4) | 34 (4) | 1 (0.3) | 2 (0.8) | B vs. A6/C, <0.001 | |
| NRTI, n (%) | A62V | 51 (2.7) | 49 (11) | 2 (0.6) | A6 vs. C, <0.001 | |||
| M184IV | 18 (0.9) | 7 (1.6) | 5 (0.6) | 6(1.9) | B vs. C, 0.043 | |||
| NNRTI, n (%) | K103N | 86 (4.5) | 16 (35) | 5 (1.1) | 53 (6.3) | 7 (2.2) | 5 (1.9) | A1 vs. all, <0.001 A1 vs. B/Other, <0.001 A6/B/C vs. Other ≤ 0.01 A1 vs. B, <0.001 NS A1 vs. A6/B/C, <0.001 |
| K103S | 8 (0.4) | 6 (13) | 1 (0.1) | 1 (0.4) | ||||
| E138A | 70 (3.7) | 1 (2.2) | 17 (3.9) | 21 (2.5) | 10 (3.1) | 21 (8) | ||
| E138G | 10 (0.5) | 2 (4.3) | 4 (0.9) | 1 (0.1) | 2 (0.6) | 1 (0.7) | ||
| E138K | 3 (0.2) | 1 (0.2) | 1 (0.1) | 1 (0.3) | ||||
| E138Q | 26 (1.4) | 22 (48) | 1 (0.2) | 2 (0.2) | 1 (8) | |||
| INSTI, n (%) | All, N = 479 | A1, N = 8 | A6, N = 112 | B, N = 202 | C, N = 65 | Other, N = 92 | ||
| L74I | 44 (9.2) | 38 (34) | 3 (1.5) | 1 (1.5) | 2 (2.2) | A6 vs. all, <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wagner, T.; Zuckerman, N.S.; Halperin, T.; Chemtob, D.; Levy, I.; Elbirt, D.; Shachar, E.; Olshtain-Pops, K.; Elinav, H.; Chowers, M.; et al. Epidemiology and Transmitted HIV-1 Drug Resistance among Treatment-Naïve Individuals in Israel, 2010–2018. Viruses 2022, 14, 71. https://doi.org/10.3390/v14010071
Wagner T, Zuckerman NS, Halperin T, Chemtob D, Levy I, Elbirt D, Shachar E, Olshtain-Pops K, Elinav H, Chowers M, et al. Epidemiology and Transmitted HIV-1 Drug Resistance among Treatment-Naïve Individuals in Israel, 2010–2018. Viruses. 2022; 14(1):71. https://doi.org/10.3390/v14010071
Chicago/Turabian StyleWagner, Tali, Neta S. Zuckerman, Tami Halperin, Daniel Chemtob, Itzchak Levy, Daniel Elbirt, Eduardo Shachar, Karen Olshtain-Pops, Hila Elinav, Michal Chowers, and et al. 2022. "Epidemiology and Transmitted HIV-1 Drug Resistance among Treatment-Naïve Individuals in Israel, 2010–2018" Viruses 14, no. 1: 71. https://doi.org/10.3390/v14010071