
How Do Rural Communities Sustain Sanitation Gains? Qualitative Comparative Analyses of Community-Led Approaches in Cambodia and Ghana


Abstract
:1. Introduction
1.1. Community Leadership
1.2. Follow-Up Activities
1.3. Financial and Pro-Poor Support
2. Materials and Methods
2.1. Study Sites and CLTS Programs
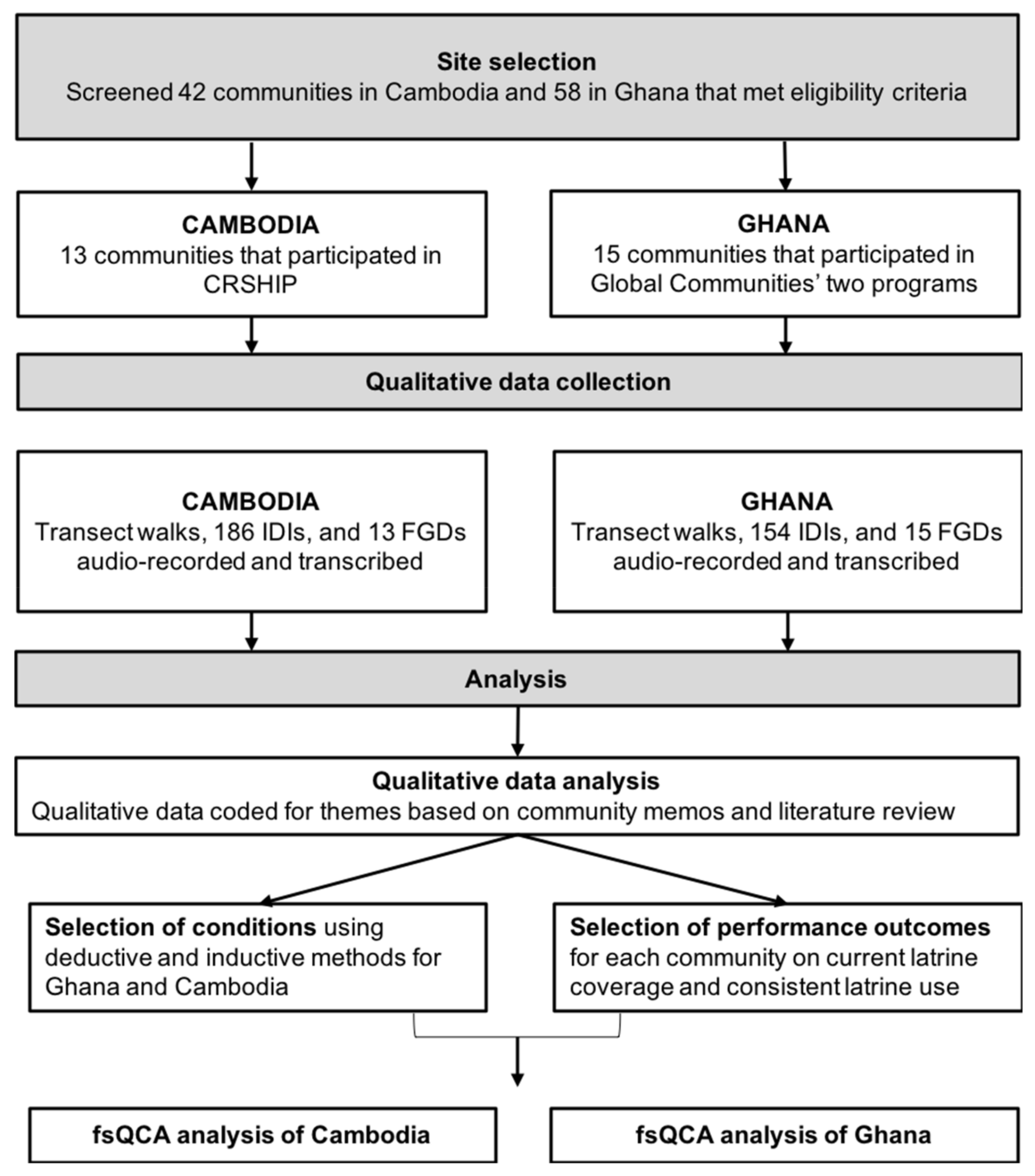
2.2. Community Selection
2.2.1. Eligibility Criteria
2.2.2. Sampling Strategy
2.3. Qualitative Data Collection
2.4. Ethical Review
2.5. Data Analysis
3. Results
3.1. Outcomes
3.1.1. Outcomes 1: Current Latrine Coverage
3.1.2. Outcome 2: Consistent Latrine Use
3.2. Condition Summaries
3.2.1. Leadership
3.2.1.1. Commune Engagement (Cambodia)
3.2.1.2. Traditional Leaders
3.2.1.3. Natural Leaders (Ghana)
3.2.2. Follow-Up
3.2.2.1. Follow-Up by External Actors (NGOs in Cambodia and CLTS Facilitators in Ghana)
3.2.2.2. Post-ODF Follow-Up by Internal Actors (Ghana)
3.2.3. Pro Poor and Financial Support
3.2.3.1. Financial Support (Cambodia)
3.2.3.2. Subsidies before Triggering (Cambodia)
3.2.3.3. Pro-Poor Support/Internal Support
3.2.4. Women in Sanitation (Ghana)
3.3. Pathway Analysis
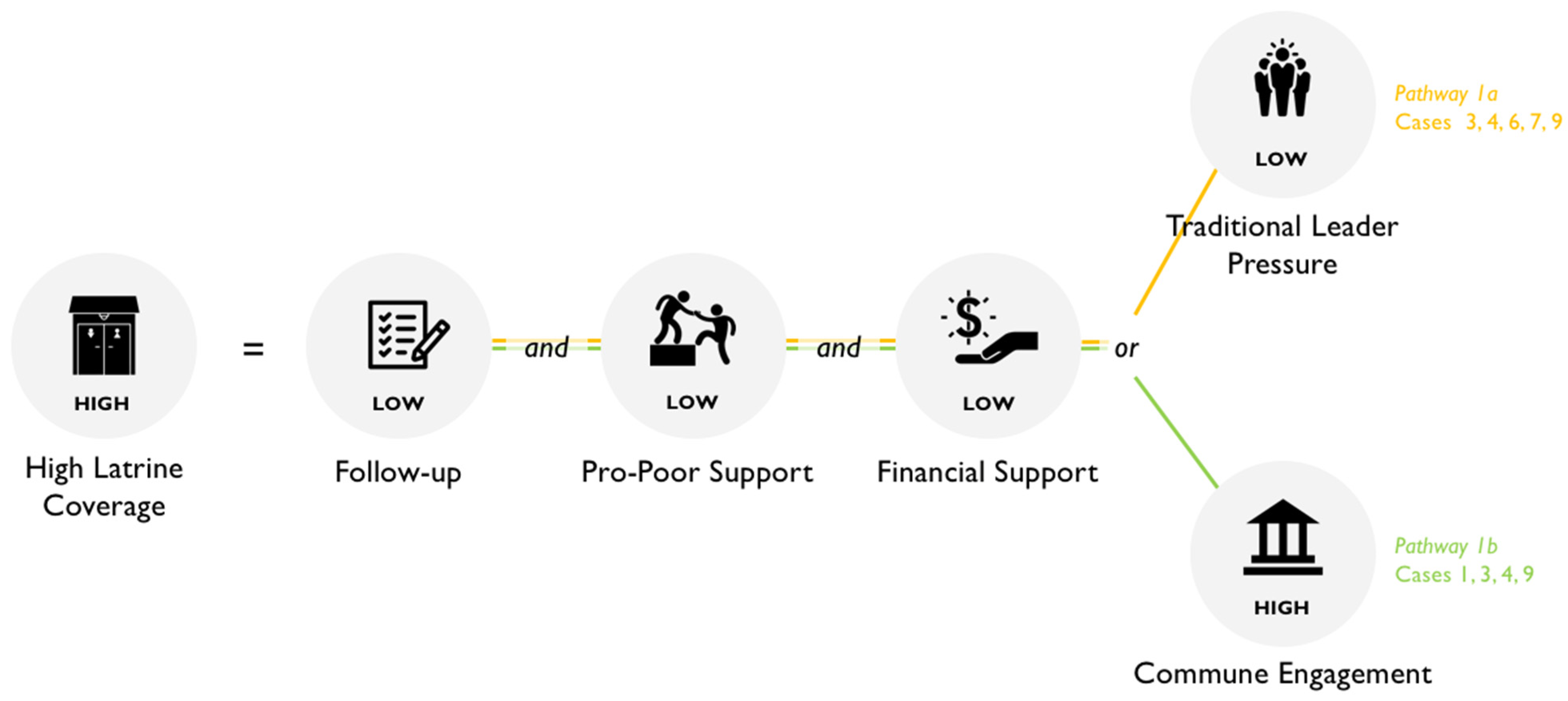
3.3.1. Latrine Coverage in Cambodia
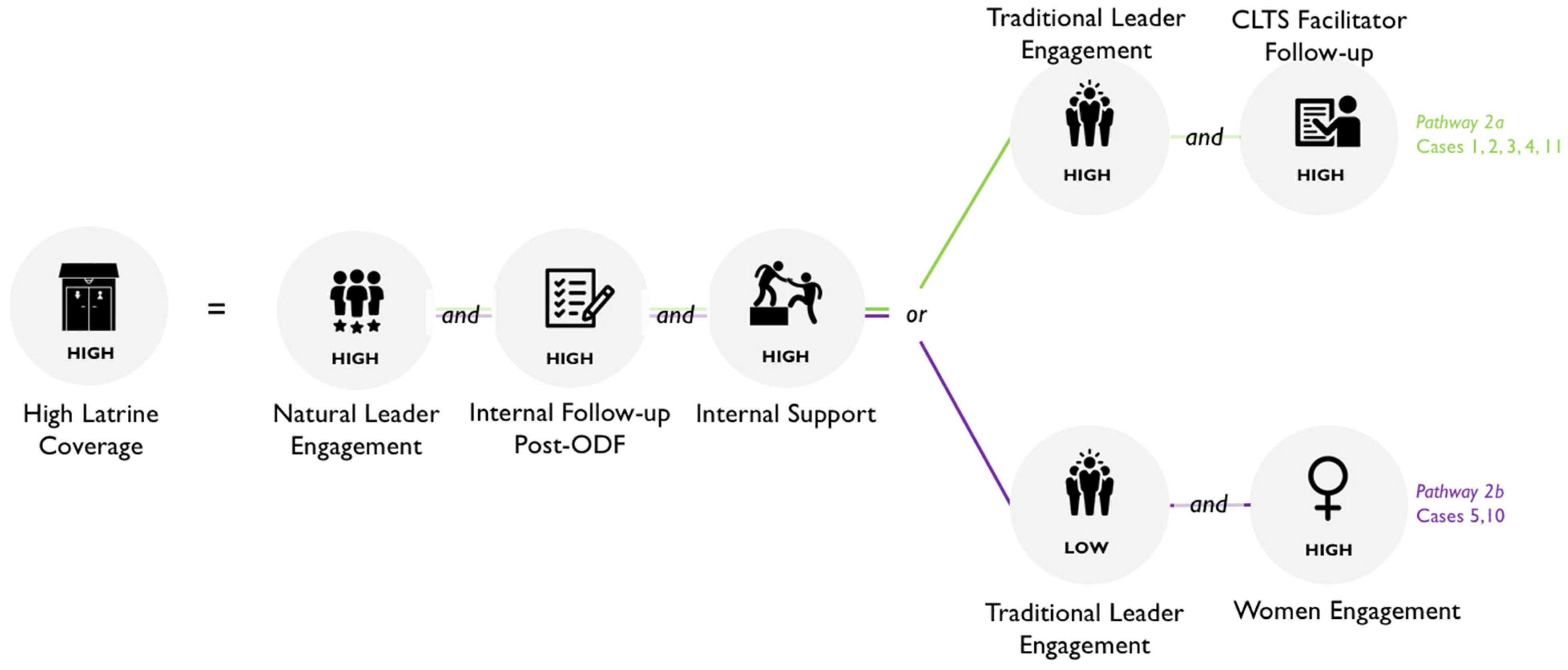
3.3.2. Latrine Coverage in Ghana
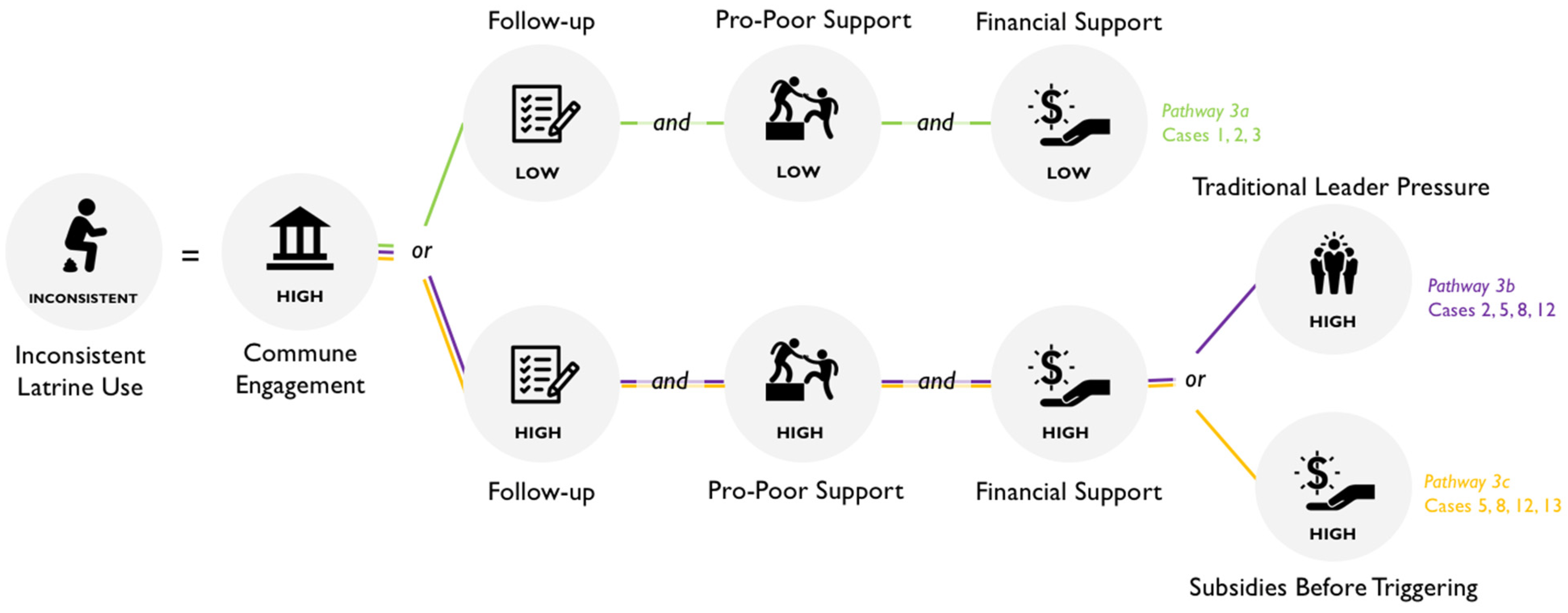
3.3.3. Inconsistent Latrine Use in Cambodia
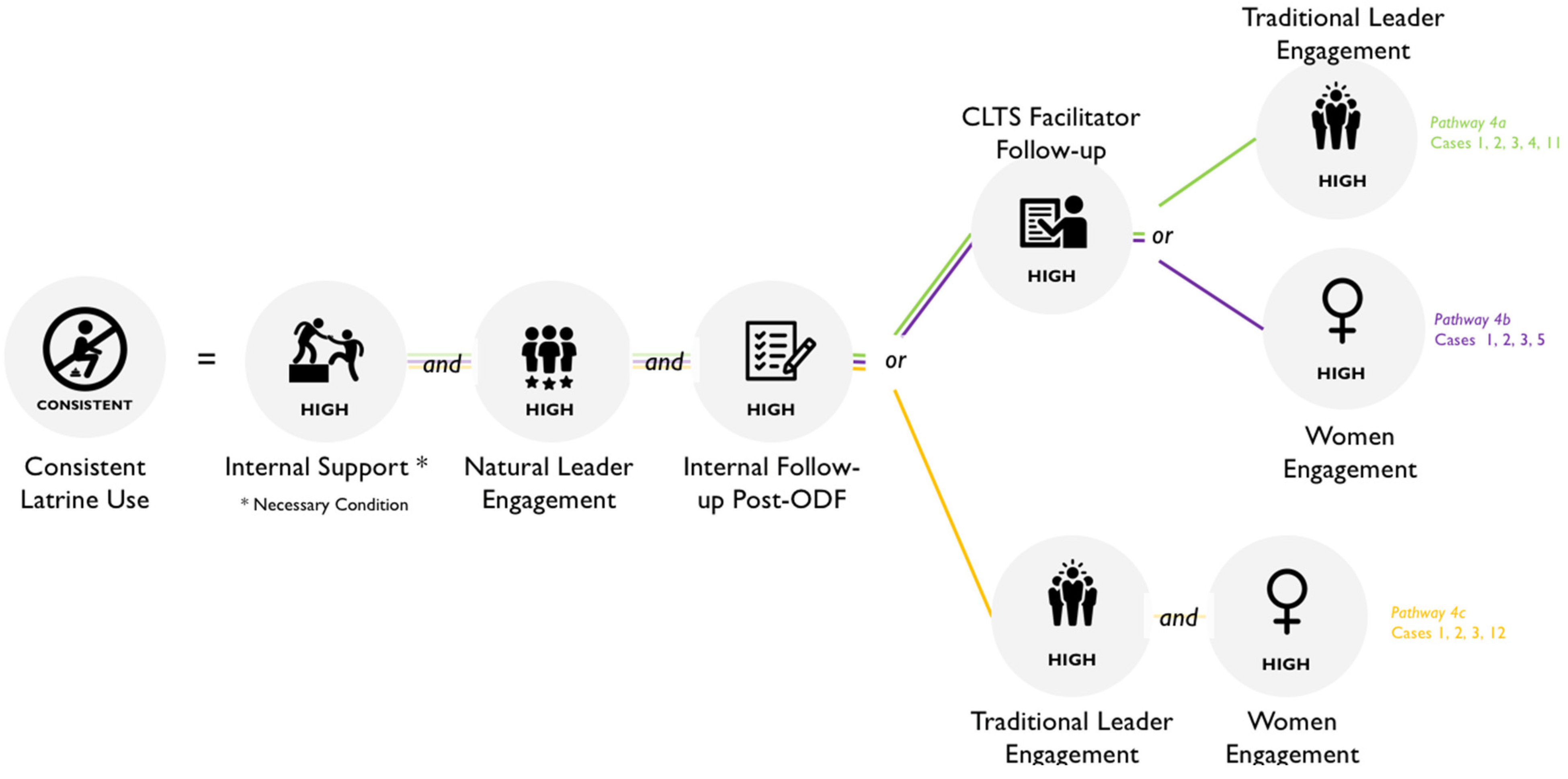
3.3.4. Consistent Latrine Use in Ghana
4. Discussion
4.1. Conditions Influencing High Latrine Coverage in Cambodia and Ghana
4.2. Conditions Influencing Latrine Use in Cambodia and Ghana
4.3. Role of Women
4.4. Implications for Future Programming and Research
4.5. Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO/UNICEF JMP. Progress on Household Drinking Water, Sanitation and Hygiene 2000–2017: Special Focus on Inequalities; UNICEF: New York, NY, USA, 2019. [Google Scholar]
- Zuin, V.; Delaire, C.; Peletz, R.; Cock-Esteb, A.; Khush, R.; Albert, J. Policy Diffusion in the Rural Sanitation Sector: Lessons from Community-Led Total Sanitation (CLTS). World Dev. 2019, 124, 104643. [Google Scholar] [CrossRef]
- Kar, K.; Chambers, R. Handbook on Community-Led Total Sanitation; Plan International: Brighton, UK, 2008; Volume 44. [Google Scholar]
- Venkataramanan, V.; Crocker, J.; Karon, A.; Bartram, J. Community-Led Total Sanitation: A Mixed-Methods Systematic Review of Evidence and Its Quality. Environ. Health Perspect. 2018, 126, 17. [Google Scholar] [CrossRef]
- WaterAid; UNICEF; Plan International. Rethinking Rural Sanitation Approaches; The Water Institute at UNC: Chapel Hill, NC, USA, 2017. [Google Scholar]
- Whittington, D.; Radin, M.; Jeuland, M. Evidence-based policy analysis? The strange case of the randomized controlled trials of community-led total sanitation. Oxford Rev. Econ. Policy. 2020, 36, 191–221. [Google Scholar] [CrossRef]
- USAID. An Examination of CLTS’s Contributions Toward Universal Sanitation; USAID: Washington, DC, USA, 2018.
- Stuart, K.; Peletz, R.; Albert, J.; Khush, R.; Delaire, C. Where Does CLTS Work Best? Quantifying Predictors of CLTS Performance in Four Countries. Environ. Sci. Technol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Cavill, S.; Chambers, R.; Vernon, N. Frontiers of CLTS: Innovations and Insights; Institute of Development Studies: Brighton, UK, 2015. [Google Scholar]
- Mukherjee, N.; Robiarto, A.; Saputra, E.; Wartono, D. Achieving and Sustaining Open Defecation Free Communities: Learning from East Java; Water Sanitation Program, World Bank: Washington, DC, USA, 2012. [Google Scholar]
- UNICEF. Evaluation of the WASH Sector Strategy ‘Community Approaches to Total Sanitation’ (CATS); UNICEF: New York, NY, USA, 2014. [Google Scholar]
- Lawrence, J.J.; Yeboah-Antwi, K.; Biemba, G.; Ram, P.K.; Osbert, N.; Sabin, L.L.; Hamer, D.H. Beliefs, Behaviors, and Perceptions of Community-Led Total Sanitation and Their Relation to Improved Sanitation in Rural Zambia. Am. J. Trop. Med. Hyg. 2016, 94, 553–562. [Google Scholar] [CrossRef]
- Robinson, A. Final Evaluation: Pan African CLTS Program 2010–2015; Plan Netherlands: Amsterdam, The Netherlands, 2016. [Google Scholar]
- Crocker, J.; Shields, K.F.; Venkataramanan, V.; Saywell, D.; Bartram, J. Building capacity for water, sanitation, and hygiene programming: Training evaluation theory applied to CLTS management training in Kenya. Soc. Sci. Med. 2016, 166, 66–76. [Google Scholar] [CrossRef] [Green Version]
- Harter, M.; Lilje, J.; Mosler, H.J. Role of Implementation Factors for the Success of Community-Led Total Sanitation on Latrine Coverage. A Case Study from Rural Ghana. Environ. Sci. Technol. 2019, 53, 5466–5472. [Google Scholar] [CrossRef]
- Kullmann, C.; Ahmed, R.; Hanchett, S.; Krieger, L.; Kahn, M.H. Long-Term Sustainability of Improved Sanitation in Rural Bangladesh; Water Sanitation Program, World Bank: Washington, DC, USA, 2011. [Google Scholar]
- Tyndale-Biscoe, P.; Bond, M.; Kidd, R. ODF Sustainability Study; Plan International: Brighton, UK, 2013. [Google Scholar]
- Gertler, P.J.; Shah, M.; Alzua, M.L.; Cameron, L.A.; Martinez, S.; Patil, S.R. How Does Health Promotion Work? Evidence from The Dirty Business of Eliminating Open Defecation; National Bureau of Economic Research: Cambridge, MA, USA, 2015. [Google Scholar] [CrossRef]
- Bateman, M.; Engel, S. To shame or not to shame—that is the sanitation question. Dev. Policy Rev. 2018, 36, 155–173. [Google Scholar] [CrossRef]
- Alzua, M.L.; Pickering, A.J.; Djebbari, H.; Lopez, C.; Cardenas, J.C.; Lopera, M.A.; Osbert, N.; Coulibaly, M. Impact Evaluation of Community-Led Total Sanitation (CLTS) in Rural Mali; CEDLAS, Working Papers 0191, CEDLAS; Universidad Nacional de La Plata: La Plata, Argentina, 2015. [Google Scholar]
- Cameron, L.A.; Shah, M. Scaling Up Sanitation: Evidence from an RCT in Indonesia; Abdul Latif Jameel Poverty Action Lab: Cambridge, MA, USA, 2017. [Google Scholar]
- Harvey, P.A. Zero subsidy strategies for accelerating access to rural water and sanitation services. Water Sci. Technol. 2011, 63, 1037–1043. [Google Scholar] [CrossRef]
- Sah, S.; Negussie, A. Community led total sanitation (CLTS): Addressing the challenges of scale and sustainability in rural Africa. Desalination 2009, 248, 666–672. [Google Scholar] [CrossRef]
- Venkataramanan, V. Testing CLTS Approaches for Scalability CLTS Learning Series: Lessons from CLTS Implementation in Seven Countries; Plan International: Washington, DC, USA, 2016. [Google Scholar]
- Crocker, J.; Abodoo, E.; Asamani, D.; Domapielle, W.; Gyapong, B.; Bartram, J. Impact Evaluation of Training Natural Leaders during a Community-Led Total Sanitation Intervention: A Cluster-Randomized Field Trial in Ghana. Environ. Sci. Technol. 2016, 50, 8867–8875. [Google Scholar] [CrossRef]
- Kar, K.; Bongartz, P. Update on Some Recent Developments in Community-Led Total Sanitation; University of Sussex, Institute of Development Studies: Brighton, UK, 2006. [Google Scholar]
- Vernon, N.; Bongartz, P. CHAPTER 1: Going beyond open defecation free. In Sustainable Sanitation for All; Bongartz, P., Vernon, N., Fox, J., Eds.; Practical Action Publishing: Rugby, UK, 2016. [Google Scholar]
- Jenkins, M.W.; Scott, B. Behavioral indicators of household decision-making and demand for sanitation and potential gains from social marketing in Ghana. Soc. Sci. Med. 2007, 64, 2427–2442. [Google Scholar] [CrossRef] [PubMed]
- Whaley, L.; Webster, J. The Effectiveness and Sustainability of Two Demand-driven Sanitation and Hygiene Approaches in Zimbabwe. J. Water Sanit. Hyg. Dev. 2011, 1, 20–36. [Google Scholar] [CrossRef] [Green Version]
- Munkhondia, T.; Simangolwa, W.; Zapico, A. CLTS and sanitation marketing: Aspects to consider for a better integrated approach. In Sustainable Sanitation for All: Experences, Challenges, and Innovations; Bongartz, P., Vernon, N., Fox, J., Eds.; Practical Action Publishing: Rugby, UK, 2016. [Google Scholar]
- Coombes, Y. CHAPTER 6: User-centred latrine guidelines—integrating CLTS with sanitation marketing: A case study from Kenya to promote informed choice. In Sustainable Sanitation for All; Bongartz, P., Vernon, N., Fox, J., Eds.; Practical Action Publishing: Rugby, UK, 2016; pp. 121–134. ISBN 9781780449272. [Google Scholar]
- Singh, S.; Balfour, N. Sustainability of ODF Practices in Kenya; UNICEF Kenya: Nairobi, Kenya, 2015. [Google Scholar]
- Thomas, A.; Bevan, J. Developing and Monitoring Protocol for the Elimination of Open Defecation in Sub-Saharan Africa; ODF Protocol. IRC: The Hague, The Netherlands, 2013. [Google Scholar]
- Guiteras, R.P.; Levinsohn, J.; Mobarak, A.M. Encouraging sanitation investment in the developing world: A cluster-randomized trial. Science 2015, 348, 903–906. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nguyen, N.K.; Nguyen, H.D.; Gerwel-Jensen, L.; Nguyen, M.T.H.; Nam, D.C. Understanding Determinants of Access to Hygienic Latrines for Rural Households in Vietnam; Water Sanitation Program, World Bank: Washington, DC, USA, 2016. [Google Scholar]
- Dumpert, J.; Ung, K. A Retrospective Review of Phase 1 of CRSHIP; WaterAid Cambodia: Phnom Penh, Cambodia, 2017. [Google Scholar]
- Ragin, C.C. Measurement Versus Calibration: A Set-Theoretic Approach. Oxford Handbook of Political Methodology 2008, 1–31. [Google Scholar] [CrossRef]
- Rihoux, B.; Ragin, C.; Berg-Schlosser, D.; Meur, G.; De Rihoux, B.; Ragin, C.C. Qualitative Comparative Analysis (QCA) as an Approach. In Configurational Comparative Methods: Qualitative Comparative Analysis (QCA) and Related Techniques; SAGE Publishing: Thousand Oaks, CA, USA, 2012; pp. 1–18. [Google Scholar] [CrossRef]
- Mukherjee, N. CHAPTER 3: Building environments to support sustainability of improved sanitation behaviours at scale: Levers of change in East Asia. In Sustainable Sanitation for All; Bongartz, P., Vernon, N., Fox, J., Eds.; Practical Action Publishing: Rugby, UK, 2016; pp. 53–82. ISBN 9781780449272. [Google Scholar]
- UNICEF. Community-Led Total Sanitation in East Asia and Pacific: Progress, Lessons and Directions; UNICEF: Bangkok, Thailand, 2013. [Google Scholar]
- Ministry of Rural Development National CLTS Guidelines; Government of Cambodia: Phnom Penh, Cambodia, 2014.
- Ministry of Sanitation and Water Resources Guidelines for Targeting the Poor and Vulnerable for Basic Sanitation Services in Ghana; Government of Ghana: Accra, Ghana, 2018.
- Kaminsky, J.; Jordan, E. Qualitative comparative analysis for WASH research and practice. J. Water Sanit. Hyg. Dev. 2017, 7, 13. [Google Scholar] [CrossRef]
- Davis, A.; Javernick-Will, A.; Cook, S.M. The use of qualitative comparative analysis to identify pathways to successful and failed sanitation systems. Sci. Total Environ. 2019, 663, 507–517. [Google Scholar] [CrossRef] [PubMed]
- CRSHIP. Fostering Collective Action To Improve Sanitation in Rural; Plan International Cambodia: Phnom Penh, Cambodia, 2018. [Google Scholar]
- World Bank GDP per Capita Growth (Annual %)—Cambodia. Available online: https://data.worldbank.org/indicator/NY.GDP.PCAP.KD.ZG?locations=KH. (accessed on 17 April 2020).
- Mukherjee, N. Factors Associated with Achieving and Sustaining Open Defecation Free Communities: Learning from East Java; Water Sanitation Program, World Bank: Washington, DC, USA, 2011. [Google Scholar]
- Huda, E. Natural Leaders Emerged through Community Led Total Sanitation (CLTS) Approach in Bangladesh (Profile and Market Promotion); CLTS Knowledge Hub, Institute for Development Studies (IDS): Brighton, UK, 2009. [Google Scholar]
- Otieno, P. Engaging Natural Leaders in Community-Led Total Sanitation in Nigeria; WaterAid Nigeria: Lagos, Nigeria, 2011. [Google Scholar]
- Haq, A.; Bod, B. Hunger, Subsidies and Process Facilitation: Challenges for Community Led Total Sanitation in Bangladesh; CLTS Knowledge Hub, Institute for Development Studies (IDS): Brighton, UK, 2009. [Google Scholar]
- Dyalchand, A.; Kale, M.; Vasudevan, S. What Communication and Institutional Arrangements Influence Sanitation Related Social Norms in Rural India? CLTS Knowledge Hub, Institute for Development Studies (IDS): Brighton, UK, 2009. [Google Scholar]
- Jha, H.B. An Assessment of CLTS Projects and Formulation of the Strategy on Sanitation Promotion; Centre for Economic and Technical Studies Pvt. Ltd.: Lalitpur, Nepal, 2007. [Google Scholar]
- Pardeshi, G.; Shirke, A.; Jagtap, M. SWOT analysis of total sanitation campaign in Yavatmal district of Maharashtra. Indian J. Community Med. 2008, 33, 255–259. [Google Scholar] [CrossRef]
- USAID. Ghana WASH Project—Lessons Learned: Hybrid CLTS Approach to Improving Sanitation; USAID: Washington, DC, USA, 2014.
- O’Reilly, K.; Louis, E. The toilet tripod: Understanding successful sanitation in rural India. Health Place 2014, 29, 43–51. [Google Scholar] [CrossRef] [Green Version]
- UNICEF. WCARO Roll-Out Evaluation of “Community Led Total Sanitation” in West and Centra Africa; UNICEF: Dakar, Senegal, 2011. [Google Scholar]
- Venkataramanan, V.; Shannon, A. CLTS Learning Series: Lessons from CLTS Implementation in Seven Countries; The Water Institute at UNC: Chapel Hill, NC, USA, 2016. [Google Scholar]
- Harter, M.; Inauen, J. The role of social identification for achieving an open-defecation free environment: A cluster-randomized, controlled trial of Community-Led Total Sanitation in Ghana. J. Environ. Psychol. 2019, 101360. [Google Scholar] [CrossRef]
- Hirai, M.; Graham, J.P.; Sandberg, J. Understanding women’s decision making power and its link to improved household sanitation: The case of Kenya. J. Water Sanit. Hyg. Dev. 2016, 6, 151–160. [Google Scholar] [CrossRef]
- USAID Water CKM Project. Evaluation Report: Madagascar Rural Access to New Opportunities for Health and Prosperity (RANO-HP) Sustainability Evaluation; USAID: Washington, DC, USA, 2017.
- Adeyeye, A. Gender and Community-Led Total Sanitation: A Case Study of Ekiti State, Nigeria. Trop. Resour. 2011, 30, 1–27. [Google Scholar]
- Arandan, S.N. Role of Gender on Community Led Total Sanitation Processes in Kanyingombe Community Health Unit, Rongo Sub County, Kenya. Eur. Int. J. Sci. Technol. 2016, 5, 89–98. [Google Scholar]
- Cavill, S.; Roose, S.; Stephen, C.; Wilbur, J. CHAPTER 15: Putting the hardest to reach at the heart of the Sustainable Development Goals. In Sustainable Sanitation for All; Bongartz, P., Vernon, N., Fox, J., Eds.; Practical Action Publishing: Rugby, UK, 2016; pp. 245–266. ISBN 9781780449272. [Google Scholar]
- O’Reilly, K. Combining sanitation and women’s participation in water supply: An example from Rajasthan. Dev. Pract. 2010, 20, 45–46. [Google Scholar] [CrossRef]
- Burt, Z.; Nelson, K.L.; Ray, I. Towards Gender Equality Through Sanitation Access; UN Women Discussion Papers; UN Women: Berkeley, CA, 2016. [Google Scholar]
- Plan Uganda. Research on the Impact of Gender on Community-Led Total Sanitation Processes; Plan Uganda: Kampala, Uganda, 2012. [Google Scholar]
- Cameron, L.A.; Olivia, S.; Shah, M. Initial Conditions Matter: Social Capital and Participatory Development. SSRN Electron. J. 2015, 35. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Category | Outcomes/Conditions | Scale | Cambodia Definitions | Ghana Definitions |
|---|---|---|---|---|
| Category 1: Community Leadership | Commune Engagement | Four-point | Level of engagement of commune Council members in sanitation at the community level post-triggering. | N/A (no communes in Ghana) |
| Traditional Leader Pressure (Cambodia)/Traditional Leader Engagement (Ghana) | Four-point | Intensity of pressure applied by community leaders to households post-triggering (includes Community Chief, Deputy Chief, or Community Focal Point) | Activity level of traditional leaders, namely Community Chiefs, in sanitation activities post-triggering. | |
| Natural Leader Engagement | Four-point | N/A (no natural leaders in Cambodia) | Activity level of natural leaders in sanitation activities post-triggering. | |
| Category 2: Follow-up Activities | NGO (Cambodia)/ CLTS Facilitator follow-up (Ghana) | Four-point | Intensity of follow-up by NGOs post-triggering. (Not limited to CLTS implementing partner.) | Intensity of follow-up by CLTS facilitators or other external actors post-triggering. |
| Internal follow-up post-ODF (Ghana) | Four-point | N/A (This condition was dropped due to insufficient variability) | Activity level of natural leaders or traditional leaders, or both, post-ODF (at the time of the research). | |
| Category 3: Financial/ Pro-poor Support | Financial Support | Four-point | Amount of financial support, such as subsidies, latrine materials or loans, received by the community (pre- or post-ODF; does not include sanitation marketing offers of low-cost latrines). | N/A (This condition was dropped due to insufficient variability) |
| Pro-poor support (Cambodia)/ Internal Support (Ghana) | Four-point | Extent to which financial support or other strategies were intentionally targeted to poor or vulnerable households. | Level of engagement of community members in sanitation activities, including supporting neighbors to construct latrines, or ensuring that poor and vulnerable households were supported. | |
| Subsidies before triggering | Binary | Presence of subsidies prior to CLTS activities in the community. | N/A (no communities had received previous subsidies) | |
| Other | Women engaged in sanitation | Four-point | N/A (This condition was dropped due to insufficient variability) | Engagement of women in sanitation activities such as triggering, the decision to construct latrines, maintaining latrines over time, or in leadership positions (i.e., natural leaders). |
| Outcomes | Outcome 1: Current Latrine Coverage | Continuous | Current number of latrines divided by number of households. | Current number of latrines divided by number of compounds (In Ghana, a compound is grouping of households; the number of households per compound varied per community.). |
| Outcome 2: Consistent Latrine Use | Four-point | Prevailing latrine use behaviors in the community compared to open defecation behaviors. | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tribbe, J.; Zuin, V.; Delaire, C.; Khush, R.; Peletz, R. How Do Rural Communities Sustain Sanitation Gains? Qualitative Comparative Analyses of Community-Led Approaches in Cambodia and Ghana. Sustainability 2021, 13, 5440. https://doi.org/10.3390/su13105440
Tribbe J, Zuin V, Delaire C, Khush R, Peletz R. How Do Rural Communities Sustain Sanitation Gains? Qualitative Comparative Analyses of Community-Led Approaches in Cambodia and Ghana. Sustainability. 2021; 13(10):5440. https://doi.org/10.3390/su13105440
Chicago/Turabian StyleTribbe, Jessica, Valentina Zuin, Caroline Delaire, Ranjiv Khush, and Rachel Peletz. 2021. "How Do Rural Communities Sustain Sanitation Gains? Qualitative Comparative Analyses of Community-Led Approaches in Cambodia and Ghana" Sustainability 13, no. 10: 5440. https://doi.org/10.3390/su13105440