
High Incidence of Zika or Chikungunya Infection among Pregnant Women Hospitalized Due to Obstetrical Complications in Northeastern Brazil—Implications for Laboratory Screening in Arbovirus Endemic Area

 , ,
, ,  , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Data Collection
2.3. Laboratory Procedures
2.4. Case Definition of Arbovirus Infection
2.5. Data Analysis
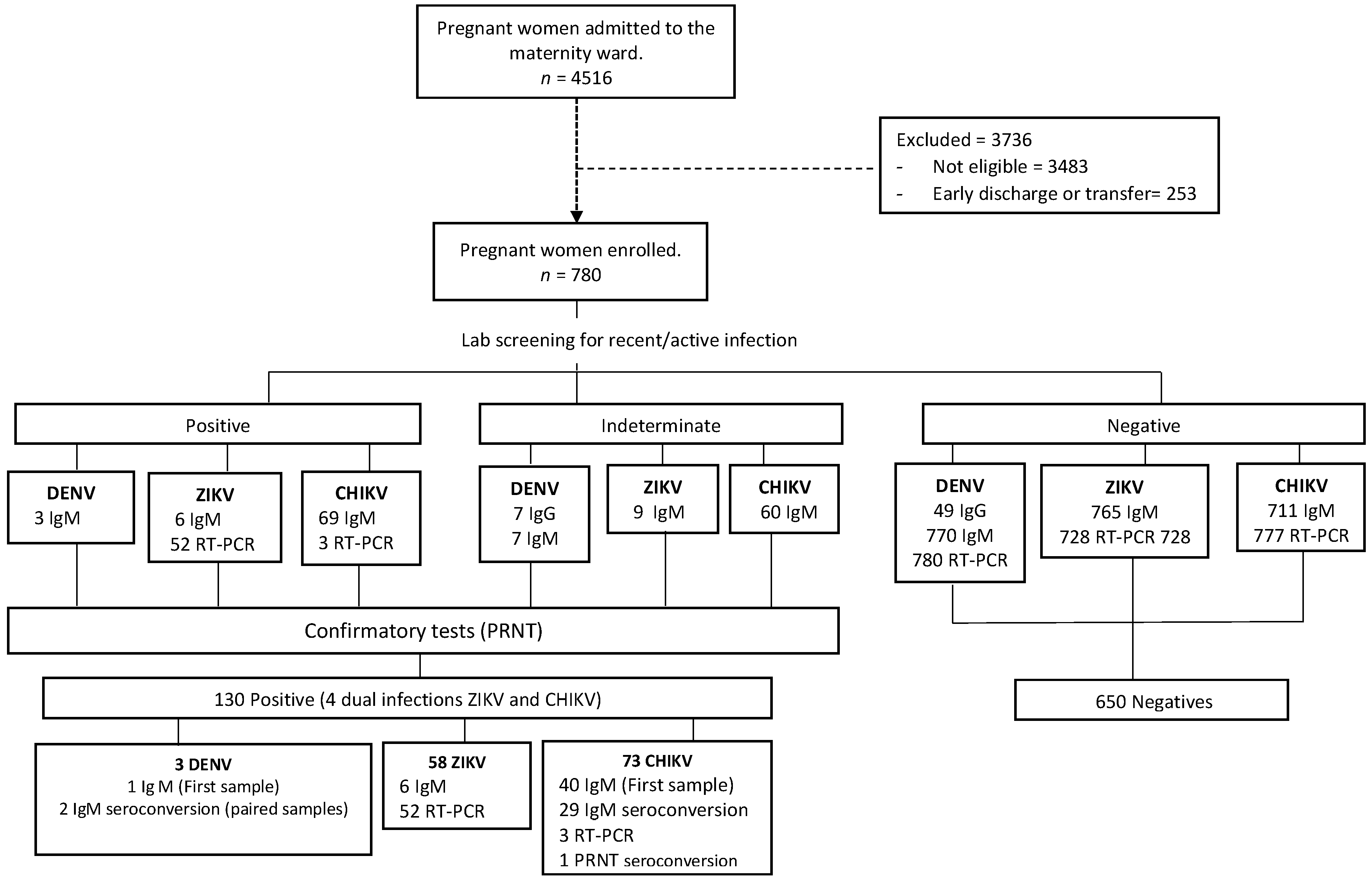
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Vector-Borne Diseases. WHO Factsheet 387. 2020. Available online: https://extranet.who.int/kobe_centre/sites/default/files/pdf/vbdfactsheet.pdf (accessed on 25 December 2020).
- Bhatt, S.; Gething, P.W.; Brady, O.J.; Messina, J.P.; Farlow, A.W.; Moyes, C.L.; Drake, J.M.; Brownstein, J.S.; Hoen, A.G.; Sankoh, O.; et al. The global distribution and burden of dengue. Nature 2013, 496, 504–507. [Google Scholar] [CrossRef]
- Paixao, E.S.; Teixeira, M.G.; Rodrigues, L.C. Zika, chikungunya and dengue: The causes and threats of new and re-emerging arboviral diseases. BMJ Glob. Health 2018, 3 (Suppl. 1), e000530. [Google Scholar] [CrossRef] [Green Version]
- Mayer, S.V.; Tesh, R.B.; Vasilakis, N. The emergence of arthropod-borne viral diseases: A global prospective on dengue, chikungunya and zika fevers. Acta Trop. 2017, 166, 155–163. [Google Scholar] [CrossRef]
- Pan American Health Organization. Chikungunya: Communicable Diseases and Health Analysis World Health Organization. 2020. Available online: http://www.paho.org/hq/index.php?option=com_topics&view=readall&cid=5927&Itemid=40931&lang=en (accessed on 18 January 2021).
- Charlier, C.; Beaudoin, M.-C.; Couderc, T.; Lortholary, O.; Lecuit, M. Arboviruses and pregnancy: Maternal, fetal, and neonatal effects. Lancet Child Adolesc. Health 2017, 1, 134–146. [Google Scholar] [CrossRef]
- Pouliot, S.H.; Xiong, X.; Harville, E.; Paz-Soldan, V.; Tomashek, K.M.; Breart, G.; Buekens, P. Maternal dengue and pregnancy outcomes: A systematic review. Obstet. Gynecol. Surv. 2010, 65, 107–118. [Google Scholar] [CrossRef]
- Nithiyanantham, S.F.; Badawi, A. Maternal infection with Zika virus and prevalence of congenital disorders in infants: Systematic review and meta-analysis. Can. J. Public Health 2019, 110, 638–648. [Google Scholar] [CrossRef] [PubMed]
- Contopoulos-Ioannidis, D.; Newman-Lindsay, S.; Chow, C.; Labeaud, A.D. Mother-to-child transmission of Chikungunya virus: A systematic review and meta-analysis. PLoS Negl. Trop. Dis. 2018, 12, e0006510. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chibueze, E.C.; Tirado, V.; Lopes, K.D.S.; Balogun, O.O.; Takemoto, Y.; Swa, T.; Dagvadorj, A.; Nagata, C.; Morisaki, N.; Menendez, C.; et al. Zika virus infection in pregnancy: A systematic review of disease course and complications. Reprod. Health 2017, 14, 28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flamand, C.; Fritzell, C.; Matheus, S.; Dueymes, M.; Carles, G.; Favre, A.; Enfissi, A.; Adde, A.; Demar, M.; Kazanji, M.; et al. The proportion of asymptomatic infections and spectrum of disease among pregnant women infected by Zika virus: Systematic monitoring in French Guiana, 2016. Eurosurveillance 2017, 22, 44. [Google Scholar] [CrossRef]
- Goncalves, A.; Peeling, R.W.; Chu, M.C.; Gubler, D.J.; de Silva, A.M.; Harris, E.; Murtagh, M.; Chua, A.; Rodriguez, W.; Kelly, C.; et al. Innovative and New Approaches to Laboratory Diagnosis of Zika and Dengue: A Meeting Report. J. Infect. Dis. 2018, 217, 1060–1068. [Google Scholar] [CrossRef] [PubMed]
- Natrajan, M.S.; Rojas, A.; Waggoner, J.J. Beyond Fever and Pain: Diagnostic Methods for Chikungunya Virus. J. Clin. Microbiol. 2019, 57, e00350-19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castanha, P.M.S.; Souza, W.V.; Braga, C.; Araújo, T.V.B.D.; Ximenes, R.A.A.; Maria de Fátima, P.M.; Montarroyos, U.R.; Miranda-Filho, D.B.; Cordeiro, M.T.; Dhalia, R.; et al. Perinatal analyses of Zika- and dengue virus-specific neutralizing antibodies: A microcephaly case-control study in an area of high dengue endemicity in Brazil. PLoS Negl. Trop. Dis. 2019, 13, e0007246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eppes, C.; Rac, M.; Dunn, J.; Versalovic, J.; Murray, K.O.; Suter, M.A.; Cortes, M.S.; Espinoza, J.; Seferovic, M.D.; Lee, W.; et al. Testing for Zika virus infection in pregnancy: Key concepts to deal with an emerging epidemic. Am. J. Obstet. Gynecol. 2017, 216, 209–225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ximenes, R.A.A.; Miranda-Filho, D.B.; Brickley, E.B.; Montarroyos, U.R.; Martelli, C.M.T.; Araujo, T.V.B.; Rodrigues, L.C.; de Souza, W.V.; da Silva Castanha, P.M.; França, R.F.; et al. Zika virus infection in pregnancy: Establishing a case definition for clinical research on pregnant women with rash in an active transmission setting. PLoS Negl. Trop. Dis. 2019, 13, e0007763. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fares, R.C.; Souza, K.P.; Anez, G.; Rios, M. Epidemiological Scenario of Dengue in Brazil. Biomed. Res. Int. 2015, 2015, 321873. [Google Scholar] [CrossRef] [Green Version]
- Do Carmo, R.F.; Silva Júnior, J.V.J.; Pastor, A.F.; De Souza, C.D.F. Spatiotemporal dynamics, risk areas and social determinants of dengue in Northeastern Brazil, 2014–2017: An ecological study. Infect. Dis. Poverty 2020, 9, 153. [Google Scholar] [CrossRef] [PubMed]
- França, G.V.A.D.; Pedi, V.D.; Garcia, M.H.D.O.; Carmo, G.M.I.D.; Leal, M.B.; Garcia, L.P. Congenital syndrome associated with Zika virus infection among live births in Brazil: A description of the distribution of reported and confirmed cases in 2015–2016. Epidemiol. Serv. Saude 2018, 27, e2017473. [Google Scholar]
- Brito, C.A.A. Alert: Severe cases and deaths associated with Chikungunya in Brazil. Rev. Soc. Bras. Med. Trop. 2017, 50, 585–589. [Google Scholar] [CrossRef] [Green Version]
- Magalhaes, T.; Braga, C.; Cordeiro, M.T.; Oliveira, A.L.S.; Castanha, P.M.S.; Maciel, A.P.R.; Amancio, N.M.; Gouveia, P.N.; Peixoto-da-Silva, V.J., Jr.; Peixoto, T.F.; et al. Zika virus displacement by a chikungunya outbreak in Recife, Brazil. PLoS Negl. Trop. Dis. 2017, 11, e0006055. [Google Scholar] [CrossRef]
- De Araújo, T.V.B.; Rodrigues, L.C.; De Alencar Ximenes, R.A.; De Barros Miranda-Filho, D.; Montarroyos, U.R.; De Melo, A.P.L.; Valongueiro, S.; Souza, W.V.; Braga, C.; Brandão Filho, S.P.; et al. Association between Zika virus infection and microcephaly in Brazil, January to May, 2016: Preliminary report of a case-control study. Lancet Infect. Dis. 2016, 16, 1356–1363. [Google Scholar] [CrossRef] [Green Version]
- Duarte, A.O.; Oliveira, J.V.; Carvalho, T.C.X.; Pessoa, L.B.; Filho, C.M.; Lima, J.G.S.; Carvalho, D.A.; Dos Santos, D.C.; Santos, C.S.; Pessoa, R.; et al. Maternal and congenital infections arising from Zika, dengue and Chikungunya arboviruses in Salvador, Brazil. Trans. R. Soc. Trop. Med. Hyg. 2020, 114, 222–225. [Google Scholar] [CrossRef]
- Costa, L.C.; Veiga, R.V.; Oliveira, J.F.; Rodrigues, M.S.; Andrade, R.F.S.; Paixao, E.S.; Teixeira, M.G.; Costa, M.D.; Cardim, L.L.; Carmo, E.H.; et al. New Insights on the Zika Virus Arrival in the Americas and Spatiotemporal Reconstruction of the Epidemic Dynamics in Brazil. Viruses 2020, 13, 12. [Google Scholar] [CrossRef]
- Albuquerque, M.D.F.P.M.D.; Souza, W.V.D.; Araújo, T.V.B.; Braga, M.C.; Miranda Filho, D.D.B.; Ximenes, R.A.D.A.; de Melo Filho, D.A.; Brito, C.A.; Valongueiro, S.; Melo, A.P.; et al. The microcephaly epidemic and Zika virus: Building knowledge in epidemiology. Cad. Saude Publica 2018, 34, e00069018. [Google Scholar]
- Brazilian Ministry of Health. National Surveillance System for Notifiable Diseases (SINAN); Sinan-Net. 2019. Available online: http://portalsinan.saude.gov.br/sinan-net (accessed on 25 January 2020).
- Committee on Practice B-O. Practice Bulletin No. 183: Postpartum Hemorrhage. Obstet. Gynecol. 2017, 130, e168–e186. [Google Scholar] [CrossRef]
- Committee on Practice B-O. ACOG Practice Bulletin No. 188: Prelabor Rupture of Membranes. Obstet. Gynecol. 2018, 131, e1–e14. [Google Scholar]
- American College of Obstetricians and Gynecologists. ACOG Practice Bulletin No. 202: Gestational Hypertension and Preeclampsia. Obstet. Gynecol. 2019, 133, 1. [Google Scholar]
- Elsasser, D.A.; Ananth, C.V.; Prasad, V.; Vintzileos, A.M. Diagnosis of placental abruption: Relationship between clinical and histopathological findings. Eur. J. Obstet. Gynecol. Reprod. Biol. 2010, 148, 125–130. [Google Scholar] [CrossRef] [PubMed]
- International Association of Diabetes and Pregnancy Study Groups Consensus Panel; Metzger, B.E.; Gabbe, S.G.; Persson, B.; Buchanan, T.A.; Catalano, P.A.; Damm, P.; Dyer, A.R.; De Leiva, A.; Hod, M.; et al. International association of diabetes and pregnancy study groups recommendations on the diagnosis and classification of hyperglycemia in pregnancy. Diabetes Care 2010, 33, 676–682. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dubil, E.A.; Magann, E.F. Amniotic fluid as a vital sign for fetal wellbeing. Australas J. Ultrasound Med. 2013, 16, 62–70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fahey, J.O. Clinical management of intra-amniotic infection and chorioamnionitis: A review of the literature. J. Midwifery Womens Health 2008, 53, 227–235. [Google Scholar] [CrossRef] [PubMed]
- Sibai, B.M. Diagnosis, controversies, and management of the syndrome of hemolysis, elevated liver enzymes, and low platelet count. Obstet. Gynecol. 2004, 103, 981–991. [Google Scholar] [CrossRef] [Green Version]
- Basurko, C.; Everhard, S.; Matheus, S.; Restrepo, M.; Hilderal, H.; Lambert, V.; Boukhari, R.; Duvernois, J.P.; Favre, A.; Valmy, L.; et al. A prospective matched study on symptomatic dengue in pregnancy. PLoS ONE 2018, 13, e0202005. [Google Scholar] [CrossRef] [PubMed]
- Engle, W.A. A recommendation for the definition of “late preterm” (near-term) and the birth weight-gestational age classification system. Semin. Perinatol. 2006, 30, 2–7. [Google Scholar] [CrossRef] [PubMed]
- Waggoner, J.J.; Gresh, L.; Mohamed-Hadley, A.; Ballesteros, G.; Davila, M.J.V.; Tellez, Y.; Sahoo, M.K.; Balmaseda, A.; Harris, E.; Pinsky, B.A. Single-Reaction Multiplex Reverse Transcription PCR for Detection of Zika, Chikungunya, and Dengue Viruses. Emerg. Infect. Dis. 2016, 22, 1295–1297. [Google Scholar] [CrossRef] [Green Version]
- Cordeiro, M.T.; Brito, C.A.; Pena, L.J.; Castanha, P.M.; Gil, L.H.; Lopes, K.G.; Dhalia, R.; Meneses, J.A.; Ishigami, A.C.; Mello, L.M.; et al. Results of a Zika Virus (ZIKV) Immunoglobulin M-Specific Diagnostic Assay Are Highly Correlated with Detection of Neutralizing Anti-ZIKV Antibodies in Neonates with Congenital Disease. J. Infect. Dis. 2016, 214, 1897–1904. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Zika Virus Disease: Interim Case Definitions; World Health Organization: Geneva, Switzerland, 2016; Available online: https://apps.who.int/iris/handle/10665/204381 (accessed on 25 December 2020).
- World Health Organization. Guidelines on Clinical Management of Chikungunya Fever; World Health Organization: Geneva, Switzerland, 2008; Available online: https://apps.who.int/iris/bitstream/handle/10665/205178/B3234.pdf?sequence=1&isAllowed=y (accessed on 25 December 2020).
- World Health Organization. Dengue and Severe Dengue; World Health Organization: Geneva, Switzerland, 2020; Available online: https://www.who.int/news-room/fact-sheets/detail/dengue-and-severe-dengue2020 (accessed on 25 December 2020).
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanchez Clemente, N.; Brickley, E.B.; Paixão, E.S.; De Almeida, M.F.; Gazeta, R.E.; Vedovello, D.; Rodrigues, L.C.; Witkin, S.S.; Passos, S.D. Zika virus infection in pregnancy and adverse fetal outcomes in São Paulo State, Brazil: A prospective cohort study. Sci. Rep. 2020, 10, 12673. [Google Scholar] [CrossRef] [PubMed]
- Bautista, L.E.; Herrera, V.M. An assessment of public health surveillance of Zika virus infection and potentially associated outcomes in Latin America. BMC Public Health 2018, 18, 656. [Google Scholar] [CrossRef]
- Piltch-Loeb, R.; Kraemer, J.; Lin, K.W.; Stoto, M.A. Public Health Surveillance for Zika Virus: Data Interpretation and Report Validity. Am. J. Public Health 2018, 108, 1358–1362. [Google Scholar] [CrossRef]
- Lozier, M.J.; Rosenberg, E.S.; Doyle, K.; Adams, L.; Klein, L.; Munoz-Jordan, J.; Alvarado, L.I.; Sharp, T.M.; Paz-Bailey, G. Prolonged Detection of Zika Virus Nucleic Acid Among Symptomatic Pregnant Women: A Cohort Study. Clin. Infect. Dis. 2018, 67, 624–627. [Google Scholar] [CrossRef]
- Mansuy, J.M.; Mengelle, C.; Pasquier, C.; Chapuy-Regaud, S.; Delobel, P.; Martin-Blondel, G.; Izopet, J. Zika Virus Infection and Prolonged Viremia in Whole-Blood Specimens. Emerg. Infect. Dis. 2017, 23, 863–865. [Google Scholar] [CrossRef]
- Gabriela, P.B.; Rosenberg Eli, S.; Kate, D.; Jorge, M.J.; Santiago Gilberto, A.; Liore, K.; Janice, P.P.; Medina Freddy, A.; Waterman Stephen, H.; Adams Laura, E.; et al. Persistence of Zika Virus in Body Fluids—Final Report. N. Engl. J. Med. 2018, 379, 1234–1243. [Google Scholar]
- Driggers, R.W.; Ho, C.Y.; Korhonen, E.M.; Kuivanen, S.; Jaaskelainen, A.J.; Smura, T.; Rosenberg, A.; Hill, D.A.; DeBiasi, R.L.; Vezina, G.; et al. Zika Virus Infection with Prolonged Maternal Viremia and Fetal Brain Abnormalities. N. Engl. J. Med. 2016, 374, 2142–2151. [Google Scholar] [CrossRef]
- Meaney-Delman, D.; Oduyebo, T.; Polen, K.N.D.; White, J.L.; Bingham, A.M.; Slavinski, S.A.; Heberlein-Larson, L.; St George, K.; Rakeman, J.L.; Hills, S.; et al. Prolonged Detection of Zika Virus RNA in Pregnant Women. Obstet. Gynecol. 2016, 128, 724–730. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fontaine, A.; De Laval, F.; Belleoud, D.; Briolant, S.; Matheus, S. Duration of Zika Viremia in Serum. Clin. Infect. Dis. 2018, 67, 1143–1144. [Google Scholar] [CrossRef]
- Bhatnagar, J.; Rabeneck, D.B.; Martines, R.B.; Reagan-Steiner, S.; Ermias, Y.; Estetter, L.B.; Suzuki, T.; Ritter, J.; Keating, M.K.; Hale, G.; et al. Zika Virus RNA Replication and Persistence in Brain and Placental Tissue. Emerg. Infect. Dis. 2017, 23, 405–414. [Google Scholar] [CrossRef] [PubMed]
- Mor, G.; Aldo, P.; Alvero, A.B. The unique immunological and microbial aspects of pregnancy. Nat. Rev. Immunol. 2017, 17, 469–482. [Google Scholar] [CrossRef] [PubMed]
- Kourtis, A.P.; Read, J.S.; Jamieson, D.J. Pregnancy and infection. N. Engl. J. Med. 2014, 371, 1077. [Google Scholar] [CrossRef] [Green Version]
- Bozza, F.; Moreira-Soto, A.; Rockstroh, A.; Fischer, C.; Nascimento, A.; Calheiros, A.; Drosten, C.; Bozza, P.T.; Souza, T.M.; Ulbert, S.; et al. Differential Shedding and Antibody Kinetics of Zika and Chikungunya Viruses, Brazil. Emerg. Infect. Dis. 2019, 25, 311. [Google Scholar] [CrossRef]
- Chua, C.-L.; Sam, I.C.; Chiam, C.-W.; Chan, Y.-F. The neutralizing role of IgM during early Chikungunya virus infection. PLoS ONE 2017, 12, e0171989. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanchez Clemente, N.; Brickley, E.; Furquim De Almeida, M.; Witkin, S.; Duarte Passos, S. Can Zika Virus Infection in High Risk Pregnant Women Be Differentiated on the Basis of Symptoms? Viruses 2020, 12, 1263. [Google Scholar] [CrossRef] [PubMed]
- Brasil, P.; Pereira, J.P., Jr.; Moreira, M.E.; Nogueira, R.M.R.; Damasceno, L.; Wakimoto, M. Zika Virus Infection in Pregnant Women in Rio de Janeiro. N. Engl. J. Med. 2016, 375, 2321–2334. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristic | (n = 780) a |
|---|---|
| Sociodemographic | |
| Age (in years), mean (±SD) | 26.5 (3.6) |
| Self-reported Race/skin color, n (%) | |
| Mixed | 480 (61.7) |
| White | 157 (20.2) |
| Black | 141 (18.1) |
| Family income (in minimum wages) | |
| ≤2 | 640 (82.8) |
| >2 | 133 (17.2) |
| Schooling, n (%) | |
| Illiterate/Elementary | 186 (23.8) |
| High school/Higher Education | 594 (76.2) |
| Clinical | |
| Gestational age (in weeks) at admission, mean (±SD) | 36.9 (±3.2) |
| Obstetric complication in previous pregnancy, n (%) b | 221 (45.9) |
| Prenatal consultation in the current pregnancy, n (%) | 758 (97.2) |
| Pregnancy, n (%) | |
| Single | 751(96.3) |
| Multiple | 29 (3.7) |
| Type of obstetric complication, n (%) | |
| Hypertensive disorder of pregnancy c | 469 (60.1) |
| Gestational diabetes | 98 (12.6) |
| Preterm labor/premature birth | 110 (14.1) |
| HELLP syndrome (complete/incomplete) | 35 (4.5) |
| Others d | 68 (8.7) |
| Arbovirus infection status, n (%) | |
| Previous DENV infection (IgG positives) | 726 (93.1) |
| Active/recent DENV infection e | 3 (0.4) |
| Active/recent ZIKV infection e | 54 (6.9) |
| Active/recent CHIKV e | 69 (8.8) |
| Dual active/recent infection (CHIKV and ZIKV) | 4 (0.5) |
| Laboratorial Evidence | Arbovirus Infection | Total (n = 130) c | ||
|---|---|---|---|---|
| Mono-Infection | Dual-Infection | |||
| ZIKV (n = 54) | CHIKV (n = 69) | ZIKV + CHIKV (n = 4) | ||
| Case definition, n (%) | ||||
| Active infection a | 49 (90.7) | 30 (43.5) | 3 (75.0) | 84 (64.6) |
| Recent infection b | 5 (9.2) | 39 (56.5) | 1 (25.0) | 46 (35.4) |
| Laboratorial assays, n (%) | ||||
| qRT-PCR positive (first sample) | 48 (88.8) | 2 (2.9) | - | - |
| Specific IgM positive (first sample) | 5 (9.2) | 39 (56.5) | - | - |
| qRT-PCR positive (first sample) and IgM seroconversion (paired samples) | 1 (1.8) | 0 (00) | - | - |
| IgM and/or IgG seroconversion (paired samples) | 0 (0.0) | 28 (40.6) | - | - |
| ZIKV and CHIKV qRT-PCR positives (First sample) | - | - | 1 (25.0) | - |
| ZIKV qRT-PCR positive and CHIKV IgM seroconversion | - | - | 2 (50.0) | - |
| ZIKV and CHIKV IgM positive (first sample) | - | - | 1 (25.0) | - |
| Clinical Characteristics | ZIKV (n = 54) | CHIKV (n = 69) | Uninfected (n = 650) | p Value a |
|---|---|---|---|---|
| n (%) | n (%) | n (%) | ||
| Self-Reported Signs and Symptoms | ||||
| Suspected cases (WHO case definition) b | 2 (3.7) | 3 (4.3) | 32 (4.9) | 0.914 |
| Acute febrile episodes | 7 (12.9) | 8 (11.6) | 111 (17.1) | 0.503 |
| Rash | 3 (5.5) | 6 (8.7) | 31 (4.8) | 0.420 |
| Arthralgia | 4 (7.4) | 13 (18.8) | 97 (14.9) | 0.285 |
| Fever and/or rash | 10 (18.5) | 11 (15.9) | 129 (19.8) | 0.802 |
| Zika, Dengue, or Chikungunya in current pregnancy | 0 (0.0) | 2 (3.1) | 2 (0.3) | - |
| Obstetrical complicationsc | ||||
| Hypertensive disorder of pregnancy | 30 (57.7) | 42 (60.9) | 390 (60.0) | 0.983 |
| Gestational diabetes | 8 (15.4) | 7 (10.1) | 82 (12.6) | 0.749 |
| Preterm labor/premature birth | 7 (13.4) | 11 (15.9) | 91 (14.0) | 0.792 |
| HELLP syndrome (complete/incomplete) | 3 (5.8) | 4 (5.8) | 28 (4.3) | 0.792 |
| Others | 4 (7.7) | 5 (7.2) | 59 (9.1) | 0.862 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jacques, I.J.A.A.; Katz, L.; Sena, M.A.; Guimarães, A.B.G.; Silva, Y.L.; Albuquerque, G.D.M.; Pereira, R.O.; de Albuquerque, C.A.M.C.; Silva, M.A.L.; Oliveira, P.A.S.; et al. High Incidence of Zika or Chikungunya Infection among Pregnant Women Hospitalized Due to Obstetrical Complications in Northeastern Brazil—Implications for Laboratory Screening in Arbovirus Endemic Area. Viruses 2021, 13, 744. https://doi.org/10.3390/v13050744
Jacques IJAA, Katz L, Sena MA, Guimarães ABG, Silva YL, Albuquerque GDM, Pereira RO, de Albuquerque CAMC, Silva MAL, Oliveira PAS, et al. High Incidence of Zika or Chikungunya Infection among Pregnant Women Hospitalized Due to Obstetrical Complications in Northeastern Brazil—Implications for Laboratory Screening in Arbovirus Endemic Area. Viruses. 2021; 13(5):744. https://doi.org/10.3390/v13050744
Chicago/Turabian StyleJacques, Iracema J. A. A., Leila Katz, Marília A. Sena, Ana B. G. Guimarães, Yasmim L. Silva, Gabriela D. M. Albuquerque, Raisa O. Pereira, Camila A. M. C. de Albuquerque, Maria Almerice L. Silva, Paula A. S. Oliveira, and et al. 2021. "High Incidence of Zika or Chikungunya Infection among Pregnant Women Hospitalized Due to Obstetrical Complications in Northeastern Brazil—Implications for Laboratory Screening in Arbovirus Endemic Area" Viruses 13, no. 5: 744. https://doi.org/10.3390/v13050744