Surgical Treatment of Severe Bowel Obstruction as a Rare Complication Following Allogenic Hematopoietic Stem Cell Transplantation

 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
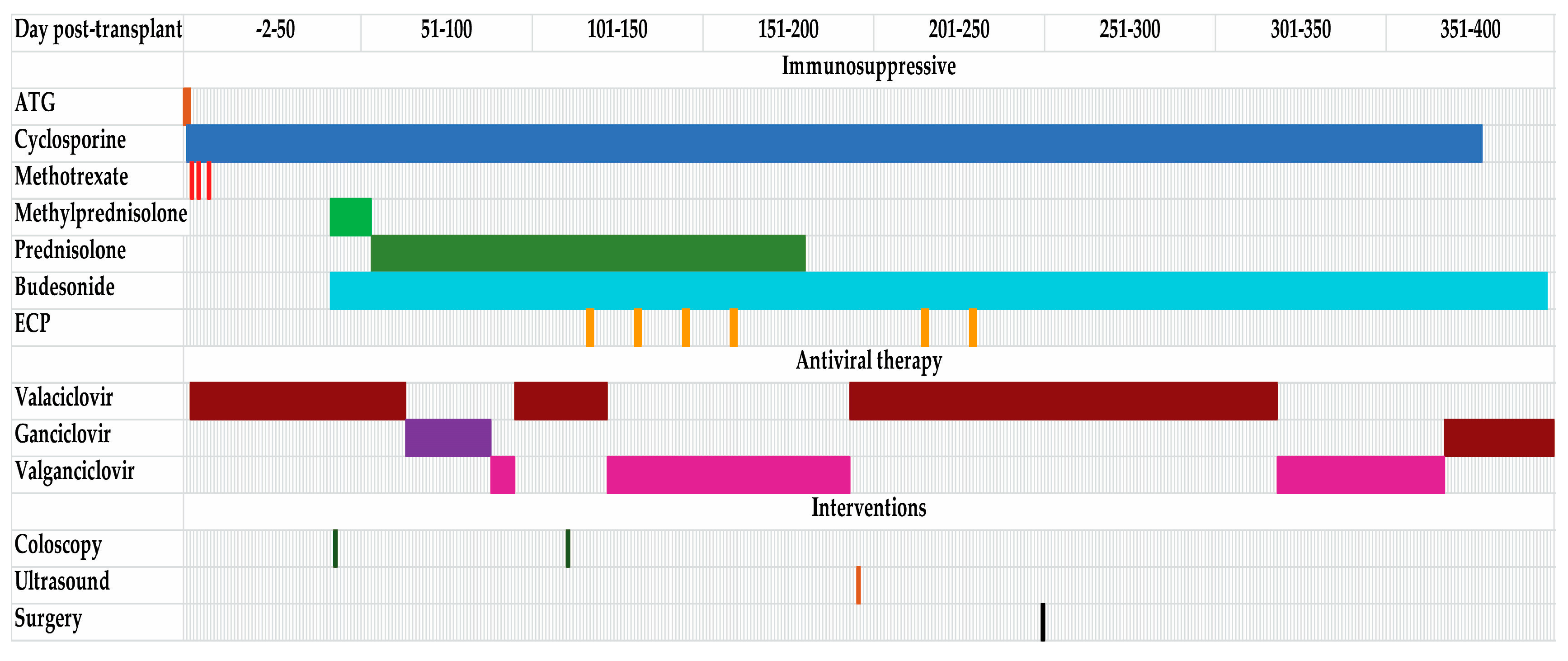
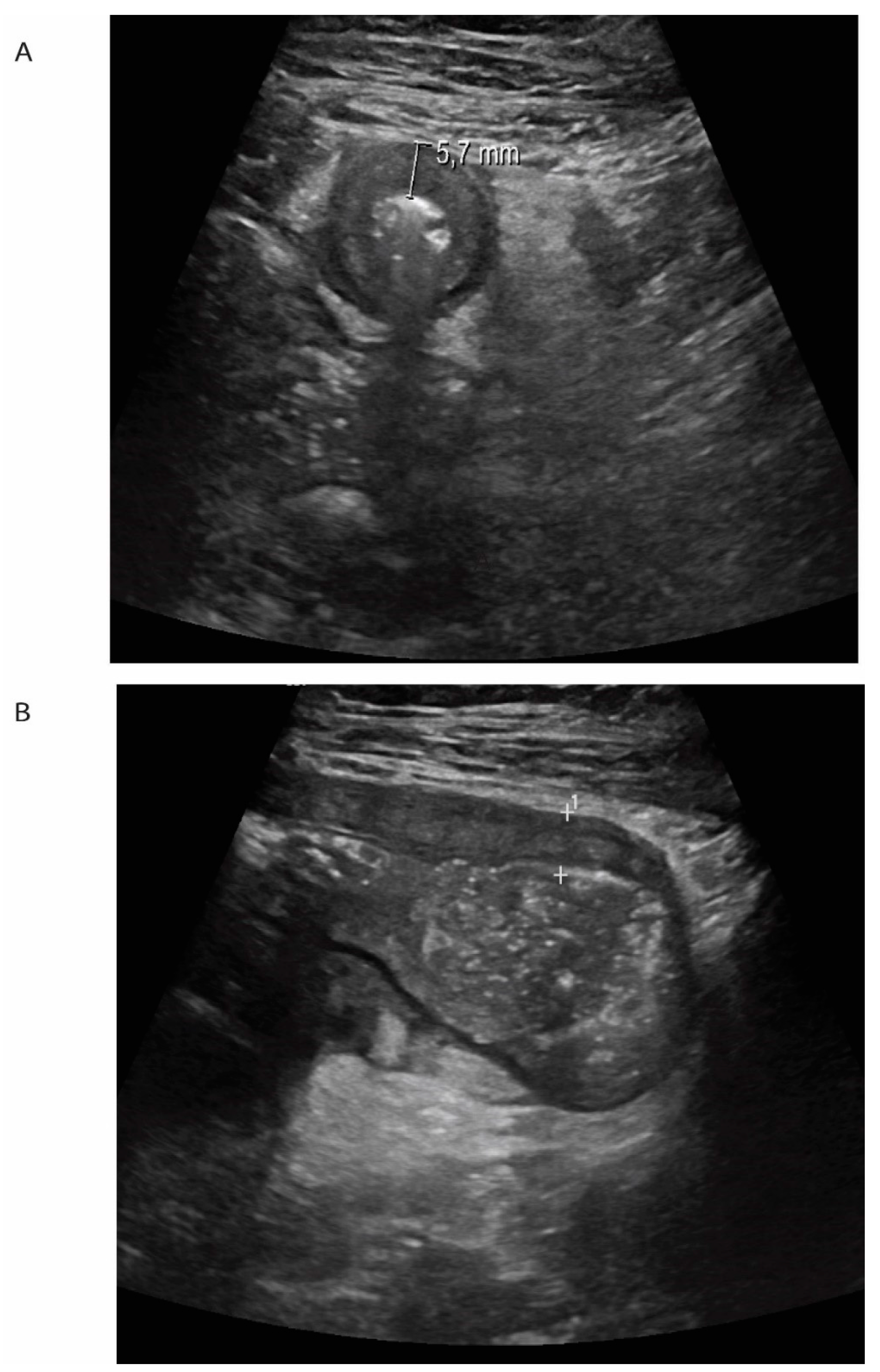
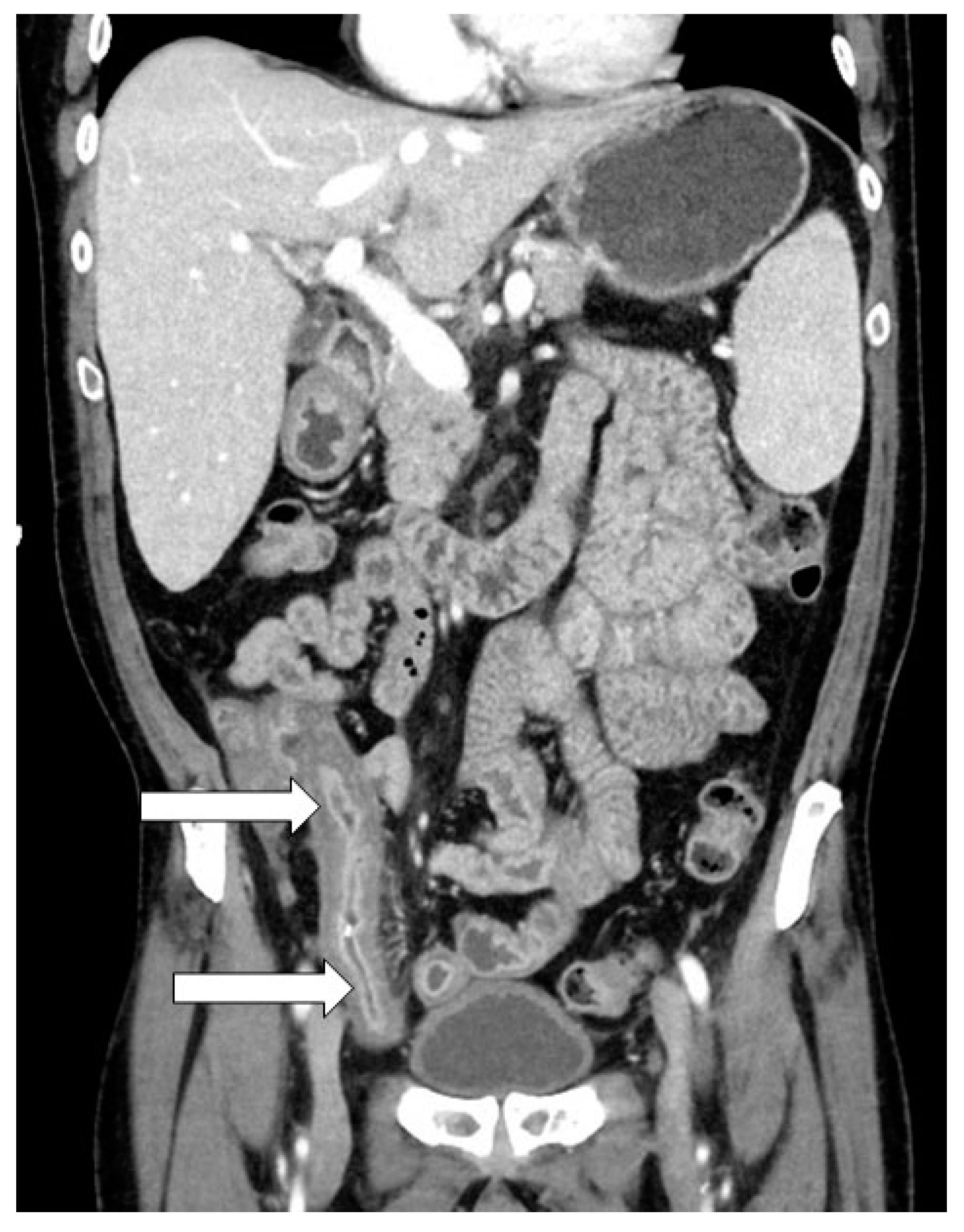
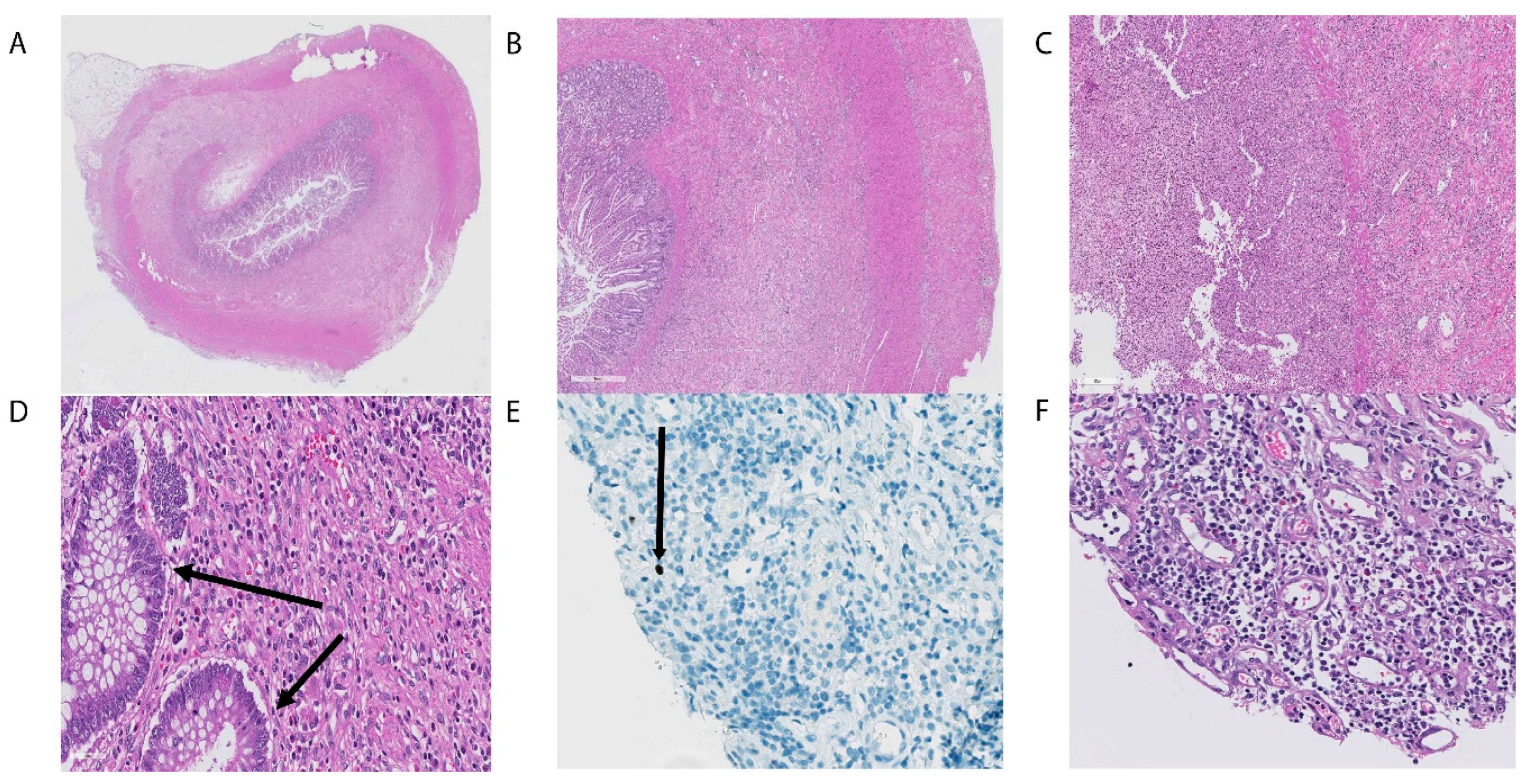
2. Case Report
3. Discussion
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Zeiser, R.; Blazar, B.R. Acute graft-versus-host disease—Biologic process, prevention, and therapy. N. Engl. J. Med. 2017, 377, 2167–2179. [Google Scholar] [CrossRef]
- Zeiser, R.; Blazar, B.R. Pathophysiology of Chronic graft-versus-host disease and therapeutic targets. N. Engl. J. Med. 2017, 377, 2565–2579. [Google Scholar] [CrossRef] [PubMed]
- Penack, O.; Marchetti, M.; Ruutu, T.; Aljurf, M.; Bacigalupo, A.; Bonifazi, F.; Ciceri, F.; Cornelissen, J.; Malladi, R.; Duarte, R.F.; et al. Prophylaxis and management of graft versus host disease after stem-cell transplantation for haematological malignancies: Updated consensus recommendations of the European Society for Blood and Marrow Transplantation. Lancet Haematol. 2020, 7, e157–e167. [Google Scholar] [CrossRef]
- Bruserud, Ø.; Tvedt, T.H.A.; Paulsen, P.Q.; Ahmed, A.B.; Gedde-Dahl, T.; Tjønnfjord, G.E.; Slåstad, H.; Heldal, D.; Reikvam, H. Extracorporeal photopheresis (photochemotherapy) in the treatment of acute and chronic graft versus host disease: Immunological mechanisms and the results from clinical studies. Cancer Immunol. Immunother. 2014, 63, 757–777. [Google Scholar] [CrossRef] [PubMed]
- Morata-Tarifa, C.; Macías-Sánchez, M.D.M.; Gutiérrez-Pizarraya, A.; Sanchez-Pernaute, R. Mesenchymal stromal cells for the prophylaxis and treatment of graft-versus-host disease—A meta-analysis. Stem Cell Res. Ther. 2020, 11, 64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hansen, B.-A.; Wendelbo, Ø.; Bruserud, Ø.; Hemsing, A.L.; Mosevoll, K.A.; Reikvam, H. Febrile neutropenia in acute leukemia. Epidemiology, etiology and treatment. Mediterr. J. Hematol. Infect. Dis. 2019, 12, e2020009. [Google Scholar] [CrossRef] [PubMed]
- Ljungman, P.; De La Camara, R.; Robin, C.; Crocchiolo, R.; Einsele, H.; Hill, J.A.; Hubacek, P.; Navarro, D.; Cordonnier, C.; Ward, K.N. Guidelines for the management of cytomegalovirus infection in patients with haematological malignancies and after stem cell transplantation from the 2017 European Conference on Infections in Leukaemia (ECIL 7). Lancet Infect. Dis. 2019, 19, e260–e272. [Google Scholar] [CrossRef]
- Della Porta, M.G.; Gallì, A.; Bacigalupo, A.; Zibellini, S.; Bernardi, M.; Rizzo, E.; Allione, B.; Van Lint, M.T.; Pioltelli, P.; Marenco, P.; et al. Clinical effects of driver somatic mutations on the outcomes of patients with myelodysplastic syndromes treated with allogeneic hematopoietic stem-cell transplantation. J. Clin. Oncol. 2016, 34, 3627–3637. [Google Scholar] [CrossRef] [PubMed]
- McDonald, G.B. How I treat acute graft-versus-host disease of the gastrointestinal tract and the liver. Blood 2016, 127, 1544–1550. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grønningsæter, I.S.; Tsykunova, G.; Lilleeng, K.; Ahmed, A.B.; Bruserud, Ø.; Reikvam, H. Bronchiolitis obliterans syndrome in adults after allogeneic stem cell transplantation-pathophysiology, diagnostics and treatment. Expert Rev. Clin. Immunol. 2017, 13, 553–569. [Google Scholar] [CrossRef]
- Martin, P.J. How I treat steroid-refractory acute graft-versus-host disease. Blood 2020, 135, 1630–1638. [Google Scholar] [CrossRef] [PubMed]
- Rao, K.; Rao, A.; Karlsson, H.; Jagani, M.; Veys, P.; Amrolia, P.J. Improved survival and preserved antiviral responses after combination therapy with daclizumab and infliximab in steroid-refractory graft-versus-host disease. J. Pediatr. Hematol. 2009, 31, 456–461. [Google Scholar] [CrossRef] [PubMed]
- Floisand, Y.; Lundin, K.E.A.; Lazarevic, V.; Kristiansen, J.D.; Osnes, L.T.N.; Tjonnfjord, G.E.; Reims, H.M.; Gedde-Dahl, T. Targeting Integrin alpha4beta7 in steroid-refractory intestinal graft-versus-host disease. Biol. Blood Marrow Transplant. 2017, 23, 172–175. [Google Scholar] [CrossRef] [Green Version]
- Ross, W. Treatment of gastrointestinal acute graft-versus-host disease. Curr. Treat. Options Gastroenterol. 2005, 8, 249–258. [Google Scholar] [CrossRef]
- Einsele, H.; Ljungman, P.T.; Boeckh, M.J. How I treat CMV reactivation after allogeneic hematopoietic stem cell transplantation. Blood 2020, 135, 1619–1629. [Google Scholar] [CrossRef] [PubMed]
- Torres, J.; Mehandru, S.; Colombel, J.F.; Peyrin-Biroulet, L. Crohn’s disease. Lancet 2017, 389, 1741–1755. [Google Scholar] [CrossRef]
- Gutierrez, C.A.; Raval, M.V.; Vester, H.R.; Chaudhury, S.; Von Allmen, D.; Rothstein, D. Surgical treatment of intestinal complications of graft versus host disease in the pediatric population: Case series and review of literature. J. Pediatr. Surg. 2017, 52, 1718–1722. [Google Scholar] [CrossRef]
- Irani, J.L.; Cutler, C.S.; Whang, E.E.; Clancy, T.E.; Russell, S.; Swanson, R.S.; Ashley, S.W.; Zinner, M.J.; Raut, C.P. Severe acute gastrointestinal graft-vs-host disease. Arch. Surg. 2008, 143, 1041–1045. [Google Scholar] [CrossRef] [Green Version]
- Gavel, G.; Marven, S.; Evans, M.J.; Walker, J.P.; Vora, A. Obliterative enteritis complicating graft versus host disease. Bone Marrow Transplant. 2003, 32, 1097–1098. [Google Scholar] [CrossRef] [Green Version]
- Cornell, R.F.; Palmer, J.; Komorowski, R.; Drobyski, W.R. Surgical resection as definitive treatment for refractory GVHD of the colon. Bone Marrow Transplant. 2012, 47, 1366–1367. [Google Scholar] [CrossRef] [Green Version]
- Chirletti, P.; Caronna, R.; Arcese, W.; Iori, A.P.; Calcaterra, D.; Cartoni, C.; Sammartino, P.; Stipa, V. Gastrointestinal emergencies in patients with acute intestinal graft-versus-host Disease. Leuk. Lymphoma 1998, 29, 129–137. [Google Scholar] [CrossRef] [PubMed]
- Turki, A.T.; Bayraktar, E.; Basu, O.; Benkö, T.; Yi, J.-H.; Kehrmann, J.; Tzalavras, A.; Liebregts, T.; Beelen, D.W.; Steckel, N.K. Ileostomy for steroid-resistant acute graft-versus-host disease of the gastrointestinal tract. Ann. Hematol. 2019, 98, 2407–2419. [Google Scholar] [CrossRef] [PubMed]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Reikvam, H.; Tvedt, T.H.A.; Johansen, S.; Aase Setran, H.; Havre, R.F. Surgical Treatment of Severe Bowel Obstruction as a Rare Complication Following Allogenic Hematopoietic Stem Cell Transplantation. Transplantology 2020, 1, 102-110. https://doi.org/10.3390/transplantology1020010
Reikvam H, Tvedt THA, Johansen S, Aase Setran H, Havre RF. Surgical Treatment of Severe Bowel Obstruction as a Rare Complication Following Allogenic Hematopoietic Stem Cell Transplantation. Transplantology. 2020; 1(2):102-110. https://doi.org/10.3390/transplantology1020010
Chicago/Turabian StyleReikvam, Håkon, Tor Henrik Anderson Tvedt, Silje Johansen, Hege Aase Setran, and Roald Flesland Havre. 2020. "Surgical Treatment of Severe Bowel Obstruction as a Rare Complication Following Allogenic Hematopoietic Stem Cell Transplantation" Transplantology 1, no. 2: 102-110. https://doi.org/10.3390/transplantology1020010