
Factors Influencing Continuous Breath Signal in Intubated and Mechanically-Ventilated Intensive Care Unit Patients Measured by an Electronic Nose

 , ,
, ,
Abstract
:1. Introduction
1.1. Introduction into Breath Analysis
1.2. Ventilated ICU Patients
2. Methods
2.1. Study Design and Population
2.2. Standard of Care
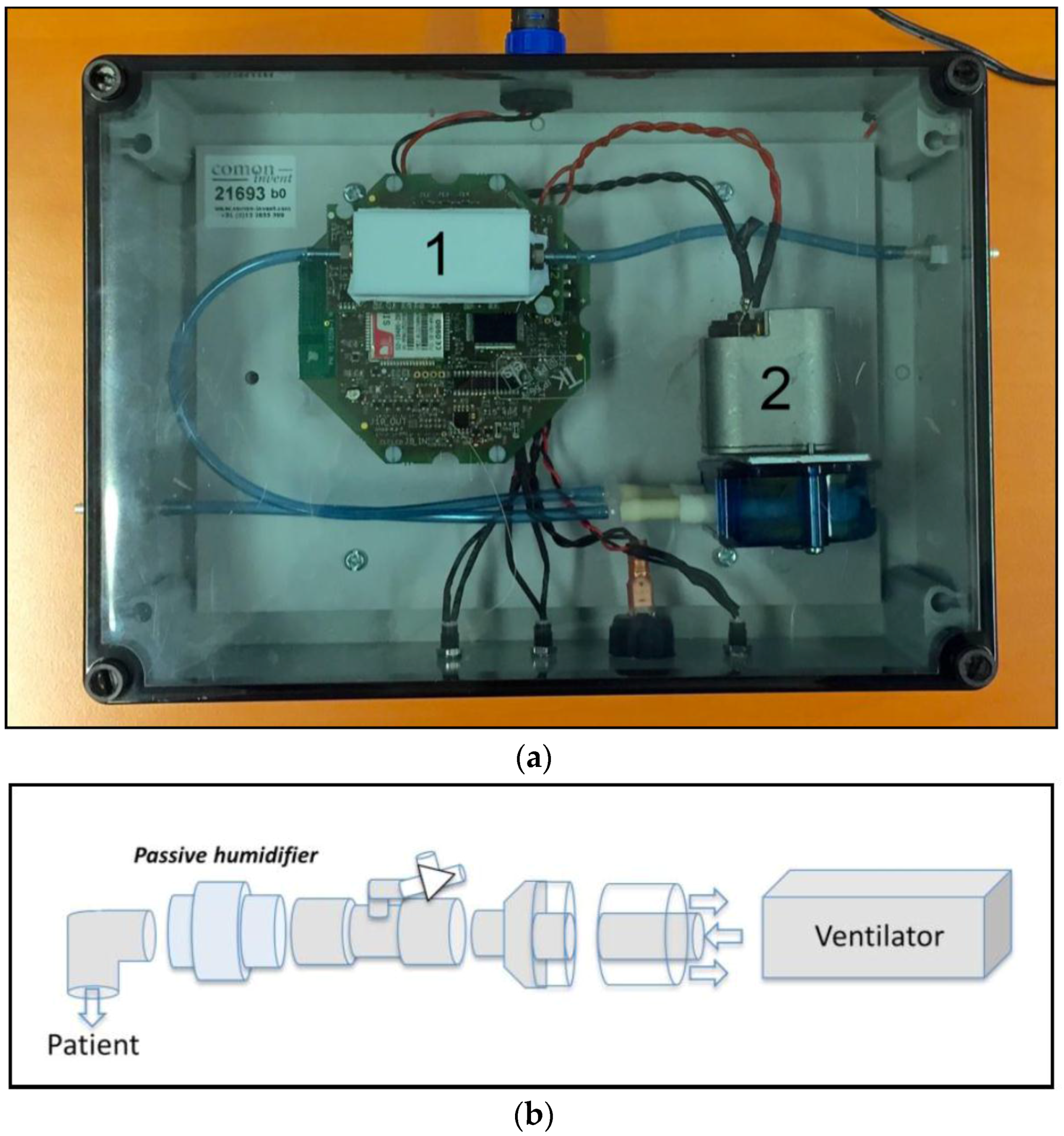
2.3. Study Procedures and Data Collection
2.4. Data Analysis
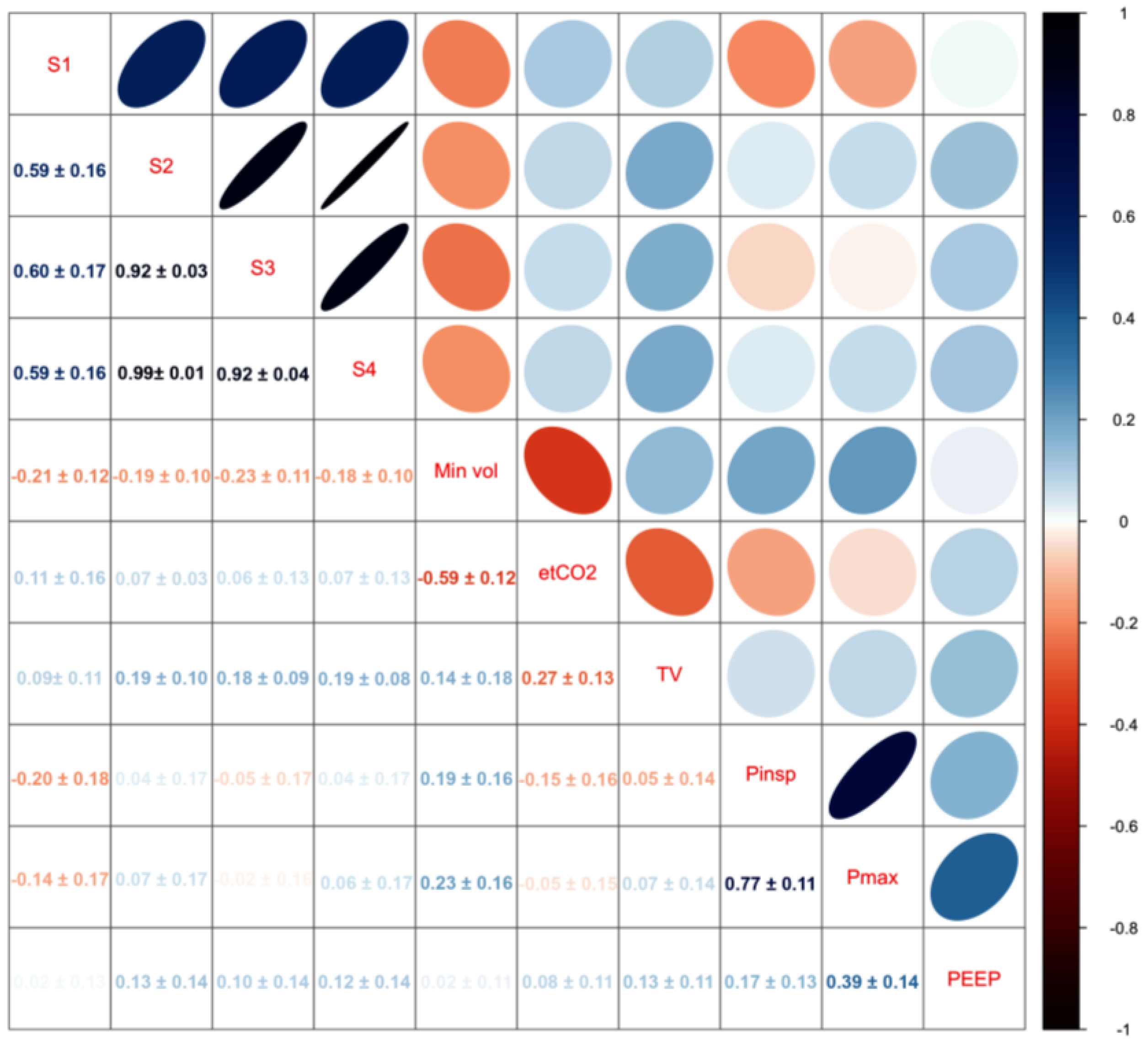
2.4.1. Noise Inducing Variables
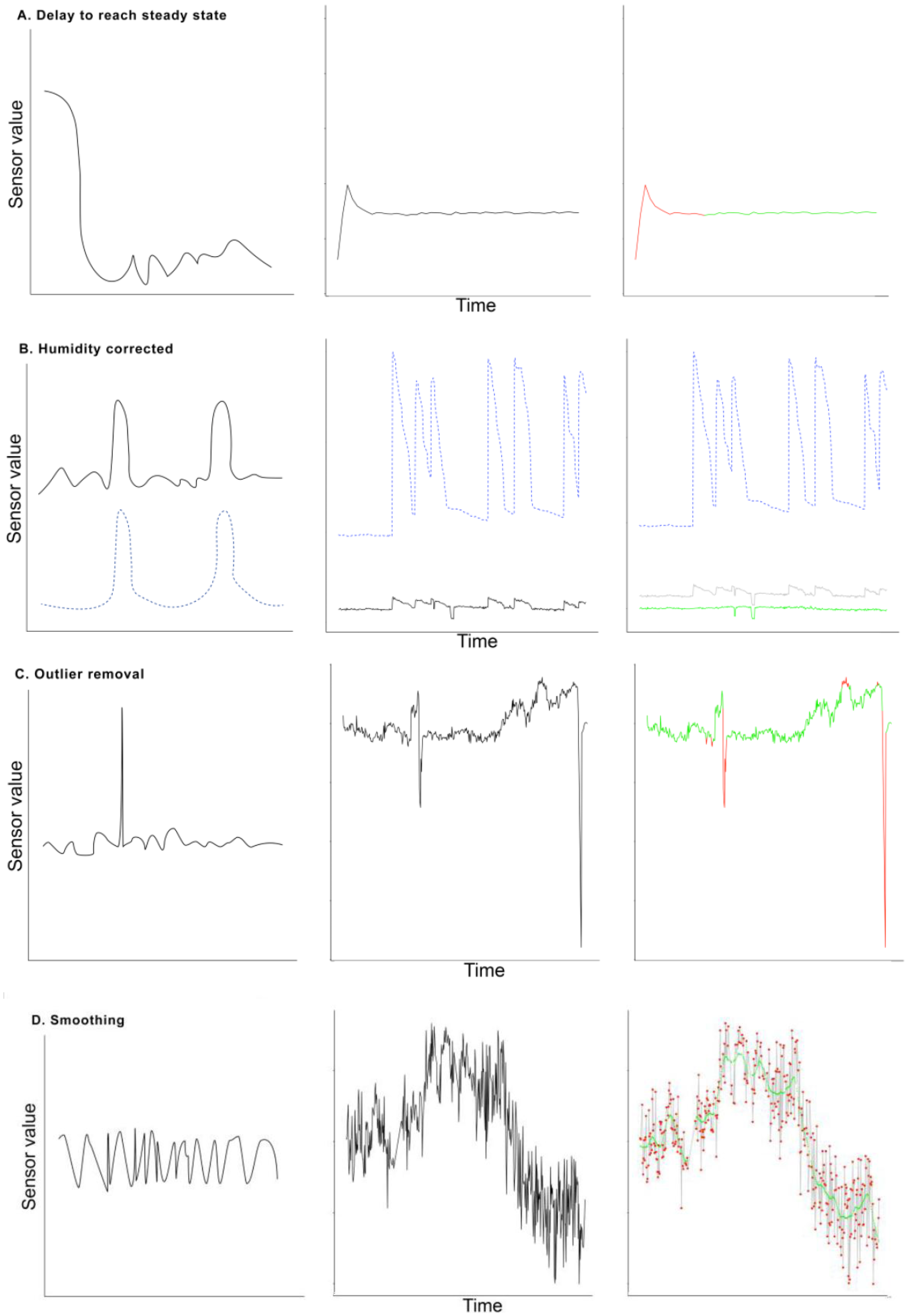
2.4.2. Time Delay to Reach Steady State
2.4.3. Changes in Humidity
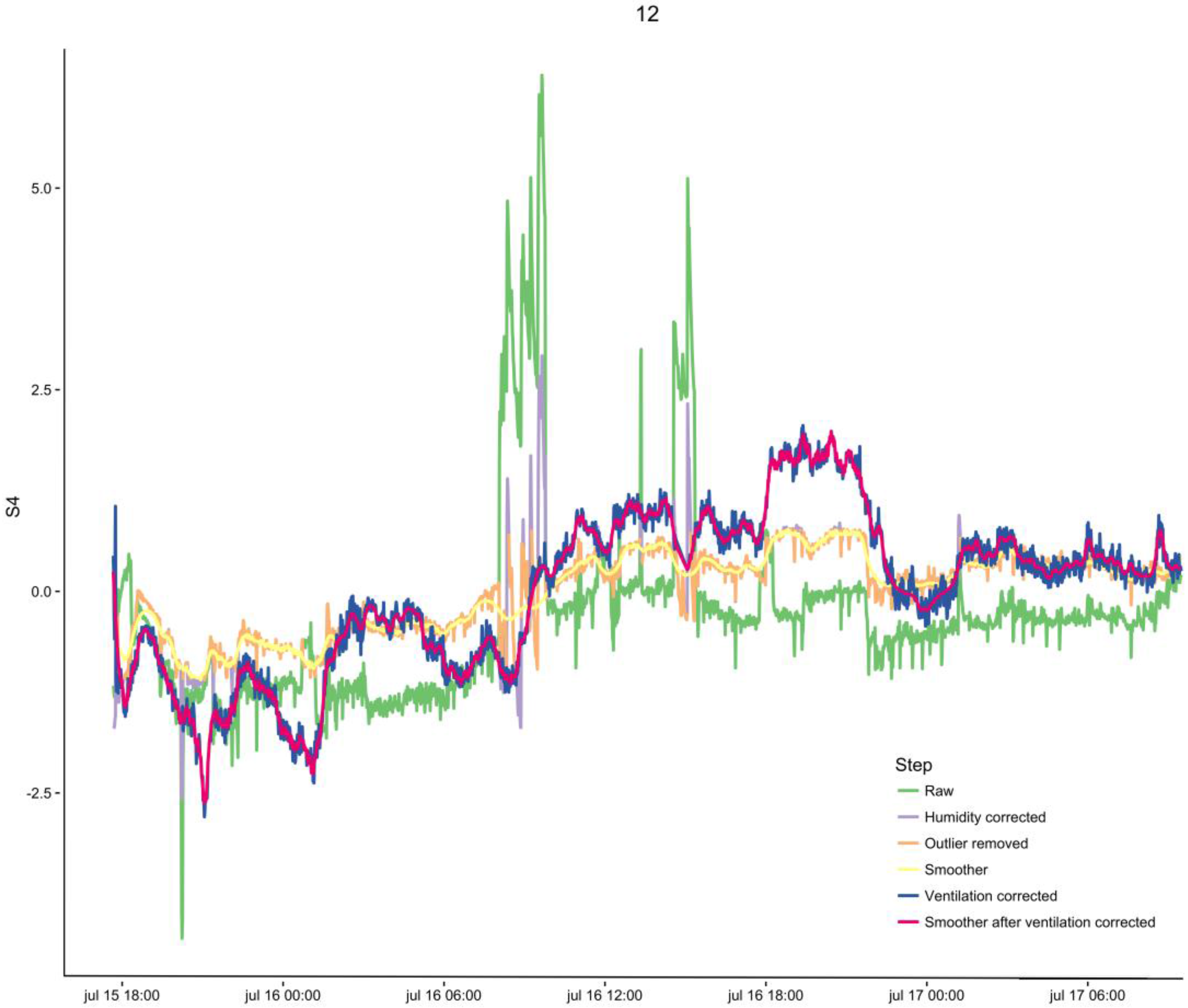
2.4.4. Outlier Removal and Smoothing
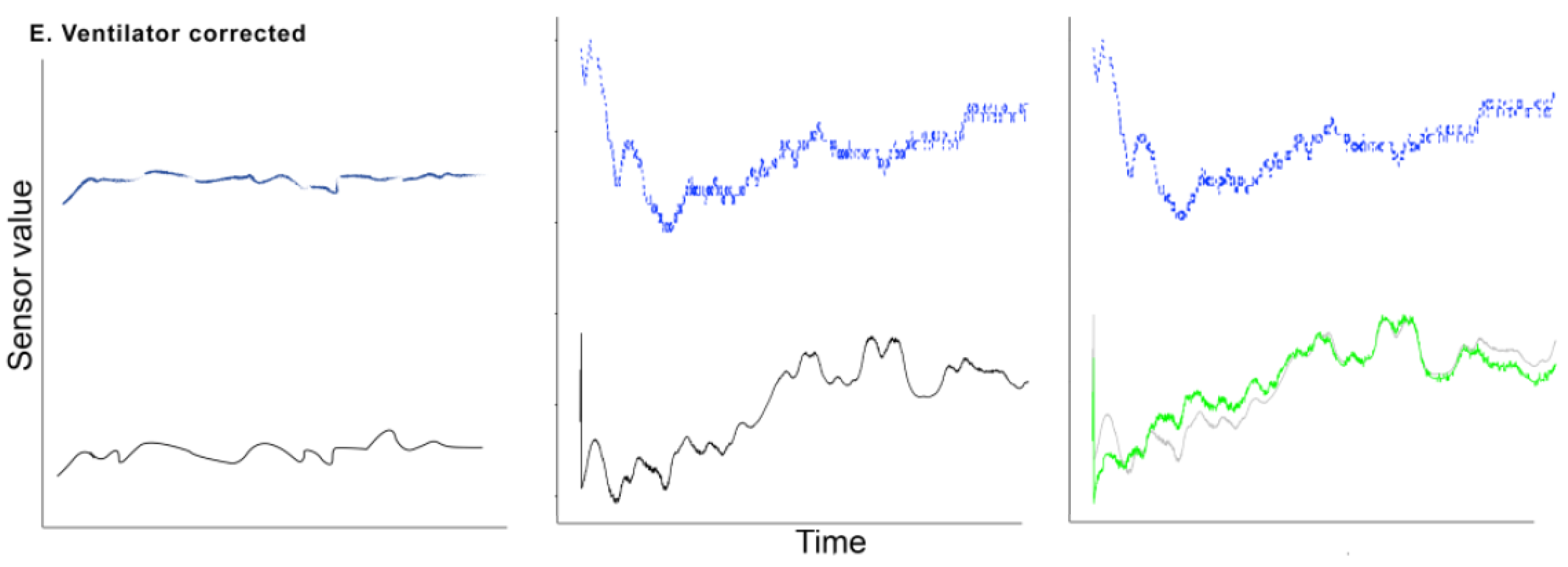
2.4.5. Changes in Ventilation Settings
3. Results of Noise Reduction
3.1. Steady State
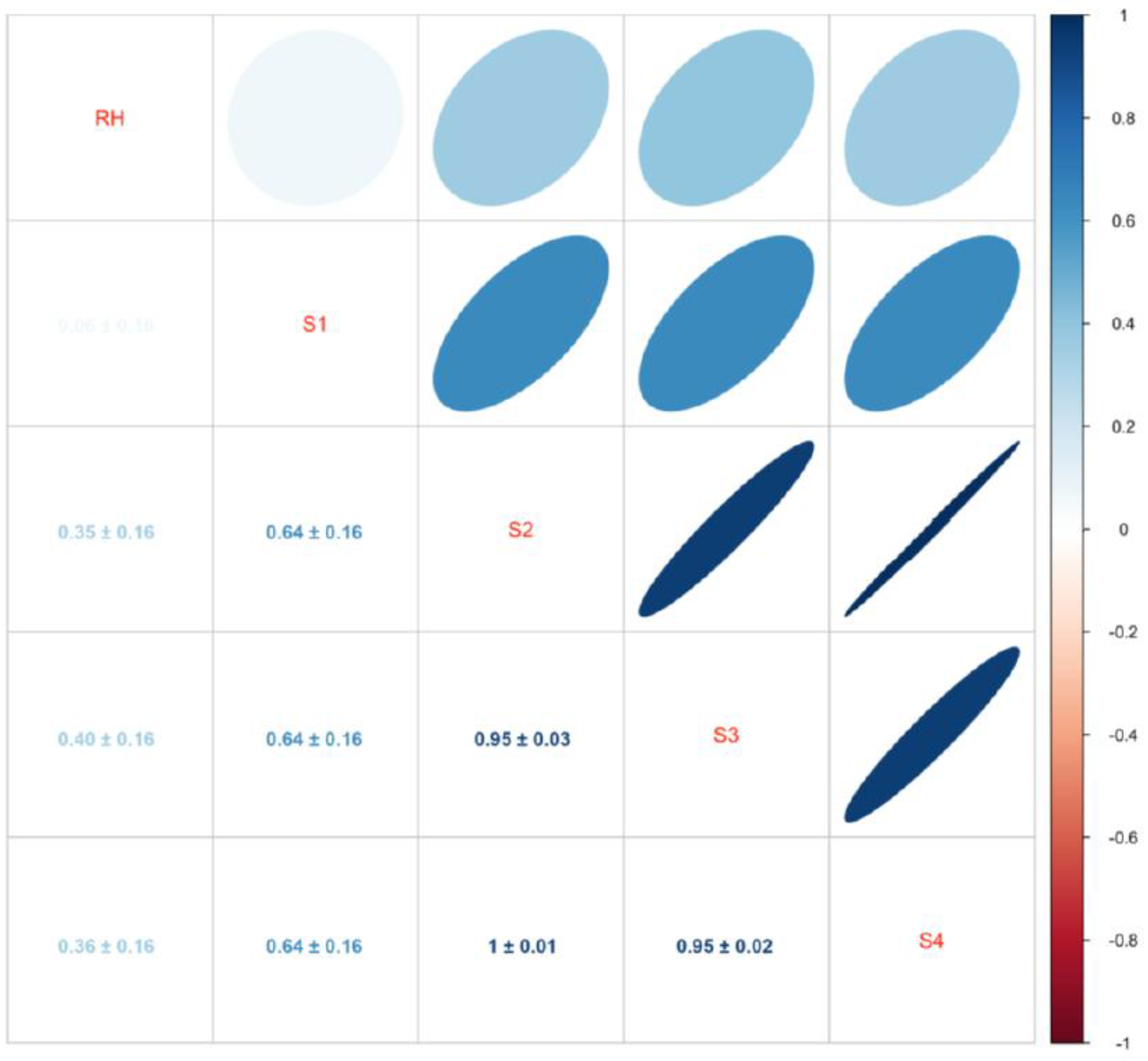
3.2. Changes in Humidity
3.3. Outlier Removal and Smoothing
3.4. Changes in Ventilation Settings
4. Discussion
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Boots, A.W.; van Berkel, J.J.; Dallinga, J.W.; Smolinska, A.; Wouters, E.F.; van Schooten, F.J. The versatile use of exhaled volatile organic compounds in human health and disease. J. Breath Res. 2012, 6, 027108. [Google Scholar] [CrossRef] [PubMed]
- Trefz, P.; Schmidt, M.; Oertel, P.; Obermeier, J.; Brock, B.; Kamysek, S.; Dunkl, J.; Zimmermann, R.; Schubert, J.K.; Miekisch, W. Continuous real time breath gas monitoring in the clinical environment by proton-transfer-reaction-time-of-flight-mass spectrometry. Anal. Chem. 2013, 85, 10321–10329. [Google Scholar] [CrossRef] [PubMed]
- Röck, F.; Barsan, N.; Weimar, U. Electronic nose: current status and future trends. Chem. Rev. 2008, 108, 705–725. [Google Scholar] [CrossRef] [PubMed]
- Boots, A.W.; Bos, L.D.; van der Schee, M.P.; van Schooten, F.-J.; Sterk, P.J. Exhaled Molecular Fingerprinting in Diagnosis and Monitoring: Validating Volatile Promises. Trends Mol. Med. 2015, 21, 633–644. [Google Scholar] [CrossRef] [PubMed]
- Bikov, A.; Lazar, Z.; Horvath, I. Established methodological issues in electronic nose research: How far are we from using these instruments in clinical settings of breath analysis? J. Breath Res. 2015, 9, 034001. [Google Scholar] [CrossRef] [PubMed]
- Fens, N.; van der Schee, M.P.; Brinkman, P.; Sterk, P.J. Exhaled breath analysis by electronic nose in airways disease. Established issues and key questions. Clin. Exp. Allergy 2013, 43, 705–715. [Google Scholar] [CrossRef] [PubMed]
- Montuschi, P.; Mores, N.; Trove, A.; Mondino, C.; Barnes, P.J. The electronic nose in respiratory medicine. Respiration 2013, 85, 72–84. [Google Scholar] [CrossRef] [PubMed]
- Wilson, A.D.; Baietto, M. Advances in Electronic-Nose Technologies Developed for Biomedical Applications. Sensors 2011, 11, 1105–1176. [Google Scholar] [CrossRef] [PubMed]
- Wilson, A.D. Advances in electronic-nose technologies for the detection of volatile biomarker metabolites in the human breath. Metabolites 2015, 5, 140–163. [Google Scholar] [CrossRef] [PubMed]
- Santini, G.; Mores, N.; Penas, A.; Capuano, R.; Mondino, C.; Trove, A.; Macagno, F.; Zini, G.; Cattani, P.; Martinelli, E.; et al. Electronic Nose and Exhaled Breath NMR-Based Metabolomics Applications in Airways Disease. Curr. Top. Med. Chem. 2016, 16, 1610–1630. [Google Scholar] [CrossRef] [PubMed]
- Wilson, A.D. Recent progress in the design and clinical development of electronic-nose technologies. Nanobiosens. Dis. Diagn. 2016, 5, 15–27. [Google Scholar] [CrossRef]
- Zohora, S.E.; Khan, A.M.; Hundewale, N. Chemical sensors employed in electronic noses: A review. In Advances in Computing and Information Technology; Springer: Berlin/Heidelberg, Germany, 2013; Volume 178, pp. 177–184. [Google Scholar]
- Brekelmans, M.P.; Fens, N.; Brinkman, P.; Bos, L.D.; Sterk, P.J.; Tak, P.P.; Gerlag, D.M. Smelling the Diagnosis: The Electronic Nose as Diagnostic Tool in Inflammatory Arthritis. A Case-Reference Study. PLoS ONE 2016, 11, e0151715. [Google Scholar] [CrossRef] [PubMed]
- De Vries, R.; Brinkman, P.; van der Schee, M.P.; Fens, N.; Dijkers, E.; Bootsma, S.K.; de Jongh, F.H.C.; Sterk, P.J. Integration of electronic nose technology with spirometry: validation of a new approach for exhaled breath analysis. J. Breath Res. 2015, 9, 046001. [Google Scholar] [CrossRef] [PubMed]
- Schnabel, R.; Fijten, R.; Smolinska, A.; Dallinga, J.; Boumans, M.-L.; Stobberingh, E.; Boots, A.; Roekaerts, P.; Bergmans, D.; van Schooten, F.-J. Analysis of volatile organic compounds in exhaled breath to diagnose ventilator-associated pneumonia. Sci. Rep. 2015, 5. [Google Scholar] [CrossRef] [PubMed]
- Schnabel, R.M.; Boumans, M.L.L.; Smolinska, A.; Stobberingh, E.E.; Kaufmann, R.; Roekaerts, P.M.; Bergmans, D.C. Electronic nose analysis of exhaled breath to diagnose ventilator-associated pneumonia. Respir. Med. 2015, 109, 1454–1459. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.; Jiang, J.; Zheng, X.; Hui, G. Hairtail (Trichiurus haumela) freshness determination method based on electronic nose. Food Meas. 2015, 9, 541–549. [Google Scholar]
- Jin, J.; Deng, S.; Ying, X.; Ye, X.; Lu, T.; Hui, G. Study of herbal tea beverage discrimination method using electronic nose. Food Meas. 2015, 9, 52–60. [Google Scholar] [CrossRef]
- Jiang, J.; Li, J.; Zheng, F.; Lin, H.; Hui, G. Rapid freshness analysis of mantis shrimps (Oratosquilla oratoria) by using electronic nose. Food Meas. 2016, 10, 48–55. [Google Scholar] [CrossRef]
- Brochard, L.; Martin, G.; Blanch, L.; Pelosi, P.; Belda, F.J.; Jubran, A.; Gattinoni, L.; Mancebo, J.; Ranieri, V.M.; Richard, J.-C.; et al. Clinical review: Respiratory monitoring in the ICU—A consensus of 16. Crit. Care 2012, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Costa, D.K.; Kahn, J.M. Organizing Critical Care for the 21st Century. JAMA 2016, 315, 751–752. [Google Scholar] [CrossRef] [PubMed]
- Bos, L.D.J.; Wang, Y.; Weda, H.; Nijsen, T.M.E.; Janssen, A.P.; Knobel, H.H.; Vink, T.J.; Schultz, M.J.; Sterk, P.J. A simple breath sampling method in intubated and mechanically ventilated critically ill patients. Respir. Physiol. Neurobiol. 2013, 191, 67–74. [Google Scholar] [CrossRef] [PubMed]
- Romain, A.C.; Nicolas, J. Long term stability of metal oxide-based gas sensors for e-nose environmental applications: An overview. Sens. Actuators B Chem. 2010, 146, 502–506. [Google Scholar] [CrossRef]
- Guo, D.; Li, N.; Zhang, D.; Yang, J. A Novel Breath Analysis System Based on Electronic Olfaction. IEEE Trans. Biomed. Eng. 2010, 57, 2753–2763. [Google Scholar]
- Van Lieshout, E.J.; van der Veer, S.N.; Hensbroek, R.; Korevaar, J.C.; Vroom, M.B.; Schultz, M.J. Interference by new-generation mobile phones on critical care medical equipment. Crit. Care 2007, 11. [Google Scholar] [CrossRef] [PubMed]
- Knaus, W.A.; Draper, E.A.; Wagner, D.P.; Zimmerman, J.E. APACHE II: A severity of disease classification system. Crit. Care Med. 1985, 13, 818–829. [Google Scholar] [CrossRef] [PubMed]
- Le Gall, J.-R. A New Simplified Acute Physiology Score (SAPS II) Based on a European/North American Multicenter Study. JAMA 1993, 270, 2957. [Google Scholar] [CrossRef] [PubMed]
- Romain, A.C.; Nicolas, J.; Andre, P. In situ measurement of olfactive pollution with inorganic semiconductors: Limitations due to humidity and temperature influence. Semin. Food Anal. 1997, 2, 283–296. [Google Scholar]
- Gattinoni, L.; Pelosi, P.; Crotti, S.; Valenza, F. Effects of positive end-expiratory pressure on regional distribution of tidal volume and recruitment in adult respiratory distress syndrome. Am. J. Respir. Crit. Care Med. 1995, 151, 1807–1814. [Google Scholar] [CrossRef] [PubMed]
- Kartal, M.; Eray, O.; Rinnert, S.; Goksu, E.; Bektas, F.; Eken, C. ETCO2: A predictive tool for excluding metabolic disturbances in nonintubated patients. Am. J. Emerg. Med. 2011, 29, 65–69. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Value | |
|---|---|---|
| Age in years, median (IQR a) | 67 | 62–75 |
| Male gender, number (%) | 9 | 39 |
| Admission type b, number (%) | ||
| Acute medical | 21 | 91 |
| Planned surgery | 2 | 9 |
| APACHE II score c, median (IQR) | 22 | 19–28 |
| SAPS II score d, median (IQR) | 52 | 42–65 |
| ICU length of stay e, days, median (IQR) | 12 | 9–15 |
| ICU mortality f, number (%) | 10 | 43 |
| Measurement duration in hours, median (IQR) | 51 | 41–65 |
| Sensor | Relative Humidity |
|---|---|
| S1 | −0.056 ± 0.002 |
| S2 | 0.116 ± 0.001 |
| S3 | 0.119 ± 0.001 |
| S4 | 0.118 ± 0.001 |
| Sensor | Minute Volume | etCO2 | Tidal Volume | Inspiratory Pressure | Peak Pressure | PEEP |
|---|---|---|---|---|---|---|
| S1 | −0.292 ± 0.043 | 0.028 ± 0.009 | 28.147 ± 1.362 | 0.164 ± 0.047 | −0.093 ± 0.054 | 0.066 ± 0.019 |
| S2 | −0.177 ± 0.054 | 0.146 ± 0.012 | 39.485 ± 1.743 | 0.091 ± 0.060 | 0.218 ± 0.065 | 0.428 ± 0.024 |
| S3 | −0.500 ± 0.089 | 0.251 ± 0.020 | 60.292 ± 2.862 | −0.728 ± 0.098 | −0.628 ± 0.106 | 0.112 ± 0.041 |
| S4 | −0.219 ± 0.057 | 0.144 ± 0.013 | 41.749 ± 1.846 | 0.041 ± 0.064 | 0.103 ± 0.079 | 0.396 ± 0.026 |
| Sensor | Minute Volume | etCO2 | Tidal Volume | Inspiratory Pressure | Peak Pressure | PEEP |
|---|---|---|---|---|---|---|
| S1 | 0.000 ± 0.015 | 0.000 ± 0.004 | 0.014 ± 0.508 | −0.001 ± 0.018 | 0.000 ± 0.018 | 0.000 ± 0.007 |
| S2 | −0.001 ± 0.015 | 0.000 ± 0.004 | 0.023 ± 0.508 | −0.001 ± 0.018 | 0.000 ± 0.018 | 0.000 ± 0.007 |
| S3 | −0.001 ± 0.015 | 0.000 ± 0.004 | 0.014 ± 0.508 | −0.001 ± 0.018 | 0.000 ± 0.018 | 0.000 ± 0.007 |
| S4 | −0.001 ± 0.015 | 0.000 ± 0.004 | 0.023 ± 0.508 | −0.001 ± 0.018 | 0.000 ± 0.018 | 0.000 ± 0.007 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leopold, J.H.; Abu-Hanna, A.; Colombo, C.; Sterk, P.J.; Schultz, M.J.; Bos, L.D.J. Factors Influencing Continuous Breath Signal in Intubated and Mechanically-Ventilated Intensive Care Unit Patients Measured by an Electronic Nose. Sensors 2016, 16, 1337. https://doi.org/10.3390/s16081337
Leopold JH, Abu-Hanna A, Colombo C, Sterk PJ, Schultz MJ, Bos LDJ. Factors Influencing Continuous Breath Signal in Intubated and Mechanically-Ventilated Intensive Care Unit Patients Measured by an Electronic Nose. Sensors. 2016; 16(8):1337. https://doi.org/10.3390/s16081337
Chicago/Turabian StyleLeopold, Jan Hendrik, Ameen Abu-Hanna, Camilla Colombo, Peter J. Sterk, Marcus J. Schultz, and Lieuwe D. J. Bos. 2016. "Factors Influencing Continuous Breath Signal in Intubated and Mechanically-Ventilated Intensive Care Unit Patients Measured by an Electronic Nose" Sensors 16, no. 8: 1337. https://doi.org/10.3390/s16081337