Clinical Evaluation of Respiratory Rate Measurements on COPD (Male) Patients Using Wearable Inkjet-Printed Sensor

 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
2. Methodology
2.1. Ethical Approval
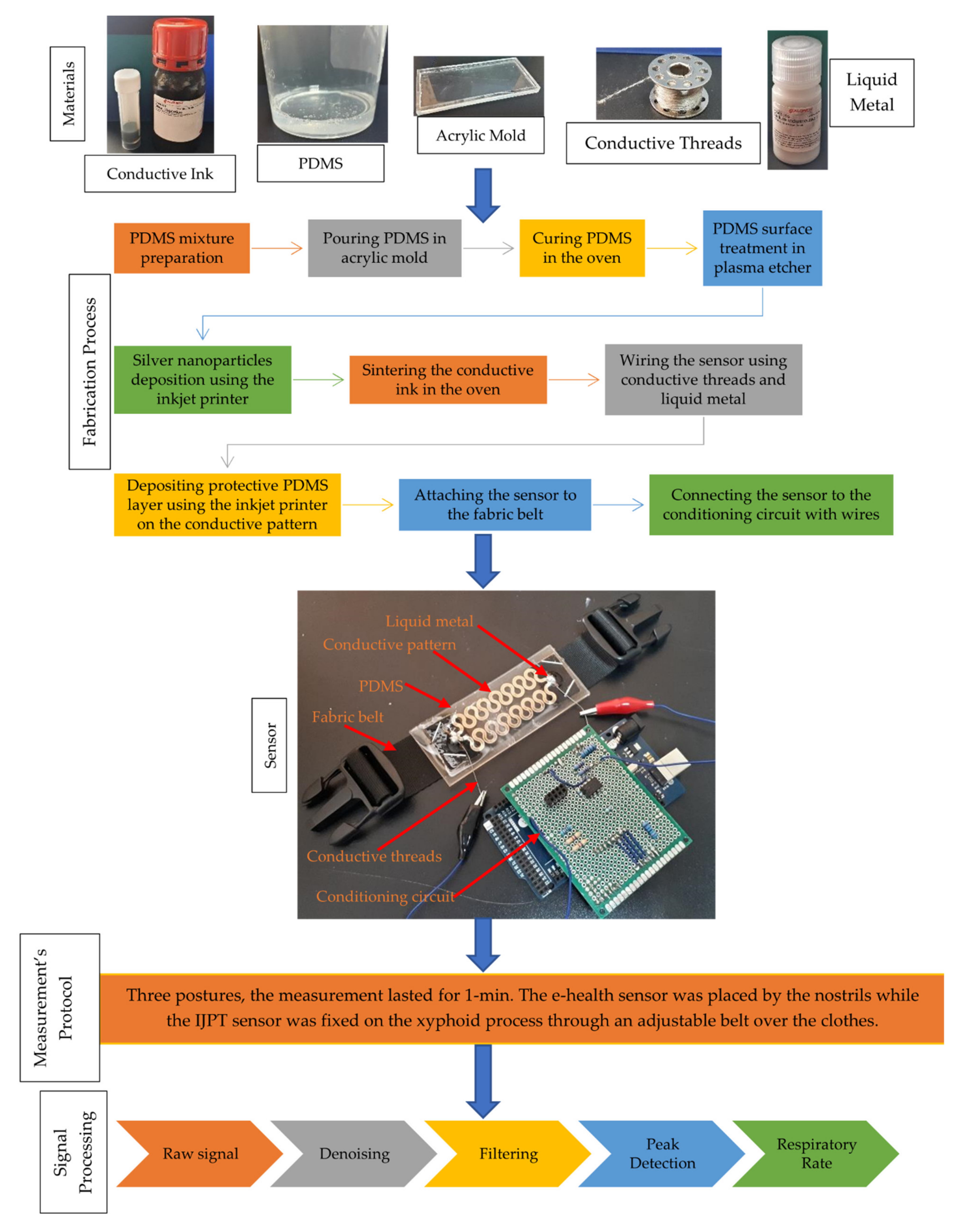
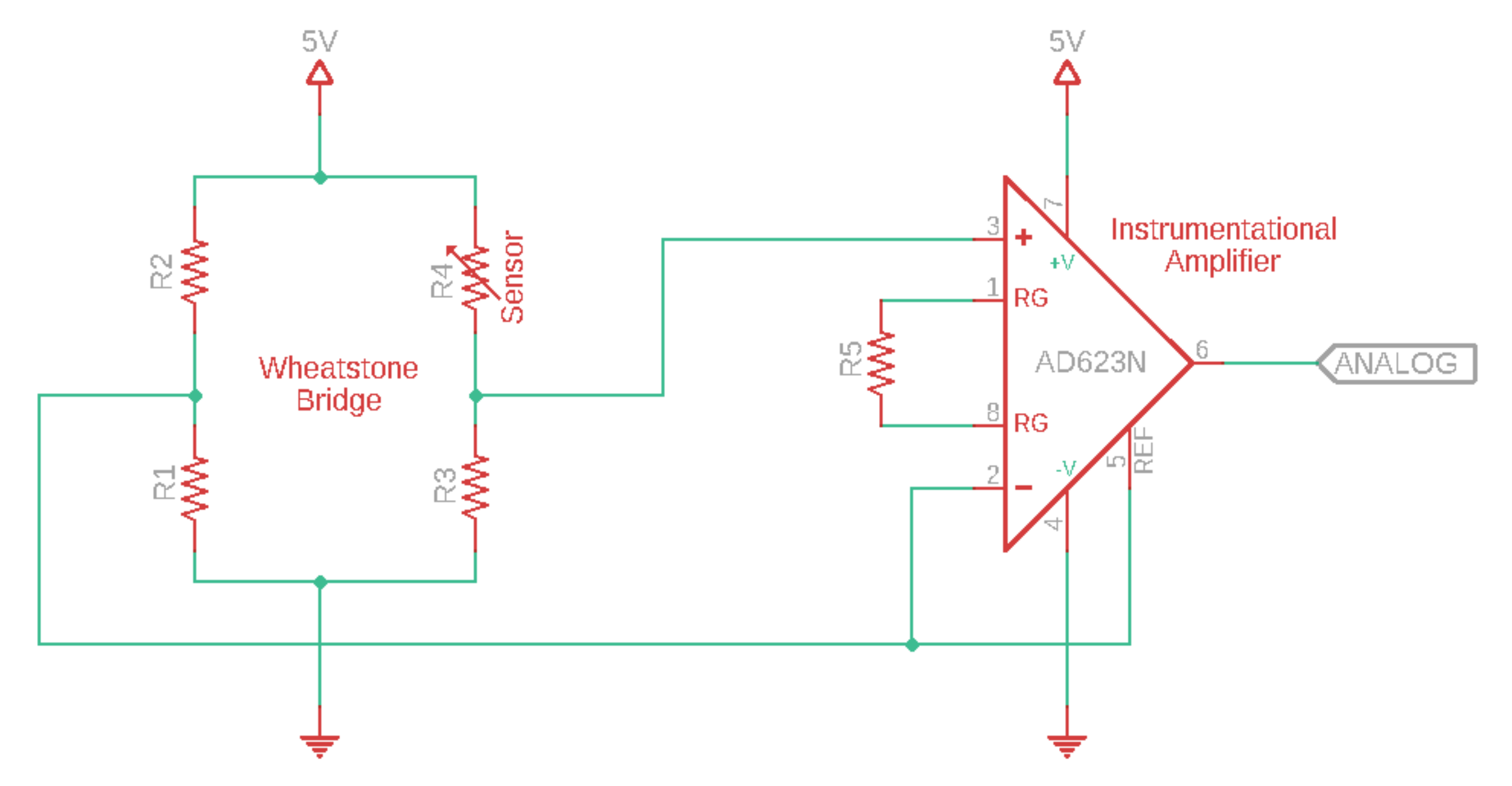
2.2. Inkjet-Printed RR Sensor
2.3. Measurements Protocol
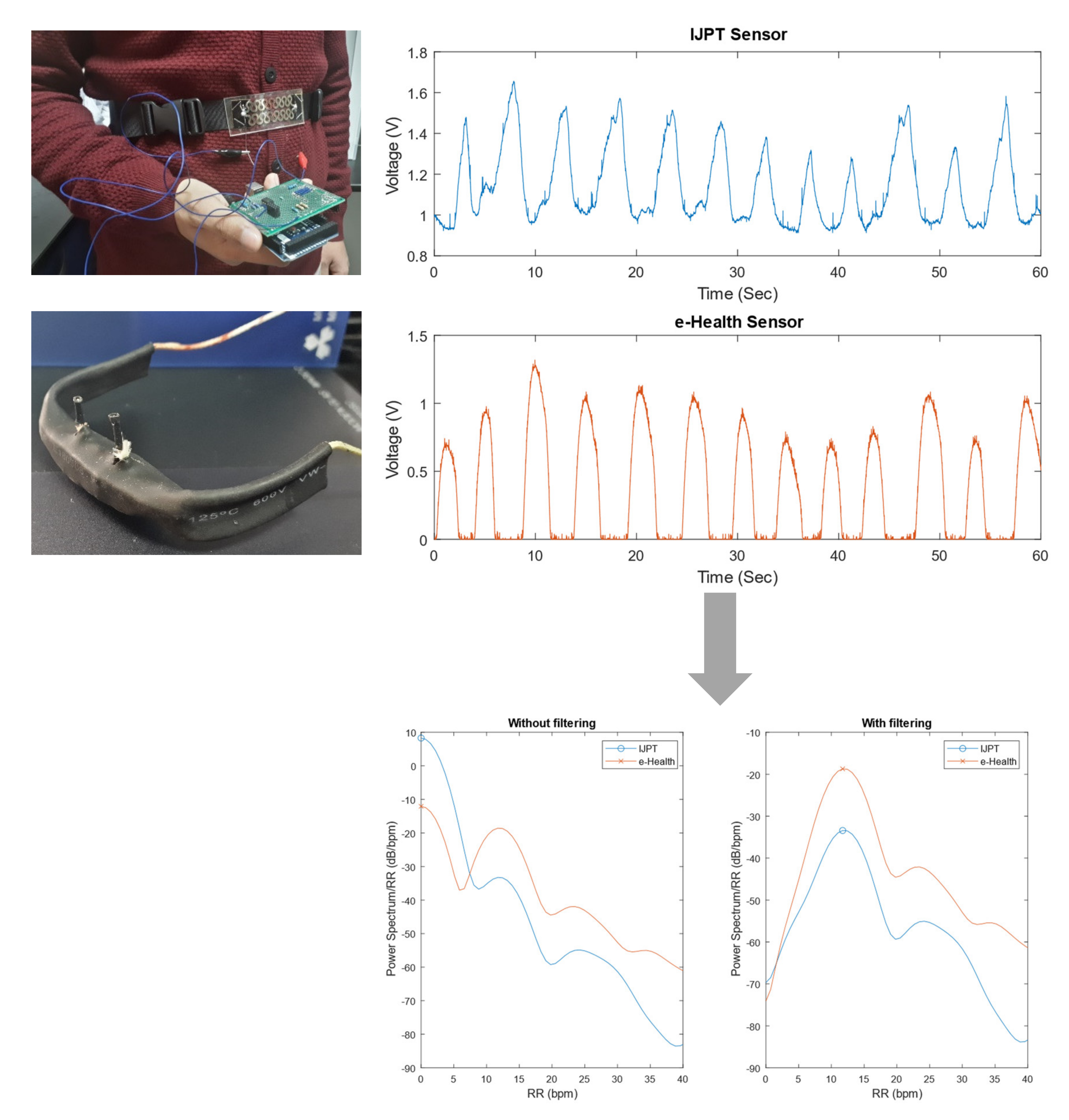
2.4. Respiration Rate Derivation
2.5. Statistical Analysis
2.5.1. Data Cleaning
2.5.2. Comparison of RR Values
2.5.3. Analysis of Errors of RR
2.5.4. Analysis of Relative Errors of RR
2.5.5. Bland-Altman Analysis
2.5.6. Regression Analysis
3. Results
3.1. Comparison of RR Values
3.2. Analysis of Errors of RR
3.3. Analysis of Relative Errors of RR
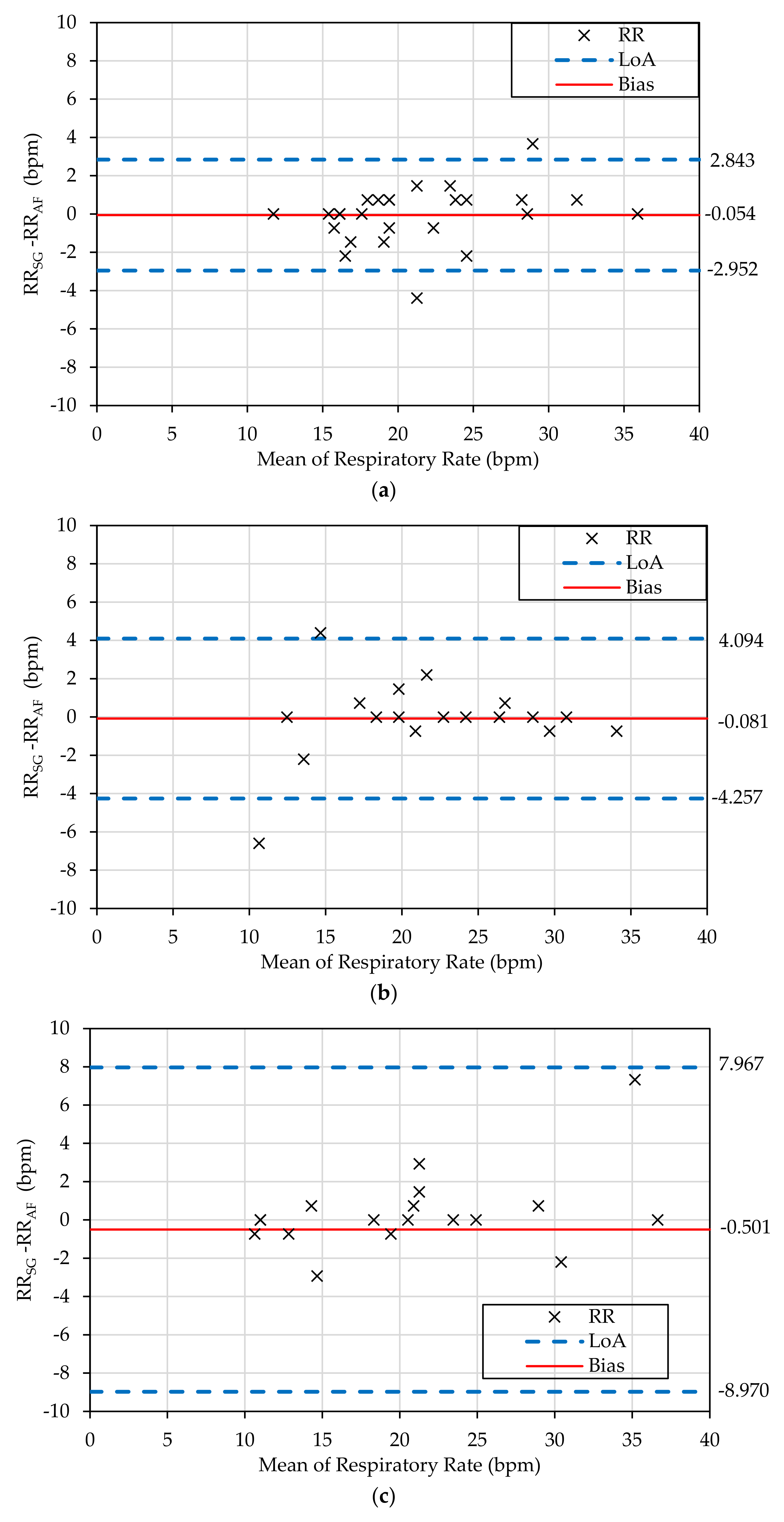
3.4. Bland-Altman Analysis
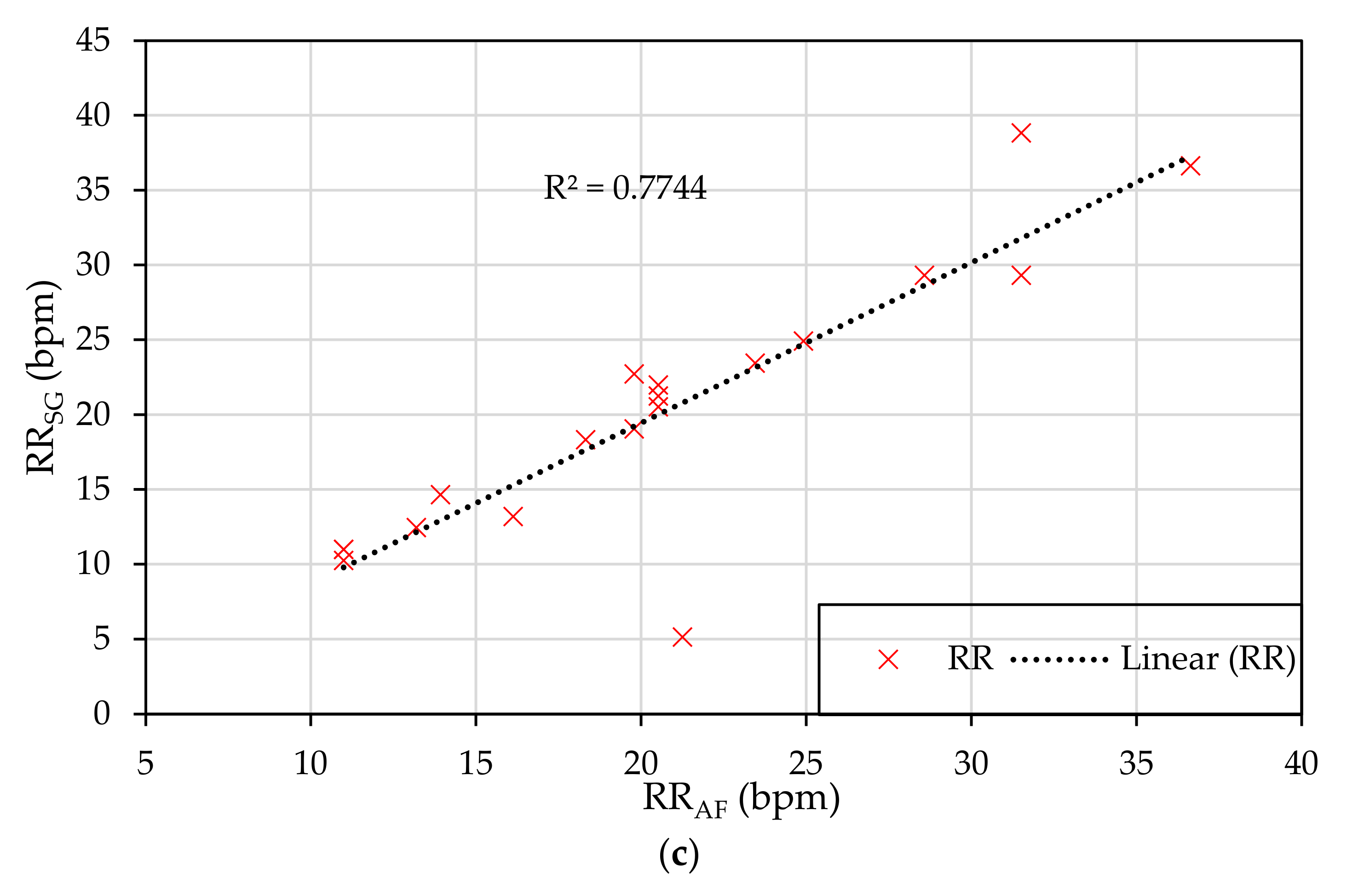
3.5. Regression Analysis
4. Discussion
4.1. Measurement of RR on COPD Patients: Difficulties and Approaches
4.2. Accuracy of IJPT Sensor: Comparison with Other Sensors
4.3. Applications of IJPT Sensor
4.4. Limitations and Future Work
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Ethical Statements
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient | Age | Gender | Height (m) | Weight (kg) | Smoking Status | GOLD Diagnosis | First Diagnosed |
|---|---|---|---|---|---|---|---|
| 1 | 50 | M | 169 | 62 | Ex-Smoker | 3 | 12/2018 |
| 2 | 51 | M | 170 | 71 | Smoker | 1 | 11/2001 |
| 3 | 46 | M | 174 | 83 | Ex-Smoker | 3 | 5/2010 |
| 4 | 30 | M | 180 | 62 | Smoker | 1 | N/A |
| 5 | 79 | M | 175 | 98 | Ex-Smoker | 2 | 4/2008 |
| 6 | 58 | M | 162 | 78 | Smoker | 3 | 4/2019 |
| 7 | 39 | M | 170 | 85 | Quit smoking | 2 | 11/2017 |
| 8 | 56 | M | 175 | 90 | Smoker | 1 | 8/2013 |
| 9 | 58 | M | 173 | 80 | Ex-Smoker | 2 | 2/2009 |
| 10 | 26 | M | 173 | 84 | Ex-Smoker | 1 | 8/2016 |
| 11 | 52 | M | 176 | 63 | Ex-Smoker | 2 | 2009 |
| 12 | 56 | M | 170 | 70 | Smoker | N/A | 2014 |
| 13 | 47 | M | 175 | 80 | Ex-smoking | 1 | 7/2018 |
| 14 | 52 | M | 168 | 80 | Smoker | 2 | 5/2007 |
| 15 | 24 | M | 173 | 63 | Smoker | 1 | 1/2020 |
| 16 | 42 | M | 164 | 85 | Smoker | 1 | 10/2014 |
| 17 | 60 | M | 178 | 84 | Smoker | 1 | 8/2019 |
| 18 | 42 | M | 165 | 75 | Smoker | 2 | 8/2014 |
| 19 | 49 | M | 167 | 64 | Smoker | 3 | 1/2020 |
| 20 | 37 | M | 172 | 98 | Smoker | 3 | 1/2020 |
| 21 | 57 | M | 167 | 60 | Smoker | 3 | 2/2020 |
| 22 | 70 | M | 160 | 50 | Smoker | 2 | 2/2020 |
| 23 | 66 | M | 179 | 77 | Smoker | 1 | 9/2013 |
| 24 | 67 | M | 175 | 70 | Ex-Smoker | 3 | 5/2001 |
| 25 | 55 | M | 167 | 58 | Quit smoking | 2 | 11/2019 |
| 26 | 69 | M | 175 | 88 | Ex-Smoker | 2 | N/A |
| 27 | 53 | F | 167 | 90 | Smoker | 1 | 2/2012 |
| 28 | 58 | M | 163 | 74 | Ex-Smoker | 1 | 1/2019 |
| 29 | 79 | M | 174 | 72 | Smoker | 3 | 8/2017 |
| 30 | 67 | M | 167 | 62 | Smoker | 2 | 8/2017 |
| 31 | 66 | M | 175 | 85 | Ex-Smoker | 1 | 6/2002 |
| 32 | 67 | M | 174 | 69 | Smoker | 3 | 6/2014 |
| 33 | 58 | M | 172 | 73 | Ex-Smoker | 3 | 3/2012 |
| 34 | 75 | M | 174 | 68 | Smoker | 1 | 11/2009 |
| 35 | 73 | M | 170 | 65 | Smoker | 1 | 7/2013 |
| Patient | Cough | Phlegm (mucus) | Tightness of Chest | Not Able to Climb a Flight of Stairs | Cannot Perform Home Activities | Can Go Out Anytime | Good Sleep | Having Energy |
|---|---|---|---|---|---|---|---|---|
| 1 | frequently | rare | never | always | rare | always | frequently | always |
| 2 | rare | rare | sometimes | always | never | always | frequently | rare |
| 3 | always | sometimes | sometimes | always | rare | never | sometimes | rare |
| 4 | rare | rare | frequently | frequently | never | always | frequently | always |
| 5 | always | sometimes | rare | frequently | frequently | rare | sometimes | rare |
| 6 | always | always | sometimes | sometimes | sometimes | always | sometimes | never |
| 7 | rare | rare | sometimes | rare | rare | rare | frequently | sometimes |
| 8 | frequently | sometimes | rare | sometimes | never | always | always | always |
| 9 | sometimes | rare | never | never | never | always | frequently | sometimes |
| 10 | never | never | never | never | never | always | frequently | always |
| 11 | rare | sometimes | never | rare | rare | frequently | frequently | sometimes |
| 12 | sometimes | sometimes | never | never | never | frequently | always | always |
| 13 | rare | sometimes | never | never | never | always | always | always |
| 14 | sometimes | never | never | rare | never | frequently | frequently | frequently |
| 15 | rare | never | never | never | never | always | always | always |
| 16 | sometimes | frequently | frequently | rare | rare | never | sometimes | frequently |
| 17 | rare | rare | rare | never | never | always | frequently | frequently |
| 18 | frequently | rare | sometimes | never | never | always | always | frequently |
| 19 | frequently | frequently | sometimes | sometimes | rare | frequently | sometimes | frequently |
| 20 | frequently | frequently | rare | always | always | sometimes | rare | frequently |
| 21 | frequently | rare | always | always | always | always | sometimes | rare |
| 22 | always | sometimes | sometimes | sometimes | sometimes | always | frequently | never |
| 23 | rare | never | never | never | never | always | frequently | frequently |
| 24 | sometimes | never | never | never | frequently | frequently | sometimes | always |
| 25 | sometimes | sometimes | frequently | always | always | sometimes | rare | never |
| 26 | sometimes | always | sometimes | frequently | frequently | sometimes | sometimes | frequently |
| 27 | frequently | rare | never | sometimes | sometimes | always | frequently | frequently |
| 28 | always | always | rare | rare | never | always | always | frequently |
| 29 | always | frequently | never | always | rare | frequently | rare | frequently |
| 30 | always | always | always | always | frequently | rare | rare | never |
| 31 | sometimes | never | sometimes | frequently | always | rare | frequently | rare |
| 32 | sometimes | never | never | rare | rare | frequently | always | always |
| 33 | frequently | always | never | sometimes | frequently | always | rare | sometimes |
| 34 | frequently | rare | rare | sometimes | never | always | sometimes | frequently |
| 35 | sometimes | rare | sometimes | sometimes | rare | sometimes | frequently | sometimes |
| Patient | Posture | RRSG (bpm) | RRAF (bpm) | Error (bpm) |
|---|---|---|---|---|
| 1 | Sitting | 28.57 | 28.57 | 0 |
| Standing | 30.77 | 30.77 | 0 | |
| 2 | Sitting | 19.05 | 18.32 | 0.73 |
| Standing | 20.51 | 19.05 | 1.46 | |
| Lying45° | 5.13 | 21.25 | −16.12 | |
| 3 | Sitting | 32.23 | 31.50 | 0.73 |
| Standing | 29.30 | 30.04 | −0.74 | |
| Lying45° | 29.30 | 31.50 | −2.2 | |
| 4 | Sitting | 18.32 | 17.58 | 0.74 |
| Standing | 7.33 | 13.92 | −6.59 | |
| Lying45° | 12.45 | 13.19 | −0.74 | |
| 5 | Sitting | 21.98 | 22.71 | −0.73 |
| Standing | 22.71 | 22.71 | 0 | |
| 6 | Sitting | 19.05 | 23.44 | −4.39 |
| 7 | Sitting | 15.38 | 17.58 | −2.2 |
| Standing | 22.71 | 20.51 | 2.2 | |
| 8 | Sitting | 30.77 | 27.11 | 3.66 |
| Standing | 18.32 | 18.32 | 0 | |
| 9 | Sitting | 11.72 | 11.72 | 0 |
| Standing | 12.45 | 12.45 | 0 | |
| Lying45° | 10.99 | 10.99 | 0 | |
| 10 | Sitting | 16.12 | 17.58 | −1.46 |
| Standing | 19.78 | 19.78 | 0 | |
| 11 | Sitting | 19.05 | 19.78 | −0.73 |
| 12 | Sitting | 18.32 | 19.78 | −1.46 |
| Standing | 24.18 | 24.18 | 0 | |
| Lying45° | 14.65 | 13.92 | 0.73 | |
| 13 | Sitting | 16.12 | 16.12 | 0 |
| Lying45° | 10.99 | 10.99 | 0 | |
| 14 | Sitting | 23.44 | 25.64 | −2.2 |
| Standing | 20.51 | 21.25 | −0.74 | |
| 15 | Sitting | 21.98 | 20.51 | 1.47 |
| Lying45° | 19.05 | 19.78 | −0.73 | |
| 16 | Standing | 28.57 | 28.57 | 0 |
| Lying45° | 21.25 | 20.51 | 0.74 | |
| 17 | Lying45° | 13.19 | 16.12 | −2.93 |
| 18 | Sitting | 17.58 | 17.58 | 0 |
| 19 | Sitting | 16.12 | 16.12 | 0 |
| Standing | 16.85 | 12.45 | 4.4 | |
| Lying45° | 18.32 | 18.32 | 0 | |
| 20 | Sitting | 35.90 | 35.90 | 0 |
| Standing | 33.70 | 34.43 | −0.73 | |
| Lying45° | 36.63 | 36.63 | 0 | |
| 21 | Lying45° | 22.71 | 19.78 | 2.93 |
| 22 | Sitting | 28.57 | 27.84 | 0.73 |
| Lying45° | 24.91 | 24.91 | 0 | |
| 23 | Sitting | 24.91 | 24.18 | 0.73 |
| 24 | Sitting | 15.38 | 16.12 | −0.74 |
| Standing | 17.58 | 16.85 | 0.73 | |
| 25 | Lying45° | 23.44 | 23.44 | 0 |
| 26 | Lying45° | 21.98 | 20.51 | 1.47 |
| 27 | Sitting | 19.78 | 19.05 | 0.73 |
| Standing | 12.45 | 14.65 | −2.2 | |
| Lying45° | 10.26 | 10.99 | −0.73 | |
| 28 | Lying45° | 38.83 | 31.50 | 7.33 |
| 29 | Sitting | 15.38 | 15.38 | 0 |
| 30 | Sitting | 24.18 | 22.71 | 1.47 |
| 31 | Lying45° | 20.51 | 20.51 | 0 |
| 32 | Sitting | 19.78 | 19.05 | 0.73 |
| 33 | Sitting | 24.18 | 23.44 | 0.74 |
| Standing | 26.37 | 26.37 | 0 | |
| 34 | Lying45° | 29.30 | 28.57 | 0.73 |
| 35 | Sitting | 16.12 | 16.12 | 0 |
| Standing | 27.11 | 26.37 | 0.74 |
References
- Lucchini, M.; Pini, N.; Burtchen, N.; Signorini, M.G.; Fifer, W.P. Transfer Entropy Modeling of Newborn Cardiorespiratory Regulation. Front. Physiol. 2020, 11, 1095. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Chen, F.; Hartmann, V.; Khalid, S.G.; Hughes, S.; Zheng, D. Comparison of different modulations of photoplethysmography in extracting respiratory rate: From a physiological perspective. Physiol. Meas. 2020, 41, 094001. [Google Scholar] [CrossRef]
- Nicolò, A.; Massaroni, C.; Schena, E.; Sacchetti, M. The Importance of Respiratory Rate Monitoring: From Healthcare to Sport and Exercise. Sensors 2020, 20, 6396. [Google Scholar] [CrossRef]
- Flenady, T.; Dwyer, T.; Applegarth, J. Accurate respiratory rates count: So should you! Australas. Emerg. Nurs. J. 2017, 20, 45–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nicolò, A.; Marcora, S.M.; Sacchetti, M. Time to reconsider how ventilation is regulated above the respiratory compensation point during incremental exercise. J. Appl. Physiol. 2020, 128, 1447–1449. [Google Scholar] [CrossRef] [PubMed]
- Hill, B.; Annesley, S.H. Monitoring respiratory rate in adults. Br. J. Nurs. 2020, 29, 12–16. [Google Scholar] [CrossRef]
- Liu, H.; Allen, J.; Zheng, D.; Chen, F. Recent development of respiratory rate measurement technologies. Physiol. Meas. 2019, 40, 07TR01. [Google Scholar] [CrossRef] [Green Version]
- Nag, A.; Mukhopadhyay, S.C.; Kosel, J. Wearable Flexible Sensors: A Review. IEEE Sens. J. 2017, 17, 3949–3960. [Google Scholar] [CrossRef] [Green Version]
- Rodgers, M.M.; Pai, V.M.; Conroy, R.S. Recent advances in wearable sensors for health monitoring. IEEE Sens. J. 2015, 15, 3119–3126. [Google Scholar] [CrossRef]
- Yetisen, A.K.; Martinez-Hurtado, J.L.; Ünal, B.; Khademhosseini, A.; Butt, H. Wearables in Medicine. Adv. Mater. 2018, 30, e1706910. [Google Scholar] [CrossRef]
- Dittmar, A.; Meffre, R.; De Oliveira, F.; Gehin, C.; Delhomme, G. Wearable Medical Devices Using Textile and Flexible Technologies for Ambulatory Monitoring. In Proceedings of the 2005 IEEE Engineering in Medicine and Biology 27th Annual Conference, Shanghai, China, 1–4 September 2005; pp. 7161–7164. [Google Scholar]
- Khan, Y.; Ostfeld, A.E.; Lochner, C.M.; Pierre, A.; Arias, A.C. Monitoring of Vital Signs with Flexible and Wearable Medical Devices. Adv. Mater. 2016, 28, 4373–4395. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Wang, H.; Zhao, W.; Zhang, M.; Qin, H.; Xie, Y. Flexible, stretchable sensors for wearable health monitoring: Sensing mechanisms, materials, fabrication strategies and features. Sensors 2018, 18, 645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abu-khalaf, J.M.; Saraireh, R.; Eisa, S.M.; Al-halhouli, A. Experimental Characterization of Inkjet-Printed Stretchable Circuits for Wearable Sensor Applications. Sensors 2018, 18, 3476. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yilmaz, T.; Foster, R.; Hao, Y. Detecting vital signs with wearablewireless sensors. Sensors 2010, 10, 10837–10862. [Google Scholar] [CrossRef] [PubMed]
- Al-Halhouli, A.; Al-Ghussain, L.; El Bouri, S.; Liu, H.; Zheng, D. Fabrication and Evaluation of a Novel Non-Invasive Stretchable and Wearable Respiratory Rate Sensor Based on Silver Nanoparticles Using Inkjet Printing Technology. Polymers 2019, 11, 1518. [Google Scholar] [CrossRef] [Green Version]
- Al-Halhouli, A.; Al-Ghussain, L.; El Bouri, S.; Habash, F.; Liu, H.; Zheng, D. Clinical Evaluation of Stretchable and Wearable Inkjet-Printed Strain Gauge Sensor for Respiratory Rate Monitoring at Different Body Postures. Appl. Sci. 2020, 10, 480. [Google Scholar] [CrossRef] [Green Version]
- Nicolò, A.; Massaroni, C.; Passfield, L. Respiratory frequency during exercise: The neglected physiological measure. Front. Physiol. 2017, 8, 922. [Google Scholar] [CrossRef]
- Massaroni, C.; Nicolò, A.; Presti, D.L.; Sacchetti, M.; Silvestri, S.; Schena, E. Contact-based methods for measuring respiratory rate. Sensors 2019, 19, 908. [Google Scholar] [CrossRef] [Green Version]
- Naranjo-Hernández, D.; Talaminos-Barroso, A.; Reina-Tosina, J.; Roa, L.M.; Barbarov-Rostan, G.; Cejudo-Ramos, P.; Márquez-Martín, E.; Ortega-Ruiz, F. Smart vest for respiratory rate monitoring of copd patients based on non-contact capacitive sensing. Sensors 2018, 18, 2144. [Google Scholar] [CrossRef] [Green Version]
- Hesse, M.; Christ, P.; Hormann, T.; Ruckert, U. A respiration sensor for a chest-strap based wireless body sensor. In Proceedings of the IEEE SENSORS 2014 Proceedings, Valencia, Spain, 2–5 November 2014; IEEE: Piscataway, NJ, USA, 2014; Volume 2014, pp. 490–493. [Google Scholar]
- Chiarugi, F.; Karatzanis, I.; Zacharioudakis, G.; Meriggi, P.; Rizzo, F.; Stratakis, M.; Louloudakis, S.; Biniaris, C.; Valentini, M.; Di Rienzo, M.; et al. Measurement of heart rate and respiratory rate using a textile-based wearable device in heart failure patients. Comput. Cardiol. 2008, 35, 901–904. [Google Scholar]
- Furtak, N.T.; Skrzetuska, E.; Krucińska, I. Development of Screen-Printed Breathing Rate Sensors. Fibres Text. East. Eur. 2013, 21, 84–88. [Google Scholar]
- Wu, D.; Wang, L.; Zhang, Y.; Huang, B.; Wang, B.; Lin, S.; Xu, X. A wearable respiration monitoring system based on digital respiratory inductive plethysmography. In Proceedings of the 2009 Annual international conference of the IEEE Engineering in Medicine and Biology Society, Minneapolis, MN, USA, 3–6 September 2009; pp. 4844–4847. [Google Scholar]
- Jeong, J.W.; Jang, Y.W.; Lee, I.; Shin, S.; Kim, S. Wearable Respiratory Rate Monitoring using Piezo-resistive Fabric Sensor. In Proceedings of the World Congress on Medical Physics and Biomedical Engineering, Munich, Germany, 7–12 September 2009; Dössel, O., Schlegel, W.C., Eds.; Springer: Berlin/Heidelberg, Germany, 2009; pp. 282–284, ISBN 978-3-642-03904-1. [Google Scholar]
- Lei, K.F.; Hsieh, Y.Z.; Chiu, Y.Y.; Wu, M.H. The structure design of piezoelectric poly(vinylidene fluoride) (PVDF) polymer-based sensor patch for the respiration monitoring under dynamic walking conditions. Sensors 2015, 15, 18801–18812. [Google Scholar] [CrossRef] [Green Version]
- Bonato, P. Clinical applications of wearable technology. In Proceedings of the 2009 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Minneapolis, MN, USA, 2–6 September 2009; pp. 6580–6583. [Google Scholar]
- Berry, C.E.; Wise, R.A. Mortality in COPD: Causes, Risk Factors, and Prevention. COPD J. Chronic Obstr. Pulm. Dis. 2010, 7, 375–382. [Google Scholar] [CrossRef] [PubMed]
- Anlló, H.; Herer, B.; Delignières, A.; Bocahu, Y.; Segundo, I.; Mach Alingrin, V.; Gilbert, M.; Larue, F. Hypnosis for the management of anxiety and dyspnea in COPD: A randomized, sham-controlled crossover trial. Int. J. Chronic Obstr. Pulm. Dis. 2020, 15, 2609–2620. [Google Scholar]
- Yañez, A.M.; Guerrero, D.; Pérez De Alejo, R.; Garcia-Rio, F.; Alvarez-Sala, J.L.; Calle-Rubio, M.; Malo De Molina, R.; Valle Falcones, M.; Ussetti, P.; Sauleda, J.; et al. Monitoring breathing rate at home allows early identification of COPD exacerbations. Chest 2012, 142, 1524–1529. [Google Scholar] [CrossRef] [PubMed]
- Bellos, C.C.; Papadopoulos, A.; Rosso, R.; Fotiadis, D.I. Identification of COPD patients’ health status using an intelligent system in the CHRONIOUS wearable platform. IEEE J. Biomed. Heal. Inform. 2014, 18, 731–738. [Google Scholar] [CrossRef] [PubMed]
- Rolfe, S. The importance of respiratory rate monitoring. Br. J. Nurs. 2019, 28, 504–508. [Google Scholar] [CrossRef] [PubMed]
- Rubio, N.; Parker, R.A.; Drost, E.M.; Pinnock, H.; Weir, C.J.; Hanley, J.; Mantoani, L.C.; Macnee, W.; McKinstry, B.; Rabinovich, R.A. Home monitoring of breathing rate in people with chronic obstructive pulmonary disease: Observational study of feasibility, acceptability, and change after exacerbation. Int. J. Chronic Obstr. Pulm. Dis. 2017, 12, 1221–1231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dias, D.; Cunha, J.P.S. Wearable health devices—Vital sign monitoring, systems and technologies. Sensors 2018, 18, 2414. [Google Scholar] [CrossRef] [Green Version]
- Ciocchetti, M.; Massaroni, C.; Saccomandi, P.; Caponero, M.; Polimadei, A.; Formica, D.; Schena, E. Smart Textile Based on Fiber Bragg Grating Sensors for Respiratory Monitoring: Design and Preliminary Trials. Biosensors 2015, 5, 602–615. [Google Scholar] [CrossRef] [Green Version]
- Sharma, P.; Hui, X.; Zhou, J.; Conroy, T.B.; Kan, E.C. Wearable radio-frequency sensing of respiratory rate, respiratory volume, and heart rate. NPJ Digit. Med. 2020, 3, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, A.; Nakamoto, H.; Bessho, Y.; Watanabe, Y.; Oki, Y.; Ono, K.; Fujimoto, Y.; Terada, T.; Ishikawa, A. Monitoring respiratory rates with a wearable system using a stretchable strain sensor during moderate exercise. Med. Biol. Eng. Comput. 2019, 57, 2741–2756. [Google Scholar] [CrossRef] [PubMed]
- Chu, M.; Nguyen, T.; Pandey, V.; Zhou, Y.; Pham, H.N.; Bar-Yoseph, R.; Radom-Aizik, S.; Jain, R.; Cooper, D.M.; Khine, M. Respiration rate and volume measurements using wearable strain sensors. NPJ Digit. Med. 2019, 2, 8. [Google Scholar] [CrossRef] [PubMed]
- Massaroni, C.; Lopes, D.S.; Lo Presti, D.; Schena, E.; Silvestri, S. Contactless monitoring of breathing patterns and respiratory rate at the pit of the neck: A single camera approach. J. Sens. 2018, 2018, 1–13. [Google Scholar] [CrossRef]
- Tomasic, I.; Tomasic, N.; Trobec, R.; Krpan, M.; Kelava, T. Continuous remote monitoring of COPD patients—justification and explanation of the requirements and a survey of the available technologies. Med. Biol. Eng. Comput. 2018, 56, 547–569. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Halhouli, A.; Al-Ghussain, L.; El Bouri, S.; Habash, F.; Liu, H.; Zheng, D. Clinical evaluation of stretchable and wearable inkjet-printed strain gauge sensor for respiratory rate monitoring at different measurements locations. J. Clin. Monit. Comput. 2020, 10, 480. [Google Scholar] [CrossRef]
- Cordova, F.C.; Ciccolella, D.; Grabianowski, C.; Gaughan, J.; Brennan, K.; Goldstein, F.; Jacobs, M.R.; Criner, G.J. A Telemedicine-Based Intervention Reduces the Frequency and Severity of COPD Exacerbation Symptoms: A Randomized, Controlled Trial. Telemed. Health 2016, 22, 114–122. [Google Scholar] [CrossRef] [Green Version]
- Carlson, R.V.; Boyd, K.M.; Webb, D.J. The revision of the Declaration of Helsinki: Past, present and future. Br. J. Clin. Pharmacol. 2004, 57, 695–713. [Google Scholar] [CrossRef]
- Hacks, C. e-Health Sensor Platform V2.0 for Arduino and Raspberry Pi [Biometric/Medical Applications]. Available online: https://www.cooking-hacks.com/documentation/tutorials/ehealth-biometric-sensor-platform-arduino-raspberry-pi-medical (accessed on 20 February 2019).
- Arduino Mega 2560 Datasheet. Available online: http://eprints.polsri.ac.id/4598/8/File%20VIII%20%28Lampiran%29.pdf (accessed on 10 January 2021).
- ATmega640/V-1280/V-1281/V-2560/V-2561/V. Available online: https://ww1.microchip.com/downloads/en/DeviceDoc/ATmega640-1280-1281-2560-2561-Datasheet-DS40002211A.pdf (accessed on 10 January 2021).
- Schmider, E.; Ziegler, M.; Danay, E.; Beyer, L.; Bühner, M. Is It Really Robust? Methodology 2010, 6, 147–151. [Google Scholar] [CrossRef]
- Bland, J.M.; Altman, D.G. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 1, 307–310. [Google Scholar] [CrossRef]
- Giavarina, D. Understanding Bland Altman analysis. Biochem. Med. 2015, 25, 141–151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siafakas, N.M.; Vermeire, P.; Pride, N.B.; Paoletti, P.; Gibson, J.; Howard, P.; Yernault, J.C.; Decramer, M.; Higenbottam, T.; Postma, D.S.; et al. Optimal assessment and management of chronic obstructive pulmonary disease (COPD). Eur. Respir. J. 1995, 8, 1398–1420. [Google Scholar] [CrossRef] [PubMed]
- Roche, N.; Chavannes, N.H.; Miravitlles, M. COPD symptoms in the morning: Impact, evaluation and management. Respir. Res. 2013, 14, 112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miravitlles, M.; Worth, H.; Soler Cataluña, J.J.; Price, D.; De Benedetto, F.; Roche, N.; Godtfredsen, N.S.; van der Molen, T.; Löfdahl, C.G.; Padullés, L.; et al. Observational study to characterise 24-hour COPD symptoms and their relationship with patient-reported outcomes: Results from the ASSESS study. Respir. Res. 2014, 15, 122. [Google Scholar] [CrossRef] [PubMed]
- Soler, J.; Alves Pegoraro, J.; Le, X.L.; Nguyen, D.P.Q.; Grassion, L.; Antoine, R.; Guerder, A.; Gonzalez-Bermejo, J. Validation of respiratory rate measurements from remote monitoring device in COPD patients. Respir. Med. Res. 2019, 76, 1–3. [Google Scholar] [CrossRef]
- Klersy, C.; De Silvestri, A.; Gabutti, G.; Raisaro, A.; Curti, M.; Regoli, F.; Auricchio, A. Economic impact of remote patient monitoring: An integrated economic model derived from a meta-analysis of randomized controlled trials in heart failure. Eur. J. Heart Fail. 2011, 13, 450–459. [Google Scholar] [CrossRef] [Green Version]
- Al Rajeh, A.; Hurst, J. Monitoring of Physiological Parameters to Predict Exacerbations of Chronic Obstructive Pulmonary Disease (COPD): A Systematic Review. J. Clin. Med. 2016, 5, 108. [Google Scholar] [CrossRef]
- Elvekjaer, M.; Aasvang, E.K.; Olsen, R.M.; Sørensen, H.B.D.; Porsbjerg, C.M.; Jensen, J.-U.; Haahr-Raunkjær, C.; Meyhoff, C.S. Physiological abnormalities in patients admitted with acute exacerbation of COPD: An observational study with continuous monitoring. J. Clin. Monit. Comput. 2020, 34, 1051–1060. [Google Scholar] [CrossRef]
- Parker, R.A.; Weir, C.J.; Rubio, N.; Rabinovich, R.; Pinnock, H.; Hanley, J.; McCloughan, L.; Drost, E.M.; Mantoani, L.C.; MacNee, W.; et al. Application of Mixed Effects Limits of Agreement in the Presence of Multiple Sources of Variability: Exemplar from the Comparison of Several Devices to Measure Respiratory Rate in COPD Patients. PLoS ONE 2016, 11, e0168321. [Google Scholar] [CrossRef]
- Miller, D.; Capodilupo, J.; Lastella, M.; Sargent, C.; Roach, G.; Lee, V.; Capodilupo, E. Analyzing changes in respiratory rate to predict the risk of COVID-19 infection. PLoS ONE 2020, 15, e0243693. [Google Scholar] [CrossRef]
- Nakano, H.; Kadowaki, M.; Furukawa, T.; Yoshida, M. Rise in nocturnal respiratory rate during CPAP may be an early sign of COVID-19 in patients with obstructive sleep apnea. J. Clin. Sleep Med. 2020, 6, 1811–1813. [Google Scholar] [CrossRef] [PubMed]







| Ref. | Method | Posture | Accuracy Parameter | Protocol | Number of COPD Patients | |
|---|---|---|---|---|---|---|
| [33] | Impedance | Activities of daily living protocol | Bias (bpm) | −1.18 | Attached to the chest and upper abdomen | 44 |
| LoA (bpm) | −20.07 to 17.72 | |||||
| Photoplethysmography (PPG) | Bias (bpm) | 3.01 | Worn on the wrist with a finger probe | |||
| LoA (bpm) | −11.17 to 17.19 | |||||
| Camera | Bias (bpm) | −3.21 | Participant was videoed while in sitting position | |||
| LoA (bpm) | −12.71 to 6.30 | |||||
| Accelerometer | Bias (bpm) | −2.18 | Attached to the upper abdomen just below the ribs and taped to the skin | |||
| LoA (bpm) | −8.63 to 4.27 | |||||
| Chest-Band (strain gauge) | Bias (bpm) | −1.60 | Chest strap and an electronics module that attaches to the strap | 62 | ||
| LoA (bpm) | −9.99 to 6.80 | |||||
| [20] | Capacitive | Rest (lying) | Bias (bpm) | −0.14 bpm | Rest (after exercises) | 9 |
| SD (bpm) | 0.28 | |||||
| [31] | Respiration band (strain gauge) | - | Relative Error (%) | 17.43 | Attached to the wearable Jacket | 30 |
| [53] | Airflow pressure sensor | - | Bias (bpm) | 0.046 | Hoses attached to the nose | 14 |
| LoA (bpm) | 3.865 to 3.957 | |||||
| This study | Strain gauge | Sitting | Bias (bpm) | −0.0542 bpm | 1 | 35 |
| LoA (bpm) | −2.951 to 2.842 | |||||
| SD (bpm) | 1.451 | |||||
| Absolute relative error (%) | 4.49 | |||||
| Standing | Bias (bpm) | −0.0814 | ||||
| LoA (bpm) | −4.257 to 4.094 | |||||
| SD (bpm) | 2.071 | |||||
| Absolute relative error (%) | 7.29 | |||||
| Lying45° | Bias (bpm) | −0.501 | ||||
| LoA (bpm) | −8.969 to 6.807.967 | |||||
| SD (bpm) | 4.227 | |||||
| Absolute relative error (%) | 9.47 | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al-Halhouli, A.; Al-Ghussain, L.; Khallouf, O.; Rabadi, A.; Alawadi, J.; Liu, H.; Al Oweidat, K.; Chen, F.; Zheng, D. Clinical Evaluation of Respiratory Rate Measurements on COPD (Male) Patients Using Wearable Inkjet-Printed Sensor. Sensors 2021, 21, 468. https://doi.org/10.3390/s21020468
Al-Halhouli A, Al-Ghussain L, Khallouf O, Rabadi A, Alawadi J, Liu H, Al Oweidat K, Chen F, Zheng D. Clinical Evaluation of Respiratory Rate Measurements on COPD (Male) Patients Using Wearable Inkjet-Printed Sensor. Sensors. 2021; 21(2):468. https://doi.org/10.3390/s21020468
Chicago/Turabian StyleAl-Halhouli, Ala’aldeen, Loiy Al-Ghussain, Osama Khallouf, Alexander Rabadi, Jafar Alawadi, Haipeng Liu, Khaled Al Oweidat, Fei Chen, and Dingchang Zheng. 2021. "Clinical Evaluation of Respiratory Rate Measurements on COPD (Male) Patients Using Wearable Inkjet-Printed Sensor" Sensors 21, no. 2: 468. https://doi.org/10.3390/s21020468