
Global and Regional Prevalence and Outcomes of COVID-19 in People Living with HIV: A Systematic Review and Meta-Analysis

 , and
, and
Abstract
:1. Introduction
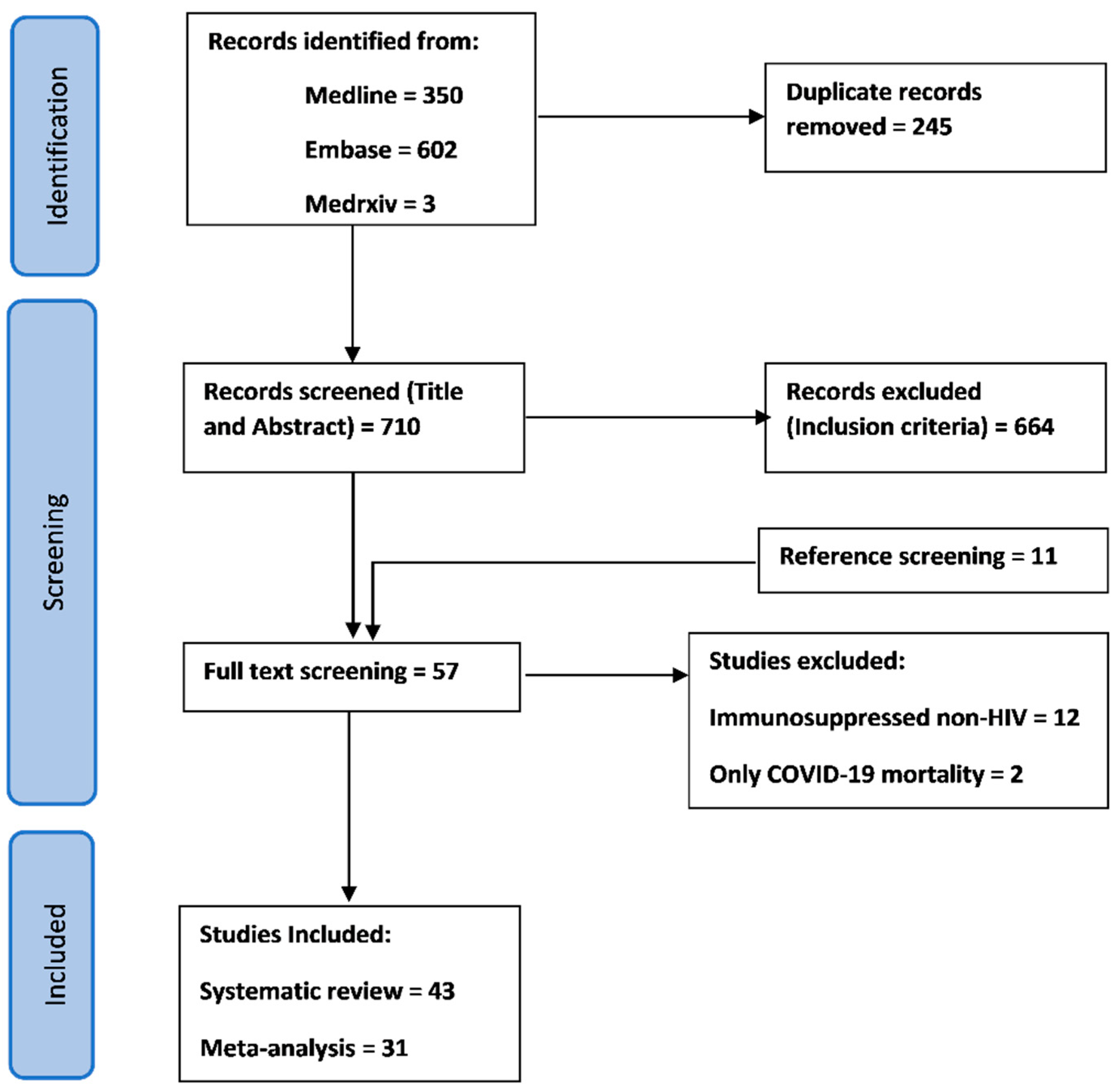
2. Methods
2.1. Inclusion and Exclusion Criteria
2.2. Data Collection
2.3. Data Extraction and Analysis
2.4. Quality Assessment
3. Results
3.1. General Description of the Studies Included
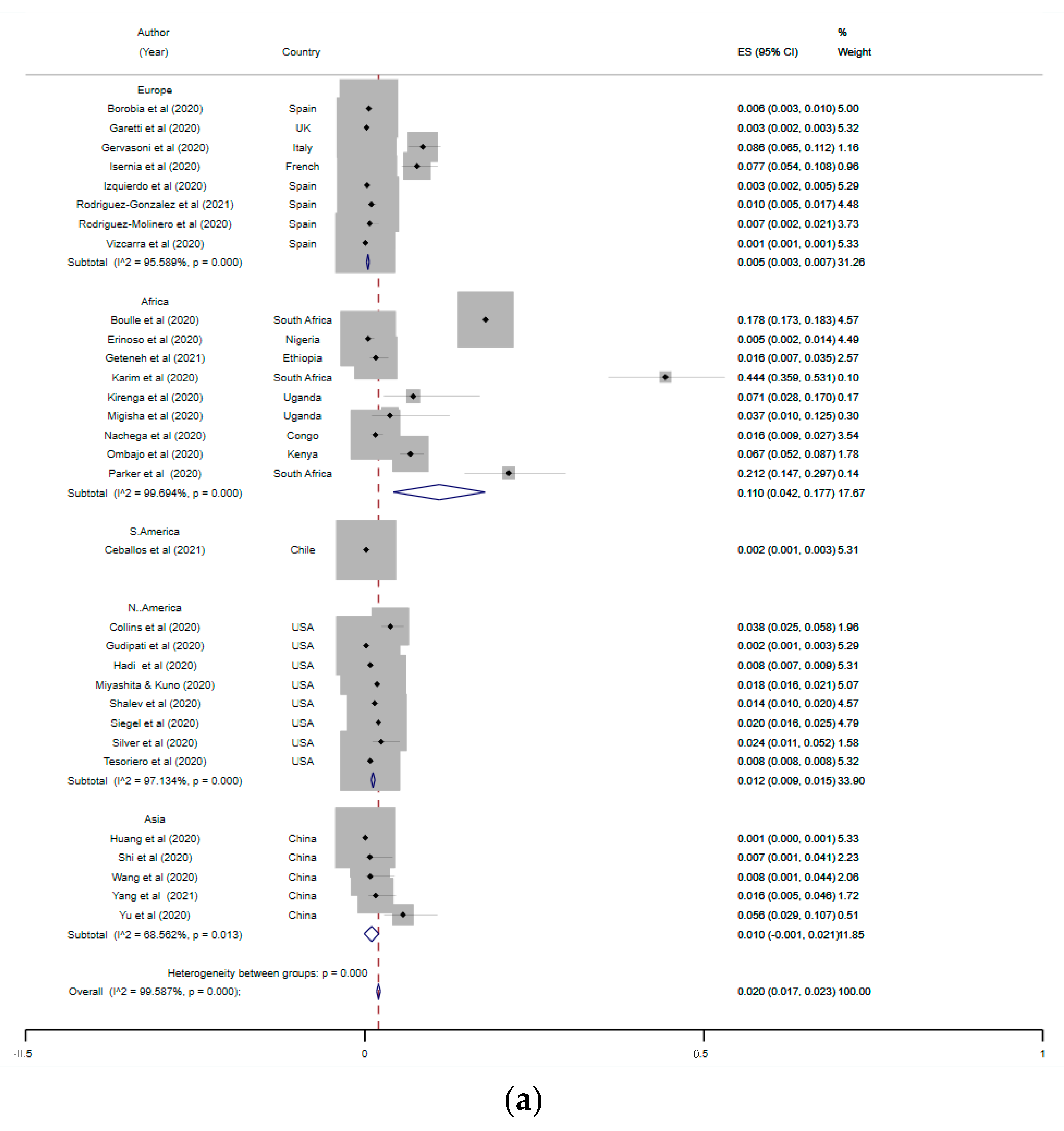
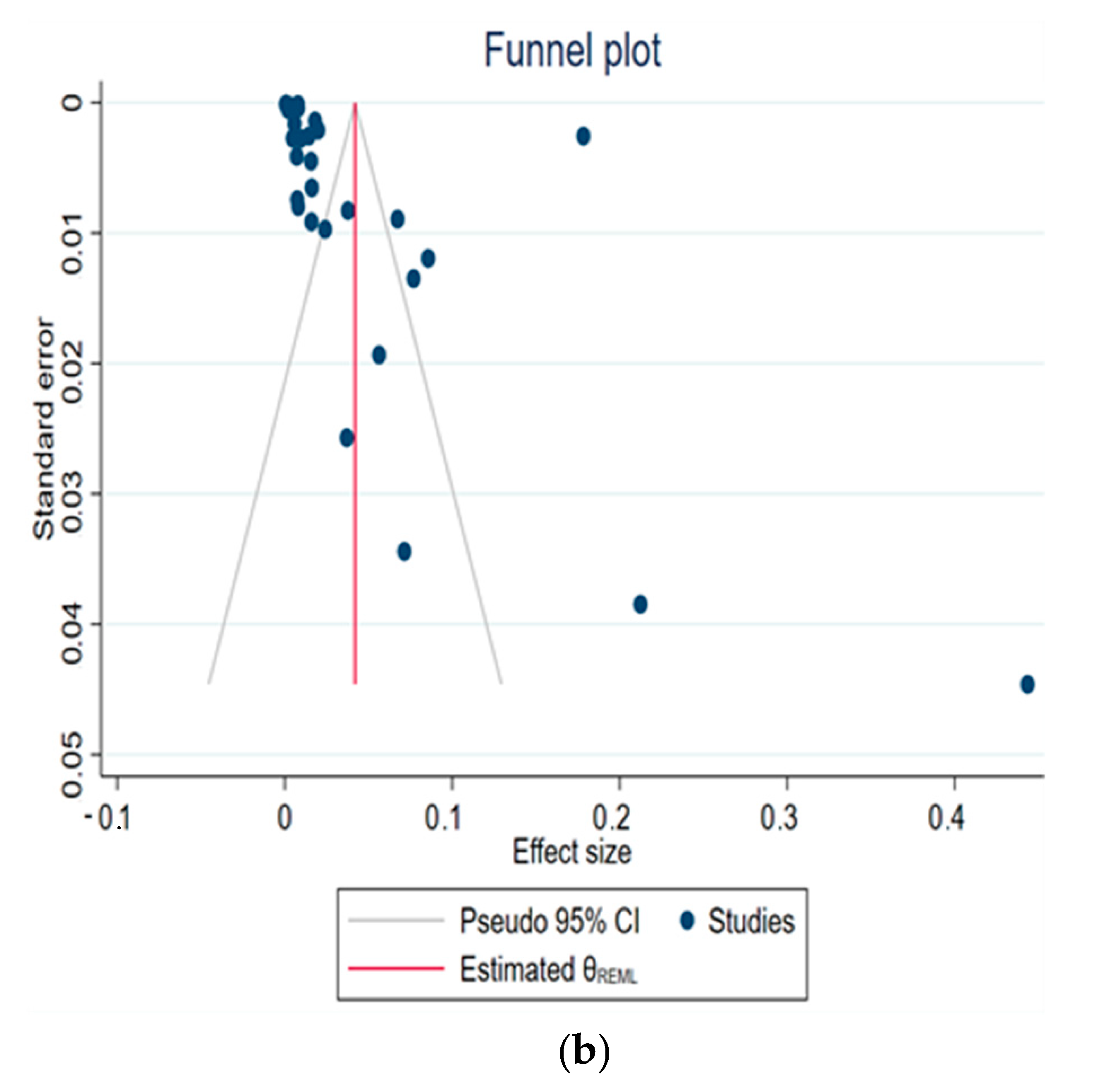
3.2. Prevalence of PLWH among COVID-19 Cases
3.3. Severity of COVID-19 in PLWH
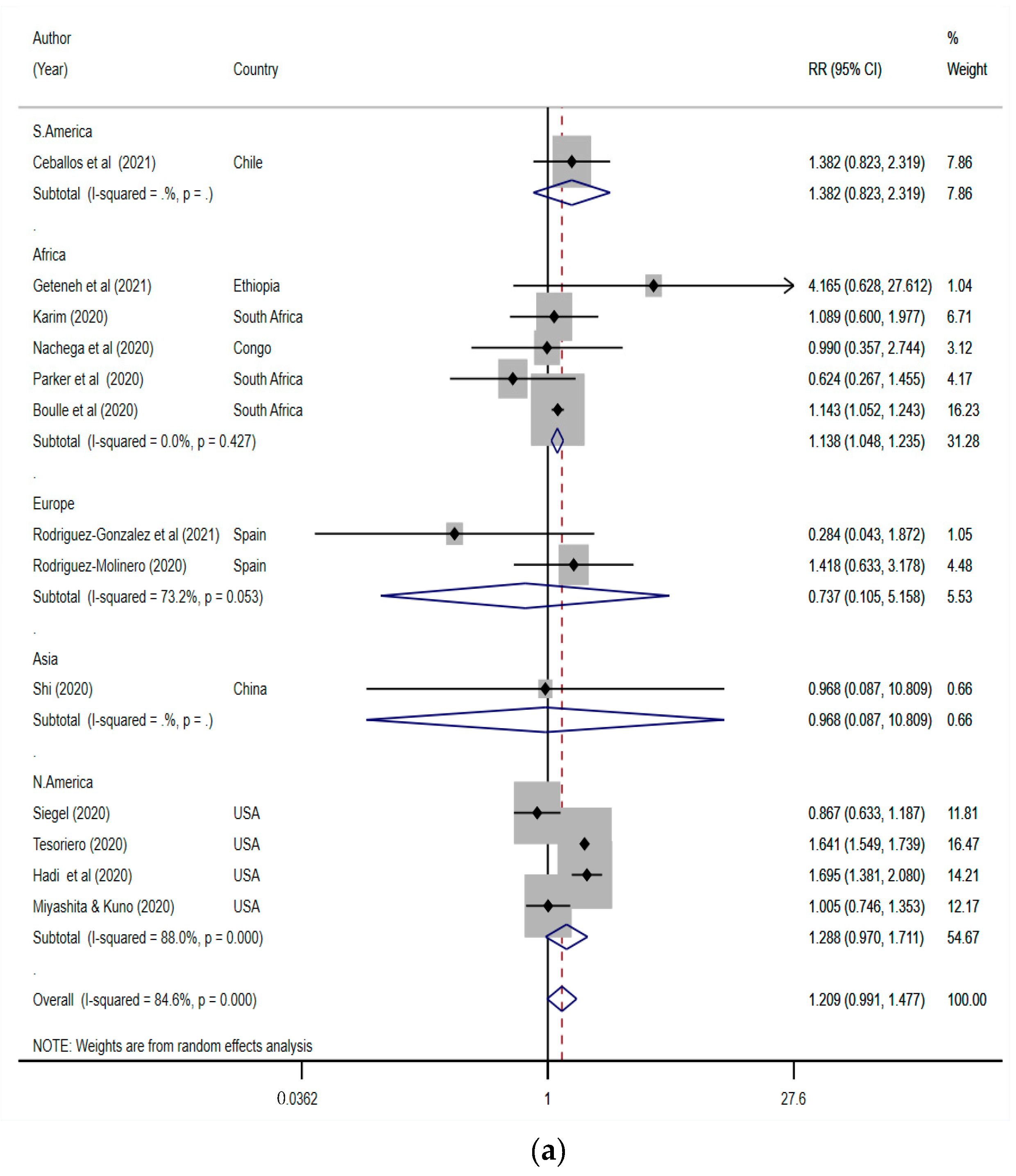
3.4. Mortality of PLWH Coinfected with SARS-CoV-2
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Worldometer: Coronavirus Update (Live). Available online: https://www.worldometers.info/coronavirus/ (accessed on 25 February 2020).
- Alqahtani, J.S.; Aldhahir, A.M.; Oyelade, T.; Alghamdi, S.M.; Almamary, A.S. Smoking cessation during COVID-19: The top to-do list. npj Prim. Care Respir. Med. 2021, 31, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Oyelade, T.; Alqahtani, J.; Canciani, G. Prognosis of COVID-19 in Patients with Liver and Kidney Diseases: An Early Systematic Review and Meta-Analysis. Trop. Med. Infect. Dis. 2020, 5, 80. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Zheng, Y.; Gou, X.; Pu, K.; Chen, Z.; Guo, Q.; Ji, R.; Wang, H.; Wang, Y.; Zhou, Y. Prevalence of comorbidities in the novel wuhan coronavirus (COVID-19) infection: A systematic review and meta-analysis. Int. J. Infect. Dis. 2020, 94, 91–95. [Google Scholar] [CrossRef] [PubMed]
- Alqahtani, J.S.; Mendes, R.G.; Aldhahir, A.; Rowley, D.; AlAhmari, M.D.; Ntoumenopoulos, G.; Alghamdi, S.M.; Sreedharan, J.K.; Aldabayan, Y.S.; Oyelade, T.; et al. Global Current Practices of Ventilatory Support Management in COVID-19 Patients: An International Survey. J. Multidiscip. Heal. 2020, 13, 1635–1648. [Google Scholar] [CrossRef]
- Guan, W.-J.; Liang, W.-H.; Zhao, Y.; Liang, H.-R.; Chen, Z.-S.; Li, Y.-M.; Liu, X.-Q.; Chen, R.-C.; Tang, C.-L.; Wang, T.; et al. Comorbidity and its impact on 1590 patients with COVID-19 in China: A nationwide analysis. Eur. Respir. J. 2020, 55, 2000547. [Google Scholar] [CrossRef] [Green Version]
- Subgroup ‘Assessment of Pathogens Transmissible by Blood’ German Advisory Committee Blood (Arbeitskreis Blut) Human Immunodeficiency Virus (HIV). Transfus. Med. Hemotherapy 2016, 43, 203–222. [CrossRef] [Green Version]
- Joint United Nations Programme on HIV and AIDS (UNAIDS). FACT SHEET 2021 Preliminary UNAIDS 2021 Epidemiological Estimates, in GLOBAL HIV STATISTICS. 2021. Available online: https://www.unaids.org/en/resources/fact-sheet (accessed on 1 December 2021).
- Kharsany, A.B.; Karim, Q.A. HIV Infection and AIDS in Sub-Saharan Africa: Current Status, Challenges and Opportunities. Open AIDS J. 2016, 10, 34–48. [Google Scholar] [CrossRef] [Green Version]
- El-Atrouni, W.; Berbari, E.; Temesgen, Z. Hiv-associated opportunistic infections. Bacterial infections. J. Med. Liban 2006, 54, 80–83. [Google Scholar]
- Lewden, C.; Salmon, D.; Morlat, P.; Bévilacqua, S.; Jougla, E.; Bonnet, F.; Héripret, L.; Costagliola, D.; May, T.; Chêne, G. Causes of death among human immunodeficiency virus (HIV)-infected adults in the era of potent antiretroviral therapy: Emerging role of hepatitis and cancers, persistent role of AIDS. Int. J. Epidemiology 2004, 34, 121–130. [Google Scholar] [CrossRef]
- Yazdanpanah, F.; Hamblin, M.R.; Rezaei, N. The immune system and COVID-19: Friend or foe? Life Sci. 2020, 256, 117900. [Google Scholar] [CrossRef]
- Chen, J.; Xia, L.; Liu, L.; Xu, Q.; Ling, Y.; Huang, D.; Huang, W.; Song, S.; Xu, S.; Shen, Y.; et al. Antiviral Activity and Safety of Darunavir/Cobicistat for the Treatment of COVID-19. Open Forum Infect. Dis. 2020, 7, ofaa241. [Google Scholar] [CrossRef] [PubMed]
- De Meyer, S.; Bojkova, D.; Cinatl, J.; Van Damme, E.; Buyck, C.; Van Loock, M.; Woodfall, B.; Ciesek, S. Lack of antiviral activity of darunavir against SARS-CoV-2. Int. J. Infect. Dis. 2020, 97, 7–10. [Google Scholar] [CrossRef] [PubMed]
- Horby, P.W.; Mafham, M.; Bell, J.L.; Linsell, L.; Staplin, N.; Emberson, J.; Palfreeman, A.; Raw, J.; Elmahi, E.; Prudon, B.; et al. Lopinavir–ritonavir in patients admitted to hospital with COVID-19 (recovery): A randomised, controlled, open-label, platform trial. Lancet 2020, 396, 1345–1352. [Google Scholar] [CrossRef]
- Ayerdi, O.; Puerta, T.; Clavo, P.; Vera, M.; Ballesteros, J.; Fuentes, M.E.; Estrada, V.; Rodríguez, C.; Del Romero, J.; Lejarraga, C.; et al. Preventive Efficacy of Tenofovir/Emtricitabine Against Severe Acute Respiratory Syndrome Coronavirus 2 Among Pre-Exposure Prophylaxis Users. Open Forum Infect. Dis. 2020, 7, ofaa455. [Google Scholar] [CrossRef]
- Hariyanto, T.I.; Rosalind, J.; Christian, K.; Kurniawan, A. Human immunodeficiency virus and mortality from coronavirus disease 2019: A systematic review and meta-analysis. South. Afr. J. HIV Med. 2021, 22, 7. [Google Scholar] [CrossRef]
- Mellor, M.M.; Bast, A.C.; Jones, N.R.; Roberts, N.W.; Ordóñez-Mena, J.M.; Reith, A.J.; Butler, C.C.; Matthews, P.C.; Dorward, J. Risk of adverse coronavirus disease 2019 outcomes for people living with HIV. AIDS 2021, 35, F1–F10. [Google Scholar] [CrossRef]
- Ssentongo, P.; Heilbrunn, E.S.; Ssentongo, A.E.; Advani, S.; Chinchilli, V.M.; Nunez, J.J.; Du, P. Epidemiology and outcomes of COVID-19 in HIV-infected individuals: A systematic review and meta-analysis. Sci. Rep. 2021, 11, 1–12. [Google Scholar] [CrossRef]
- Gao, Y.; Chen, Y.; Liu, M.; Shi, S.; Tian, J. Impacts of immunosuppression and immunodeficiency on COVID-19: A systematic review and meta-analysis. J. Infect. 2020, 81, e93–e95. [Google Scholar] [CrossRef]
- Lee, K.; Yap, S.; Ngeow, Y.; Lye, M. COVID-19 in People Living with HIV: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Heal. 2021, 18, 3554. [Google Scholar] [CrossRef]
- Joint United Nations Programme on HIV/AIDS; WHO. 2008 Report on the Global AIDS Epidemic; WHO: Geneva, Switzerland, 2008; Available online: https://scholar.google.co.uk/scholar?cluster=9760571076381553660&hl=en&as_sdt=0,5&as_vis=1 (accessed on 1 December 2021).
- Ambrosioni, J.; Blanco, J.L.; Reyes-Urueña, J.M.; Davies, M.-A.; Sued, O.; Marcos, M.A.; Martínez, E.; Bertagnolio, S.; Alcamí, J.; Miro, J.M.; et al. Overview of SARS-CoV-2 infection in adults living with HIV. Lancet HIV 2021, 8, e294–e305. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morgan, R.L.; Whaley, P.; Thayer, K.A.; Schünemann, H.J. Identifying the PECO: A framework for formulating good questions to explore the association of environmental and other exposures with health outcomes. Environ. Int. 2018, 121, 1027–1031. [Google Scholar] [CrossRef] [PubMed]
- Vizcarra, P.; Pérez-Elías, M.J.; Quereda, C.; Moreno, A.; Vivancos, M.J.; Dronda, F.; Casado, J.L.; Moreno, S.; Fortún, J.; Navas, E.; et al. Description of COVID-19 in HIV-infected individuals: A single-centre, prospective cohort. Lancet HIV 2020, 7, e554–e564. [Google Scholar] [CrossRef]
- Geretti, A.M.; Stockdale, A.J.; Kelly, S.H.; Cevik, M.; Collins, S.; Waters, L.; Villa, G.; Docherty, A.; Harrison, E.M.; Turtle, L.; et al. Outcomes of Coronavirus Disease 2019 (COVID-19) Related Hospitalization Among People With Human Immunodeficiency Virus (HIV) in the ISARIC World Health Organization (WHO) Clinical Characterization Protocol (UK): A Prospective Observational Study. Clin. Infect. Dis. 2020, 73, e2095–e2106. [Google Scholar] [CrossRef] [PubMed]
- Docherty, A.B.; Harrison, E.M.; Green, C.A.; Hardwick, H.E.; Pius, R.; Norman, L.; Holden, K.A.; Read, J.M.; Dondelinger, F.; Carson, G.; et al. Features of 20 133 UK patients in hospital with COVID-19 using the ISARIC WHO Clinical Characterisation Protocol: Prospective observational cohort study. BMJ 2020, 369, m1985. [Google Scholar] [CrossRef]
- WHO. COVID-19 Clinical Management: Living Guidance; WHO: Geneva, Switzerland, 2021. [Google Scholar]
- Johnson, J.K.; Barach, P.; Vernooij-Dassen, M.; HANDOVER Research Collaborative. Conducting a multicentre and multinational qualitative study on patient transitions. BMJ Qual. Saf. 2012, 21, i22–i28. [Google Scholar] [CrossRef] [Green Version]
- Liang, M.; Luo, N.; Chen, M.; Chen, C.; Singh, S.; Singh, S.; Tan, S. Prevalence and Mortality due to COVID-19 in HIV Co-Infected Population: A Systematic Review and Meta-Analysis. Infect. Dis. Ther. 2021, 10, 1267–1285. [Google Scholar] [CrossRef]
- WHO. Laboratory Testing for Coronavirus Disease (COVID-19) in Suspected Human Cases: Interim Guidance; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- WHO. Consolidated Guidelines on HIV Testing Services: 5Cs: Consent, Confidentiality, Counselling, Correct Results and Connection 2015; WHO: Geneva, Switzerland, 2015. [Google Scholar]
- Stoeckle, K.; Johnston, C.D.; Jannat-Khah, D.P.; Williams, S.C.; Ellman, T.M.; Vogler, M.A.; Gulick, R.M.; Glesby, M.J.; Choi, J.J. COVID-19 in Hospitalized Adults With HIV. Open Forum Infect. Dis. 2020, 7, ofaa327. [Google Scholar] [CrossRef]
- Borobia, A.; Carcas, A.; Arnalich, F.; Álvarez-Sala, R.; Monserrat-Villatoro, J.; Quintana, M.; Figueira, J.; Santos-Olmo, R.T.; García-Rodríguez, J.; Martín-Vega, A.; et al. A Cohort of Patients with COVID-19 in a Major Teaching Hospital in Europe. J. Clin. Med. 2020, 9, 1733. [Google Scholar] [CrossRef]
- Boulle, A.; Davies, M.-A.; Hussey, H.; Ismail, M.; Morden, E.; Vundle, Z.; Zweigenthal, V.; Mahomed, H.; Paleker, M.; Pienaar, D. Risk factors for COVID-19 death in a population cohort study from the Western Cape Province, South Africa. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2020. [Google Scholar] [CrossRef]
- Ceballos, M.E.; Ross, P.; Lasso, M.; Dominguez, I.; Puente, M.; Valenzuela, P.; Enberg, M.; Serri, M.; Muñoz, R.; Pinos, Y.; et al. Clinical characteristics and outcomes of people living with HIV hospitalized with COVID-19: A nationwide experience. Int. J. STD AIDS 2021, 32, 435–443. [Google Scholar] [CrossRef] [PubMed]
- Collins, L.F.; Moran, C.A.; Oliver, N.T.; Moanna, A.; Lahiri, C.D.; Colasanti, J.A.; Kelley, C.F.; Nguyen, M.L.; Marconi, V.C.; Armstrong, W.S.; et al. Clinical characteristics, comorbidities and outcomes among persons with HIV hospitalized with coronavirus disease 2019 in Atlanta, Georgia. AIDS 2020, 34, 1789–1794. [Google Scholar] [CrossRef] [PubMed]
- Del Amo, J.; Polo, R.; Moreno, S.; Diaz-Brito, V.; Martínez, E.; Arribas, J.R.; Jarrín, I.; Hernán, M.A. Incidence and Severity of COVID-19 in HIV-Positive Persons Receiving Antiretroviral Therapy. Ann. Intern. Med. 2020, 173, 536–541. [Google Scholar] [CrossRef] [PubMed]
- Di Biagio, A.; Ricci, E.; Calza, L.; Squillace, N.; Menzaghi, B.; Rusconi, S.; Orofino, G.; Bargiacchi, O.; Molteni, C.; Valsecchi, L.; et al. Factors associated with hospital admission for COVID-19 in HIV patients. AIDS 2020, 34. [Google Scholar] [CrossRef]
- Erinoso, O.A.; Wright, K.O.; Anya, S.; Bowale, A.; Adejumo, O.; Adesola, S.; Osikomaiya, B.; Mutiu, B.; Saka, B.; Falana, A.; et al. Clinical characteristics, predictors of symptomatic coronavirus disease 2019 and duration of hospitalisation in a cohort of 632 Patients in Lagos State, Nigeria. Niger. Postgrad. Med. J. 2020, 27, 285–292. [Google Scholar] [CrossRef]
- Etienne, N.; Karmochkine, M.; Slama, L.; Pavie, J.; Batisse, D.; Usubillaga, R.; Letembet, V.-A.; Brazille, P.; Canouï, E.; Slama, D.; et al. HIV infection and COVID-19: Risk factors for severe disease. AIDS 2020, 34, 1771–1774. [Google Scholar] [CrossRef]
- Gervasoni, C.; Meraviglia, P.; Riva, A.; Giacomelli, A.; Oreni, L.; Minisci, D.; Atzori, C.; Ridolfo, A.; Cattaneo, D. Clinical Features and Outcomes of Patients With Human Immunodeficiency Virus With COVID-19. Clin. Infect. Dis. 2020, 71, 2276–2278. [Google Scholar] [CrossRef]
- Geteneh, A.; Alemnew, B.; Tadesse, S.; Girma, A. Clinical characteristics of patients infected with SARS-CoV-2 in North Wollo Zone, North-East Ethiopia. Pan Afr. Med. J. 2021, 38. [Google Scholar] [CrossRef]
- Gudipati, S.; Brar, I.; Murray, S.; McKinnon, J.E.; Yared, N.; Markowitz, N. Descriptive Analysis of Patients Living With HIV Affected by COVID-19. JAIDS J. Acquir. Immune Defic. Syndr. 2020, 85, 123–126. [Google Scholar] [CrossRef]
- Hadi, Y.B.; Naqvi, S.F.; Kupec, J.T.; Sarwari, A.R. Characteristics and outcomes of COVID-19 in patients with HIV: A multicentre research network study. AIDS 2020, 34, F3–F8. [Google Scholar] [CrossRef]
- Härter, G.; Spinner, C.D.; Roider, J.; Bickel, M.; Krznaric, I.; Grunwald, S.; Schabaz, F.; Gillor, D.; Postel, N.; Mueller, M.C.; et al. COVID-19 in people living with human immunodeficiency virus: A case series of 33 patients. Infection 2020, 48, 681–686. [Google Scholar] [CrossRef] [PubMed]
- Ho, H.-E.; Peluso, M.J.; Margus, C.; Lopes, J.P.M.; He, C.; Gaisa, M.M.; Osorio, G.; Aberg, J.A.; Mullen, M.P. Clinical Outcomes and Immunologic Characteristics of Coronavirus Disease 2019 in People With Human Immunodeficiency Virus. J. Infect. Dis. 2020, 223, 403–408. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Xie, N.; Hu, X.; Yan, H.; Ding, J.; Liu, P.; Ma, H.; Ruan, L.; Li, G.; He, N.; et al. Epidemiological, Virological and Serological Features of Coronavirus Disease 2019 (COVID-19) Cases in People Living With Human Immunodeficiency Virus in Wuhan: A Population-based Cohort Study. Clin. Infect. Dis. 2020, 73, e2086–e2094. [Google Scholar] [CrossRef] [PubMed]
- Inciarte, A.; Gonzalez-Cordon, A.; Rojas, J.; Torres, B.; De Lazzari, E.; De La Mora, L.; Martinez-Rebollar, M.; Laguno, M.; Callau, P.; Gonzalez-Navarro, A.; et al. Clinical characteristics, risk factors, and incidence of symptomatic coronavirus disease 2019 in a large cohort of adults living with HIV: A single-center, prospective observational study. AIDS 2020, 34, 1775–1780. [Google Scholar] [CrossRef] [PubMed]
- Isernia, V.; Julia, Z.; Le Gac, S.; Bachelard, A.; Landman, R.; Lariven, S.; Joly, V.; Deconinck, L.; Rioux, C.; Lescure, X.; et al. SARS-COV2 infection in 30 HIV-infected patients followed-up in a French University Hospital. Int. J. Infect. Dis. 2020, 101, 49–51. [Google Scholar] [CrossRef] [PubMed]
- Izquierdo, J.L.; Ancochea, J.; Soriano, J.B. Savana COVID-19 Research Group Clinical Characteristics and Prognostic Factors for Intensive Care Unit Admission of Patients With COVID-19: Retrospective Study Using Machine Learning and Natural Language Processing. J. Med Internet Res. 2020, 22, e21801. [Google Scholar] [CrossRef] [PubMed]
- Karim, F.; Gazy, I.; Cele, S.; Zungu, Y.; Krause, R.; Bernstein, M.; Ganga, Y.; Rodel, H.; Mthabela, N.; Mazibuko, M. Hiv infection alters sars-cov-2 responsive immune parameters but not clinical outcomes in COVID-19 disease. medRxiv 2020. [Google Scholar] [CrossRef]
- Kirenga, B.; Muttamba, W.; Kayongo, A.; Nsereko, C.; Siddharthan, T.; Lusiba, J.; Mugenyi, L.; Byanyima, R.K.; Worodria, W.; Nakwagala, F. Characteristics and outcomes of admitted patients infected with sars-cov-2 in uganda. BMJ Open Respir. Res. 2020, 7, e000646. [Google Scholar] [CrossRef]
- Liu, J.; Zeng, W.; Cao, Y.; Cui, Y.; Li, Y.; Yao, S.; Alwalid, O.; Yang, F.; Fan, Y.; Shi, H. Effect of a previous history of antiretroviral treatment on the clinical picture of patients with co-infection of SARS-CoV-2 and hiv: A preliminary study. Int. J. Infect. Dis. 2020, 100, 141–148. [Google Scholar] [CrossRef]
- Maggiolo, F.; Zoboli, F.; Arosio, M.; Valenti, D.; Guarneri, D.; Sangiorgio, L.; Ripamonti, D.; Callegaro, A. SARS-CoV-2 infection in persons living with hiv: A single center prospective cohort. J. Med. Virol. 2021, 93, 1145–1149. [Google Scholar] [CrossRef]
- Migisha, R.; Kwesiga, B.; Mirembe, B.B.; Amanya, G.; Kabwama, S.N.; Kadobera, D.; Bulage, L.; Nsereko, G.; Wadunde, I.; Tindyebwa, T. Early cases of sars-cov-2 infection in uganda: Epidemiology and lessons learned from risk-based testing approaches–march-april 2020. Glob. Health 2020, 16, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Miyashita, H.; Kuno, T. Prognosis of coronavirus disease 2019 (COVID-19) in patients with HIV infection in New York City. HIV Med. 2020, 22. [Google Scholar] [CrossRef] [PubMed]
- Nachega, J.B.; Ishoso, D.K.; Otokoye, J.O.; Hermans, M.P.; Machekano, R.N.; Sam-Agudu, N.A.; Nswe Bongo-Pasi, C.; Mbala-Kingebeni, P.; Ntwan Madinga, J.; Mukendi, S.; et al. Clinical characteristics and outcomes of patients hospitalized for COVID-19 in Africa: Early insights from the Democratic Republic of the Congo. Am. J. Trop. Med. Hyg. 2020, (in press). [Google Scholar] [CrossRef] [PubMed]
- Ombajo, L.A.; Mutono, N.; Sudi, P.; Mutua, M.; Sood, M.; Loo, A.M.A.; Juma, P.; Odhiambo, J.; Shah, R.; Wangai, F.; et al. Epidemiological and clinical characteristics of COVID-19 patients in kenya. medRxiv 2020. [Google Scholar] [CrossRef]
- Parker, A.; Koegelenberg, C.F.N.; Moolla, M.S.; Louw, E.H.; Mowlana, A.; Nortjé, A.; Ahmed, R.; Brittain, N.; Lalla, U.; Allwood, B.W.; et al. High HIV prevalence in an early cohort of hospital admissions with COVID-19 in Cape Town, South Africa. S. Afr. Med. J. 2020, 110, 982. [Google Scholar] [CrossRef]
- Pujari, S.; Gaikwad, S.; Chitalikar, A.; Dabhade, D.; Joshi, K.; Bele, V. Short Communication: Coronavirus Disease 19 Among People Living with HIV in Western India: An Observational Cohort Study. AIDS Res. Hum. Retrovir. 2021, 37, 620–623. [Google Scholar] [CrossRef]
- Rodriguez-Gonzalez, C.G.; Chamorro-De-Vega, E.; Valerio, M.; Amor-Garcia, M.A.; Tejerina, F.; Sancho-Gonzalez, M.; Narrillos-Moraza, A.; Gimenez-Manzorro, A.; Manrique-Rodriguez, S.; Machado, M.; et al. COVID-19 in hospitalised patients in Spain: A cohort study in Madrid. Int. J. Antimicrob. Agents 2020, 57, 106249. [Google Scholar] [CrossRef]
- Rodríguez-Molinero, A.; Gálvez-Barrón, C.; Miñarro, A.; Macho, O.; López, G.F.; Robles, M.T.; Dapena, M.D.; Martínez, S.; Ràfols, N.M.; Monaco, E.E.; et al. Association between COVID-19 prognosis and disease presentation, comorbidities and chronic treatment of hospitalized patients. PLoS ONE 2020, 15, e0239571. [Google Scholar] [CrossRef]
- Shalev, N.; Scherer, M.; Lasota, E.D.; Antoniou, P.; Yin, M.T.; Zucker, J.; Sobieszczyk, M.E. Clinical Characteristics and Outcomes in People Living With Human Immunodeficiency Virus Hospitalized for Coronavirus Disease 2019. Clin. Infect. Dis. 2020, 71, 2294–2297. [Google Scholar] [CrossRef]
- Shi, P.; Ren, G.; Yang, J.; Li, Z.; Deng, S.; Li, M.; Wang, S.; Xu, X.; Chen, F.; Li, Y.; et al. Clinical characteristics of imported and second-generation coronavirus disease 2019 (COVID-19) cases in shaanxi outside wuhan, china: A multicentre retrospective study. Epidemiol. Infect. 2020, 148, e238. [Google Scholar] [CrossRef]
- Sigel, K.; Swartz, T.; Golden, E.; Paranjpe, I.; Somani, S.; Richter, F.; De Freitas, J.K.; Miotto, R.; Zhao, S.; Polak, P.; et al. Coronavirus 2019 and People Living With Human Immunodeficiency Virus: Outcomes for Hospitalized Patients in New York City. Clin. Infect. Dis. 2020, 71, 2933–2938. [Google Scholar] [CrossRef] [PubMed]
- Tesoriero, J.M.; Swain, C.-A.E.; Pierce, J.L.; Zamboni, L.; Wu, M.; Holtgrave, D.R.; Gonzalez, C.J.; Udo, T.; Morne, J.E.; Hart-Malloy, R.; et al. COVID-19 Outcomes Among Persons Living With or Without Diagnosed HIV Infection in New York State. JAMA Netw. Open 2021, 4, e2037069. [Google Scholar] [CrossRef] [PubMed]
- Virata, M.D.; Shenoi, S.; Ladines-Lim, J.B.; Villanueva, M.; Aoun-Barakat, L. 111. Outcomes Related to COVID-19 Among People Living with HIV: Cohort from a Large Academic Center. Open Forum Infect. Dis. 2020, 7, S184. [Google Scholar] [CrossRef]
- Wang, R.; Pan, M.; Zhang, X.; Han, M.; Fan, X.; Zhao, F.; Miao, M.; Xu, J.; Guan, M.; Deng, X.; et al. Epidemiological and clinical features of 125 Hospitalized Patients with COVID-19 in Fuyang, Anhui, China. Int. J. Infect. Dis. 2020, 95, 421–428. [Google Scholar] [CrossRef] [PubMed]
- Yang, R.; Gui, X.; Zhang, Y.; Xiong, Y.; Gao, S.; Ke, H. Clinical characteristics of COVID-19 patients with HIV coinfection in Wuhan, China. Expert Rev. Respir. Med. 2020, 15, 403–409. [Google Scholar] [CrossRef]
- Yu, Y.; Tu, J.; Lei, B.; Shu, H.; Zou, X.; Li, R.; Huang, C.; Qu, Y.; Shang, Y. Incidence and Risk Factors of Deep Vein Thrombosis in Hospitalized COVID-19 Patients. Clin. Appl. Thromb. 2020, 26. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Diagnoses of Hiv Infection in the United States and Dependent Areas, 2014; HIV Surveillance Report; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2015; Volume 25, pp. 1–82. [Google Scholar]
- Joint United Nations Programme on HIV/AIDS (UNAIDS). Global HIV & AIDS Statistics—Fact Sheet; UNAIDS: Geneva, Switzerland, 2021. [Google Scholar]
- 2020 Global AIDS Update—Seizing the Moment—Tackling Entrenched Inequalities to End Epidemics. Available online: https://www.unaids.org/en/resources/documents/2020/global-aids-report (accessed on 24 August 2021).
- Blanco, J.L.; Ambrosioni, J.; García, F.; Martínez, E.; Soriano, A.; Mallolas, J.; Miro, J.M. COVID-19 in patients with HIV: Clinical case series. Lancet HIV 2020, 7, e314–e316. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. CDC COVID Data Tracker. Available online: https://covid.cdc.gov/covid-data-tracker/#national-lab (accessed on 24 August 2021).
- Patel, R.H.; Acharya, A.; Chand, H.S.; Mohan, M.; Byrareddy, S.N. Human Immunodeficiency Virus and Severe Acute Respiratory Syndrome Coronavirus 2 Coinfection: A Systematic Review of the Literature and Challenges. AIDS Res. Hum. Retroviruses 2021, 37, 266–282. [Google Scholar] [CrossRef]
- Pelchen-Matthews, A.; Ryom, L.; Borges, H.; Edwards, S.; Duvivier, C.; Stephan, C.; Sambatakou, H.; Maciejewska, K.; Portu, J.J.; Weber, J.; et al. Aging and the evolution of comorbidities among HIV-positive individuals in a European cohort. AIDS 2018, 32, 2405–2416. [Google Scholar] [CrossRef] [Green Version]
- Zhang, H.; Wu, T. CD4+T, CD8+T counts and severe COVID-19: A meta-analysis. J. Infect. 2020, 81, e82–e84. [Google Scholar] [CrossRef]
- Atyeo, C.; Fischinger, S.; Zohar, T.; Slein, M.D.; Burke, J.; Loos, C.; McCulloch, D.J.; Newman, K.L.; Wolf, C.; Yu, J.; et al. Distinct Early Serological Signatures Track with SARS-CoV-2 Survival. Immunity 2020, 53, 524–532.e4. [Google Scholar] [CrossRef] [PubMed]
- Fenwick, C.; Joo, V.; Jacquier, P.; Noto, A.; Banga, R.; Perreau, M.; Pantaleo, G. T-cell exhaustion in HIV infection. Immunol. Rev. 2019, 292, 149–163. [Google Scholar] [CrossRef] [PubMed]
- Moir, S.; Fauci, A.S. B-cell responses to HIV infection. Immunol. Rev. 2017, 275, 33–48. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.-Y.; Tsai, M.-S.; Kuo, K.-C.; Tsai, J.-C.; Sun, H.-Y.; Cheng, A.C.; Chang, S.-Y.; Lee, C.-H.; Hung, C.-C. Pneumococcal vaccination among HIV-infected adult patients in the era of combination antiretroviral therapy. Hum. Vaccines Immunother. 2014, 10, 3700–3710. [Google Scholar] [CrossRef] [Green Version]
- Ceravolo, A.; Orsi, G.B.; Parodi, V.; Ansaldi, F. Influenza vaccination in HIV-positive subjects: Latest evidence and future perspective. J. Prev. Med. Hyg. 2013, 54. [Google Scholar] [CrossRef]
- Geretti, A.M.; Doyle, T. Immunization for HIV-positive individuals. Curr. Opin. Infect. Dis. 2010, 23, 32–38. [Google Scholar] [CrossRef]
- Hogan, A.B.; Jewell, B.L.; Sherrard-Smith, E.; Vesga, J.F.; Watson, O.J.; Whittaker, C.; Hamlet, A.; Smith, J.A.; Winskill, P.; Verity, R.; et al. Potential impact of the COVID-19 pandemic on HIV, tuberculosis, and malaria in low-income and middle-income countries: A modelling study. Lancet Glob. Health 2020, 8, e1132–e1141. [Google Scholar] [CrossRef]
- Jewell, B.L.; Mudimu, E.; Stover, J.; Ten Brink, D.; Phillips, A.N.; Smith, J.A.; Martin-Hughes, R.; Teng, Y.; Glaubius, R.; Mahiane, S.G.; et al. Potential effects of disruption to HIV programmes in sub-Saharan Africa caused by COVID-19: Results from multiple mathematical models. Lancet HIV 2020, 7, e629–e640. [Google Scholar] [CrossRef]
- Simões, D.; Stengaard, A.R.; Combs, L.; Raben, D. The EuroTEST COVID-19 impact assessment consortium of partners Impact of the COVID-19 pandemic on testing services for HIV, viral hepatitis and sexually transmitted infections in the WHO European Region, March to August 2020. Eurosurveillance 2020, 25, 2001943. [Google Scholar] [CrossRef]
- WHO. Disruption in HIV, Hepatitis and STI Services Due to COVID-19, in Global HIV, Hepatitis and STI Programmes; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- Bhaskaran, K.; Rentsch, C.T.; MacKenna, B.; Schultze, A.; Mehrkar, A.; Bates, C.J.; Eggo, R.M.; Morton, C.E.; Bacon, S.C.J.; Inglesby, P.; et al. HIV infection and COVID-19 death: A population-based cohort analysis of UK primary care data and linked national death registrations within the OpenSAFELY platform. Lancet HIV 2020, 8, e24–e32. [Google Scholar] [CrossRef]
- Lunny, C.; Pieper, D.; Thabet, P.; Kanji, S. Managing overlap of primary study results across systematic reviews: Practical considerations for authors of overviews of reviews. BMC Med. Res. Methodol. 2021, 21, 1–14. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study Name (Year) | Country | Type of Study | Study Participants | Sample Size (M; F; T) | Age (Mean ± SD or Median, Range) | PLWH | PLWH Surviving | PLWH Non-Surviving | PLWH Severe | PLWH Non-Severe |
|---|---|---|---|---|---|---|---|---|---|---|
| Borobia et al. (2020) [35] | Spain | Retrospective | COVID-19 cases | 2226 (M = 1074; F = 1152) | 61 (IQR 46–78) | 13 | 9 | 4 | NR | NR |
| Boulle et al. (2020) [36] | South Africa | Retrospective | COVID-19 cases | 22,308 (NR) | (NR) | 3978 | 3863 | 115 | 601 | 3262 |
| Ceballos et al. (2021) [37] | Chile | Prospective | COVID-19 cases | 18,321 (M = 10300; F = 8021) | NR | 36 | 31 | 5 | 11 | 25 |
| Collins et al. (2020) [38] | USA | Case series | COVID-19 cases | 530 (NR) | NR | 20 | 17 | 3 | 3 | 17 |
| Del Amo et al. (2020) [39] | Spain | Prospective | HIV–SARS-CoV-2 coinfected cases | 236 (M = 204; F = 32; all PLWH) | NR | 236 | 216 | 20 | 15 | 221 |
| Di Biagio et al. (2020) [40] | Italy | Prospective | HIV–SARS-CoV-2 coinfected cases | 69 (NR; all PLWH) | NR | 69 | 62 | 7 | 4 | 58 |
| Docherty et al. (2020) [28] | UK | Prospective | COVID-19 cases | 20,133 (M = 12,068; F = 8065) | 73 (IQR 58–62) | 83 | 37 | 23 | NR | NR |
| Erinoso et al. (2020) [41] | Nigeria | Retrospective | COVID-19 cases | 632 (M = 385, F = 247) | 40.1 (SD ± 13.9) | 3 | NR | NR | NR | NR |
| Etienne et al. (2020) [42] | France | Prospective | HIV–SARS-CoV-2 coinfected cases | 54 (M = 33; F = 21; all PLWH) | 54 (range 47–60) | 54 | 53 | 1 | 19 | 35 |
| Geretti et al. (2020) [27] | UK | Prospective | COVID-19 cases | 47,592 (NR) | NR | 122 | 75 | 30 | NR | NR |
| Gervasoni et al. (2020) [43] | Italy | Retrospective | COVID-19 cases | 549 (NR) | 51 ± 11 | 47 | 45 | 2 | 2 | 34 |
| Geteneh et al. (2021) [44] | Ethiopia | Retrospective | COVID-19 cases | 372 (M = 279; F = 93) | 30 (5–85) | 6 | 5 | 1 | 1 | 5 |
| Gudipati et al. (2020) [45] | USA | Case series | COVID-19 cases | 7372 (NR) | NR | 14 | 11 | 3 | 2 | 12 |
| Hadi et al. (2020) [46] | USA | Retrospective | COVID-19 cases | 50,167 (NR) | NR | 404 | 384 | 20 | 78 | 326 |
| Harter et al. (2020) [47] | Germany | Retrospective | HIV–SARS-CoV-2 coinfected cases | 33 (M = 30; F = 3) | 48 (range 26–82) | 33 | 29 | 3 | 8 | 25 |
| Ho et al. (2021) [48] | USA | Retrospective | HIV–SARS-CoV-2 coinfected cases | 93 (M = 67; F = 23, T = 3; all PLWH) | 58 (range 52–65) | 93 | 74 | 19 | 19 | 74 |
| Huang et al. (2020) [49] | China | Retrospective | COVID-19 cases | 50368 (NR) | NR | 35 | 33 | 2 | 15 | 20 |
| Inciarte et al. (2020) [50] | Spain | Prospective | HIV–SARS-CoV-2 coinfected cases | 53 (NR) | NR | 53 | 51 | 2 | 10 | 43 |
| Isernia et al. (2020) [51] | France | Case series | COVID-19 cases | 390 (NR) | NR | 30 | 24 | 2 | 4 | 24 |
| Izquierdo et al. (2020) [52] | Spain | Retrospective | COVID-19 cases | 10504 (M = 5519; F = 4984) | 58.2 ± 19.7 | 34 | NR | NR | 1 | 33 |
| Karim et al. (2020) [53] | South Africa | Retrospective | COVID-19 cases | 124 (M = 30; F = 94) | 45 (IQR, 35.0–57.4) | 55 | NR | NR | 16 | 39 |
| Kirenga et al. (2020) [54] | Uganda | Prospective | COVID-19 cases | 56 (M = 38; F = 18) | 34.2 ± 15.5 | 4 | 4 | 0 | NR | NR |
| Liu et al. (2020) [55] | China | Retrospective | HIV–SARS-CoV-2 coinfected cases | 20 (M = 5; F = 15) | 46.5 (IQR, 39.3–50.5) | 20 | 19 | 1 | 3 | 17 |
| Maggiolo et al. (2021) [56] | Italy | Prospective | HIV–SARS-CoV-2 coinfected cases | 55 (M = 44; F = 11) | 54 (49–58) | 55 | 51 | 4 | 11 | 44 |
| Migisha et al. (2020) [57] | Uganda | Retrospective | COVID-19 cases | 54 (M = 34; F = 20) | NR | 2 | 2 | 0 | 0 | 2 |
| Miyashita and Kuno (2021) [58] | USA | Retrospective | COVID-19 cases | 8912 (NR) | NR | 161 | 138 | 23 | 36 | 125 |
| Nachega et al. (2020) [59] | Congo | Retrospective | COVID-19 cases | 766 (M = 500; F = 262; unknown = 4) | 34 ± 4.5 | 12 | 10 | 2 | 3 | 9 |
| Ombajo et al. (2020) [60] | Kenya | Retrospective | COVID-19 cases | 787 (M = 505; F = 282) | 43 (range 0–109) | 53 | 42 | 11 | NR | NR |
| Parker et al. (2020) [61] | South Africa | Retrospective | COVID-19 cases | 113 (M = 44; F = 69) | NR | 24 | 18 | 6 | 5 | 19 |
| Pujari et al. (2021) [62] | India | Retrospective | HIV–SARS-CoV-2 coinfected cases | 86 (M = 66; F = 20) | 45 ± 52.3 | 86 | 80 | 6 | 17 | 69 |
| Rodriguez-Gonzalez et al. (2021) [63] | Spain | Retrospective | COVID-19 cases | 1255 (M = 725; F = 530) | 65 (range 51–77) | 12 | 9 | 3 | 1 | 11 |
| Rodriguez-Molinero et al. (2020) [64] | Spain | Prospective | COVID-19 cases | 418 (M = 238; F = 180) | 65.4 ± 16.6 | 3 | 2 | 1 | 3 | 0 |
| Shalev et al. (2020) [65] | USA | Retrospective | COVID-19 cases | 2159 (NR) | NR | 31 | 23 | 8 | 2 | 29 |
| Shi et al. (2020) [66] | China | Retrospective | COVID-19 cases | 134 (M = 65; F = 69) | 46 (IQR: 34–58) | 1 | 1 | 0 | 0 | 1 |
| Sigel et al. (2020) [67] | USA | Retrospective | COVID-19 cases | 4402 (NR) | NR | 88 | 70 | 18 | 18 | 70 |
| Silver et al. (2020) (60) | USA | Retrospective | COVID-19 cases | 249 (M = 110; F = 139) | 59.6 | 6 | NR | NR | NR | NR |
| Stoeckle et al. (2020) [34] | USA | Retrospective (case-control) | COVID-19 cases | 120 (M = 96; F = 24) | 60.5 (range 56.6–70.0) | 30 | 24 | 2 | 4 | NR |
| Tesoriero et al. (2021) [68] | USA | Descriptive | COVID-19 cases | 378248 (M = 192,646; F = 183,319) | NR | 2988 | 689 | 207 | 896 | 2092 |
| Virata et al. (2020) [69] | USA | Retrospective | HIV–SARS-CoV-2 coinfected cases | 40 (M = 20; F = 20) | NR | 40 | 40 | 0 | 4 | 36 |
| Vizcarra et al. (2020) [26] | Spain | Prospective | COVID-19 cases | 61,577 (NR) | NR | 51 | 44 | 2 | 6 | 45 |
| Wang et al. (2020) [70] | China | Descriptive | COVID-19 cases | 125 (M = 71; F = 54) | 38.76 ± 13.799 | 1 | 1 | 0 | NR | NR |
| Yang et al. (2021) [71] | China | Retrospective | COVID-19 cases | 188 | NR | 3 | NR | NR | NR | NR |
| Yu et al. (2020) [72] | China | Retrospective | COVID-19 cases | 142 (M = 81; F = 61) | 61.9 ± 12.4 | 8 | NR | NR | NR | NR |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oyelade, T.; Alqahtani, J.S.; Hjazi, A.M.; Li, A.; Kamila, A.; Raya, R.P. Global and Regional Prevalence and Outcomes of COVID-19 in People Living with HIV: A Systematic Review and Meta-Analysis. Trop. Med. Infect. Dis. 2022, 7, 22. https://doi.org/10.3390/tropicalmed7020022
Oyelade T, Alqahtani JS, Hjazi AM, Li A, Kamila A, Raya RP. Global and Regional Prevalence and Outcomes of COVID-19 in People Living with HIV: A Systematic Review and Meta-Analysis. Tropical Medicine and Infectious Disease. 2022; 7(2):22. https://doi.org/10.3390/tropicalmed7020022
Chicago/Turabian StyleOyelade, Tope, Jaber S. Alqahtani, Ahmed M. Hjazi, Amy Li, Ami Kamila, and Reynie Purnama Raya. 2022. "Global and Regional Prevalence and Outcomes of COVID-19 in People Living with HIV: A Systematic Review and Meta-Analysis" Tropical Medicine and Infectious Disease 7, no. 2: 22. https://doi.org/10.3390/tropicalmed7020022