
Are Millets More Effective in Managing Hyperlipidaemia and Obesity than Major Cereal Staples? A Systematic Review and Meta-Analysis

 ,
,  , , ,
, , , 
Abstract
:1. Introduction
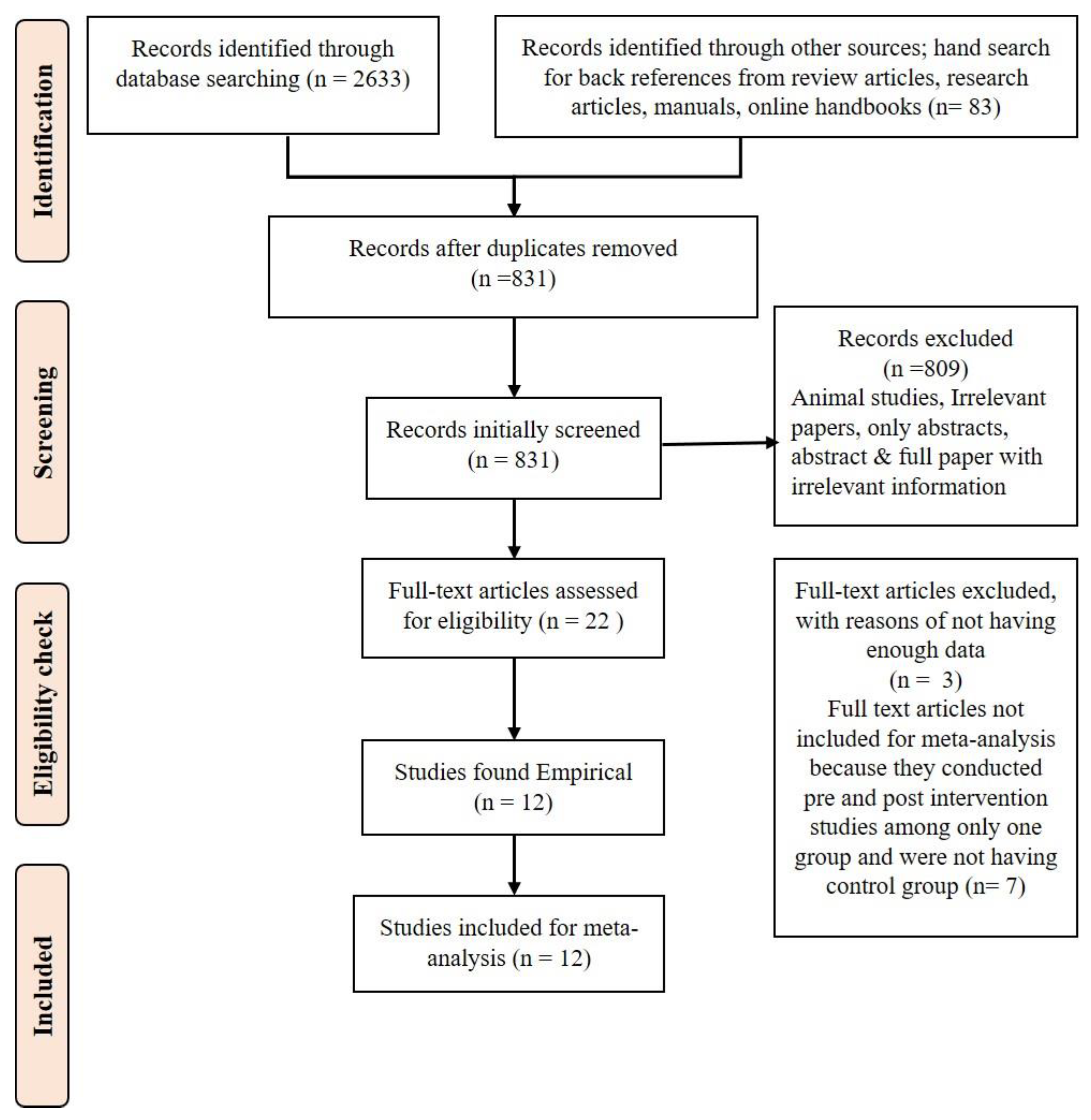
2. Materials and Methods
2.1. Study Period
2.2. Information Sources
2.3. Inclusion Criteria
2.4. Exclusion Criteria
2.5. Data Extraction
2.6. GRADE to Assess the Quality of Evidence
2.7. Summary Measures and Result Synthesis
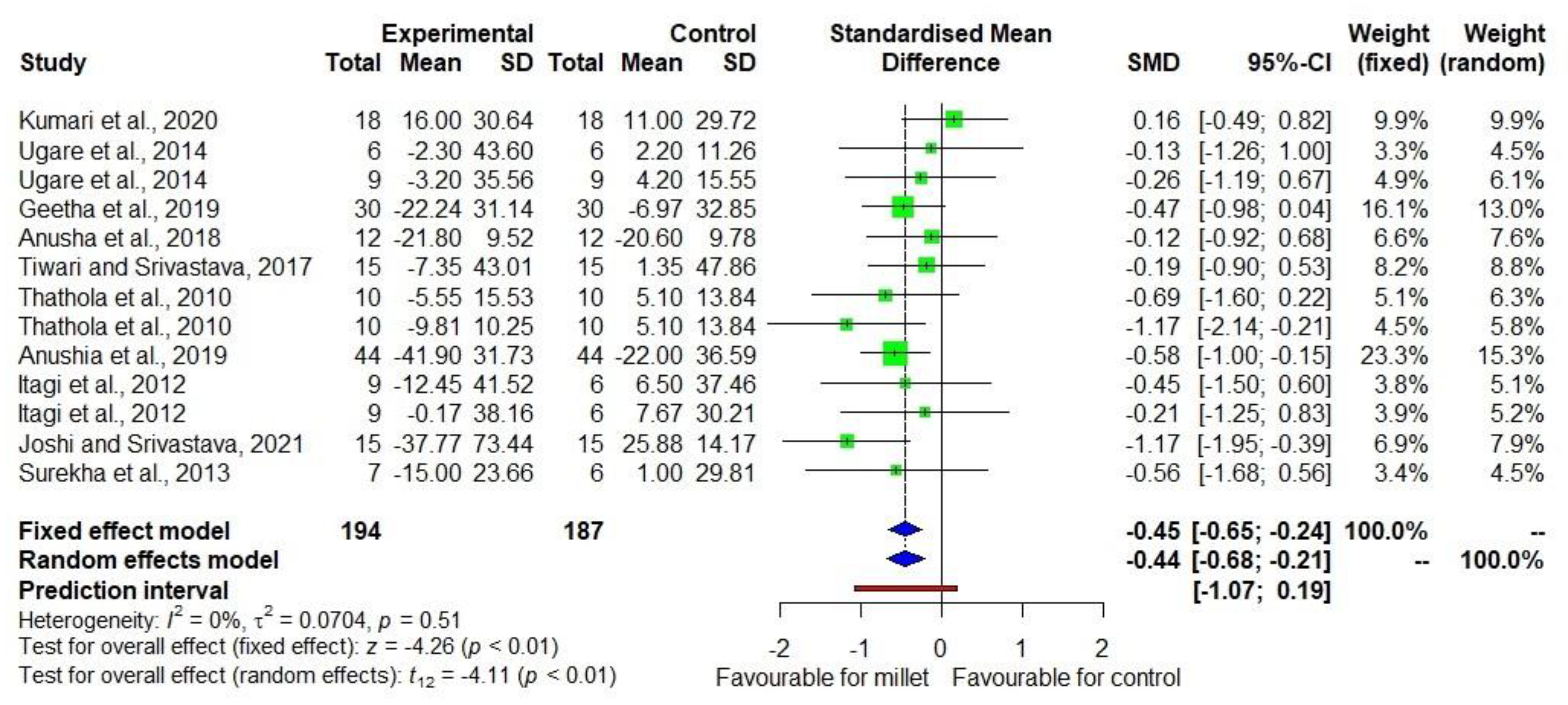
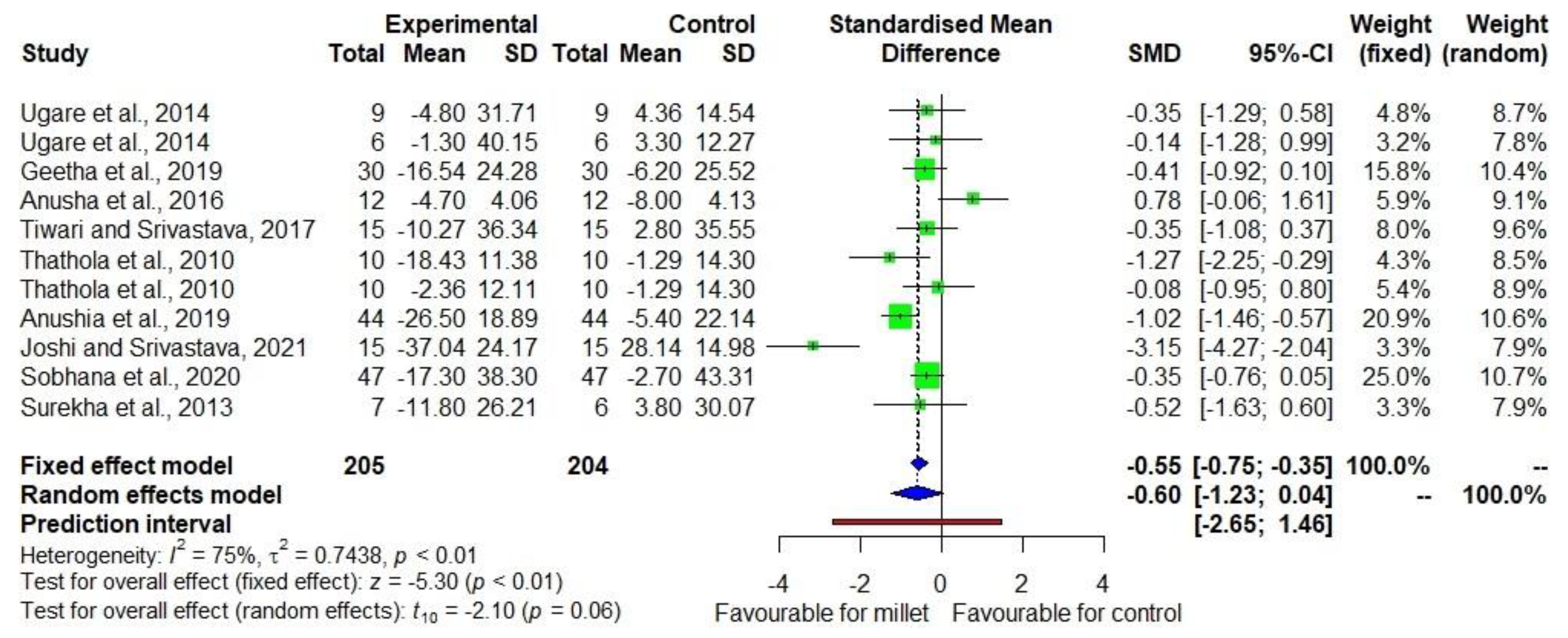
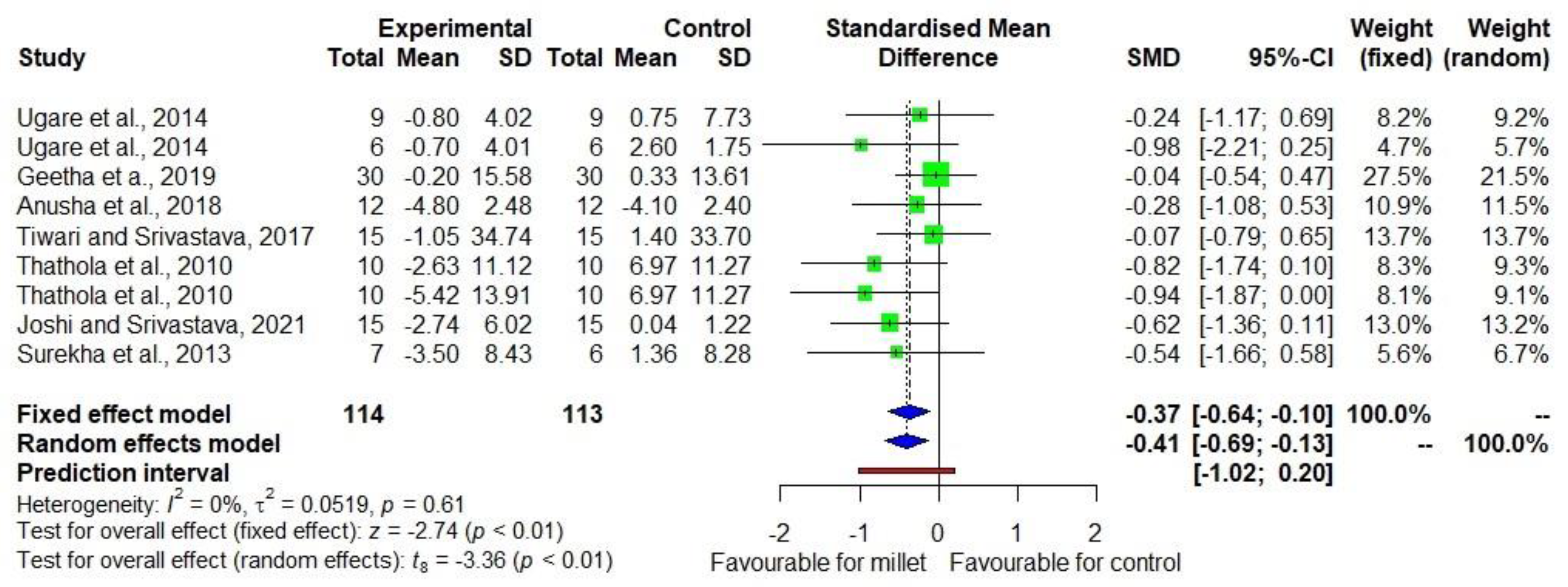
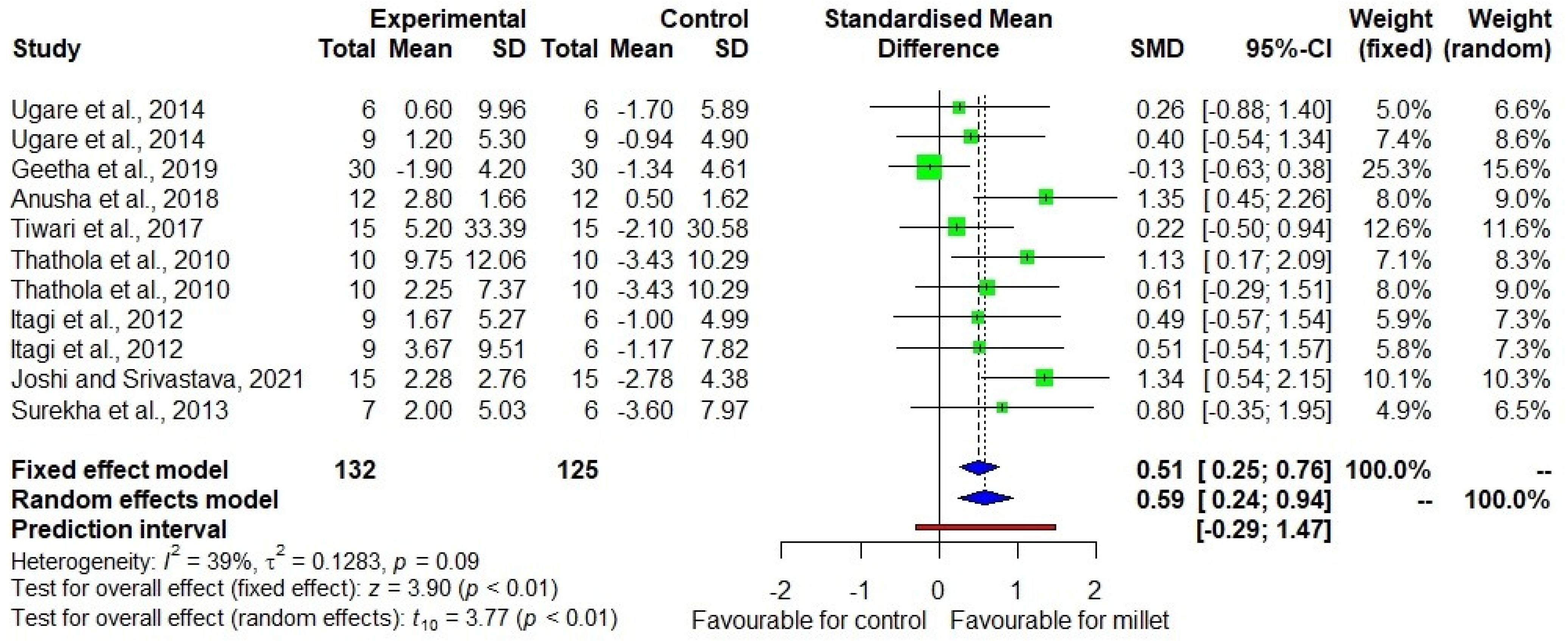
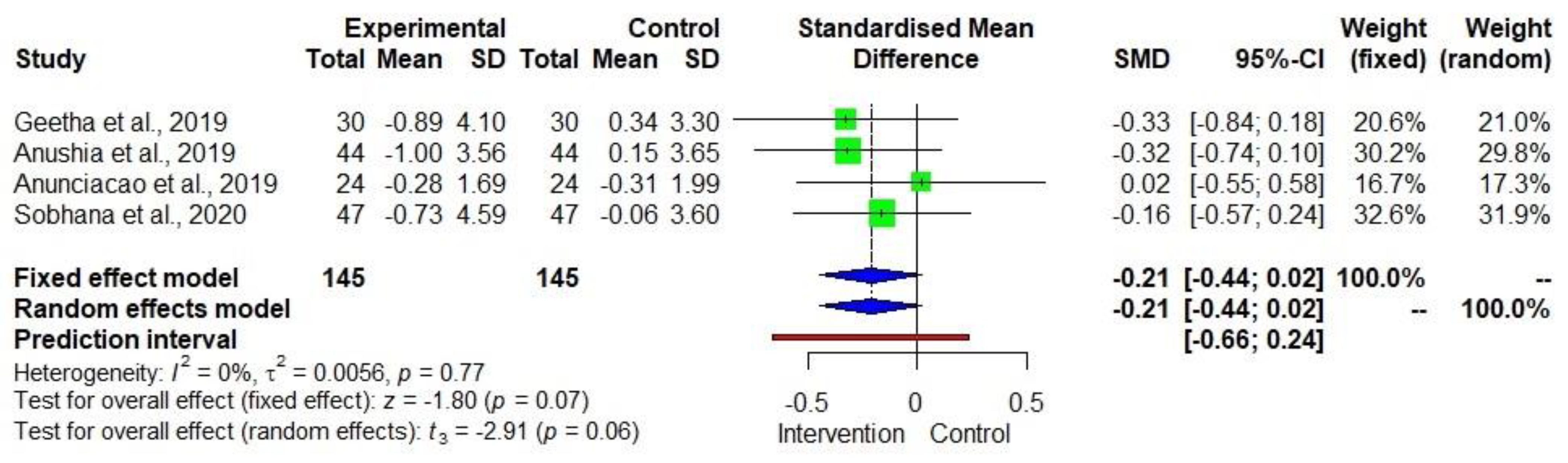
3. Results
4. Discussions
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Willett, W.; Rockström, J.; Loken, B.; Springmann, M.; Lang, T.; Vermeulen, S.; Garnett, T.; Tilman, D.; DeClerck, F.; Wood, A.; et al. Food in the Anthropocene: The EAT-Lancet commission on healthy diets from sustainable food systems. Lancet 2019, 393, 447–492. [Google Scholar] [CrossRef]
- Vidal, A.; Jeantet, F.; Fellus, E.; De Nardi, C.; Kane-Potaka, J. Staple Crop Diversification Why and How to Diversify from the Big Five Crops (Wheat, Rice, Maize, Potato & Soy), World Business Council for Sustainable Development and One Planet Business for Biodiversity. 2020. Available online: https://www.wbcsd.org/download/file/12605 (accessed on 13 February 2021).
- Kane-Potaka, J.; Poole, N.; Diama, A.; Kumar, P.; Anitha, S.; Akinbamijo, O. The Smart Food Approach: The importance of the triple bottom line and diversifying staples. In Orphan Crops for Sustainable Food and Nutrition Security; Padulosi, S., Israel Oliver King, E.D., Hunter, D., Swaminathan, M.S., Eds.; Routledge Taylor & Francis Group: New York, NY, USA, 2022; pp. 327–334. [Google Scholar]
- Anitha, S.; Kane-Potaka, J.; Tsusaka, T.W.; Botha, R.; Rajendran, A.; Givens, D.I.; Parasannanavar, D.J.; Subramaniam, K.; Prasad, K.D.V.; Vetriventhan, M.; et al. A systematic review and meta-analysis of the potential of millets and sorghum for managing and preventing diabetes mellitus. Front. Nutr. 2021, 8, 687428. [Google Scholar] [CrossRef]
- Anitha, S.; Botha, R.; Kane-Potaka, J.; Givens, D.I.; Rajendran, A.; Tsusaka, T.W.; Bhandari, R.K. Can millet consumption help to manage hyperlipidaemia and obesity—A systematic review and meta-analysis. Front. Nutr. 2021, 8, 700778. [Google Scholar] [CrossRef]
- Anitha, S.; Kane-Potaka, J.; Botha, R.; Givens, D.I.; Sulaiman, N.L.B.; Upadhyay, S.; Vetriventhan, M.; Tsusaka, T.W.; Parasannanavar, D.J.; Longvah, T.; et al. Millets can have a major impact on improving iron status, haemoglobin level and in reducing iron deficiency anaemia—A systematic review and meta-analysis. Front. Nutr. 2021, 712, 725529. [Google Scholar] [CrossRef]
- Mohar, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analysis: The PRISMA statement. Open Med. 2009, 3, 123–130. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 88, 105906. [Google Scholar]
- Atkinson, L.Z.; Cipriani, A. How to carry out a literature search for a systematic review: A practical guide. BJP Sych. Adv. 2018, 24, 74–82. [Google Scholar] [CrossRef]
- Harrer, M.; Cuijpers, P.; Furukawa, T.A.; Ebert, D.D. Doing Meta-Analysis with R: A Hands-On Guide. 2019. Available online: https://bookdown.org/MathiasHarrer/Doing_Meta_Analysis_in_R/ (accessed on 28 February 2021).
- Ryan, R.; Hill, S. How to GRADE the Quality of the Evidence? Cochrane Consumers and Communication Group. Version 3.0. 2016. Available online: http://cccrg.cochrance.org/author-resources (accessed on 7 December 2021).
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2021; Available online: https://www.R-project.org/ (accessed on 1 March 2021).
- Balduzzi, S.; Rücker, G.; Schwarzer, G. How to perform a meta-analysis with R: A practical tutorial? Evid. Based Ment. Health 2019, 22, 153–160. [Google Scholar] [CrossRef]
- Bell, A.; Fairbrother, M.; Jones, K. Fixed and random effects models: Making an informed choice. Qual. Quant. 2019, 53, 1051–1074. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J. Cochrane Handbook for Systematic Reviews of Interventions Version 6.2 (Updated February 2021); Welch, V.A., Ed.; Cochrane: London, UK, 2021; Available online: www.training.cochrane.org/handbook (accessed on 13 April 2021).
- Ahn, E.; Kang, H. Introduction to systematic review and meta-analysis. Korean J. Anaesthesiol. 2019, 71, 103–112. [Google Scholar] [CrossRef]
- Hak, T.; Van Rhee, H.J.; Suurmond, R. How to Interpret Results of Meta-Analysis; Erasmus Rotterdam Institute of Management: Rotterdam, The Netherlands, 2016; pp. 1–2. Available online: https://www.erim.eur.nl/research-support/metaessentials/downloads (accessed on 26 April 2021).
- Isreal, H.; Richter, R.P. A guide to understanding meta-analysis. J. Orthop. Sports Phys. Ther. 2011, 41, 496–504. [Google Scholar] [CrossRef]
- Kumari, D.; Chandrasekara, A.; Athukorale, P.; Shahidi, F. Finger millet porridges subjected to different processing conditions showed low glycemic index and variable efficacy on plasma antioxidant capacity of healthy adults. Food Prod. Process. Nutr. 2020, 2, 13. [Google Scholar] [CrossRef]
- Ugare, R.; Chimmad, B.; Naik, R.; Bharati, P.; Itagi, S. Glycemic index and significance of barnyard millet (Echinochloa frumentacae) in type II diabetics. J. Food Sci. Technol. 2014, 51, 392–395. [Google Scholar] [CrossRef]
- Geetha, K.; Yankanchi, M.G.; Hiremath, N. Effect of high fibre food mix on lipid profile and body weight in obese subjects. Biomed. Res. 2019, 30, 655–658. [Google Scholar]
- Anusha, B.; Hymavathi, T.V.; Vijayalaskhmi, V.; Reddy, P.; Robert, T.P. Lipid lowering effects of foxtail millet (Setaria italic) and Quinoa (Chenopodium quinoawild) in pre-diabetics. J. Pharm. Res. Int. 2018, 24, 1–7. [Google Scholar] [CrossRef]
- Tiwari, N. Srivastava. Effect of finger millet (Eleusine coracana) buns supplementation on serum glucose and serum lipids level in type 2 diabetics. Asian J. Dairy Food Res. 2017, 36, 337–340. [Google Scholar] [CrossRef]
- Thathola, A.; Srivastava, S.; Singh, G. Effect of foxtail millet (Setaria Italica) supplementation on serum glucose, serum lipids and glycosylated haemoglobin in type 2 diabetics. Diabetol. Croatica. 2011, 40, 23–29. [Google Scholar]
- Anushia, K.; Uma Mageshwari, J.; Trueman, P.; Viswanathan, V. The effect of millet supplementation on weight and lipid profile. TAPI J. 2019, 13, 1–7. [Google Scholar]
- Itagi, S.; Naik, R.; Bharati, P.; Sharma, P. Readymade foxtail millet mix for diabetics. Int. J. Sci. Nat. 2012, 3, 47–50. [Google Scholar]
- Joshi, S.; Srivastava, S. Hypoglycemic and hypolipidemic effect of barnyard millet consumption in type 2 diabetic subjects. Int. J. Curr. Microbiol. Appl. Sci. 2021, 10, 467–477. [Google Scholar]
- Surekha, N.; Chimmad, B.V.; Naik, R.S. Hypoglycaemic and hypolipidemic efficacy of barnyard millet (Echinochloa frumentacea Link) based health food. Asian J. Home Sci. 2013, 8, 383–387. [Google Scholar]
- Sobhana, P.P.; Kandlakunta, B.; Nagaraju, R.; Thappatla, D.; Epparapalli, S.; Vemula, S.R.; Govaravarapu, S.M.; Korrapati, D. Human clinical trial to assess the effect of consumption of multigrain Indian bread on glycemic regulation in type 2 diabetic participants. J. Food Biochem. 2020, 44, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Anunciacao, P.C.; Cardoso, L.D.M.; Alfenas, R.D.C.G.; Queiroz, V.A.V.; Carvalho, C.W.P.; Martino, H.S.D.; Pinheiro-SantAna, H.M. Extruded sorghum consumption assoicated with a caloric restricted diet reduces body fat in overweight men: A randomized controlled trial. Food Res. Int. 2019, 119, 693–700. [Google Scholar] [CrossRef] [PubMed]
- Stern, J.A.C.; Sutton, A.J.; Loannidis, J.P.A.; Terrin, N.; Jones, D.R.; Lau, J.; Carpenter, J.; Rücker, G.; Harbord, R.M.; Schmid, C.H.; et al. Recommendations for examining and interpreting funnel plot asymmetry in meta-analyses of randomised controlled trials. BMJ 2011, 342, 4002. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Anitha, S.; Tsusaka, T.W.; Botha, R.; Kane-Potaka, J.; Givens, D.I.; Rajendran, A.; Bhandari, R.K. Are Millets More Effective in Managing Hyperlipidaemia and Obesity than Major Cereal Staples? A Systematic Review and Meta-Analysis. Sustainability 2022, 14, 6659. https://doi.org/10.3390/su14116659
Anitha S, Tsusaka TW, Botha R, Kane-Potaka J, Givens DI, Rajendran A, Bhandari RK. Are Millets More Effective in Managing Hyperlipidaemia and Obesity than Major Cereal Staples? A Systematic Review and Meta-Analysis. Sustainability. 2022; 14(11):6659. https://doi.org/10.3390/su14116659
Chicago/Turabian StyleAnitha, Seetha, Takuji W. Tsusaka, Rosemary Botha, Joanna Kane-Potaka, David Ian Givens, Ananthan Rajendran, and Raj Kumar Bhandari. 2022. "Are Millets More Effective in Managing Hyperlipidaemia and Obesity than Major Cereal Staples? A Systematic Review and Meta-Analysis" Sustainability 14, no. 11: 6659. https://doi.org/10.3390/su14116659