1. Introduction
Potassium permanganate (KMnO
4), an inorganic compound composed of potassium (K
+) and manganate (MnO
4−) is an oxidizing agent which, when in contact with tissue, causes cellular destruction with liquefactive necrosis due to the formation of potassium hydroxide, a strong alkaline corrosive agent [
1].
Potassium permanganate is used both by large-scale industry and in domestic dwellings. Potassium permanganate has numerous applications including its use as an oxidizing reagent in the chemical synthesis of many organic compounds [
2]. Significant amounts are used for the synthesis of ascorbic acid, chloramphenicol, saccharin, isonicotinic acid and pyrazinoic acid. In well water treatment, KMnO
4 is used for removal of hydrogen sulphide and iron, eliminating the rotten egg odour, via a Manganese greensand filter [
3]. It also is used to control nuisance fresh-water organisms, such as zebra mussels, in water collection and treatment facilities [
4]. The shelf life/preservation of bananas is extended with KMnO
4 as it removes the ethylene which causes fruit to ripen and rot [
5,
6,
7].
Medically, KMnO
4 is used topically for skin conditions including fungal infections of the foot, impetigo, pemphigus, superficial wounds, dermatitis, and tropical ulcers [
8,
9].
It is commercially available as powder, crystals, tablets, and in solution. Tablets of 400 mg of KMnO
4 and the standard solution of 1 in 100 parts both require dilution with water to a final concentration of 1 in 10,000 parts before medical use [
10]. A 2% of the molar mass solution can be made by dissolving 3.2 g of KMnO
4 crystals in one litre of water for topical use [
11].
In our setting KMnO
4 is kept in most homes and is frequently prescribed by traditional health practitioners (THP) for numerous ailments including swelling, abdominal pain, rashes and wounds [
12].
There is a high incidence of poisoning with KMnO
4 reported in paediatric studies. A South African study over a three-year period found KMnO
4 to be the most frequently ingested caustic agent in 54% (27) of their paediatric study group with a mean age of 2.4 years [
13].
However, there are no studies other than case reports of teenagers and adults ingesting KMnO4 in the literature. In our unit, the admission of teenage and adult patients for KMnO4 ingestion is not uncommon. The rationale of this study was to assess the number of admissions with KMnO4 ingestion and evaluate their outcomes as we have observed that these patients tend to have limited injury to the upper gastrointestinal tract, need minimal intervention, and seemingly have good outcomes compared to published case reports.
In many of the published case reports, patients ingested solid forms of KMnO
4 and sustained caustic effects and/or systemic complications. The immediate concern highlighted in case reports is the threat of airway obstruction [
14] or massive haemorrhage due to gastrointestinal erosions. Some patients required emergent intubation for airway oedema [
14,
15,
16] and others haemorrhage control of upper gastrointestinal bleeding [
17]. Systemic concerns in the literature include hepatic and renal failure, in some instances fatal [
14,
18,
19]. Methemoglobinemia is also documented as a complication of KMnO
4 ingestion from drinking household products [
20], well water [
21], and as prescribed by “witch doctors” [
22]. Cardiovascular depression and collapse with shock is another feature of severe KMnO
4 poisoning although the pathogenesis is uncertain [
18].
The aim of this study was to ascertain the reasons for ingestion, the extent and severity of injury as determined by upper gastro-intestinal studies, and patient outcomes in comparison with the available global literature.
2. Materials and Methods
A retrospective study was performed of all patients admitted with KMnO4 ingestion to the adult wards at Ngwelezana Hospital, Empangeni, South Africa. At our institution, any patient over the age of twelve is admitted to the adult wards. The study was done over a two-year period between December 2019 and December 2021.
Patients were identified from the General Surgery patient admissions database using search terms: KMnO4, caustic ingestion, poisoning, and potassium permanganate. Patient files were retrieved from the hospital registry office and data collected, collated and stored with no personal identifiers on a password encrypted laptop.
Inclusion criteria were all patients over twelve years of age, admitted to the adult wards with only KMnO4 ingestion. Patients who had swallowed unknown substances or KMnO4 with other agents were excluded.
Data collected included patient demographics (age, gender and ethnicity), the reason for KMnO4 ingestion, and quantity/volume and form (tablets, solution, powder or crystals) swallowed. Findings of the clinical inspection of the oral cavity were noted.
All patients with KMnO
4 ingestion undergo an upper gastro-intestinal endoscopy (UGIE) if presenting within 72 h from the time of ingestion as per surgical unit protocol. If presentation is delayed over 72 h, a contrast swallow is performed. The investigation performed and the findings were collated. The oesophageal and gastric findings were graded as per the Zargar classification (
Table 1) [
23].
The duration of hospital stay and clinical outcomes were evaluated.
Statistical Analysis
Demographic data are expressed as original data or mean percentage where indicated. Categorical parametric data were compared using Chi-squared. A p-value of <0.05 was considered statistically significant. All statistical analyses were performed using GraphPad Prism 7.01 for Windows (GraphPad Software, San Diego, CA, USA).
3. Results
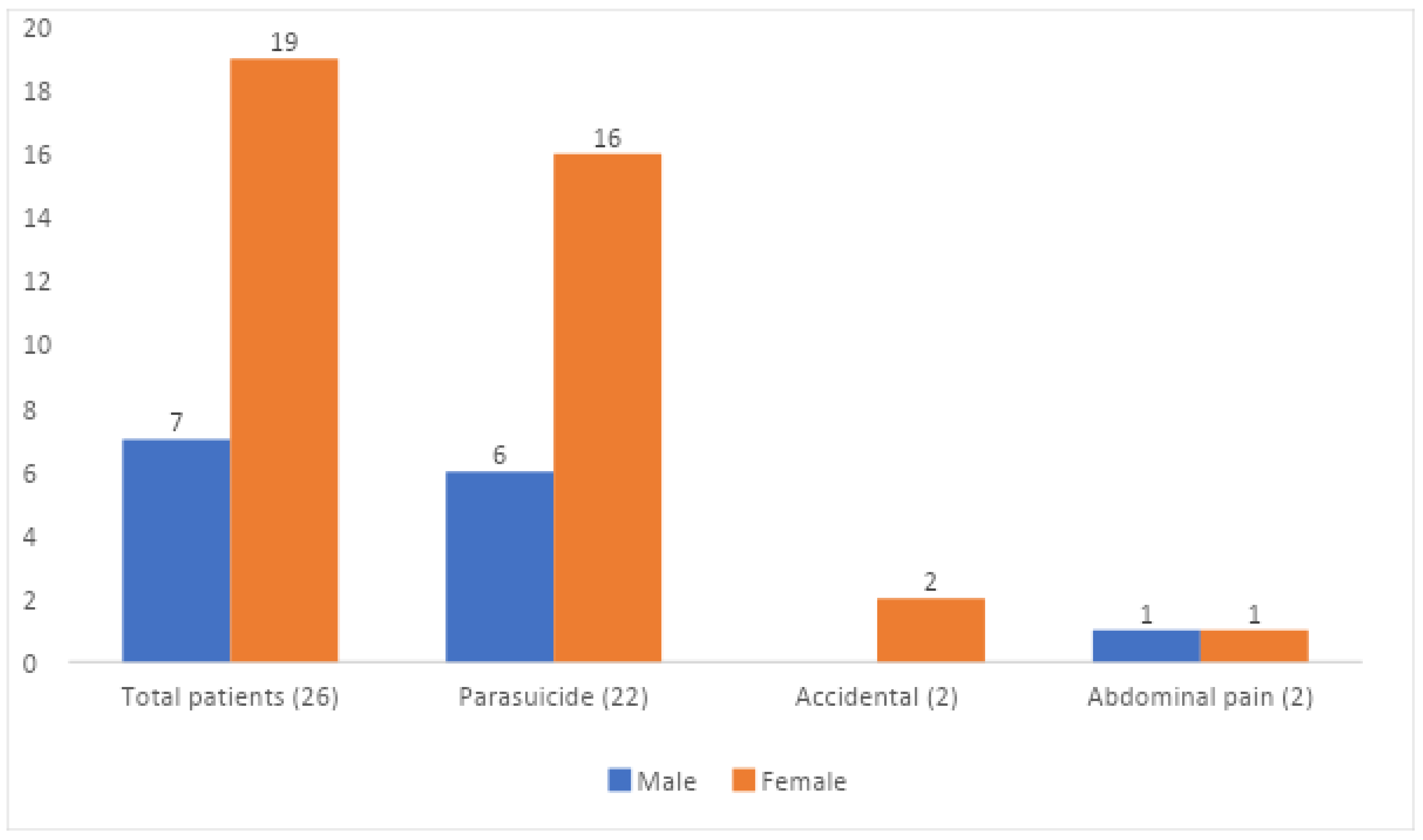
Data were collected on 26 patients who had ingested KMnO4: 19 (73%) female and seven (27%) males. The age range was 14–71 years with an average of 23.4 years. Two patients were less than 18 years of age; (14 and 17 years), and three patients were over 30 years of age. There was no significant difference in age between genders (female 23.7 years and male 22.7 years), p > 0.05.
All patients were of black ethnicity.
The main reason for ingestion of KMnO4 was parasuicide in 22 (84.6%), accidental in 2 (7.7%) and taken for abdominal pain in 2 (7.7%) cases.
There was no significant difference in suicidal intention between genders; 16/19 females (84.2%) and 6/7 (85.7%) males;
p = 0.60 (
Figure 1). The average age for female parasuicide was 20.4 years (14–31 years) and males, 23.6 years (21–41 years).
All bar one patient drank KMnO4 in solution (96%). The volume or amount of KMnO4 that was taken was difficult to assess; patients reported ingesting between 5 mL to 250 mL (average 70 mL) of liquid KMnO4 and one patient ate a few crystals.
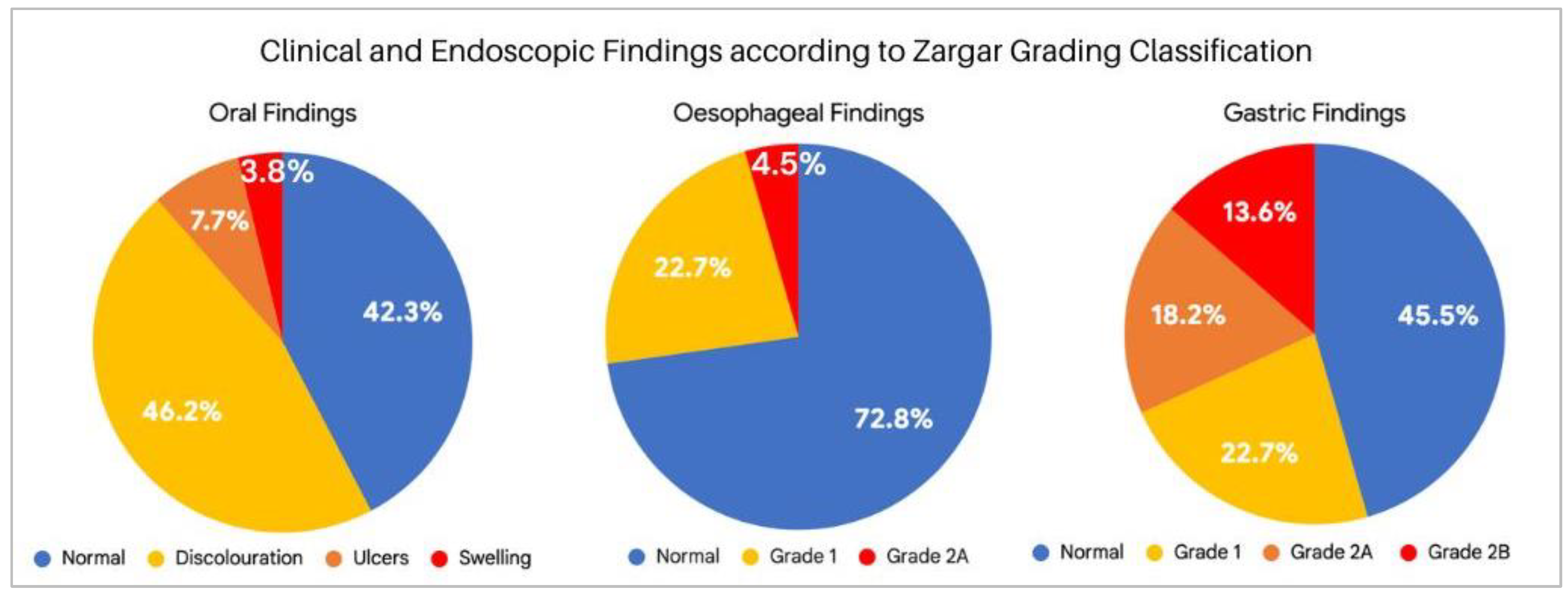
Inspection of the mouth and oral mucosa showed purple-blackish discoloration in 15 patients (58%), with associated oral mucosal ulceration in two (13%), while one patient (7%) also had intraoral swelling. The remaining 11 patients (42%) had no oral abnormality (
Figure 2).
The majority of patients, 24/26 (92%) underwent UGIE. Two patients (8%) had a contrast swallow due to delay in presentation to hospital.
Two endoscopy reports were not found.
Endoscopy findings were graded according to the Zargar classification of corrosive injury (
Table 1). Abnormalities were found in 69% of the 22 reported UGIEs.
Injury to the oesophagus alone was evident in three patients (14%). Corrosive injury to both the oesophagus and stomach was found in a further three patients (14%). The stomach alone was involved in nine patients (41%). One patient with gastric injury also had duodenal inflammation.
In total, six patients had an oesophageal injury: Zargar grade 1—83%; Zargar grade 2A—17% (
Figure 2).
The 12 patients with gastric injuries were classified as Zargar grade 1 in 42% (5 patients), Zargar grade 2A in 33% (4 patients) and Zargar grade 2B in 25% (3 patients). See
Figure 2.
The two contrast swallow studies were normal.
Patients who reported swallowing larger volumes—over 50 mL of KMnO4 solution—did not have worse endoscopy findings compared to those who drank less than 50 mL, p = 0.7. No patients in this cohort had systemic complications or features of organ failure.
All patients were discharged home well with a hospital duration ranging from 1 to 8 days with an average stay of 2.9 days. The three patients with Zargar grade 2B gastric injury were discharged on day two. The longer stays were for referral to psychiatric and social work services prior to discharge.
There were no reported complications at six weeks post KMnO4 ingestion.
4. Discussion
Caustic ingestion is common in children. It is usually accidental and KMnO
4 is often the substance ingested [
13]. However, the current literature on KMnO
4 ingestion in teenagers and adults is scanty and comprises only single case reports. This gives the impression that KMnO
4 poisoning is not commonly encountered in youth and adults.
At Ngwelezana Hospital it is not uncommon to admit adults and teenagers following KMnO4 ingestion. We undertook this study to document the assessment of these patients, the extent of the corrosive injury, and their outcomes.
Ngwelezana Hospital is in the province of KwaZulu-Natal, South Africa. The population demographics show that black Africans make up approximately 87% of the province’s population [
24]. All the patients in this study were of black ethnicity. Our facility, which is semi-rural, is the designated tertiary hospital for three districts. We receive referrals from 18 district hospitals and serve a predominantly rural population of around three million [
24].
Potassium permanganate is a readily accessible substance in our South African setting. Most black African households keep a bottle of KMnO
4 solution for cleaning purposes and use as a topical antiseptic agent. This is in an unknown concentration as over the counter KMnO
4 administrations require dilution prior to use [
10,
11]. Furthermore, in South Africa, KMnO
4 is commonly prescribed for medicinal use by up to 79% of traditional health practitioners (THP) [
12]. It is advocated for ailments such as wounds, rashes, aches, swelling and abdominal pain. It is advised for oral administration by THP in up to 42% of cases [
12]. Consulting a THP is a frequent undertaking by our rural population. A 2008 South African national survey noted that “three-quarters of the poorest quintile spent more than 10 per cent of their household expenditure in the previous month on traditional healers” [
25]. This emphasizes the potentially hazardous use (ingestion) of KMnO
4 in South Africa and the familiarity of this substance to patients as it is a household agent.
It appears that patients understand the potential health risk in drinking KMnO4, since the commonest indication for ingestion in this report was parasuicide (85% of patients).
Despite more females being admitted with KMnO
4 ingestion (3:1), males were as likely as females to swallow KMnO
4 in a suicide attempt, and were of a similar average age (early 20 s). Ingestion of KMnO
4 as a parasuicide agent may be due to the easy accessibility of the substance. Several case reports [
14,
17,
18,
26,
27] have been published with the same patient intent. The majority of patients in these parasuicide case reports were female with an average age of 36 years. Similarly, most of the suicide attempts in this study were by females. Females are more likely to perform less violent suicidal acts. The younger age of patients in our study and those attemping suicide may reflect the age spectrum of our province where about three-quarters of the population is less than 35 years of age [
24].
Two patients in this study (8%) had ingested KMnO4 for abdominal pain as per advice from a THP. In a 1975 case report, from our province in South Africa, two patients ingested KMnO4 for pain on advice from “witch doctors” and developed methemoglobinemia. Thus, the oral administration of KMnO4 by THP has been in practice for at least 50 years.
The question relating to volume or amount ingested and what was the KMnO
4 concentration is difficult to evaluate. All bar one patient swallowed a liquid solution of KMnO
4, but there is uncertainty with patient estimation of volume ingested and knowledge of dilution of KMnO
4. Ten grams (equivalent to 1.5 teaspoons of crystals) is lethal to an adult according to the 1969 Toxicology of Drugs and Chemicals [
2]. Ingestion of small amounts (4–20 mg/kg) of aqueous KMnO
4 solutions that are above 200 mg/L causes gastrointestinal distress [
28].
Bolus liquid KMnO
4 ingestion has caused respiratory arrest following coagulative necrosis and hemorrhage in the oesophagus, stomach, or liver [
28]. More than 1:5000 (200 mg/L) dilutions can irritate or discolor sensitive mucous membranes and direct skin or ocular contact with concentrated KMnO
4 can perforate tissues [
28]. In our study the greater volumes of KMnO
4 ingested (over 50 mL) did not show increased severity of mucosal injury on upper gastrointestinal endoscopy compared to those who ingested lesser volumes. This may be due to erroneous patient reporting on the volume of KMnO
4 solution taken or it being a very dilute solution.
The literature reports that KMnO
4 ingestion can be fatal as a consequence of local and systemic lesions, with most of the deaths occurring because of airway oedema, obstruction and hemorrhagic shock from massive upper gastrointestinal bleeding [
17,
19,
29].
Systemic toxic effects such as adult respiratory distress syndrome, coagulopathy, hepatic-renal failure, pancreatitis and death are believed to be due to oxidative injury [
19,
29]. In the majority of these case reports KMnO
4 was swallowed in a solid form (crystals, tablets and powder). None of these complications of toxic ingestion were noted in our study and there were no deaths.
A typical sign of KMnO
4 crystal ingestion is discoloration and oedema of the oral cavity [
1]. Only one of our study patients ingested KMnO
4 in a solid form (crystals). Oral discoloration with purple-blackish staining was however seen in over half (58%) of the patients from drinking KMnO
4 in solution. This shows that despite fluids being in the mouth for a shorter time, there still may be a visible abnormality. Two patients also had ulceration and one oral oedema from KMnO
4 solution. We postulate that the patients with intraoral ulceration and oedema drank KMnO
4 of a greater concentration.
As per our surgical unit protocol, all patients were admitted for analgesia and intravenous fluids and kept nil per mouth in preparation for UGIE. This was performed within 24 h of admission unless more than 72 h had elapsed since injury, in which case a contrast study was undertaken instead. This is done to avoid scope damage in a potentially injured friable gastrointestinal tract as the corrosive effect and possible necrosis progresses from the time of ingestion. Endoscopy is useful in diagnosing the extent and severity of injury to the upper gastro-intestinal tract, and it helps with the decision of when to feed the patient orally as well as when to discharge.
Endoscopic abnormalities compatible with KMnO
4 injury were present in over two-thirds (68%) of the 22 patients with available UGIE reports. The majority of these injuries to the oesophagus and stomach were Zargar grade 1 and 2A. These are less severe and did not impact on early dietary intake and discharge of patients. Potassium permanganate is an alkaline agent and therefore more likely to cause liquefactive necrosis of the oesophagus, and less likely to affect the stomach. In this study however we found gastric injury in over half (55%) of the patients undergoing UGIE. This has also been described in isolated case reports [
14,
15,
17]. The reason for the injury to the stomach may be due to KMnO
4 being ingested as a liquid, and therefore shorter oesophageal transit time.
Patients were discharged between one and eight days, with an average stay of 2.9 days. Those with more severe stomach injury (Zargar grade 2B) did not require longer hospital stays and all three were discharged on day two.
Longer in-hospital stays were for social worker and/or psychologist review of patients and not a result of complications of KMnO4 ingestion. Most case study patients in the literature were discharged after seven to fourteen days; a longer time period than our patients but many had more severe injuries and some were associated with an intensive care stay.
Despite what appears to be a relatively high incidence of KMnO4 ingestion in our semi-rural South African centre, complications and gastro-intestinal damage after ingestion are less than expected and of limited severity when compared to existing data.
Limitations of this Study
Limitations of this study include the inability to quantify the amount of KMnO4 taken, as most patients ingested a solution of unknown concentration and patient reporting of quantity is subjective. Additionally, no follow-up endoscopies were done to ensure healing of abnormalities; however, the absence of residual symptoms negated the need for follow-up endoscopy.





{kind=link}
{kind=link}