
Infrared Thermography for Measuring Elevated Body Temperature: Clinical Accuracy, Calibration, and Evaluation

 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Experimental Setup and Temperature Measurement Procedure
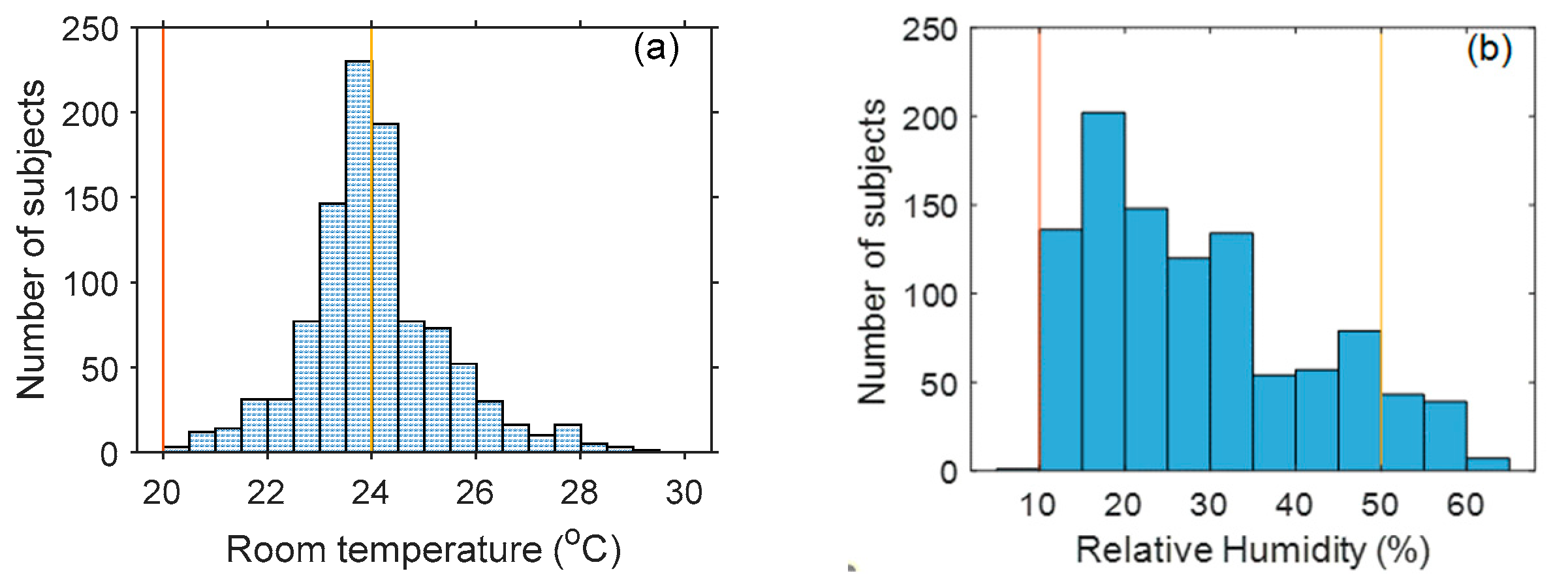
2.2. Subject Demographics
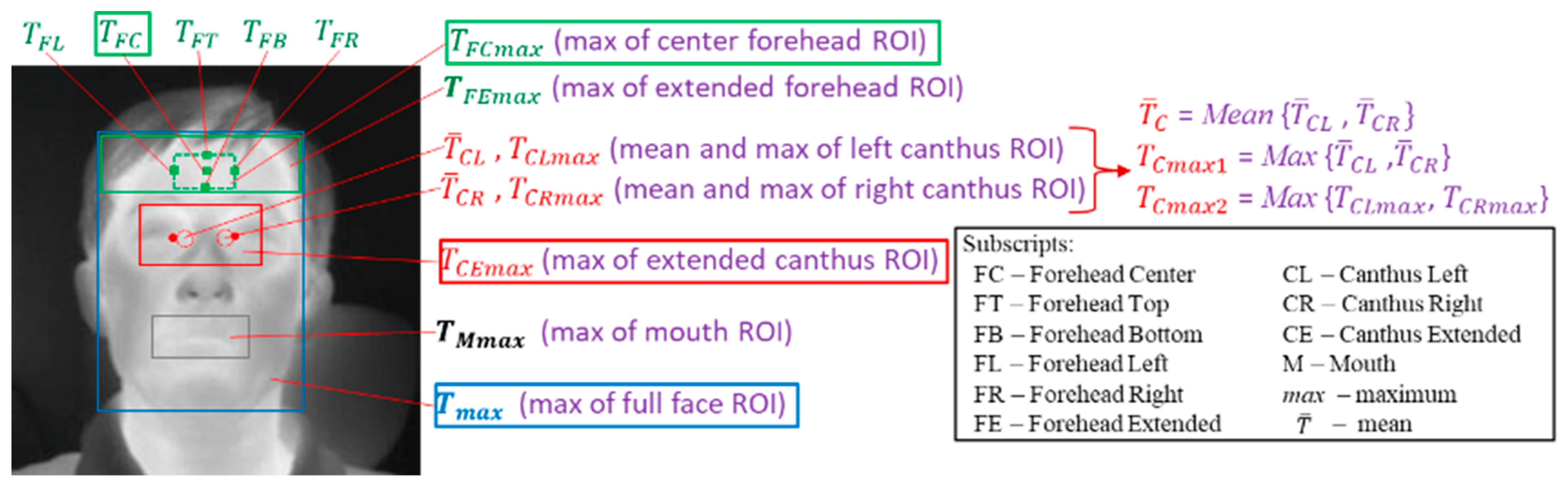
2.3. Facial Region Delineation and Temperature Measurement
2.4. Clinical Data
2.5. Regression Methods for Imputing Oral Temperature
2.6. Clinical Accuracy Assessment
2.6.1. Metrics for Temperature Measurement Accuracy
2.6.2. Metrics for Diagnostic Performance
3. Results
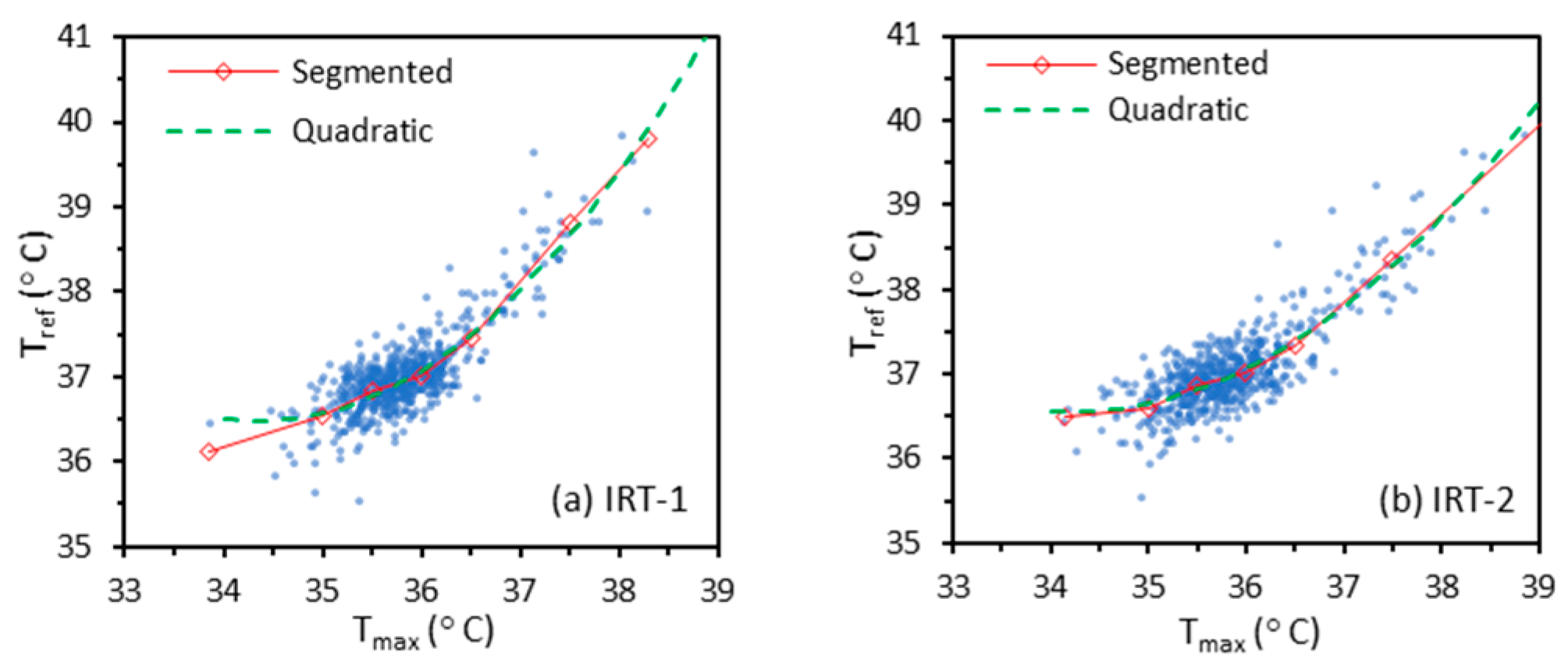
3.1. Regression Methods for Calibration
3.2. Temperature Measurement Accuracy—Quantitative Analysis
3.3. Temperature Measurement Accuracy—Graphical Analysis
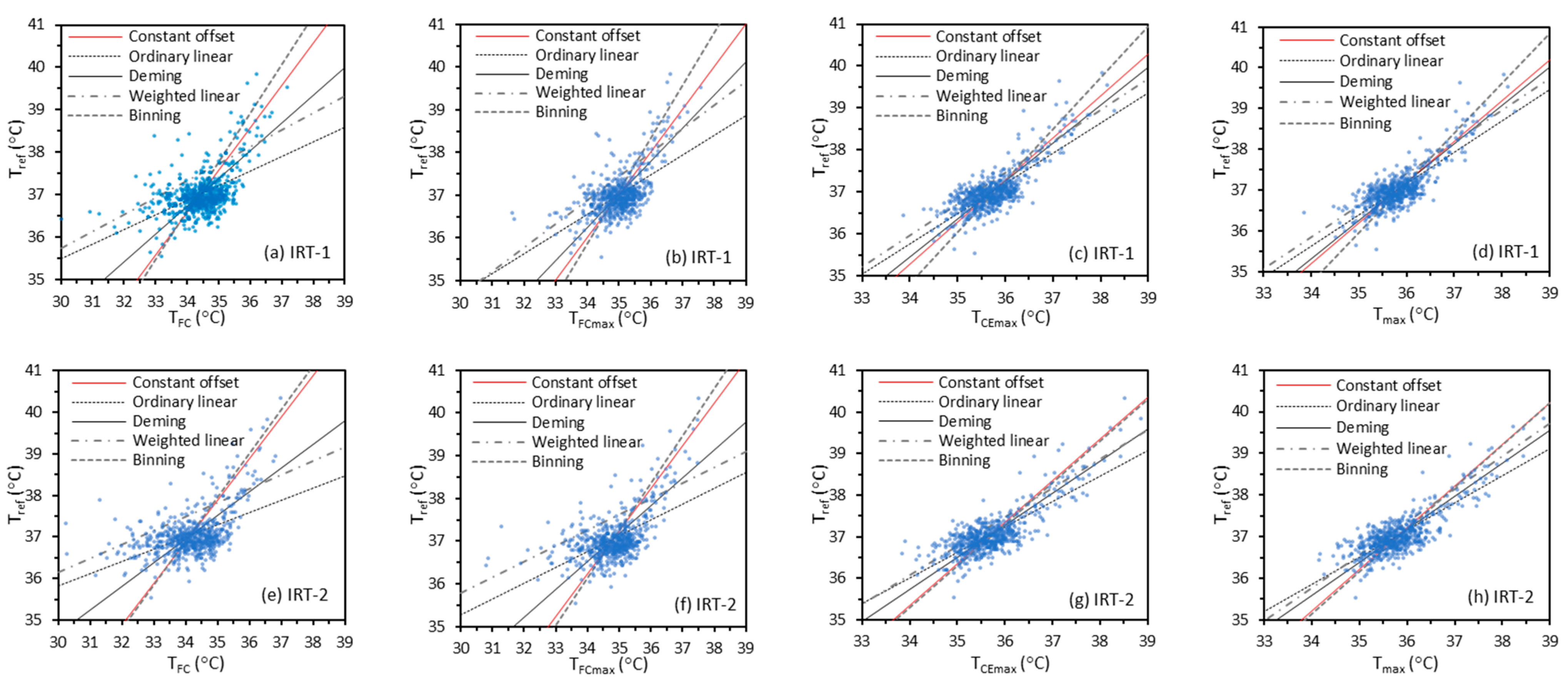
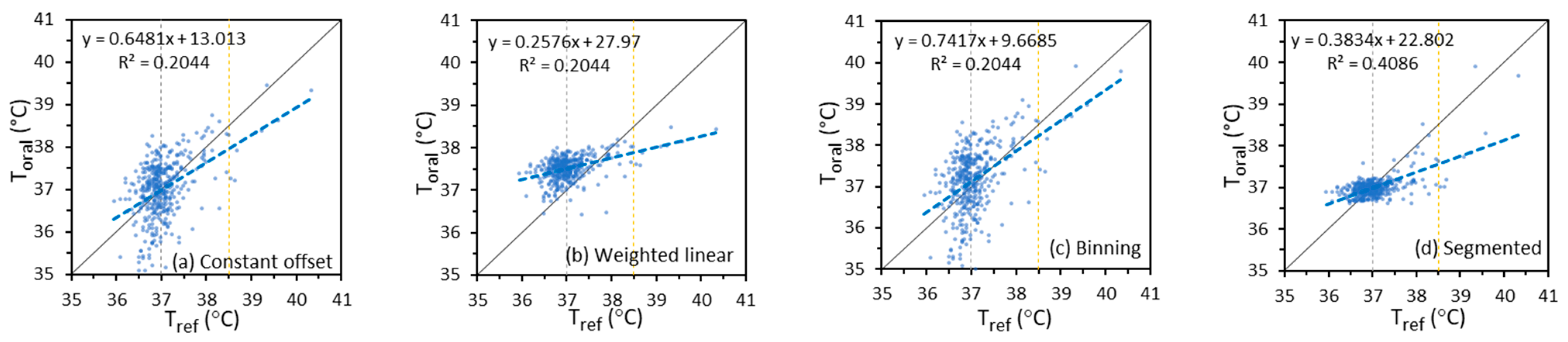
3.3.1. Scatter Plots
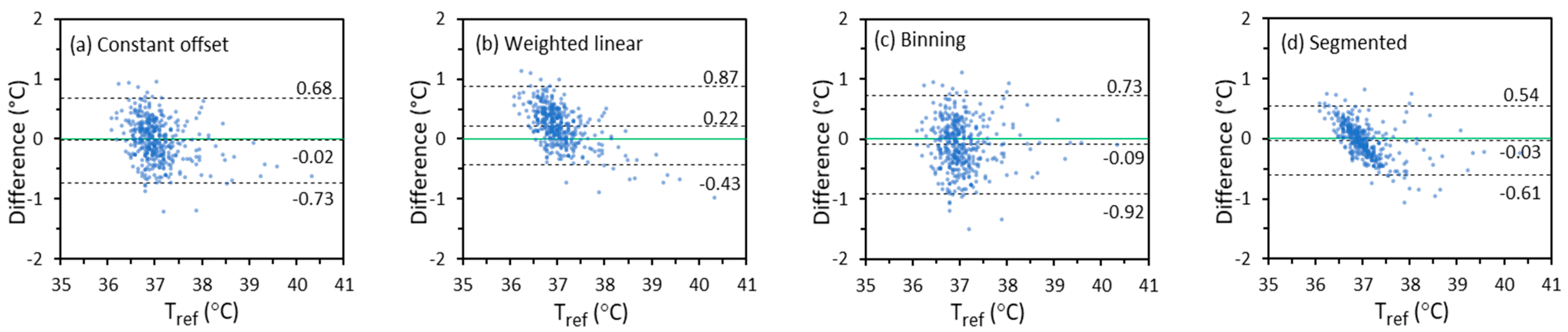
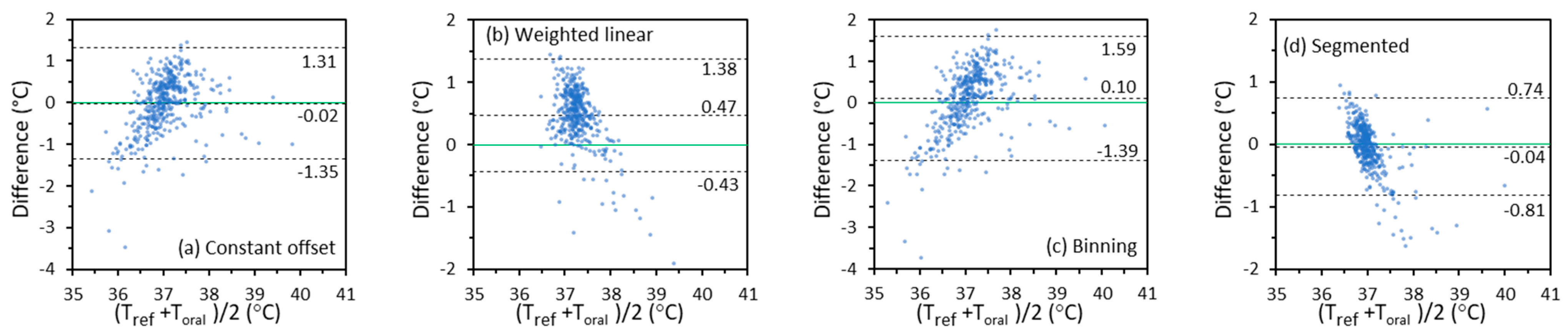
3.3.2. Difference Plots
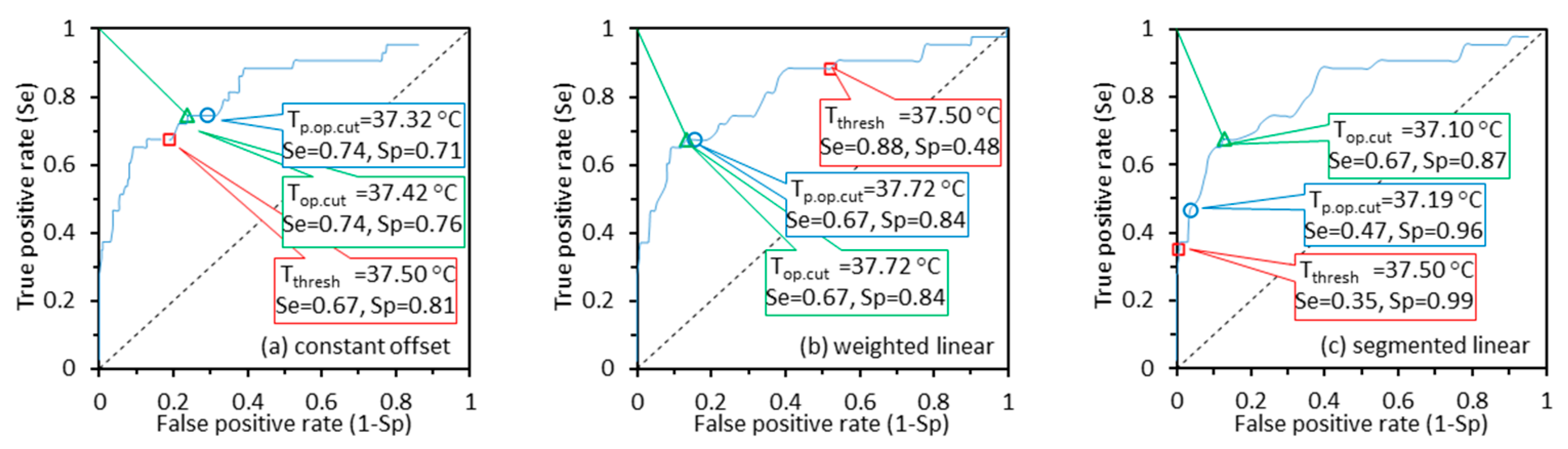
3.4. Diagnostic Performance
3.5. Clinical Accuracy—IRTs Versus NCITs
3.5.1. Direct Performance Comparison
3.5.2. Indirect Comparison Based on Imaging Results
4. Discussion
4.1. Effects of Regression Methods on the Clinical Accuracy
4.2. Metrics and Requirements for Evaluating Clinical Accuracy
4.3. Difference Plot Methods
4.4. Performance Comparison of IRTs and NCITs
4.5. Study Challenges and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Disclaimer
Appendix A. Additional Data for Based on Forehead Temperatures

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Offset | Ordinary | Weighted | Segmented | Deming | Binning | Offset | Ordinary | Weighted | Segmented | Deming | Binning | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| All | −0.02 | −0.02 | 0.47 | −0.04 | −0.02 | 0.10 | −0.03 | −0.02 | 0.41 | −0.04 | −0.03 | 0.07 | |
| Tref | 0.67 | 0.45 | 0.45 | 0.39 | 0.51 | 0.75 | 0.55 | 0.43 | 0.44 | 0.37 | 0.48 | 0.66 | |
| 0.66 | 0.45 | 0.65 | 0.39 | 0.51 | 0.75 | 0.55 | 0.43 | 0.60 | 0.37 | 0.48 | 0.66 | ||
| Tref< | 0.12 | 0.21 | 0.70 | 0.18 | 0.17 | 0.21 | 0.10 | 0.19 | 0.61 | 0.16 | 0.14 | 0.17 | |
| 37 °C | 0.63 | 0.26 | 0.28 | 0.22 | 0.42 | 0.72 | 0.52 | 0.27 | 0.31 | 0.21 | 0.41 | 0.64 | |
| 0.64 | 0.33 | 0.75 | 0.28 | 0.45 | 0.75 | 0.53 | 0.33 | 0.68 | 0.27 | 0.43 | 0.66 | ||
| 37 °C≤ | −0.18 | −0.28 | 0.22 | −0.31 | −0.24 | −0.04 | −0.19 | −0.27 | 0.18 | −0.29 | −0.22 | −0.05 | |
| Tref | 0.66 | 0.34 | 0.35 | 0.30 | 0.46 | 0.75 | 0.53 | 0.32 | 0.34 | 0.31 | 0.42 | 0.65 | |
| ≤38.5 °C | 0.68 | 0.44 | 0.41 | 0.43 | 0.51 | 0.75 | 0.56 | 0.42 | 0.39 | 0.42 | 0.48 | 0.65 | |
| Tref> | −0.87 | −1.71 | −1.15 | −1.10 | −1.32 | −0.56 | −0.96 | −1.61 | −1.06 | −0.93 | −1.23 | −0.57 | |
| 38.5 °C | 0.46 | 0.38 | 0.36 | 0.74 | 0.32 | 0.56 | 0.43 | 0.34 | 0.32 | 0.64 | 0.33 | 0.58 | |
| 0.97 | 1.75 | 1.20 | 1.30 | 1.35 | 0.77 | 1.04 | 1.64 | 1.10 | 1.11 | 1.27 | 0.79 | ||
| 0.20 | 0.07 | 0.08 | 0.08 | 0.13 | 0.23 | 0.18 | 0.08 | 0.10 | 0.08 | 0.14 | 0.22 | ||
| Se | 0.67 | 0.14 | 0.88 | 0.35 | 0.58 | 0.74 | 0.67 | 0.33 | 0.86 | 0.42 | 0.58 | 0.72 | |
| Sp | 0.82 | 1.00 | 0.48 | 0.99 | 0.92 | 0.72 | 0.87 | 1.00 | 0.62 | 0.99 | 0.94 | 0.78 | |
| 0.37 | 0.86 | 0.53 | 0.65 | 0.43 | 0.38 | 0.35 | 0.67 | 0.41 | 0.58 | 0.42 | 0.36 | ||
| Offset | Ordinary | Weighted | Segmented | Deming | Binning | Offset | Ordinary | Weighted | Segmented | Deming | Binning | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| All | 0.14 | 0.07 | 0.58 | 0.04 | 0.10 | 0.19 | 0.06 | 0.05 | 0.56 | 0.02 | 0.05 | 0.07 | |
| Tref | 0.70 | 0.43 | 0.43 | 0.40 | 0.48 | 0.73 | 0.57 | 0.40 | 0.40 | 0.36 | 0.44 | 0.63 | |
| 0.71 | 0.43 | 0.72 | 0.40 | 0.49 | 0.76 | 0.58 | 0.40 | 0.69 | 0.36 | 0.44 | 0.63 | ||
| Tref< | 0.23 | 0.27 | 0.77 | 0.22 | 0.25 | 0.26 | 0.14 | 0.24 | 0.75 | 0.18 | 0.19 | 0.13 | |
| 37 °C | 0.65 | 0.25 | 0.27 | 0.23 | 0.39 | 0.68 | 0.53 | 0.24 | 0.24 | 0.22 | 0.36 | 0.59 | |
| 0.69 | 0.37 | 0.82 | 0.31 | 0.46 | 0.73 | 0.55 | 0.34 | 0.79 | 0.28 | 0.40 | 0.60 | ||
| 37 °C≤ | 0.01 | −0.21 | 0.31 | −0.24 | −0.12 | 0.07 | −0.06 | −0.21 | 0.31 | −0.24 | −0.14 | −0.03 | |
| Tref | 0.76 | 0.37 | 0.38 | 0.37 | 0.49 | 0.80 | 0.63 | 0.35 | 0.35 | 0.35 | 0.45 | 0.69 | |
| ≤38.5 °C | 0.76 | 0.42 | 0.49 | 0.44 | 0.50 | 0.80 | 0.63 | 0.41 | 0.47 | 0.43 | 0.47 | 0.69 | |
| Tref> | 0.06 | −1.33 | −0.75 | −0.23 | −0.79 | 0.21 | −0.04 | −1.22 | −0.71 | −0.34 | −0.69 | 0.17 | |
| 38.5 °C | 0.71 | 0.19 | 0.20 | 1.24 | 0.34 | 0.76 | 0.51 | 0.15 | 0.15 | 0.82 | 0.26 | 0.59 | |
| 0.67 | 1.35 | 0.77 | 1.18 | 0.85 | 0.74 | 0.48 | 1.23 | 0.72 | 0.84 | 0.73 | 0.58 | ||
| 0.22 | 0.06 | 0.07 | 0.08 | 0.13 | 0.23 | 0.20 | 0.07 | 0.07 | 0.08 | 0.13 | 0.22 | ||
| Se | 0.70 | 0.26 | 0.86 | 0.33 | 0.60 | 0.74 | 0.74 | 0.35 | 0.88 | 0.37 | 0.60 | 0.74 | |
| Sp | 0.75 | 1.00 | 0.35 | 0.99 | 0.90 | 0.73 | 0.84 | 0.99 | 0.40 | 0.99 | 0.93 | 0.82 | |
| 0.39 | 0.74 | 0.67 | 0.67 | 0.41 | 0.37 | 0.30 | 0.65 | 0.61 | 0.63 | 0.40 | 0.31 | ||



References
- Chiu, W.; Lin, P.; Chiou, H.; Lee, W.; Lee, C.; Yang, Y.; Lee, H.; Hsieh, M.; Hu, C.; Ho, Y. Infrared thermography to mass-screen suspected SARS patients with fever. Asia-Pac. J. Public Health 2005, 17, 26–28. [Google Scholar] [CrossRef]
- Nishiura, H.; Kamiya, K. Fever screening during the influenza (H1N1-2009) pandemic at Narita International Airport, Japan. BMC Infect. Dis. 2011, 11, 111. [Google Scholar] [CrossRef] [Green Version]
- Shi, H.; Han, X.; Jiang, N.; Cao, Y.; Alwalid, O.; Gu, J.; Fan, Y.; Zheng, C. Radiological findings from 81 patients with COVID-19 pneumonia in Wuhan, China: A descriptive study. Lancet Infect. Dis. 2020, 20, 425–434. [Google Scholar] [CrossRef]
- Yang, X.; Yu, Y.; Xu, J.; Shu, H.; Liu, H.; Wu, Y.; Zhang, L.; Yu, Z.; Fang, M.; Yu, T. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: A single-centered, retrospective, observational study. Lancet Respir. Med. 2020, 8, 475–481. [Google Scholar] [CrossRef] [Green Version]
- Goeijenbier, M.; Van Kampen, J.; Reusken, C.; Koopmans, M.; Van Gorp, E. Ebola virus disease: A review on epidemiology, symptoms, treatment and pathogenesis. Neth. J. Med. 2014, 72, 442–448. [Google Scholar]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Schuchat, A.; Covid, C.; Team, R. Public health response to the initiation and spread of pandemic COVID-19 in the United States, February 24–April 21, 2020. Morb. Mortal. Weekly Rep. 2020, 69, 551. [Google Scholar] [CrossRef] [PubMed]
- Widmaier, E.P.; Raff, H.; Strang, K.T. Regulation of Organic Metabolism and Energy Balance-Section B: Regulation of Total-Body Energy Balance and Temperature. In Vander’s Human Physiology; McGraw-Hill: New York, NY, USA, 2008; pp. 583–596. [Google Scholar]
- Lu, S.-H.; Dai, Y.-T. Normal body temperature and the effects of age, sex, ambient temperature and body mass index on normal oral temperature: A prospective, comparative study. Int. J. Nurs. Stud. 2009, 46, 661–668. [Google Scholar] [CrossRef]
- Kessel, L.; Johnson, L.; Arvidsson, H.; Larsen, M. The relationship between body and ambient temperature and corneal temperature. Investig. Ophthalmol. Vis. Sci. 2010, 51, 6593–6597. [Google Scholar] [CrossRef]
- Reilly, T.; Brooks, G. Exercise and the circadian variation in body temperature measures. Int. J. Sports Med. 1986, 7, 358–362. [Google Scholar] [CrossRef]
- Landsberg, L.; Young, J.B.; Leonard, W.R.; Linsenmeier, R.A.; Turek, F.W. Is obesity associated with lower body temperatures? Core temperature: A forgotten variable in energy balance. Metabolism 2009, 58, 871–876. [Google Scholar] [CrossRef] [PubMed]
- Bailey, S.L.; Heitkemper, M.M. Circadian rhythmicity of cortisol and body temperature: Morningness-eveningness effects. Chronobiol. Int. 2001, 18, 249–261. [Google Scholar] [CrossRef] [PubMed]
- Conroy, D.A.; Spielman, A.J.; Scott, R.Q. Daily rhythm of cerebral blood flow velocity. J. Circadian Rhythm. 2005, 3, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blatteis, C.M. Age-dependent changes in temperature regulation–A mini review. Gerontology 2012, 58, 289–295. [Google Scholar] [CrossRef] [PubMed]
- Moghissi, K.S.; Syner, F.N.; Evans, T.N. A composite picture of the menstrual cycle. Am. J. Obstet. Gynecol. 1972, 114, 405–418. [Google Scholar] [CrossRef]
- Chiappini, E.; Sollai, S.; Longhi, R.; Morandini, L.; Laghi, A.; Osio, C.E.; Persiani, M.; Lonati, S.; Picchi, R.; Bonsignori, F. Performance of non-contact infrared thermometer for detecting febrile children in hospital and ambulatory settings. J. Clin. Nurs. 2011, 20, 1311–1318. [Google Scholar] [CrossRef]
- Teran, C.; Torrez-Llanos, J.; Teran-Miranda, T.; Balderrama, C.; Shah, N.; Villarroel, P. Clinical accuracy of a non-contact infrared skin thermometer in paediatric practice. Child Care Health Dev. 2011, 38, 471–476. [Google Scholar] [CrossRef]
- Ng, E.Y.K.; Acharya, R.U. Remote-sensing infrared thermography. IEEE Eng. Med. Biol. Mag. 2009, 28, 76–83. [Google Scholar] [CrossRef]
- Bitar, D.; Goubar, A.; Desenclos, J. International travels and fever screening during epidemics: A literature review on the effectiveness and potential use of non-contact infrared thermometers. Eurosurveillance 2009, 14, 19115. [Google Scholar] [CrossRef]
- Selent, M.U.; Molinari, N.M.; Baxter, A.; Nguyen, A.V.; Siegelson, H.; Brown, C.M.; Plummer, A.; Higgins, A.; Podolsky, S.; Spandorfer, P.; et al. Mass screening for fever in children: A comparison of 3 infrared thermal detection systems. Pediatr. Emerg. Care 2013, 29, 305–313. [Google Scholar] [CrossRef]
- Tay, M.; Low, Y.; Zhao, X.; Cook, A.; Lee, V. Comparison of Infrared Thermal Detection Systems for mass fever screening in a tropical healthcare setting. Public Health 2015, 129, 1471–1478. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.-C.; Chang, R.-E.; Chang, W.-C. Limitations of forehead infrared body temperature detection for fever screening for severe acute respiratory syndrome. Infect. Control Hosp. Epidemiol. 2004, 25, 1109–1111. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, A.V.; Cohen, N.J.; Lipman, H.; Brown, C.M.; Molinari, N.A.; Jackson, W.L.; Kirking, H.; Szymanowski, P.; Wilson, T.W.; Salhi, B.A.; et al. Comparison of 3 infrared thermal detection systems and self-report for mass fever screening. Emerg. Infect. Dis. 2010, 16, 1710–1717. [Google Scholar] [CrossRef]
- Chan, L.; Lo, J.L.; Kumana, C.R.; Cheung, B.M. Utility of infrared thermography for screening febrile subjects. Hong Kong Med. J. 2013, 19, 109–115. [Google Scholar]
- Hewlett, A.L.; Kalil, A.C.; Strum, R.A.; Zeger, W.G.; Smith, P.W. Evaluation of an infrared thermal detection system for fever recognition during the H1N1 influenza pandemic. Infect. Control Hosp. Epidemiol. 2011, 32, 504–506. [Google Scholar] [CrossRef]
- Priest, P.C.; Duncan, A.R.; Jennings, L.C.; Baker, M.G. Thermal Image Scanning for Influenza Border Screening: Results of an Airport Screening Study. PLoS ONE 2011, 6, e14490. [Google Scholar] [CrossRef] [Green Version]
- Cho, K.S.; Yoon, J. Fever screening and detection of febrile arrivals at an international airport in Korea: Association among self-reported fever, infrared thermal camera scanning, and tympanic temperature. Epidemiol. Health 2014, 36, e2014004. [Google Scholar] [CrossRef] [Green Version]
- Mouchtouri, V.A.; Christoforidou, E.P.; Lemos, C.M.; Fanos, M.; Rexroth, U.; Grote, U.; Belfroid, E.; Swaan, C.; Hadjichristodoulou, C. Exit and entry screening practices for infectious diseases among travelers at points of entry: Looking for evidence on public health impact. Int. J. Env. Res. Public Health 2019, 16, 4638. [Google Scholar] [CrossRef] [Green Version]
- IEC & ISO. IEC 80601-2-59: Medical Electrical Equipment-Part 2-59: Particular Requirements for the Basic Safety and Essential Performance of Screening Thermographs for Human Febrile Temperature Screening; International Electrotechnical Commission, International Organization for Standardization: Geneva, Switzerland, 2017. [Google Scholar]
- ISO. ISO/TR 13154: Medical Electrical Equipment—Deployment, Implementation and Operational Guidelines for Identifying Febrile Humans Using a Screening Thermograph; International Organization for Standardization: Geneva, Switzerland, 2017. [Google Scholar]
- Ghassemi, P.; Pfefer, T.J.; Casamento, J.P.; Simpson, R.; Wang, Q. Best practices for standardized performance testing of infrared thermographs intended for fever screening. PLoS ONE 2018, 13, e0203302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- ASTM. ASTM E1965-98: Standard Specification for Infrared Thermometers for Intermittent Determination of Patient Temperature; ASTM Committee E20 on Temperature Measurement: West Conshohocken, PA, USA, 2016; p. 19428. [Google Scholar]
- ISO. ISO 80601-2-56: Medical Electrical Equipment-Part 2-56: Particular Requirements for Basic Safety and Essential Performance of Clinical Thermometers for Body Temperature Measurement; International Organization for Standardization: Geneva, Switzerland, 2017. [Google Scholar]
- Brengelmann, G. Dilemma of body temperature measurement. In Man in Stressful Environments: Thermal and Work Physiology; Shiraki, K., Yousef, M., Eds.; Charles C. Thomas: Springfield, IL, USA, 1987; pp. 5–22. [Google Scholar]
- Moran, D.S.; Mendal, L. Core temperature measurement. Sports Med. 2002, 32, 879–885. [Google Scholar] [CrossRef] [PubMed]
- Yetman, R.J.; Coody, D.K.; West, M.S.; Montgomery, D.; Brown, M. Comparison of temperature measurements by an aural infrared thermometer with measurements by traditional rectal and axillary techniques. J. Pediatr. 1993, 122, 769–773. [Google Scholar] [CrossRef]
- Doezema, D.; Lunt, M.; Tandberg, D. Cerumen occlusion lowers infrared tympanic membrane temperature measurement. Acad. Emerg. Med. 1995, 2, 17–19. [Google Scholar] [CrossRef]
- Mairiaux, P.; Sagot, J.; Candas, V. Oral temperature as an index of core temperature during heat transients. Eur. J. Appl. Physiol. Occup. Physiol. 1983, 50, 331–341. [Google Scholar] [CrossRef]
- Geneva, I.I.; Cuzzo, B.; Fazili, T.; Javaid, W. Normal body temperature: A systematic review. Open Forum Infect. Dis. 2019, 6, ofz032. [Google Scholar] [CrossRef]
- Zhou, Y.; Ghassemi, P.; Chen, M.; McBride, D.; Casamento, J.P.; Pfefer, T.J.; Wang, Q. Clinical evaluation of fever-screening thermography: Impact of consensus guidelines and facial measurement location. J. Biomed. Opt. 2020, 25, 097002. [Google Scholar] [CrossRef]
- Purslow, C. Clinical Implications for Thermography in the Eye World: A short History of Clinical Ocular Thermography. In Image Modeling of the Human Eye; Acharya, U.R., Ng, Y.K.E., Suri, J.S., Eds.; Artech House: New York, NY, USA, 2008; pp. 301–315. [Google Scholar]
- Steketee, J. Spectral emissivity of skin and pericardium. Phys. Med. Biol. 1973, 18, 686. [Google Scholar] [CrossRef]
- Tkáčová, M.; Živčák, J.; Foffová, P. A Reference for Human Eye Surface Temperature Measurements in Diagnostic Process of Ophthalmologic Diseases. In Proceedings of the Measurement 2011, Smolenice, Slovakia, 27–30 April 2011; pp. 406–409. [Google Scholar]
- Sullivan, S.J.L.; Rinaldi, J.E.; Hariharan, P.; Casamento, J.P.; Baek, S.; Seay, N.; Vesnovsky, O.; Topoleski, L.D.T. Clinical Evaluation of Non-Contact Infrared Thermometers. Res. Sq. 2021, 11, 22079. [Google Scholar] [CrossRef]
- Chenna, Y.N.D.; Ghassemi, P.; Pfefer, T.J.; Casamento, J.; Wang, Q. Free-form deformation approach for registration of visible and infrared facial images in fever screening. Sensors 2018, 18, 125. [Google Scholar] [CrossRef] [Green Version]
- Ng, D.K.; Chan, C.-H.; Chow, P.-Y.; Kwok, K.-L. Infrared ear thermometry. Br. J. Gen. Pract. 2004, 54, 869. [Google Scholar] [PubMed]
- Mercer, J.B.; Ring, E.F.J. Fever screening and infrared thermal imaging: Concerns and guidelines. Thermol. Int. 2009, 19, 67–69. [Google Scholar]
- Del Bene, V.E. Temperature. In Clinical Methods: The History, Physical, and Laboratory Examinations; Walker, H.K., Hall, W.D.H., Hurst, J.W., Eds.; Butterworth Publishers, a Division of Reed Publishing: Boston, MA, USA, 1990; pp. 990–993. [Google Scholar]
- Clinical and Laboratory Standards Institute. EP09c: Measurement Procedure Comparison and Bias Estimation Using Patient Samples; Clinical and Laboratory Standards Institute: Wayne, PA, USA, 2018. [Google Scholar]
- ISO. ISO 80601-2-61: Medical Electrical Equipment—Part 2-61: Particular Requirements for Basic Safety and Essential Performance of Pulse Oximeter Equipment; International Organization for Standardization: Geneva, Switzerland, 2017. [Google Scholar]
- Kumar, R.; Indrayan, A. Receiver operating characteristic (ROC) curve for medical researchers. Indian Pediatr. 2011, 48, 277–287. [Google Scholar] [CrossRef] [PubMed]
- Hanley, J.A.; McNeil, B.J. The meaning and use of the area under a receiver operating characteristic (ROC) curve. Radiology 1982, 143, 29–36. [Google Scholar] [CrossRef] [Green Version]
- Bland, J.M.; Altman, D.G. Comparing methods of measurement: Why plotting difference against standard method is misleading. Lancet 1995, 346, 1085–1087. [Google Scholar] [CrossRef] [Green Version]
- Centers for Disease Control and Prevention. Non-Contact Temperature Measurement Devices: Considerations for Use in Port of Entry Screening Activities; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2014. [Google Scholar]
- Sullivan, S.J.; Seay, N.; Zhu, L.; Rinaldi, J.E.; Hariharan, P.; Vesnovsky, O.; Topoleski, L.T. Performance characterization of non-contact infrared thermometers (NCITs) for forehead temperature measurement. Med. Eng. Phys. 2021, 93, 93–99. [Google Scholar] [CrossRef]
- Fletcher, T.; Whittam, A.; Simpson, R.; Machin, G. Comparison of non-contact infrared skin thermometers. J. Med. Eng. Technol. 2018, 42, 65–71. [Google Scholar] [CrossRef]
- ASTM. In ASTM E1112-00: Standard Specification for Electronic Thermometer for Intermittent Determination of Patient Temperature; ASTM Committee F04 on Medical and Surgical Materials and Devices: West Conshohocken, PA, USA, 2011; p. 19428.
- Giavarina, D. Understanding bland altman analysis. Biochem. Med. Biochem. Med. 2015, 25, 141–151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krouwer, J.S. Why Bland–Altman plots should use X, not (Y + X)/2 when X is a reference method. Stat. Med. 2008, 27, 778–780. [Google Scholar] [CrossRef]
- Usamentiaga, R.; Venegas, P.; Guerediaga, J.; Vega, L.; Molleda, J.; Bulnes, F.G. Infrared thermography for temperature measurement and non-destructive testing. Sensors 2014, 14, 12305–12348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- FDA. Enforcement Policy for Telethermographic Systems During the Coronavirus Disease 2019 (COVID-19) Public Health Emergency; FDA: Silver Spring, MD, USA, 2020. Available online: https://www.fda.gov/media/137079/download (accessed on 29 October 2021).
- Cheung, B.; Chan, L.; Lauder, I.; Kumana, C. Detection of body temperature with infrared thermography: Accuracy in detection of fever. Hong Kong Med. J. 2012, 18 (Suppl. 3), 31–34. [Google Scholar]
- Simpson, R.; Machin, G.; McEvoy, H.; Rusby, R. Traceability and calibration in temperature measurement: A clinical necessity. J. Med. Eng. Technol. 2006, 30, 212–217. [Google Scholar] [CrossRef]
- Charles, A.C.; Janet, C.Z.; Joseph, M.R.; Martin, C.M.-E.; Elliot, D.W. Timing of REM sleep is coupled to the circadian rhythm of body temperature in man. Sleep 1980, 2, 329–346. [Google Scholar] [CrossRef] [Green Version]
- Harding, C.; Pompei, F.; Bordonaro, S.F.; McGillicuddy, D.C.; Burmistrov, D.; Sanchez, L.D. Fevers Are Rarest in the Morning: Could We Be Missing Infectious Disease Cases by Screening for Fever Then? medRxiv 2020. [Google Scholar] [CrossRef]
- Denoble, A.E.; Hall, N.; Pieper, C.F.; Kraus, V.B. Patellar skin surface temperature by thermography reflects knee osteoarthritis severity. Clin. Med. Insights. Arthritis Musculoskelet. Disord. 2010, 3, 69. [Google Scholar] [CrossRef] [Green Version]
- Martinez-Jimenez, M.A.; Loza-Gonzalez, V.M.; Kolosovas-Machuca, E.S.; Yanes-Lane, M.E.; Ramirez-GarciaLuna, A.S.; Ramirez-GarciaLuna, J.L. Diagnostic accuracy of infrared thermal imaging for detecting covid-19 infection in minimally symptomatic patients. Eur. J. Clin. Investig. 2020, 51, e13474. [Google Scholar] [CrossRef] [PubMed]









| IRT-1 | IRT-2 | ||||
|---|---|---|---|---|---|
| Subjects | % | Subjects | % | ||
| Female | 606 | 59.41 | 601 | 59.50 | |
| Male | 414 | 40.59 | 409 | 40.50 | |
| Age | 18–20 | 534 | 52.35 | 527 | 52.18 |
| 21–30 | 432 | 42.35 | 429 | 42.48 | |
| 31–40 | 31 | 3.04 | 31 | 3.07 | |
| 41–50 | 9 | 0.88 | 9 | 0.89 | |
| 51–60 | 11 | 1.08 | 11 | 1.09 | |
| >60 | 3 | 0.29 | 3 | 0.30 | |
| Ethnicity | White | 506 | 49.61 | 500 | 49.50 |
| Black/African-American | 143 | 14.02 | 143 | 14.16 | |
| Hispanic/Latino | 57 | 5.59 | 55 | 5.45 | |
| Asian | 260 | 25.49 | 258 | 25.54 | |
| Multiracial | 50 | 4.90 | 50 | 4.95 | |
| American Indian | 4 | 0.39 | 4 | 0.40 | |
| > 37.5 °C | 111 | 10.88 | 111 | 10.99 | |
| Ambient Temperature (°C) | Relative Humidity | Subject # for IRT-1 | Subject # for IRT-2 | |
|---|---|---|---|---|
| Group 1 [41] | 20–24 | 10–62% (7.5% subject data in the 50–62% range) | 544 | 540 |
| Group 2 | 24–29 | 10–62% (9.9% subject data in the 50–62% range) | 476 | 470 |
| Forehead | Inner Canthi | Mouth | Face | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Group 1 [41] | IRT-1 | 0.46 | 0.41 | 0.49 | 0.47 | 0.43 | 0.55 | 0.63 | 0.60 | 0.58 | 0.63 | 0.65 | 0.70 | 0.71 | 0.73 | 0.75 | 0.60 | 0.78 |
| IRT-2 | 0.46 | 0.39 | 0.49 | 0.46 | 0.41 | 0.54 | 0.62 | 0.53 | 0.51 | 0.56 | 0.59 | 0.70 | 0.69 | 0.73 | 0.76 | 0.60 | 0.79 | |
| Group 2 | IRT-1 | 0.50 | 0.37 | 0.52 | 0.46 | 0.43 | 0.56 | 0.60 | 0.62 | 0.61 | 0.65 | 0.66 | 0.74 | 0.75 | 0.77 | 0.79 | 0.69 | 0.81 |
| IRT-2 | 0.50 | 0.37 | 0.53 | 0.46 | 0.42 | 0.57 | 0.61 | 0.63 | 0.56 | 0.62 | 0.65 | 0.73 | 0.72 | 0.76 | 0.80 | 0.69 | 0.82 | |
| Forehead | Inner Canthi | Mouth | Face | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Group 1 [41] | IRT-1 | 0.82 | 0.79 | 0.82 | 0.80 | 0.81 | 0.84 | 0.86 | 0.88 | 0.87 | 0.88 | 0.88 | 0.94 | 0.93 | 0.94 | 0.95 | 0.89 | 0.95 |
| IRT-2 | 0.82 | 0.79 | 0.82 | 0.79 | 0.79 | 0.84 | 0.87 | 0.91 | 0.87 | 0.90 | 0.92 | 0.95 | 0.93 | 0.94 | 0.95 | 0.88 | 0.97 | |
| Group 2 | IRT-1 | 0.82 | 0.76 | 0.82 | 0.80 | 0.78 | 0.85 | 0.87 | 0.93 | 0.91 | 0.93 | 0.93 | 0.97 | 0.96 | 0.97 | 0.97 | 0.91 | 0.97 |
| IRT-2 | 0.82 | 0.76 | 0.82 | 0.78 | 0.79 | 0.84 | 0.85 | 0.94 | 0.88 | 0.92 | 0.94 | 0.96 | 0.94 | 0.97 | 0.97 | 0.90 | 0.97 | |
| Offset | Ordinary | Deming | Weighted | Binning | Segmented | Offset | Ordinary | Deming | Weighted | Binning | Segmented | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| All | −0.03 | −0.03 | −0.03 | 0.21 | −0.13 | −0.03 | −0.02 | −0.02 | −0.02 | 0.22 | −0.09 | −0.03 | |
| Tref | 0.40 | 0.35 | 0.37 | 0.35 | 0.47 | 0.30 | 0.35 | 0.33 | 0.34 | 0.33 | 0.41 | 0.29 | |
| 0.40 | 0.35 | 0.37 | 0.41 | 0.49 | 0.30 | 0.35 | 0.33 | 0.34 | 0.39 | 0.42 | 0.29 | ||
| Tref< | 0.05 | 0.11 | 0.07 | 0.34 | −0.10 | 0.10 | 0.05 | 0.10 | 0.07 | 0.34 | −0.06 | 0.10 | |
| 37 °C | 0.37 | 0.29 | 0.34 | 0.29 | 0.45 | 0.22 | 0.33 | 0.27 | 0.32 | 0.27 | 0.40 | 0.21 | |
| 0.38 | 0.30 | 0.35 | 0.45 | 0.46 | 0.24 | 0.34 | 0.29 | 0.32 | 0.44 | 0.41 | 0.23 | ||
| 37°C≤ | −0.14 | −0.19 | −0.16 | 0.05 | −0.19 | −0.21 | −0.12 | −0.17 | −0.13 | 0.08 | −0.14 | −0.20 | |
| Tref | 0.40 | 0.30 | 0.36 | 0.30 | 0.50 | 0.30 | 0.35 | 0.28 | 0.33 | 0.29 | 0.43 | 0.28 | |
| ≤38.5 °C | 0.42 | 0.35 | 0.39 | 0.31 | 0.53 | 0.37 | 0.37 | 0.33 | 0.35 | 0.30 | 0.45 | 0.35 | |
| Tref> | −0.42 | −0.91 | −0.58 | −0.62 | −0.12 | −0.39 | −0.49 | −0.87 | −0.58 | −0.61 | −0.18 | −0.39 | |
| 38.5 °C | 0.26 | 0.24 | 0.24 | 0.23 | 0.36 | 0.35 | 0.23 | 0.22 | 0.22 | 0.22 | 0.31 | 0.36 | |
| 0.48 | 0.93 | 0.62 | 0.65 | 0.36 | 0.51 | 0.53 | 0.90 | 0.62 | 0.65 | 0.34 | 0.52 | ||
| 0.11 | 0.08 | 0.10 | 0.09 | 0.14 | 0.07 | 0.18 | 0.14 | 0.17 | 0.14 | 0.22 | 0.13 | ||
| Offset | Ordinary | Deming | Weighted | Binning | Segmented | Offset | Ordinary | Deming | Weighted | Binning | Segmented | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| All | 0.02 | 0.03 | 0.03 | 0.25 | −0.03 | 0.02 | 0.01 | 0.02 | 0.02 | 0.19 | −0.04 | 0.01 | |
| Tref | 0.42 | 0.32 | 0.35 | 0.33 | 0.42 | 0.29 | 0.38 | 0.31 | 0.32 | 0.32 | 0.39 | 0.27 | |
| 0.42 | 0.32 | 0.35 | 0.41 | 0.42 | 0.29 | 0.38 | 0.31 | 0.32 | 0.37 | 0.39 | 0.27 | ||
| Tref< | 0.06 | 0.15 | 0.11 | 0.35 | 0.00 | 0.15 | 0.05 | 0.14 | 0.10 | 0.27 | −0.01 | 0.14 | |
| 37 °C | 0.44 | 0.29 | 0.35 | 0.32 | 0.44 | 0.23 | 0.39 | 0.27 | 0.32 | 0.32 | 0.40 | 0.22 | |
| 0.44 | 0.33 | 0.37 | 0.47 | 0.44 | 0.27 | 0.40 | 0.30 | 0.34 | 0.42 | 0.40 | 0.26 | ||
| 37 °C≤ | −0.05 | −0.14 | −0.10 | 0.10 | −0.10 | −0.20 | −0.05 | −0.14 | −0.10 | 0.06 | −0.10 | −0.19 | |
| Tref | 0.38 | 0.26 | 0.30 | 0.28 | 0.38 | 0.23 | 0.35 | 0.25 | 0.28 | 0.28 | 0.35 | 0.22 | |
| ≤38.5 °C | 0.38 | 0.29 | 0.31 | 0.29 | 0.40 | 0.30 | 0.35 | 0.28 | 0.30 | 0.28 | 0.37 | 0.29 | |
| Tref> | 0.25 | −0.58 | −0.25 | −0.17 | 0.21 | −0.09 | 0.14 | −0.57 | −0.28 | −0.13 | 0.11 | −0.19 | |
| 38.5 °C | 0.39 | 0.22 | 0.28 | 0.25 | 0.39 | 0.47 | 0.36 | 0.21 | 0.27 | 0.26 | 0.37 | 0.38 | |
| 0.44 | 0.62 | 0.36 | 0.29 | 0.42 | 0.45 | 0.36 | 0.61 | 0.38 | 0.28 | 0.36 | 0.41 | ||
| 0.15 | 0.09 | 0.11 | 0.10 | 0.15 | 0.07 | 0.22 | 0.15 | 0.18 | 0.18 | 0.23 | 0.12 | ||
| Offset | Ordinary | Deming | Weighted | Binning | Segmented | Offset | Ordinary | Deming | Weighted | Binning | Segmented | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Se | 0.73 | 0.61 | 0.73 | 0.89 | 0.73 | 0.61 | 0.74 | 0.60 | 0.71 | 0.88 | 0.76 | 0.55 | |
| IRT-1 | Sp | 0.94 | 0.97 | 0.95 | 0.87 | 0.94 | 0.97 | 0.94 | 0.98 | 0.95 | 0.89 | 0.93 | 0.99 |
| 0.28 | 0.39 | 0.28 | 0.18 | 0.28 | 0.39 | 0.27 | 0.41 | 0.29 | 0.17 | 0.25 | 0.45 | ||
| Se | 0.84 | 0.68 | 0.75 | 0.86 | 0.84 | 0.66 | 0.81 | 0.67 | 0.77 | 0.84 | 0.79 | 0.58 | |
| IRT-2 | Sp | 0.91 | 0.98 | 0.96 | 0.85 | 0.94 | 0.99 | 0.94 | 0.99 | 0.97 | 0.89 | 0.95 | 0.99 |
| 0.18 | 0.32 | 0.25 | 0.20 | 0.17 | 0.34 | 0.20 | 0.33 | 0.23 | 0.20 | 0.22 | 0.42 | ||
| Standards | Devices (Required Minimum Display Range) | Maximum Permissible Errors, in Specific Temperature Ranges | Accuracy Type (Laboratory/Clinical) | Note |
|---|---|---|---|---|
| IEC 80601-2-59: 2017 [30] | IRTs (None) | ±0.5 °C, 34.0–39.0 °C. | Laboratory | Errors from all the test devices are combined. |
| ISO 80601-2-56: 2017 [34] | clinical thermometers (34.0–43.0 °C) | ±0.3 °C, withing the rated output range; ±0.4 °C, withing the rated extended output range. | Laboratory | This standard is under revision for improvement. |
| ASTM E1112-00: 2011 [58] | electronic thermometers (35.5–41.0 °C) | ±0.3 °C, < 35.8 °C; ±0.2 °C, 35.8–37.0 °C; ±0.1 °C, 37.0–39.0 °C; ±0.2 °C, 39.0–41.0 °C; ±0.3 °C, > 41.0 °C. | Not clear | |
| ASTM E1965-98: 2016 [33] | IR thermometers (Ear canal: 34.4–42.2 °C; Skin: 22.0–40.0 °C) | For ear canal IR thermometers: ±0.3 °C, < 36.0 °C; ±0.2 °C, 36.0–39.0 °C; ±0.3 °C, > 39.0 °C. For skin IR thermometers: ±0.3 °C, over the display range. | Laboratory |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, Q.; Zhou, Y.; Ghassemi, P.; McBride, D.; Casamento, J.P.; Pfefer, T.J. Infrared Thermography for Measuring Elevated Body Temperature: Clinical Accuracy, Calibration, and Evaluation. Sensors 2022, 22, 215. https://doi.org/10.3390/s22010215
Wang Q, Zhou Y, Ghassemi P, McBride D, Casamento JP, Pfefer TJ. Infrared Thermography for Measuring Elevated Body Temperature: Clinical Accuracy, Calibration, and Evaluation. Sensors. 2022; 22(1):215. https://doi.org/10.3390/s22010215
Chicago/Turabian StyleWang, Quanzeng, Yangling Zhou, Pejman Ghassemi, David McBride, Jon P. Casamento, and T. Joshua Pfefer. 2022. "Infrared Thermography for Measuring Elevated Body Temperature: Clinical Accuracy, Calibration, and Evaluation" Sensors 22, no. 1: 215. https://doi.org/10.3390/s22010215