Effects of Novel Inverted Rocker Orthoses for First Metatarsophalangeal Joint on Gastrocnemius Muscle Electromyographic Activity during Running: A Cross-Sectional Pilot Study

 ,
,  , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
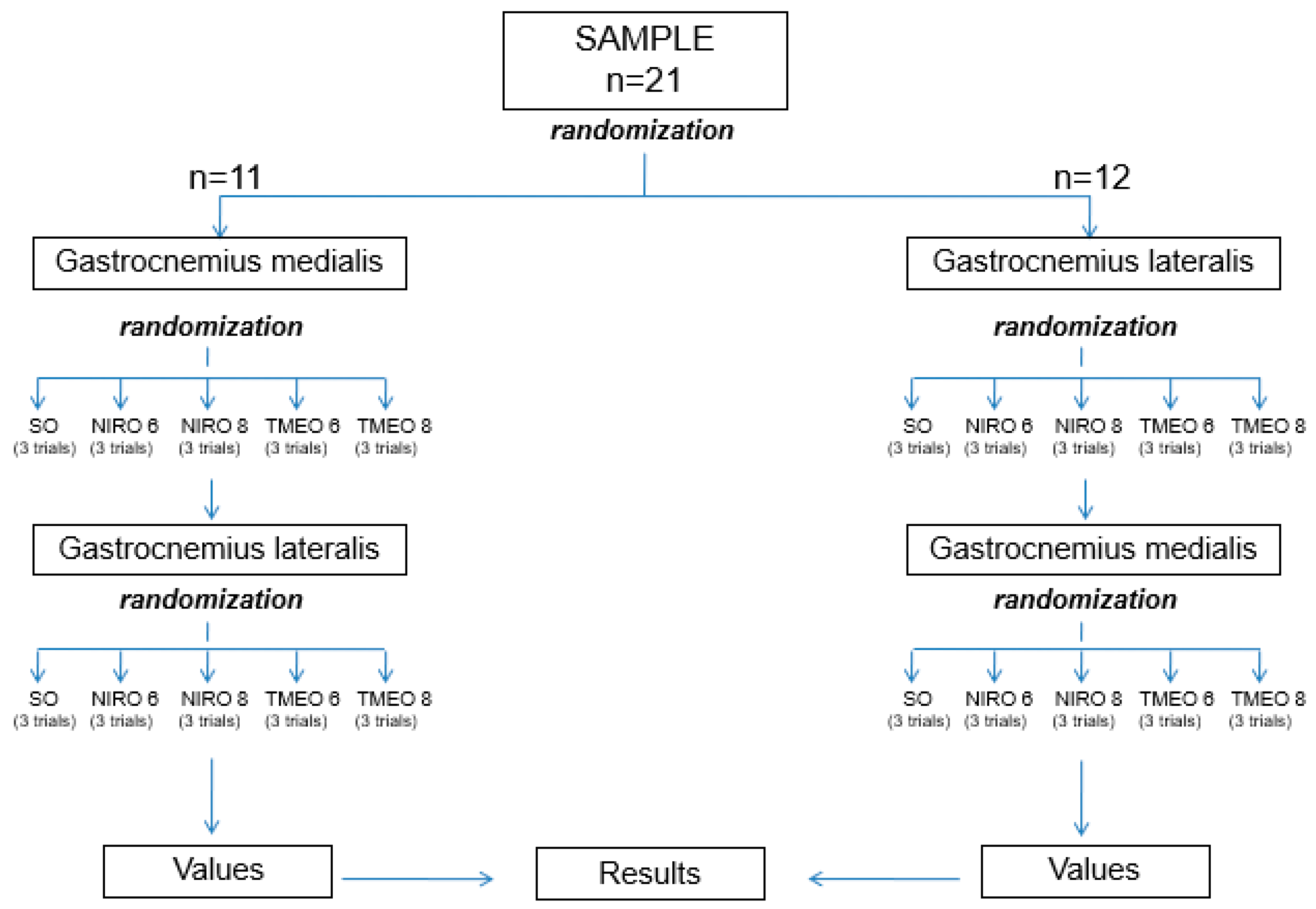
2.1. Design and Sample Size
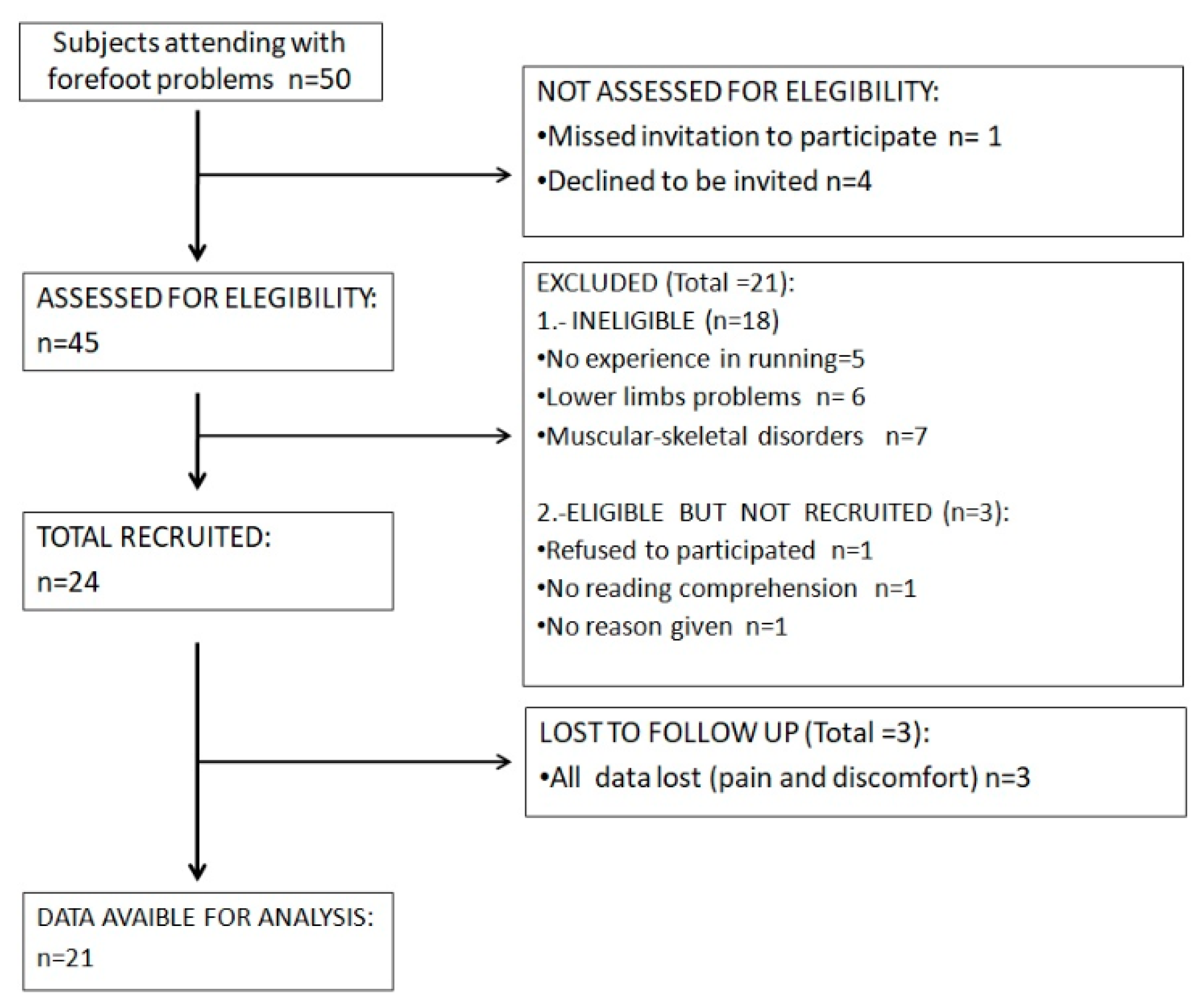
2.2. Subjects
2.3. Instrumentation and Assessments
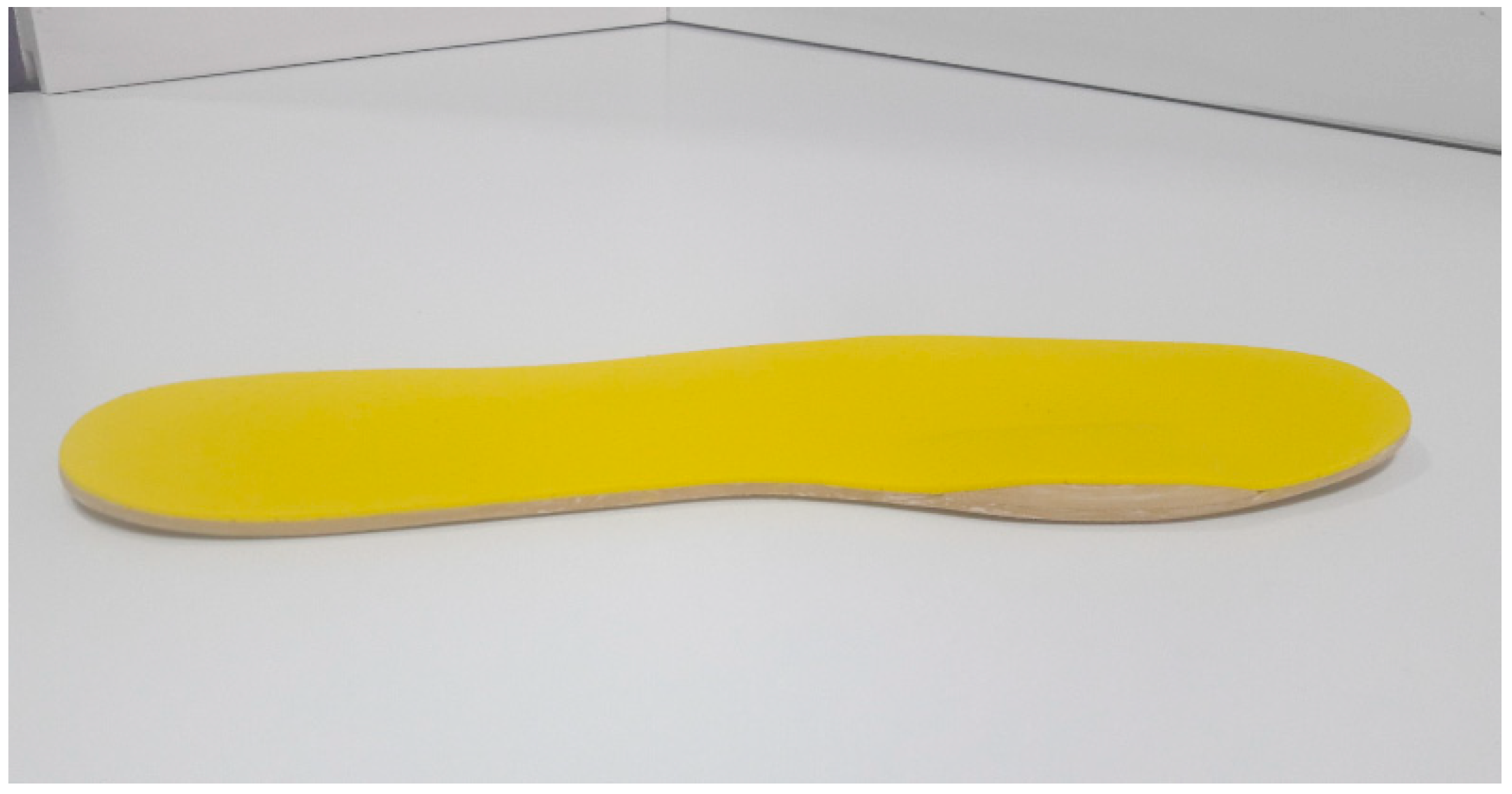
2.4. Materials
2.5. Procedure
2.6. Statistical Analysis
3. Results
4. Discussion
4.1. TMEO and NIRO Effects
4.2. Osteoarthritis
4.3. Running Economy
5. Limitations
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Cotterill, J.M. Stiffness of the Great Toe in Adolescents. Br. Med. J. 1887, 1, 1158. Available online: http://www.ncbi.nlm.nih.gov/pubmed/20751923 (accessed on 21 February 2019). [CrossRef] [PubMed] [Green Version]
- Laird, P.O. Functional Hallux Limitus. Ill. Podiatr. 1972, 9, 4. [Google Scholar]
- Drago, J.J.; Oloff, L.; Jacobs, A.M. A comprehensive review of hallux limitus. J. Foot Surg. 1984, 23, 213–220. [Google Scholar] [PubMed]
- Zammit, G.V.; Menz, H.B.; Munteanu, S.E. Structural factors associated with hallux limitus/rigidus: A systematic review of case control studies. J. Orthop. Sports Phys. Ther. 2009, 39, 733–742. [Google Scholar] [CrossRef] [PubMed]
- Dananberg, H.J. Functional hallux limitus and its relationship to gait efficiency. J. Am. Podiatr. Med. Assoc. 1986, 76, 648–652. Available online: http://www.ncbi.nlm.nih.gov/pubmed/3814239 (accessed on 17 August 2015). [CrossRef]
- Tenforde, A.S.; Yin, A.; Hunt, K.J. Foot and Ankle Injuries in Runners. Physical Medicine and Rehabilitation Clinics of North America; Saunders, W.B., Ed.; Elsevier Inc.: Amsterdam, The Netherlands, 2016; Volume 27, pp. 121–137. Available online: http://www.ncbi.nlm.nih.gov/pubmed/26616180 (accessed on 15 May 2020).
- Polzer, H.; Polzer, S.; Brumann, M.; Mutschler, W.; Regauer, M. Hallux rigidus: Joint preserving alternatives to arthrodesis—A review of the literature. World J. Orthop. 2014, 5, 6–13. [Google Scholar] [CrossRef]
- Shurnas, P.S. Hallux Rigidus: Etiology, Biomechanics, and Nonoperative Treatment. Foot Ankle Clin. 2009, 14, 1–8. [Google Scholar] [CrossRef]
- Dananberg, H.J. Gait style as an etiology to chronic postural pain. Part, I. Functional hallux limitus. J. Am. Podiatr. Med. Assoc. 1993, 83, 433–441. [Google Scholar] [CrossRef]
- Smith, R.W.; Katchis, S.D.; Ayson, L.C. Outcomes in hallux rigidus patients treated nonoperatively: A long-term follow-up study. Foot Ankle Int. 2000, 21, 906–913. [Google Scholar] [CrossRef]
- Grady, J.F.; Axe, T.M.; Zager, E.J.; Sheldon, L.A. A retrospective analysis of 772 patients with hallux limitus. J. Am. Podiatr. Med. Assoc. 2002, 92, 102–108. [Google Scholar] [CrossRef]
- Menz, H.B.; Auhl, M.; Tan, J.M.; Levinger, P.; Roddy, E.; Munteanu, S.E. Biomechanical Effects of Prefabricated Foot Orthoses and Rocker-Sole Footwear in Individuals with First Metatarsophalangeal Joint Osteoarthritis. Arthritis Care Res. 2016, 68, 603–611. [Google Scholar] [CrossRef] [Green Version]
- Romkes, J.; Rudmann, C.; Brunner, R. Changes in gait and EMG when walking with the Masai Barefoot Technique. Clin. Biomech. 2006, 21, 75–81. Available online: https://www.sciencedirect.com/science/article/abs/pii/S0268003305001816 (accessed on 15 May 2020). [CrossRef] [PubMed]
- Saunders, P.U.; Pyne, D.B.; Telford, R.D.; Hawley, J.A. Reliability and variability of running economy in elite distance runners. Med. Sci. Sports Exerc. 2004, 36, 1972–1976. [Google Scholar] [CrossRef] [PubMed]
- Hayes, P.R.; Bowen, S.J.; Davies, E.J. The relationships between local muscular endurance and kinematic changes during a run to exhaustion at vVO2MAX. J. Strength Cond. Res. 2004, 18, 898–903. [Google Scholar]
- Roca-Dols, A.; Losa-Iglesias, M.E.; Sánchez-Gómez, R.; Becerro-de-Bengoa-Vallejo, R.; López-López, D.; Rodríguez-Sanz, D.; Martínez-Jiménez, E.M.; Calvo-Lobo, C. Effect of the cushioning running shoes in ground contact time of phases of gait. J. Mech. Behav. Biomed. Mater. 2018, 88, 196–200. [Google Scholar] [CrossRef] [PubMed]
- Roca-Dols, A.; Elena Losa-Iglesias, M.; Sánchez-Gómez, R.; Becerro-de-Bengoa-Vallejo, R.; López-López, D.; Palomo-López, P.; Rodríguez-Sanz, D.; Calvo-Lobo, C. Electromyography activity of triceps surae and tibialis anterior muscles related to various sports shoes. J. Mech. Behav. Biomed. Mater. 2018, 86, 158–171. [Google Scholar] [CrossRef]
- Roca-Dols, A.; Losa-Iglesias, M.E.; Sánchez-Gómez, R.; López-López, D.; Becerro-de-Bengoa-Vallejo, R.; Calvo-Lobo, C. Electromyography comparison of the effects of various footwear in the activity patterns of the peroneus longus and brevis muscles. J. Mech. Behav. Biomed. Mater. 2018, 82, 126–132. [Google Scholar] [CrossRef]
- Blagrove, R.C.; Howatson, G.; Hayes, P.R. Effects of Strength Training on the Physiological Determinants of Middle- and Long-Distance Running Performance: A Systematic Review. Sports Medicine; Springer International Publishing: Cham, Switzerland, 2018; Volume 48, pp. 1117–1149. [Google Scholar]
- Tam, N.; Tucker, R.; Santos-Concejero, J.; Prins, D.; Lamberts, R.P. Running Economy: Neuromuscular and Joint-Stiffness Contributions in Trained Runners. Int. J. Sports Physiol. Perform. 2019, 14, 16–22. [Google Scholar] [CrossRef]
- Hicks, J. The mechanics of the foot. II. The plantar aponeurosis and the arch. J. Anat. 1954, 88, 25–30. [Google Scholar]
- Stearne, S.M.; McDonald, K.A.; Alderson, J.A.; North, I.; Oxnard, C.E.; Rubenson, J. The Foot’s Arch and the Energetics of Human Locomotion. Sci. Rep. 2016, 6, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Ker, R.F.; Bennett, M.B.; Bibby, S.R.; Kester, R.C.; Alexander, R.M. The spring in the arch of the human foot. Nature 1987, 325, 147–149. [Google Scholar] [CrossRef]
- Maceira, E.; Monteagudo, M. Functional hallux rigidus and the Achilles-calcaneus-plantar system. Foot Ankle Clin. 2014, 19, 669–699. [Google Scholar] [CrossRef]
- Welte, L.; Kelly, L.A.; Lichtwark, G.A.; Rainbow, M.J. Influence of the windlass mechanism on arch-spring mechanics during dynamic foot arch deformation. J. R. Soc. Interface 2018, 15, 20180270. [Google Scholar] [CrossRef] [Green Version]
- Johanson, M.A.; Allen, J.C.; Matsumoto, M.; Ueda, Y.; Wilcher, K.M. Effect of Heel Lifts on Plantarflexor and Dorsiflexor Activity During Gait. Foot Ankle Int. 2010, 31, 1014–1020. [Google Scholar] [CrossRef] [PubMed]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for reporting observational studies. Int. J. Surg. 2014, 12, 1495–1499. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Redmond, A.C.; Crosbie, J.; Ouvrier, R.A. Development and validation of a novel rating system for scoring standing foot posture: The Foot Posture Index. Clin. Biomech. (Bristol. Avon.) 2006, 21, 89–98. [Google Scholar] [CrossRef]
- Root, M.L.; Orien, W.P.; Weed, J.H.; Hughes, R.J. Normal and Abnormal Function of the Foot; Clinical Biomechanics Corp.: Los Angeles, CA, USA, 1977; Volume 2. [Google Scholar]
- Sánchez-Gómez, R.; Becerro-de-Bengoa-Vallejo, R.; Losa-Iglesias, M.E.; Calvo-Lobo, C.; Navarro-Flores, E.; Palomo-López, P.; Romero-Morales, C.; López-López, D. Reliability Study of Diagnostic Tests for Functional Hallux Limitus. Foot Ankle Int. 2020, 41, 457–462. [Google Scholar] [CrossRef] [PubMed]
- Garrow, J.S.; Webster, J. Quetelet’s index (W/H2) as a measure of fatness. Int. J. Obes. 1985, 9, 147–153. [Google Scholar] [PubMed]
- Naess, I.; Bø, K. Can maximal voluntary pelvic floor muscle contraction reduce vaginal resting pressure and resting EMG activity? Int. Urogynecol. J. 2018, 29, 1623–1627. [Google Scholar] [CrossRef] [Green Version]
- Hermens, H.J.; Freriks, B.; Disselhorst-Klug, C.; Rau, G. Development of recommendations for SEMG sensors and sensor placement procedures. J. Electromyogr. Kinesiol. 2000, 10, 361–374. [Google Scholar] [CrossRef]
- Murley, G.S.; Buldt, A.K.; Trump, P.J.; Wickham, J.B. Tibialis posterior EMG activity during barefoot walking in people with neutral foot posture. J. Electromyogr. Kinesiol. 2009, 19, e69–e77. [Google Scholar] [CrossRef] [PubMed]
- Shih, Y.; Lin., K.-L.; Shiang, T.-Y. Is the foot striking pattern more important than barefoot or shod conditions in running? Gait Posture 2013, 38, 490–494. [Google Scholar] [CrossRef] [PubMed]
- Goto, K.; Abe, K. Gait characteristics in women’s safety shoes. Appl. Ergon. 2017, 65, 163–167. [Google Scholar] [CrossRef]
- Fleming, N.; Walters, J.; Grounds, J.; Fife, L.; Finch, A. Acute response to barefoot running in habitually shod males. Hum. Mov. Sci. 2015, 42, 27–37. [Google Scholar] [CrossRef] [PubMed]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jacobson, N.; Truax, P. Clinical significance: A statistical approach to defining meaningful change in psychotherapy research. J. Consult Clin. Psychol. 1991, 59, 12–19. [Google Scholar] [CrossRef]
- Myers, K.A.; Long, J.T.; Klein, J.P.; Wertsch, J.J.; Janisse, D.; Harris, G.F. Biomechanical implications of the negative heel rocker sole shoe: Gait kinematics and kinetics. Gait Posture 2006, 24, 323–330. [Google Scholar] [CrossRef]
- Honert, E.C.; Bastas, G.; Zelik, K.E. Effect of toe joint stiffness and toe shape on walking biomechanics. Bioinspir. Biomim. 2018, 13, 066007. [Google Scholar] [CrossRef]
- Sebbag, E.; Felten, R.; Sagez, F.; Sibilia, J.; Devilliers, H.; Arnaud, L. The world-wide burden of musculoskeletal diseases: A systematic analysis of the World Health Organization Burden of Diseases Database. Ann. Rheum. Dis. 2019, 78, 844–848. [Google Scholar] [CrossRef]
- Biewener, A.A.; Roberts, T.J. Muscle and tendon contributions to force, work, and elastic energy savings: A comparative perspective. Exerc. Sport Sci. Rev. 2000, 28, 99–107. [Google Scholar]
- Wilson, A.; Lichtwark, G. The anatomical arrangement of muscle and tendon enhances limb versatility and locomotor performance. Philos. Trans. R. Soc. Lond. B Biol. Sci. 2011, 366, 1540–1553. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boyer, K.A.; Nigg, B.M. Muscle activity in the leg is tuned in response to impact force characteristics. J. Biomech. 2004, 37, 1583–1588. [Google Scholar] [CrossRef] [PubMed]
- Hamner, S.R.; Seth, A.; Delp, S.L. Muscle contributions to propulsion and support during running. J. Biomech. 2010, 43, 2709–2716. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | n = 21 Mean ± SD (95% CI) |
|---|---|
| Age | 31.41 ± 4.33 (32.26–35.09) |
| FPI (scores) | 3.12 ± 0.17 (2.07–3.41) |
| Weight (kg) | 67.50 ± 8.06 (62.36–70.06) |
| Height (cm) | 170.08 ± 6.91 (166.9–172.43) |
| BMI (kg/m2) | 23.15 ± 3.05 (21.7–24.7) |
| Variables | SO | NIRO-6 mm | NIRO-8 mm | TMEO-6 mm | TMEO-8 mm | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ICC (95% CI) | MDC | ICC (95% CI) | MDC | ICC (95% CI) | MDC | ICC (95% CI) | MDC | ICC (95% CI) | MDC | ||||||
| SEM | 0.950 | SEM | 0.950 | SEM | 0.950 | SEM | 0.950 | SEM | 0.950 | ||||||
| Gastrocnemius lateralis (mV) | 0.839 | 0.932 | 0.971 | 0.937 | 0.458 | ||||||||||
| (0.651–0.935) | 1.010 | 3.560 | (0.852–0.973) | 1.254 | 3.477 | (0.938–0.988) | 0.817 | 2.264 | (0.861–0.975) | 1.359 | 3.766 | (0.148–0.777) | 2.092 | 5.798 | |
| Gastrocnemius medialis (mV) | 0.848 | 0.832 | 0.767 | 0.872 | 0.894 | ||||||||||
| (0.649–0.94) | 0.913 | 2.530 | (0.637–0.931) | 1.707 | 4.731 | (0.501–0.905) | 2.083 | 5.775 | (0.723–0.948) | 1.408 | 3.904 | (0.77–0.957) | 0.326 | 0.904 | |
| SO | NIRO 6 mm | NIRO 8 mm | TMEO 6 mm | TMEO 8 mm | p-Value SO | p-Value SO | p-Value SO | p-Value SO | p-Value NIRO 6 mm | p-Value NIRO 6 mm | p-Value NIRO 6 mm | p-Value NIRO 8 mm | p-Value NIRO 8 mm | p-Value TMEO 6 mm | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Variable | mean (mV) | mean(mV) | mean (mV) | mean (mV) | mean (mV) | vs. | vs. | vs. | vs. | vs. | vs. | vs. | vs. | vs. | vs. |
| gastrocnemius lateralis | ±SD (95% CI) | ±SD (95% CI) | ±SD (95% CI) | ±SD (95% CI) | ±SD (95% CI) | NIRO 6 mm | NIRO 8 mm | TMEO 6 mm | TMEO 8 mm | NIRO 8 mm | TMEO 6 mm | TMEO 8 mm | TMEO 6 mm | TMEO 8 mm | TMEO 8 mm |
| 22.27 ± 2.51 | 24.65 ± 4.51 | 25.96 ± 4.68 | 24.72 ± 5.08 | 25.49 ± 1.97 | |||||||||||
| (20.77–23.279) | (22.41–26.897) | (23.634–28.29) | (23.675–27.35) | (22.19–27.253) | 0.085 | <0.05 * | <0.05 * | <0.001 ** | 0.39 | 0.88 | 0.356 | 0.372 | 0.67 | 0.913 | |
| 22.93 ± 2.1 | 26.44 ± 3.63 | 28.89 ± 3.6 | 25.12 ± 3.51 | 26.38 ± 3.02 | |||||||||||
| gastrocnemius medialis | (21.88–23.97) | (24.63–28.24) | (27–30.68) | (23.37–26.87) | (24.88–27.89) | <0.001 ** | <0.001 ** | <0.05 * | <0.05 * | <0.05 * | 0.06 | 0.67 | <0.001 ** | <0.05 * | 0.22 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sánchez-Gómez, R.; Romero-Morales, C.; Gómez-Carrión, Á.; De-la-Cruz-Torres, B.; Zaragoza-García, I.; Anttila, P.; Kantola, M.; Ortuño-Soriano, I. Effects of Novel Inverted Rocker Orthoses for First Metatarsophalangeal Joint on Gastrocnemius Muscle Electromyographic Activity during Running: A Cross-Sectional Pilot Study. Sensors 2020, 20, 3205. https://doi.org/10.3390/s20113205
Sánchez-Gómez R, Romero-Morales C, Gómez-Carrión Á, De-la-Cruz-Torres B, Zaragoza-García I, Anttila P, Kantola M, Ortuño-Soriano I. Effects of Novel Inverted Rocker Orthoses for First Metatarsophalangeal Joint on Gastrocnemius Muscle Electromyographic Activity during Running: A Cross-Sectional Pilot Study. Sensors. 2020; 20(11):3205. https://doi.org/10.3390/s20113205
Chicago/Turabian StyleSánchez-Gómez, Rubén, Carlos Romero-Morales, Álvaro Gómez-Carrión, Blanca De-la-Cruz-Torres, Ignacio Zaragoza-García, Pekka Anttila, Matti Kantola, and Ismael Ortuño-Soriano. 2020. "Effects of Novel Inverted Rocker Orthoses for First Metatarsophalangeal Joint on Gastrocnemius Muscle Electromyographic Activity during Running: A Cross-Sectional Pilot Study" Sensors 20, no. 11: 3205. https://doi.org/10.3390/s20113205