
A Novel Perspective for Examining and Comparing Real and Virtual Test Tasks Performed by the Dominant and Non-Dominant Hand in Healthy Adults

Bioinformatics Laboratory, Mossakowski Medical Research Institute Polish Academy of Sciences, 02-106 Warsaw, Poland
Symmetry 2021, 13(10), 1810; https://doi.org/10.3390/sym13101810
Submission received: 5 September 2021
/
Revised: 21 September 2021
/
Accepted: 24 September 2021
/
Published: 28 September 2021
(This article belongs to the Special Issue Cognition, Neuroscience and Asymmetry)
Abstract
:This study presents a novel perspective for the study of functional lateralization in a virtual reality environment. In the model study of handedness, the recognition of the dominant and non-dominant hand in real and virtual conditions was assessed using selected tests, such as a real light exposure test of Piórkowski’s apparatus and classical clinical tests, as well as virtual test tasks, in healthy adults. Statistically significant differences between the dominant and non-dominant hand were observed for tests carried out both in classical conditions and the virtual environment. The results and findings of other studies suggest that the virtual reality approach is a very promising and sensitive tool in the research on functional asymmetries in healthy and disease for motor skills and cognition processes.
1. Introduction
1.1. Novel Information Technologies and Virtual Reality Environments
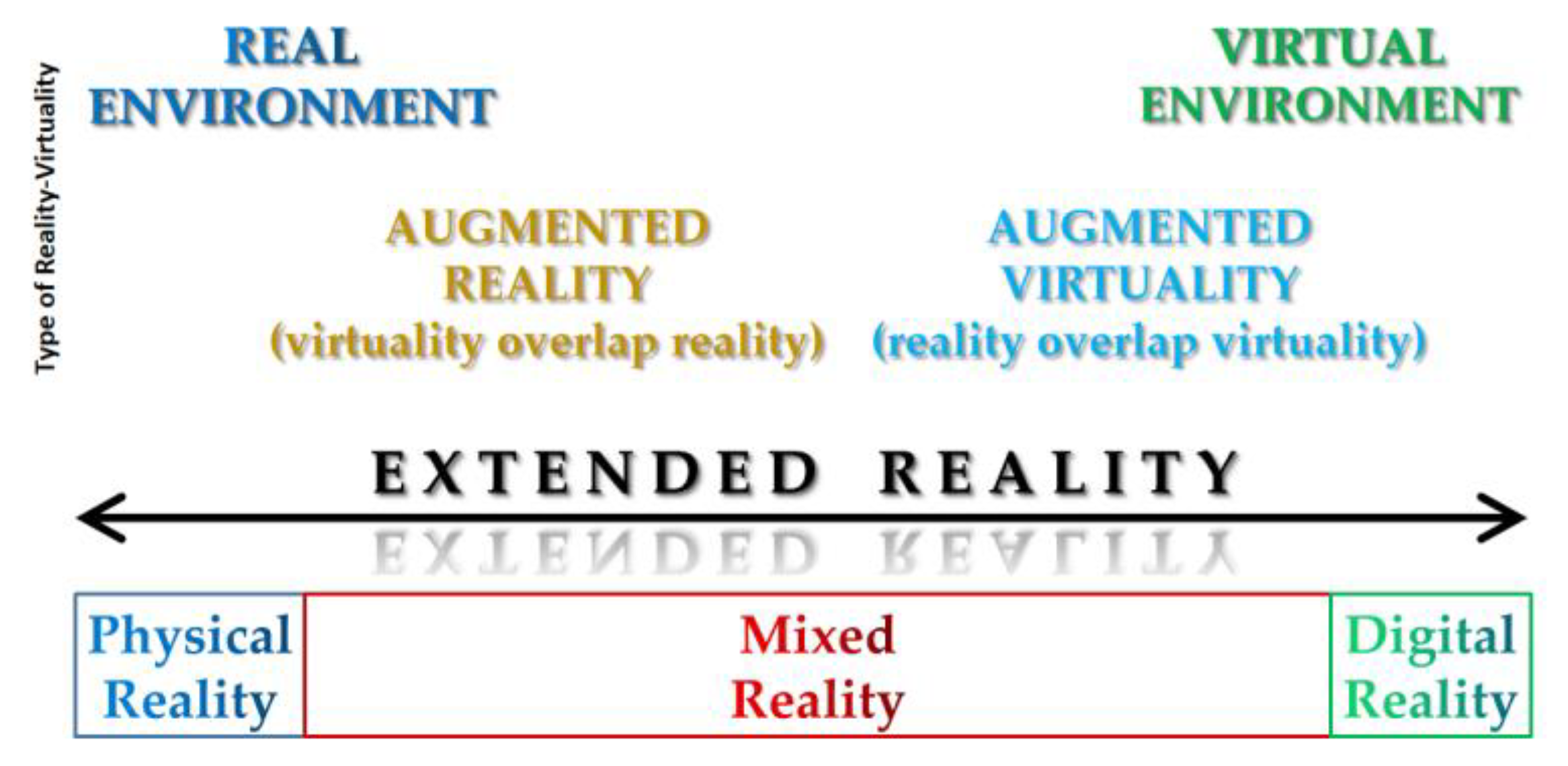
In the era of Internet and global digitalization, the development of information technology (IT) is evolving faster than ever [1,2]. The impact of the application of modern technologies on the life of human population is investigated, both in health and disease [3,4]. Among innovative technological solutions, such as artificial intelligence (AI), internet of things (IoT) platforms/devices/datasets, serverless computing or function as a service (FaaS) platforms, biometrics, robotics, virtual/augmented/mixed reality (VR/AR/MR) technologies, which are collectively known as extended reality (XR), play a special role [5,6]. In general, XR is a term that refers to all real-and-virtual combined environments and interactions generated by computer technology. An illustration of the type of reality classification based on the Reality-Virtuality continuum concept developed by Milgram, et al. [7] is shown in Figure 1 [8,9,10].
Virtual reality is the most known and used of novel technologies [11,12,13,14]. It is immersive, which prompts participants’ senses into thinking that events are happening in a different world from the real one. Additionally, by using, for example, a head-mounted display (HMD)/headset, participants experience a computer-generated world where they can manipulate objects/elements with a console, joystick or PC. In the case, augmented reality overlays digital information on elements of the real world to complement them [15,16]. Mixed reality combines the real world and digital elements. Overall, in MR, participants interact and manipulate both physical and virtual objects. MR allows users to see and immerse themself in the world around them, even while interacting with the virtual space. Thus, the concept of XR is a term that covers all technologies that enhance the senses, whether they provide additional information about the real world or create completely unreal, simulated worlds that we can experience. Currently, XR is expanding in many areas of human activity from games, movies/theaters/museums, travels, businesses, through the military, professional sports and education, to (neuro)science, healthcare and modern medical practice, and much more [17,18,19,20,21,22,23,24].
1.2. Hemispheric Asymmetries and Phenomenon of Handedness
The nature of the structural and functional hemispheric asymmetry (lateralization) has been extensively and thoroughly investigated in species from all major classes of vertebrate and in many invertebrates [27,28,29,30,31,32,33]. In humans, lateralization typically refers to a division of functional processing between two cerebral hemispheres, for instance left-hemisphere specialization for language and praxis and that of the right hemisphere for spatial attention, face recognition, and speech prosody is observed [34,35,36,37]. The phenomenon of handedness is an interesting example of functional asymmetry [38,39,40]. Approximately 75–90% of the human population prefer to use their right hand to realize a lot of tasks involving various levels of dexterity, and about 80% are right footed [41,42]. Control of hands is contralateral, the right hand is under the control of the left hemisphere and the left hand is under the control of the right hemisphere. Lateralization is a progressive process that develops with age [43] to include neuromotor development [40,44,45]. Various techniques are used to estimate lateralization, both in health [46,47,48] and disease [49,50]. Not only traditional hand preference questionnaires are used to measure handedness, but most of all performance variables because, as the studies emphasize, they are more objective than questionnaires [40,51]. Scientists also suggest that handedness cannot be predicted with a single measure of manual performance, because the measurements are unreliable due to their subjectivity [40,52].
Taking into account the above facts and in accordance with the proposal presented by Michel in his review [40], at least four basic methods of assessing human handedness can be distinguished. The first method is associated with the individual’s narrative or self-identified handedness, e.g., “I’m right-handed/left-handed/mixed-handed” or “I use ambilateral hands”. Subjects may describe a preference of which hand they use for various manual activities (such as writing, hammering, throwing, sewing with a needle, slicing bread, etc.). The second method concerns the self-report of the hand preferred for manual actions by different questionnaires often used in (neuro)psychological research, such as: the Edinburgh Handedness Inventory [53,54,55], the Waterloo Handedness Questionnaire [56,57], the Annett Questionnaire [58,59,60], Home Handedness Questionnaire [61,62], or the Florkiewicz Colour-Cards Questionnaire [63]. The third method is derived from observation of the preferred use of hands in daily activities (e.g., self-grooming, gesturing) [64]. The fourth method estimates the differences between hands in actual skilled activities (e.g., speed and accuracy between hands, or coordination across muscles, fingers, and hands) by different functional tasks [65,66,67,68,69,70].
In this study, a multi-step model approach to the assessment of handedness based on all four methods was applied, as shown in Figure 2.
1.3. Aim of the Study
The aim of the presented research was to examine and compare test tasks performed with the right and left hand, independently. The study used a novel model approach to assess handedness that also estimated accurate the dominant and non-dominant hand recognition in real and virtual test tasks, as shown in Figure 2.
2. Subjects and Methods
2.1. Participants and Study Design
The study involved 20 healthy adults: 10 women and 10 men, aged 18–43 years (31.1 ± 7.7 yr), height 1.72 ± 0.08 m (1.55–1.84 m), weight 69.4 kg (51–89 kg), BMI 23.8 ± 3.6 kg/m2 (16.7–30.1 kg/m2). As shown in Figure 2, which presents the proposed model approach for assessing handedness, the dominant and non-dominant hand was determined for each person on basis, the first phase, of classical methods such as: (1) an interview about the handedness in live activity; (2) completed Florkiewicz’s questionnaire of functional lateralization, which is a test tool using the picture cards illustrate of various daily activities [63]; and (3) observed the simple physical trials similar to those presented in the test questionnaire. In the second phase of the examination, after an initial learning test training, the subjects practiced (4) real tests with Piórkowski’s apparatus (Figure 3), and then (5) virtual test tasks in virtual reality environment created by the NEUROFORMA computer system (Figure 4). The total duration of real and virtual test session was approximately one hour. All subjects were right-handed according to the classical assessment based on their self-narrative, the answers to the lateralization questionnaire, and effective use of the right hand in laboratory questionnaire tasks.
The study is statutory non-invasive model research with the participation of healthy volunteers and is carried out in cooperation with medical experts for the (tele)rehabilitation VR NEUROFORMA system. The project protocol of the statutory study was notified to the Bioethics Committee of the Medical University of Warsaw. All subjects gave their informed consent for inclusion before they participated in the research. The study was conducted in accordance with the Declaration of Helsinki.
2.2. Real Tests Using Piórkowski’s Apparatus
Piórkowski’s apparatus is a popular tool among occupational psychologists that enables the study of eye-hand coordination and the ability to concentrate attention, as well as allows to determine the precision of movements (manual dexterity) of the examined person under conditions of (imposed) strong time pressure [71]. The classic Piórkowski’s machine was used (Figure 3), consisting of: (a) Piórkowski’s console (green one in the foreground) and (b) a module device for controlling/programming tests (one in the background). The Piórkowski’s console has 10 large buttons arranged in a row at equal intervals (red buttons on the console in Figure 3). Above the row of these buttons is a set of LEDs, also arranged at equal intervals. The LEDs (in the form of arrows here) are used to indicate/signal the active button during the test. The operation of the device is very simple and intuitive. Three different frequencies of light stimuli were used: (a) 75 stimuli per minute (defined as the easy task level), (b) 107/min (as the medium task level), and (c) 125/min (as the difficult task). Participants performed the test session twice with Piórkowski’s console for these frequencies: a) the first with the right and left hand, and b) then with the left and right hand, independently. The percentage of correct reactions was calculated and analyzed.
2.3. Virtual Test Tasks
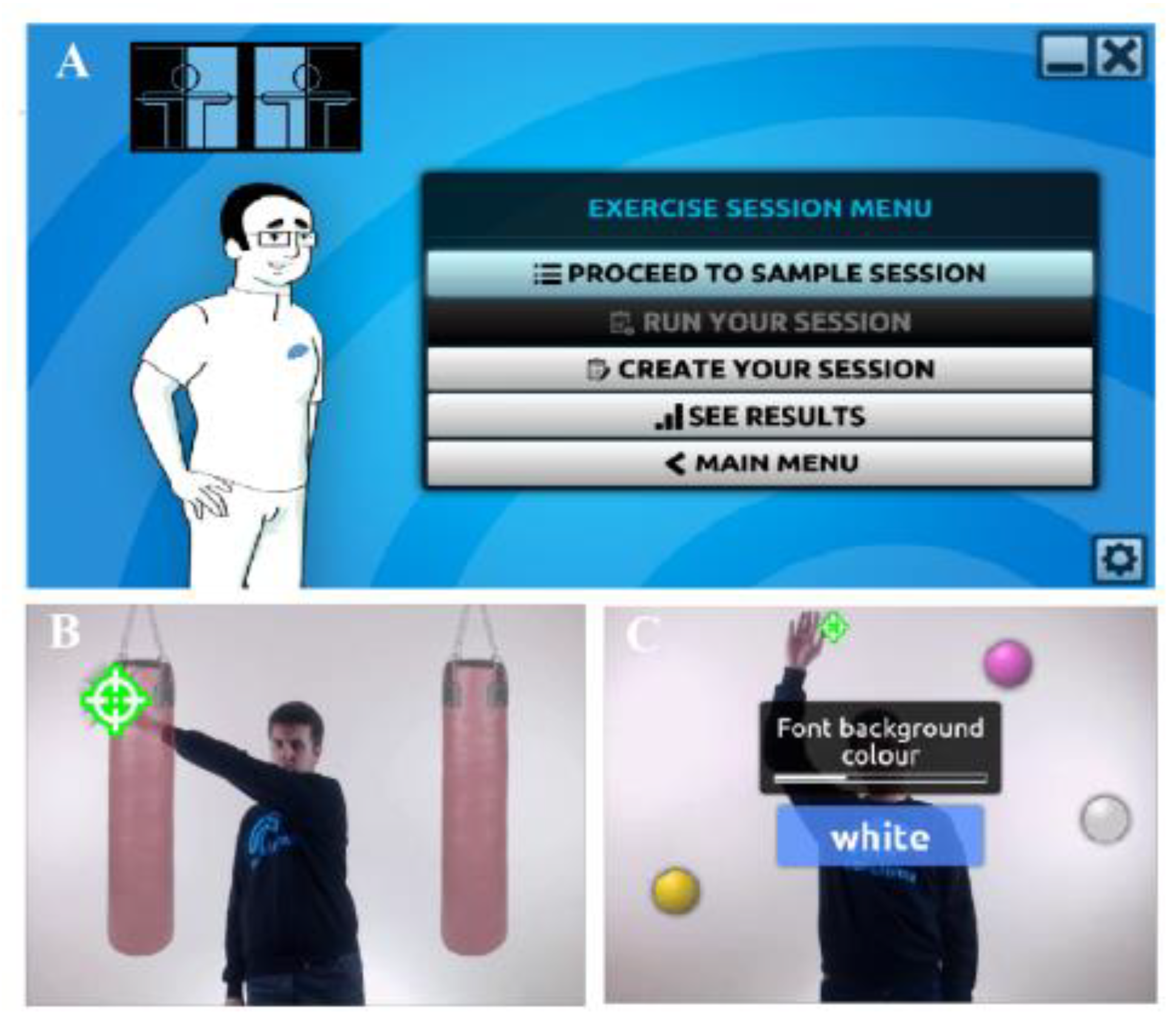
Virtual tests were conducted in the VR NEUROFORMA environment (Figure 4). The NEUROFORMA is an innovative computer stand for mobility and cognitive exercises [72,73]. It consists of a large display, a computerized data analysis system and an optical system for 3D motion analysis (Figure 4). During a virtual session, the participant stands in front of a screen showing his/her real, mirror image. Several virtual objects appear around the reflection. The main task is to move the body/part of one in such a way that the reflection displayed on the screen catches, hits or moves the appearing objects. The researcher can decide on the baseline complexity, the number of repetitions, and the range of motion by created the VR session (Figure 5A). If the exercise proves to be too easy or too difficult, it will be also modified by intelligent algorithms embedded into the system. Three difficult levels are defined: easy, medium and difficult. In the research, participants performed a test training program based on exercise such as a BOX and BALLS for two 1-min rounds at each level (Figure 5B,C). These exercises, similar to Piórkowski’s apparatus, allow for the assessment of motor skills, eye-hand-coordination and attention processes. The VR session was conducted twice, just like the real session with Piórkowski’s console, on three difficulty levels.
The BOX exercise (Figure 5B) required the opposing “punching” with the white markers (“sites”) that appeared on the “training bags” on right or left side of the screen (right hand-left bag and left hand-right bag). An additional requirement was to avoid random emerging black markers (distractors). The time of the white sites was displayed decreased as the difficulty level increased, and then it was necessary to hit faster. Additionally, black markers appeared directly beneath the white ones, so the hand was quickly withdrawn. The practitioner received a point for each white site hit and lost a point for hitting the black site. This exercise was easy to perform with both dominant and non-dominant hands and was willingly chosen by the subjects. In turn, in the group of cognitive exercises, especially those liked by practitioners, there were BALLS, in which colored balls had to be knocked down, according to the rules displayed in the frame on the screen (Figure 5C). At higher levels of difficulty, the time needed to complete this task was shorter and the number of balls increased. For each correctly thrown ball, the participant was awarded points.
2.4. Statistical Analysis
The analysis was performed using the statistical package of the STATISTICA 9.0 PL software (StatSoft Polska Ltd., Kraków, Poland). The normality of the distribution of variables was checked using the Shapiro–Wilk test. As the distributions were non-normal, the Friedman (ANOVA) test (p < 0.05) with Wilcoxon test as a post hoc test with Bonferroni correction was applied (p < 0.017 was considered statistically significant). The results of the dominant and non-dominant hand were compared for different difficult levels of real and virtual tasks. The data are presented as mean and standard deviation.
3. Results
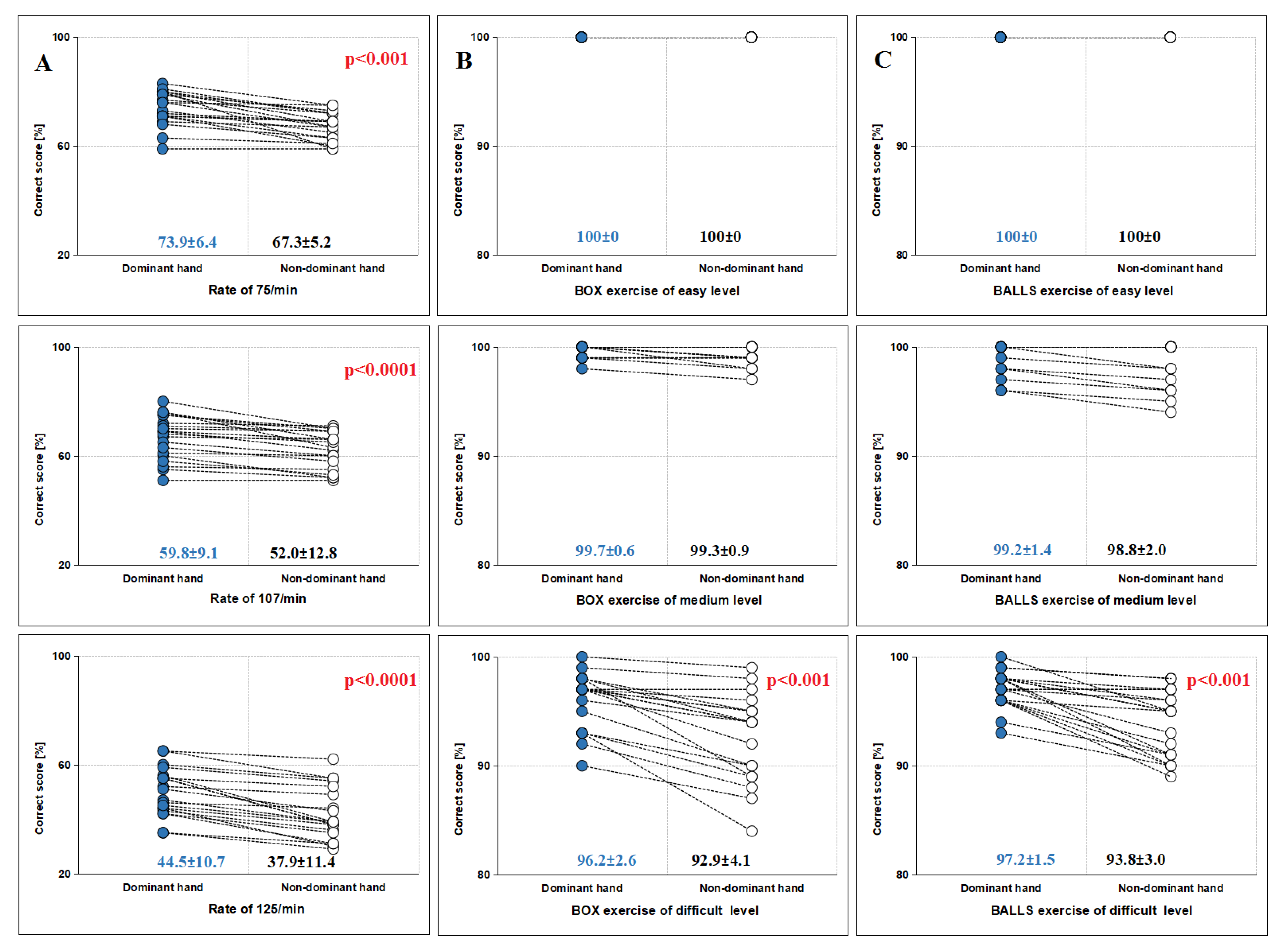
Figure 6 shows the results of assessed real tests using Piórkowski’s apparatus (panel A) and virtual test exercises of BOX and BALLS (panels B and C, respectively) at three levels of difficulty: easy, medium and difficult.
In the case of real tests with Piórkowski’s console, for each of rates of exposure to light stimuli: 75, 107 and 125 per minute, better results of correct performance for the dominant hand were observed (Figure 6A). However, the scores declined as the rate rose. Values for the dominant and non-dominant hand, for the frequency of 75/min, were 73.9 ± 6.4 vs. 67.3 ± 5.2 (p = 0.00013), slightly lower for f = 107/min, 59.8 ± 9.1 vs. 52.0 ± 12.8 (p = 0.0009), and the lowest was for f = 125/min, 44.5 ± 10.7 vs. 37.9 ± 11.4 (p = 0.0009).
As can be seen in Table 1, which illustrates the difference in scores between the dominant and non-dominant hand, the greatest difference occurs at the light stimulus rate f = 107/min, while for the other frequencies is slightly lower. This is due to the fact that a lower frequency is conducive to the correct performance of the test with both the dominant and non-dominant hand. On the other hand, with a faster (more difficult) stimulus, more errors are observed for the dominant and non-dominant hand, which in turn reduces the differences between them (also note that in this case both hands fatigue more quickly).
In the case of virtual test tasks, statistically significant differences between the dominant and non-dominant hand were observed only at the highest level of exercise difficulty, for BOX (Figure 6B) the scores were 96.2 ± 2.6 vs. 92.9 ± 4.1 (p = 0.00013), and for BALLS (Figure 6C) 97.2 ± 1.5 vs. 93.8 ± 3.0 (p = 0.00018). At the easy level of difficulty, healthy participants performed them excellently, i.e., without mistakes and achieved the maximum score of 100% (see Figure 6 and Table 1). A slight (but statistically insignificant) difference in the level of performing the virtual test with dominant and non-dominant hand was observed at the medium difficulty level, but it was only 0.4 ± 0.6 for the BOX and 0.5 ± 0.7 for the BALLS exercise. At the difficult level statistically significant differences of about 3% were observed. These virtual differences are about half lower than the real ones obtained for Piórkowski’s apparatus. It is worth noting that Piórkowski’s apparatus, as indicated earlier, is used to assess fatigue strength, hence lower results were achieved compared to virtual tasks. Tasks in the VR environment of NEUROFORMA are designed in such a way that only at high degree of difficulty they require significant effort in terms of motor skills and cognitive processes.
In turn, Table 2 shows the obtained results of other real tests from the previous clinical study [68], such as, for example, “Turning Balls” or “Twisting a Bracket” (Figure 7A,B, respectively). In the case of the clinical tests, the statistically significant differences between the right and left hand were also observed in right-handed healthy control group, i.e., in the moving balls test about 1.1 ± 0.9 sec (p = 0.000002) and in the buckle twist test about 1.0 ± 1.5 sec (p = 0.00014).
4. Discussion
It is worth noting that in an example similar to the Human Genome Project, the Human Brain Project was created to map the structure of the human brain in detail, and has contributed to rapid progress in neuroscience [75,76,77]. A recent interesting large-scale (1,766,671 participants) genome-wide association study (GWAS) revealed that 48 genetic variants are statistically associated with different forms of self-identified handedness (41 left-handed and 7 mixed) [78]. However, as Michel indicated in his review [40], GWAS does not identify genes that are commonly found associated with handedness in other primate species or across different phases of human development, and these studies do not identify deep handedness homology. In addition, the author pointed out that genetics might have some influence on the initiation of the developmental trajectory of handedness, slightly affecting the probability of one form over another. Currently, despite great hopes and expectations, genetics cannot yet explain the developmental emergence of handedness in any direct or informative manner [79,80]. Other studies demonstrate that older adults reveal a stronger laterality preference compared to younger adults [81,82,83], and also confirm that handedness develops—or, at least, become more stable—in the postnatal life, and remains consistent during adulthood [84,85]. Moreover, in the elderly, it was observed that the difference between the dominant and non-dominant hand changed and often decreased with age [86,87,88]. It is worth emphasizing that today also the mechanisms underlying these hemispheric differences in the structure and function are still unclear [33,89]. Note that despite the use of the most modern and innovative methods, approaches and technologies, interesting known and common biological phenomena such as structural/functional/behavioral asymmetries still require deeper knowledge, understanding and comprehensive multi-level research.
In the case assessment of handedness, research focuses primarily on the degree of hand preference and the difference in performance (e.g., strength, speed, precision) between the dominant and non-dominant hand [40,47,50]. Several tests are used to evaluate dexterity. The majority of these measures are based on self-narrative assessments or self-report questionnaires. In own study, the novel model approach of assessing handedness was applied (Figure 2), consistent with the conclusions of Michel [40]. In addition, the research compared the result of right- and left-hand tests in both the real and virtual environment, which were consistent with the classical questionnaire diagnosis of the participants’ dexterity, as well as correctly identified the domination of the body side in virtual tasks [90,91,92].
For example, in general, the same idea of real and VR recognition of the left and right body side is realized in clinical diagnosis/treatment/(neuro)rehabilitation of post-stroke patients with hemispatial neglect [93,94,95,96]. After a stroke, two basic categories of impairment or disability are identified, such as motor disability and cognitive impairments [97,98,99]. The most common cognitive impairment after a stroke, which occurs in ~50% of patients, is unilateral spatial neglect (USN). USN is a poor prognostic sign for both motor and cognitive effects of rehabilitation. The Buxbaum team [93] proposed a virtual reality lateralized attention test (VRLAT) test, which is a virtual diagnostic test. The researchers indicated that unilateral spatial neglect is often diagnosed by pencil-and-paper tasks (requiring the cancellation or intersection of lines or other stimuli), but this classic test may not be sensitive enough to detect subtle deficits. The VRLAT involves travelling (~90 min) along a virtual, non-branching path at six task levels, and participants are asked to identify virtual objects on both sides of the path and avoid collisions with them. The results of the study showed that the VRLAT, like clinical tests, can effectively measure the hemispatial neglect, and is even better at diagnosing USN than the classical approach. Ogourtsova and colleagues [95] also demonstrated the impact of virtual scene complexity in the assessment of post-stroke USN by proposed functional shopping activity in an ecological VR-based evaluation of neglect symptoms (EVENS) environment. EVENS is immersive and consists of simple and complex 3D scenes illustrating store shelves, where object recognition and navigation tasks are realized using a joystick. The authors showed that the proposed virtual EVENS tasks allow the detection of lateralized and non-lateralized deficits related to USN. They also noted, as did Buxbaum’s team, that USN is conventionally estimated with paper-and-pencil tests that lack ecological validity and are easily compensated for in chronic cases, and that virtual reality methods can overcome these limitations and effectively support the traditional approach. The Tae-Lim Kim group proposed another FOPR test using a virtual reality-based technique to assess field of perception (FOP) and field of regard (FOR) in hemispatial neglect [96]. The results confirm the conclusions about the good effectiveness and diagnostic accuracy of virtual methods compared to conventional tests. The FOPR test is conducted using a stereo HMD system and a 3D-dimensional development platform and takes approximately 10–20 min to accomplish.
An important issue is how to perform suitable extended reality sessions/programs without discomfort/negative influences (such as nausea, dizziness, disorientation, instability or fatigue, etc.), for example in education, scientific research or clinical practice. The appearance of any negative symptoms is a reason to stop being in the XR environment. Currently, there are still no standards for the use of innovative technologies in both life activities and clinical medicine. Hence the importance of research on healthy subjects and the inclusion of healthy controls in clinical trials with patients in a virtual environment. For example, Kourtesis and co-workers [100] proposed a test approach to validation using a tool such as Virtual Reality Neuroscience Questionnaire (VRNQ) to assess of VR software quality and user well-being. The study involved 40 healthy subjects (aged 28–43 years), 18 players and 22 non-players. Participants performed three different VR sessions until feeling tired or uncomfortable, and then completed the VRNQ. The authors suggested that the maximum duration of VR sessions should be in the range of 55–70 min when the VR software complies with the requirements of the proposed VRNQ and subjects are familiar with the tested VR system. Researchers also pointed out that the gaming experience did not appear to have an impact on how long VR tasks should last. Deeper immersion, better visual and audio quality, as well as prompts and helpful instructions have been found to reduce negative symptoms. In own study in the VR NEUROFORMA environment (similar to serious games): (a) the total duration of real and VR sessions was about an hour (after the initial learning with instructions of the system assistant, Figure 5); (b) VR tasks (including both motor and mental functions) are attractive and emotionally engaging; and (c) the scoring system with biofeedback monitoring is motivated and helps participants complete the test tasks correctly. None of the participants experienced any negative symptoms and all reported that the test sessions were interesting and doable.
Overall, our own studies and those of other researchers/clinicians who have used innovative virtual technology demonstrate the effectiveness of the VR approach for the quantitative estimation of asymmetry of motor skills and cognitive processes. Notice that this is important because the new technologies are very promised effective tools for diagnosis, therapy and (neuro)rehabilitation in modern medical practice. Consequently, it is observed that IT systems are already the novel face of 21st century neuroscience and biomedicine.
5. Concluding Remarks and Perspectives
Studies of human functional asymmetries using novel approaches and technologies still require intensive research into their beneficial effects on human life, both in terms of health (e.g., entertainment, marketing, military, sport, education, (neuro)science) and in disease (e.g., neurological, balance or gait disturbances/disorders). Of particular importance are studies involving healthy people, which allow one to assess the potential possibilities and unfavorable limitations, including natural biological barriers (such as fatigue, inability to perform a “computer” task by a biological being, e.g., a human). The presented research proposes a new model analytical approach to functional lateralization, but the limitation is, of course, the small number of subjects, although the obtained results demonstrate the high effectiveness of the methods used. Future research perspectives relate to research in various groups, both among healthy subjects and patients, incl. according to the classification of handedness (right-handed, left-handed, and other dexterity models), age (e.g., children, adults, elderly), the impact of treatment/rehabilitation, preparation of application standards and comparison of results/effects for classic and virtual methods/programs/technologies used, for example, in education, neuroscience, healthcare or clinical practice.
Notice that the novel technologies of the 21st century are very attractive, arouse natural curiosity, willingness to engage and evoke strong emotions in subjects participating in the new virtual world, created and offered by innovative IT systems. These systems are subject to rapid changes and continuous development in all fields of human activity. The future of XR research and potential applications seems very promising.
Funding
The research received no external funding.
Acknowledgments
The author would like to thank Andrzej Ziemba and Tomasz Mikulski for enabling the test on the APK device with Piórkowski console. The research used the NEUROFORMA platform by the Titanis Ltd. The author would like to specially thank Emeritus Bogdan Lesyng, Ewa Sokołowska and Teresa Sadura-Sieklucka for the inspiration in conducting this research.
Conflicts of Interest
The author declares no conflict of interest.
References
- Tripathy, B.K.; Anuradha, J. Internet of Things (IoT): Technologies, Applications, Challenges, and Solutions; Taylor & Francis Group; CRP Press: Boca Raton, FL, USA, 2018. [Google Scholar]
- Blas, S.S.H.; Sales Mendes, A.; García Encinas, F.; Silva, L.A.; González, G.V. A Multi-Agent System for Data Fusion Techniques Applied to the Internet of Things Enabling Physical Rehabilitation Monitoring. Appl. Sci. 2021, 11, 331. [Google Scholar] [CrossRef]
- Crawford, S.B.; Baily, L.W.; Monks, S.M. (Eds.) Comprehensive Healthcare Simulation: Operations, Technology, and Innovative Practice; Springer International Publishing: Cham, Switzerland, 2019. [Google Scholar] [CrossRef]
- Siani, A.; Marley, S.A. Impact of the recreational use of virtual reality on physical and mental wellbeing during the COVID-19 lockdown. Health Technol. 2021, 11, 425–435. [Google Scholar] [CrossRef] [PubMed]
- Grant, C.; Mairn, C. 3D, virtual, augmented, extended, mixed reality, and extended content forms: The technology and the challenges. Inf. Serv. Use 2020, 40, 225–230. [Google Scholar] [CrossRef]
- Amuso, V.; Poletti, G.; Montibello, D. Virtual, Augmented and Mixed Reality: What are the Benefits for SMEs? Global Policy 2021, 12, 167–170. [Google Scholar] [CrossRef]
- Milgram, P.; Takemura, H.; Utsumi, A.; Kishino, F. Augmented Reality: A class of displays on the reality-virtuality continuum. In Telemanipulator and Telepresence Technologies; SPIE: Bellingham, WA, USA, 1994; Volume 2351, pp. 282–292. [Google Scholar] [CrossRef]
- Flavián, C.; Ibáñez-Sánchez, S.; Orús, C. The impact of virtual, augmented and mixed reality technologies on the customer experience. J. Bus. Res. 2019, 100, 547–560. [Google Scholar] [CrossRef]
- Patel, S.; Panchotiya, B.; Ribadiya, S.A. Survey: Virtual, Augmented and Mixed Reality in Education. IJERT 2020, 9, 1067–1072. [Google Scholar] [CrossRef]
- Skarbez, R.; Smith, M.; Whitton, M.C. Revisiting Milgram and Kishino’s Reality-Virtuality Continuum. Front. Virtual Real. 2021, 2, 647997. [Google Scholar] [CrossRef]
- Torner, J.; Skouras, S.; Molinuevo, J.L.; Gispert, J.D.; Alpiste, F. Multipurpose virtual reality environment for biomedical and health applications. IEEE Trans. Neural Syst. Rehabil. Eng. 2019, 27, 1511–1520. [Google Scholar] [CrossRef]
- Zając-Lamparska, L.; Wiłkość-Dębczyńska, M.; Wojciechowski, A.; Podhorecka, M.; Polak-Szabela, A.; Warchoł, Ł.; Kędziora-Kornatowska, K.; Araszkiewicz, A.; Izdebski, P. Effects of virtual reality-based cognitive training in older adults living without and with mild dementia: A pretest-posttest design pilot study. BMC Res. Notes 2019, 12, 776. [Google Scholar] [CrossRef]
- Singh, R.P.; Javaid, M.; Kataria, R.; Tyagi, M.; Haleem, A.; Suman, R. Significant applications of virtual reality for COVID-19 pandemic. Diabetes Metab. Syndr. 2020, 14, 661–664. [Google Scholar] [CrossRef] [PubMed]
- Abich, J.; Parker, J.; Murphy, J.S.; Eudy, M. A review of the evidence for training effectiveness with virtual reality technology. Virtual Real. 2021. [Google Scholar] [CrossRef]
- Eshuis, L.V.; van Gelderen, M.J.; van Zuiden, M.; Nijdam, M.J.; Vermetten, E.; Olff, M.; Bakker, A. Efficacy of immersive PTSD treatments: A systematic review of virtual and augmented reality exposure therapy and a meta-analysis of virtual reality exposure therapy. J. Psychiatr. Res. 2020. [Google Scholar] [CrossRef] [PubMed]
- Iwanaga, J.; Kamura, Y.; Nishimura, Y.; Terada, S.; Kishimoto, N.; Tanaka, T.; Tubbs, R.S. A new option for education during surgical procedures and related clinical anatomy in a virtual reality workspace. Clin. Anat. 2021, 34, 496–503. [Google Scholar] [CrossRef] [PubMed]
- Sherman, W.; Craig, A. Understanding Virtual Reality. Interface, Application, and Design, 2nd ed.; Elsevier Ltd.: Oxford, MS, USA, 2018. [Google Scholar] [CrossRef]
- Tom Dieck, M.C.; Jung, T. (Eds.) Augmented Reality and Virtual Reality. The Power of AR and VR for Business; Springer Nature: Cham, Switzerland, 2019. [Google Scholar] [CrossRef]
- Isernia, S.; Di Tella, S.; Pagliari, C.; Jonsdottir, J.; Castiglioni, C.; Gindri, P.; Salza, M.; Gramigna, C.; Palumbo, G.; Molteni, F.; et al. Effects of an Innovative Telerehabilitation Intervention for People with Parkinson’s Disease on Quality of Life, Motor, and Non-motor Abilities. Front. Neurol. 2020, 11, 846. [Google Scholar] [CrossRef] [PubMed]
- Cai, Y.; van Joolingen, W.; Veermans, K. (Eds.) Virtual and Augmented Reality, Simulation and Serious Games for Education; Springer: Singapore, 2021. [Google Scholar] [CrossRef]
- Cerritelli, F.; Chiera, M.; Abbro, M.; Megale, V.; Esteves, J.; Gallace, A.; Manzotti, A. The Challenges and Perspectives of the Integration Between Virtual and Augmented Reality and Manual Therapies. Front. Neurol. 2021, 12, 700211. [Google Scholar] [CrossRef] [PubMed]
- Giglioli, I.A.C.; Carrasco-Ribelles, L.A.; Parra, E.; Marín-Morales, J.; Alcañiz Raya, M. An Immersive Serious Game for the Behavioral Assessment of Psychological Needs. Appl. Sci. 2021, 11, 1971. [Google Scholar] [CrossRef]
- Hoffman, H.G. Interacting with virtual objects via embodied avatar hands reduces pain intensity and diverts attention. Sci. Rep. 2021, 11, 10672. [Google Scholar] [CrossRef]
- Trost, Z.; France, C.; Anam, M.; Shum, C. Virtual reality approaches to pain: Toward a state of the science. Pain 2021, 162, 325–331. [Google Scholar] [CrossRef]
- Chang, E.; Kim, H.T.; Yoo, B. Virtual reality sickness: A review of causes and measurements. Int. J. Hum. Comput. Int. 2020, 36, 1658–1682. [Google Scholar] [CrossRef]
- Martirosov, S.; Bureš, M.; Zítka, T. Cyber sickness in low-immersive, semi-immersive, and fully immersive virtual reality. Virtual Real. 2021, 1–18. [Google Scholar] [CrossRef]
- Rogers, L.J. Brain Asymmetry of Structure and/or Function. In Symmetry; MDPI: Basel, Switzerland, 2017. [Google Scholar] [CrossRef] [Green Version]
- Rogers, L.J. Left Versus Right Asymmetries of Brain and Behaviour. In Symmetry; MDPI: Basel, Switzerland, 2019. [Google Scholar] [CrossRef] [Green Version]
- Güntürkün, O.; Ströckens, F.; Ocklenburg, S. Brain Lateralization: A Comparative Perspective. Physiol. Rev. 2020, 100, 1019–1063. [Google Scholar] [CrossRef]
- Esteves, M.; Ganz, E.; Sousa, N.; Leite-Almeida, H. Asymmetrical Brain Plasticity: Physiology and Pathology. Neuroscience 2021, 454, 3–14. [Google Scholar] [CrossRef]
- Frasnelli, E. Looking at lateralization as a dynamic and plastic feature of nervous systems. Laterality 2021, 26, 323–326. [Google Scholar] [CrossRef]
- Palomero-Gallagher, N.; Amunts, K. A short review on emotion processing: A lateralized network of neuronal networks. Brain Struct. Funct. 2021. [Google Scholar] [CrossRef] [PubMed]
- Sha, Z.; Schijven, D.; Carrion-Castillo, A.; Joliot, M.; Mazoyer, B.; Fisher, S.E.; Crivello, F.; Francks, C. The genetic architecture of structural left-right asymmetry of the human brain. Nat. Hum. Behav. 2021. [Google Scholar] [CrossRef] [PubMed]
- Costanzo, E.Y.; Villarreal, M.; Drucaroff, L.J.; Ortiz-Villafañe, M.; Castro, M.N.; Goldschmidt, M.; Wainsztein, A.E.; Ladrón-de-Guevara, M.S.; Romero, C.; Brusco, L.I.; et al. Hemispheric specialization in affective responses, cerebral dominance for language, and handedness: Lateralization of emotion, language, and dexterity. Behav. Brain Res. 2015, 288, 11–19. [Google Scholar] [CrossRef] [PubMed]
- Volz, L.J.; Gazzaniga, M.S. Interaction in isolation: 50 years of insights from split-brain research. Brain 2017, 140, 2051–2060. [Google Scholar] [CrossRef] [PubMed]
- Bishop, C.; Turner, A.; Read, P. Effects of inter-limb asymmetries on physical and sports performance: A systematic review. J. Sports Sci. 2018, 36, 1135–1144. [Google Scholar] [CrossRef]
- De Haan, E.H.F.; Corballis, P.M.; Hillyard, S.A.; Marzi, C.A.; Seth, A.; Lamme, V.A.F.; Volz, L.; Fabri, M.; Schechter, E.; Bayne, T.; et al. Split-Brain: What We Know Now and Why This is Important for Understanding Consciousness. Neuropsychol. Rev. 2020, 30, 224–233. [Google Scholar] [CrossRef]
- Marcori, A.J.; Okazaki, V.H.A. A historical, systematic review of handedness origins. Laterality 2020, 25, 87–108. [Google Scholar] [CrossRef]
- Papadatou-Pastou, M.; Ntolka, E.; Schmitz, J.; Martin, M.; Munafò, M.R.; Ocklenburg, S.; Paracchini, S. Human handedness: A meta-analysis. Psychol. Bull. 2020, 146, 481–524. [Google Scholar] [CrossRef]
- Michel, G.F. Handedness Development: A Model for Investigating the Development of Hemispheric Specialization and Interhemispheric Coordination. Symmetry 2021, 13, 992. [Google Scholar] [CrossRef]
- Corbetta, D.; Williams, J.; Snapp-Childs, W. Plasticity in the development of handedness: Evidence from normal development and early asymmetric brain injury. Dev. Psychobiol. 2006, 48, 460–471. [Google Scholar] [CrossRef] [PubMed]
- Muraleedharan, A.; Ragavan, S.; Devi, R. Are Footedness and Lateral Postures Better Predictors of Hemispheric Dominance Than Handedness: A Cross-sectional Questionnaire-Based Clinical and Pedigree Study. J. Neurosci. Rural. Pract. 2020, 11, 130–134. [Google Scholar] [CrossRef] [Green Version]
- Duboc, V.; Dufourcq, P.; Blader, P.; Roussigné, M. Asymmetry of the Brain: Development and Implications. Annu. Rev. Genet. 2015, 49, 647–672. [Google Scholar] [CrossRef] [PubMed]
- Derakhshan, I. Lateralities of motor control and the alien hand always coincide: Further observations on directionality in callosal traffic underpinning handedness. Neurol. Res. 2009, 31, 258–264. [Google Scholar] [CrossRef] [PubMed]
- Coddard Blythe, S. (Ed.) Attention, Balance and Coordination: The A.B.C. of Learning Success; John Wiley & Sons: Hoboken, NJ, USA, 2017; ISBN 978-1-119-16476-0. [Google Scholar]
- Utesch, T.; Mentzel, S.V.; Strauss, B.; Büsch, D. Chapter 4—Measurement of Laterality and Its Relevance for Sports. In Laterality in Sports. Theories and Applications, 1st ed.; Loffing, F., Hagemann, N., Strauss, B., MacMahon, C., Eds.; Elsevier Academic Press: Cambridge, MA, USA, 2016; pp. 65–86. [Google Scholar] [CrossRef]
- Yang, L.Z.; Zhang, W.; Wang, W.; Yang, Z.; Wang, H.; Deng, Z.D.; Li, C.; Qiu, B.; Zhang, D.R.; Kadosh, R.C.; et al. Neural and Psychological Predictors of Cognitive Enhancement and Impairment from Neurostimulation. Adv. Sci. 2020, 7, 1902863. [Google Scholar] [CrossRef]
- Ruck, L.; Schoenemann, P.T. Handedness measures for the Human Connectome Project: Implications for data analysis. Laterality 2021, 26, 584–606. [Google Scholar] [CrossRef]
- Buchmann, I.; Randerath, J. Selection and application of familiar and novel tools in patients with left and right hemispheric stroke: Psychometrics and normative data. Cortex 2017, 94, 49–62. [Google Scholar] [CrossRef]
- Paquet, A.; Golse, B.; Girard, M.; Olliac, B.; Vaivre-Douret, L. Laterality and Lateralization in Autism Spectrum Disorder, Using a Standardized Neuro-Psychomotor Assessment. Dev. Neuropsychol. 2017, 42, 39–54. [Google Scholar] [CrossRef]
- Bryden, P.J.; Pryde, K.M.; Roy, E.A. A performance measure of the degree of hand preference. Brain Cogn. 2000, 44, 402–414. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brown, S.G.; Roy, E.A.; Rohr, L.E.; Snider, B.R.; Bryden, P.J. Preference and performance measures of handedness. Brain Cogn. 2004, 55, 283–285. [Google Scholar] [CrossRef]
- Oldfield, R.C. The assessment and analysis of handedness: The Edinburgh inventory. Neuropsychologia 1971, 9, 97–113. [Google Scholar] [CrossRef]
- Oldfield Handedness Questionnaire. Available online: https://www.brainmapping.org/shared/Edinburgh.php (accessed on 5 September 2021).
- Veale, J.F. Edinburgh Handedness Inventory—Short Form: A revised version based on confirmatory factor analysis. Laterality 2014, 19, 164–177. [Google Scholar] [CrossRef]
- Bryden, M. Measuring handedness with questionnaires. Neuropsychologia 1977, 15, 617–624. [Google Scholar] [CrossRef]
- Williams, N.; Scharoun Benson, S.M.; Bryden, P.J. Investigating the Efficacy of the Hand Selection Complexity Task Across the Lifespan. Front. Psychol. 2019, 10, 1130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Annett, M. A classification of hand preference by association analysis. Br. J. Psychol. 1970, 61, 303–321. [Google Scholar] [CrossRef] [PubMed]
- Annett, M. Patterns of hand preference for pairs of actions and the classification of handedness. Br. J. Psychol. 2009, 100, 491–500. [Google Scholar] [CrossRef] [Green Version]
- Beaton, A.A.; Corballis, M.; McManus, C. Obituary for Dr. Marian Annett, 1931–2018. Laterality 2020, 5, 405–412. [Google Scholar] [CrossRef]
- Nelson, E.L.; Gonzalez, S.L.; El-Asmar, J.M.; Ziade, M.F.; Abu-Rustum, R.S. The home handedness questionnaire: Pilot data from preschoolers. Laterality 2019, 24, 482–503. [Google Scholar] [CrossRef]
- Gonzalez, S.L.; Nelson, E.L. Factor analysis of the Home Handedness Questionnaire: Unimanual and role differentiated bimanual manipulation as separate dimensions of handedness. Appl. Neuropsychol. Adult 2021, 28, 173–184. [Google Scholar] [CrossRef] [PubMed]
- Florkiewicz, V. My Profile of Domination—The Illustrated Test to Investigation of Lateralization at Children and Adult; Harmonia Publisher: Gdańsk, Poland, 2016. (In Polish) [Google Scholar]
- Bryden, P.J.; Roy, E.A.; Spence, J. An observational method of assessing handedness in children and adults. Dev. Neuropsychol. 2007, 32, 825–846. [Google Scholar] [CrossRef] [PubMed]
- Incel, N.A.; Sezgin, M.; As, I.; Cimen, O.B.; Sahin, G. The geriatric hand: Correlation of hand-muscle function and activity restriction in elderly. Int. J. Rehabil. Res. 2009, 32, 213–218. [Google Scholar] [CrossRef] [PubMed]
- Księżopolska-Orłowska, K.; Sadura-Sieklucka, T.; Kasprzak, K.; Gaszewska, E.; Rodkiewicz-Bogusławska, A.; Sokołowska, B. The beneficial effects of rehabilitation on hand function in patients with rheumatoid arthritis. Reumatologia 2016, 54, 285–290. [Google Scholar] [CrossRef] [PubMed]
- McManus, I.C.; Van Horn, J.D.; Bryden, P.J. The Tapley and Bryden test of performance differences between the hands: The original data, newer data, and the relation to pegboard and other tasks. Laterality 2016, 21, 371–396. [Google Scholar] [CrossRef] [Green Version]
- Sadura-Sieklucka, T.; Sokołowska, B.; Prusinowska, A.; Trzaska, A.; Księżopolska-Orłowska, K. Benefits of wrist splinting in patients with rheumatoid arthritis. Reumatologia 2018, 56, 362–367. [Google Scholar] [CrossRef]
- El-Gohary, T.M.; Abd Elkader, S.M.; Al-Shenqiti, A.M.; Ibrahim, M.I. Assessment of hand-grip and key-pinch strength at three arm positions among healthy college students: Dominant versus non-dominant hand. J. Taibah. Univ. Med. Sci. 2019, 14, 566–571. [Google Scholar] [CrossRef]
- Olczak, A.; Truszczyńska-Baszak, A. Influence of the Passive Stabilization of the Trunk and Upper Limb on Selected Parameters of the Hand Motor Coordination, Grip Strength and Muscle Tension, in Post-Stroke Patients. J. Clin. Med. 2021, 10, 2402. [Google Scholar] [CrossRef]
- Chruzik, K.; Korchut, A. A new method of psychotechnical testing of transport operators. MATEC Web Conf. 2018, 231, 1–8. [Google Scholar] [CrossRef]
- Neuroforma System. Available online: https://www.neuro-forma.com/ (accessed on 5 September 2021).
- Pawlowski, M. Neuroforma—Innovative Solution for Neurorehabilitation. J. Alzheimers Dement. 2019, 2. Available online: https://www.imedpub.com/abstract/neuroforma--innovative-solution-for-neurorehabilitation-28329.html (accessed on 5 September 2021).
- Sokołowska, B.; Sadura-Sieklucka, T.; Sokołowska, E. Examples of examination and assessment of the dominant and non-dominant hand function in health and disease conditions. In Problems in the Field of Medicine and Related Sciences—Review and Research; Maciąg, M., Danielewska, A., Eds.; TYGIEL Scientific Publisher: Lublin, Poland, 2019; Volume 1, pp. 228–248. Available online: http://bc.wydawnictwo-tygiel.pl/publikacja/2ECFE981-664B-C8BA-B77E-EF0346FFFE68 (accessed on 5 September 2021). (In Polish)
- HBP. Available online: https://www.humanbrainproject.eu/ (accessed on 5 September 2021).
- Amunts, K.; Knoll, A.C.; Lippert, T.; Pennartz, C.M.A.; Ryvlin, P.; Destexhe, A.; Jirsa, V.K.; D’Angelo, E.; Bjaalie, J.G. The Human Brain Project-Synergy between neuroscience, computing, informatics, and brain-inspired technologies. PLoS Biol. 2019, 17, e3000344. [Google Scholar] [CrossRef]
- Kong, X.Z.; Postema, M.C.; Guadalupe, T.; de Kovel, C.; Boedhoe, P.S.W.; Hoogman, M.; Mathias, S.R.; van Rooij, D.; Schijven, D.; Glahn, D.C.; et al. Mapping brain asymmetry in health and disease through the ENIGMA consortium. Hum. Brain Mapp. 2020. [Google Scholar] [CrossRef] [PubMed]
- Cuellar-Partida, G.; Tung, J.Y.; Eriksson, N.; Albrecht, E.; Aliev, F.; Andreassen, O.A.; Barroso, I.; Beckmann, J.S.; Boks, M.P.; Boomsma, D.I.; et al. Genome-wide association study identifies 48 common genetic variants associated with handedness. Nat. Hum. Behav. 2021, 5, 59–70. [Google Scholar] [CrossRef] [PubMed]
- Brandler, W.M.; Paracchini, S. The genetic relationship between handedness and neurodevelopmental disorders. Trends Mol. Med. 2014, 20, 83–90. [Google Scholar] [CrossRef] [Green Version]
- Schmitz, J.; Metz, G.A.S.; Güntürkün, O.; Ocklenburg, S. Beyond the genome-Towards an epigenetic understanding of handedness ontogenesis. Prog. Neurobiol. 2017, 159, 69–89. [Google Scholar] [CrossRef] [PubMed]
- Marcori, A.J.; Grosso, N.D.S.; Porto, A.B.; Okazaki, V.H.A. Beyond handedness: Assessing younger adults and older people lateral preference in six laterality dimensions. Laterality 2019, 24, 163–175. [Google Scholar] [CrossRef]
- Hill, C.; Van Gemmert, A.W.A.; Fang, Q.; Hou, L.; Wang, J.; Pan, Z. Asymmetry in the aging brain: A narrative review of cortical activation patterns and implications for motor function. Laterality 2020, 25, 413–429. [Google Scholar] [CrossRef]
- Woytowicz, E.J.; Sainburg, R.L.; Westlake, K.P.; Whitall, J. Competition for limited neural resources in older adults leads to greater asymmetry of bilateral movements than in young adults. J. Neurophysiol. 2020, 123, 1295–1304. [Google Scholar] [CrossRef]
- Carmeli, E.; Patish, H.; Coleman, R. The aging hand. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2003, 58, 146–152. [Google Scholar] [CrossRef] [Green Version]
- Park, J.; Pažin, N.; Friedman, J.; Zatsiorsky, V.M.; Latash, M.L. Mechanical properties of the human hand digits: Age-related differences. Clin. Biomech. 2014, 29, 129–137. [Google Scholar] [CrossRef] [Green Version]
- Dolcos, F.; Rice, H.J.; Cabeza, R. Hemispheric asymmetry and aging: Right hemisphere decline or asymmetry reduction. Neurosci. Biobehav. Rev. 2002, 26, 819–825. [Google Scholar] [CrossRef]
- Wang, J.; D’Amato, A.; Bambrough, J.; Swartz, A.M.; Miller, N.E. A positive association between active lifestyle and hemispheric lateralization for motor control and learning in older adults. Behav. Brain Res. 2016, 314, 38–44. [Google Scholar] [CrossRef]
- Sebastjan, A.; Skrzek, A.; Ignasiak, Z.; Sławińska, T. Age-related changes in hand dominance and functional asymmetry in older adults. PLoS ONE 2017, 12, e0177845. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jasper, J.D.; Christman, S.D.; Clarkson, E. Predicting interactions in handedness research: The role of integrated versus independent dual-processes. Laterality 2021, 15, 1–17. [Google Scholar] [CrossRef]
- Sokołowska, B.; Sokołowska, E. An Example of the Assessment of Human Laterality Using Virtual Reality. IJIRCCE 2019, 7, 3555–3562. Available online: http://ijircce.com/admin/main/storage/app/pdf/KdxZlKhLTCPJ5Fekz5R9wfuhT7qtfDYfS9dn2Atb.pdf (accessed on 5 September 2021). [CrossRef]
- Sokołowska, B.; Sokołowska, E. Machine Learning algorithms to study of laterality in Virtual Reality. Neuroinformatics 2019. [Google Scholar] [CrossRef]
- Sokołowska, B. A novel virtual reality approach for functional lateralization in healthy adults. Brain Res. 2021, 1766, 147537. [Google Scholar] [CrossRef] [PubMed]
- Buxbaum, L.J.; Dawson, A.M.; Linsley, D. Reliability and validity of the Virtual Reality Lateralized Attention Test in assessing hemispatial neglect in right-hemisphere stroke. Neuropsychology 2012, 26, 430–441. [Google Scholar] [CrossRef]
- Pedroli, E.; Serino, S.; Cipresso, P.; Pallavicini, F.; Riva, G. Assessment and rehabilitation of neglect using virtual reality: A systematic review. Front. Behav. Neurosci. 2015, 9, 226. [Google Scholar] [CrossRef] [Green Version]
- Ogourtsova, T.; Archambault, P.; Sangani, S.; Lamontagne, A. Ecological Virtual Reality Evaluation of Neglect Symptoms (EVENS): Effects of Virtual Scene Complexity in the Assessment of Poststroke Unilateral Spatial Neglect. Neurorehabil. Neural. Repair. 2018, 32, 46–61. [Google Scholar] [CrossRef] [Green Version]
- Kim, T.L.; Kim, K.; Choi, C.; Lee, J.Y.; Shin, J.H. FOPR test: A virtual reality-based technique to assess field of perception and field of regard in hemispatial neglect. J. Neuroeng. Rehabil. 2021, 18, 39. [Google Scholar] [CrossRef] [PubMed]
- Hillis, A.E. Neurobiology of unilateral spatial neglect. Neuroscientist 2006, 12, 153–163. [Google Scholar] [CrossRef]
- Rode, G.; Fourtassi, M.; Pagliari, C.; Pisella, L.; Rossetti, Y. Complexity vs. unity in unilateral spatial neglect. Rev. Neurol. 2017, 173, 440–450. [Google Scholar] [CrossRef] [PubMed]
- Gammeri, R.; Iacono, C.; Ricci, R.; Salatino, A. Unilateral Spatial Neglect After Stroke: Current Insights. Neuropsychiatr. Dis. Treat. 2020, 16, 131–152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kourtesis, P.; Collina, S.; Doumas, L.A.A.; MacPherson, S.E. Validation of the Virtual Reality Neuroscience Questionnaire: Maximum Duration of Immersive Virtual Reality Sessions Without the Presence of Pertinent Adverse Symptomatology. Front. Hum. Neurosci. 2019, 13, 417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
Figure 1.
The illustration of the classification of extended reality technologies.

Figure 2.
The diagram of the model approach used in own study, consisting of the following steps: (1) the self-identified of handedness by participants; (2) the report in the form of a completed the functional lateralization questionnaire; (3) the observing the hand preferences of subjects in real manual action (to verify of step 2); and finally (4) the realization of real and virtual test tasks (after the initial learning phase).
Figure 2.
The diagram of the model approach used in own study, consisting of the following steps: (1) the self-identified of handedness by participants; (2) the report in the form of a completed the functional lateralization questionnaire; (3) the observing the hand preferences of subjects in real manual action (to verify of step 2); and finally (4) the realization of real and virtual test tasks (after the initial learning phase).

Figure 3.
The view of Piórkowski’s apparatus (APK 2/04 by UNI-PAR, Szczecin, Poland used in the real part of the research session (material from the lab repository).
Figure 3.
The view of Piórkowski’s apparatus (APK 2/04 by UNI-PAR, Szczecin, Poland used in the real part of the research session (material from the lab repository).

Figure 4.
The view of the VR NEUROFORMA system in our laboratory (material from the lab repository).
Figure 4.
The view of the VR NEUROFORMA system in our laboratory (material from the lab repository).

Figure 5.
The view of (A) the exercise session menu and virtual exercises such as (B) the BOX and (C) the BALLS in the VR NEUROFORMA environment (with the permission of Titanis Ltd., Warsaw, Poland).
Figure 5.
The view of (A) the exercise session menu and virtual exercises such as (B) the BOX and (C) the BALLS in the VR NEUROFORMA environment (with the permission of Titanis Ltd., Warsaw, Poland).

Figure 6.
Results of the research session for the dominant and non-dominant hand in: (A) real tests with Piórkowski’s console for three different frequencies of light stimuli: 75/min (easy level), 107/min (medium level) and 125/min (difficult level); (B) virtual BOX exercises at easy, medium and difficult level; (C) virtual BALL exercises at these levels. Scores of individual participants and the mean with standard deviation are given.
Figure 6.
Results of the research session for the dominant and non-dominant hand in: (A) real tests with Piórkowski’s console for three different frequencies of light stimuli: 75/min (easy level), 107/min (medium level) and 125/min (difficult level); (B) virtual BOX exercises at easy, medium and difficult level; (C) virtual BALL exercises at these levels. Scores of individual participants and the mean with standard deviation are given.

Figure 7.
The illustration of selected real clinical tests: (A) “Turning Balls-Moving small balls from place to place”; and (B) “Twisting a Bracket-Locking turns (these and other tests are described in e.g., [66,68,74].


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Differences of scores between the dominant and non-dominant hand.
| Test Tasks | Score Differences between the Dominant and Non-Dominant Hand [%] | ||
|---|---|---|---|
| Easy Level | Medium Level | Difficult Level | |
| Real BUTTONS | 6.6 ± 5.1 ** | 7.9 ± 7.4 *** | 6.5 ± 4.9 *** |
| Virtual BOX | 0.0 ± 0.0 | 0.4 ± 0.6 | 3.3 ± 2.4 ** |
| Virtual BALLS | 0.0 ± 0.0 | 0.5 ± 0.7 | 3.4 + 2.5 ** |
** p < 0.001, *** p < 0.0001 for comparisons between the right (dominant) and left (non-dominant) hand.
Table 2.
The example of results of the right and left hand in the healthy right-handed control group (n = 40) according to the clinical study using real clinical tests (data and analysis based on [68]).
Table 2.
The example of results of the right and left hand in the healthy right-handed control group (n = 40) according to the clinical study using real clinical tests (data and analysis based on [68]).
| Examples of Real Clinical Test Tasks | Duration of the Performed Test [Seconds] | ||
|---|---|---|---|
| Right (Dominat) Hand | Left (Non-Dominat) Hand | Difference | |
| Moving small balls from place to place | 21.3 ± 3.7 | 20.2 ± 3.4 | 1.1 ± 0.9 *** |
| Locking turns | 13.3 ± 3.4 | 12.3 ± 2.9 | 1.0 ± 1.5 *** |
*** p < 0.0001 for comparisons between the right and left hand.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Sokołowska, B. A Novel Perspective for Examining and Comparing Real and Virtual Test Tasks Performed by the Dominant and Non-Dominant Hand in Healthy Adults. Symmetry 2021, 13, 1810. https://doi.org/10.3390/sym13101810
AMA Style
Sokołowska B. A Novel Perspective for Examining and Comparing Real and Virtual Test Tasks Performed by the Dominant and Non-Dominant Hand in Healthy Adults. Symmetry. 2021; 13(10):1810. https://doi.org/10.3390/sym13101810
Chicago/Turabian StyleSokołowska, Beata. 2021. "A Novel Perspective for Examining and Comparing Real and Virtual Test Tasks Performed by the Dominant and Non-Dominant Hand in Healthy Adults" Symmetry 13, no. 10: 1810. https://doi.org/10.3390/sym13101810
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.