
Development and Optimization of Nanolipid-Based Formulation of Diclofenac Sodium: In Vitro Characterization and Preclinical Evaluation

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Experimental
2.1. Materials
2.2. Methods
2.2.1. Formulation of Bilosomes
2.2.2. Optimization
2.2.3. Bilosomes Evaluation
2.2.4. Entrapment Efficiency (EE)
2.2.5. Surface Morphology
2.2.6. Thermal Analysis
2.3. In Vitro Drug Release
2.4. Ex Vivo Permeation Study
2.5. In Vivo Study
2.5.1. Bioavailability Study
2.5.2. Pharmacodynamic Study
2.6. Statistical Analysis
3. Result and Discussion
3.1. Optimization
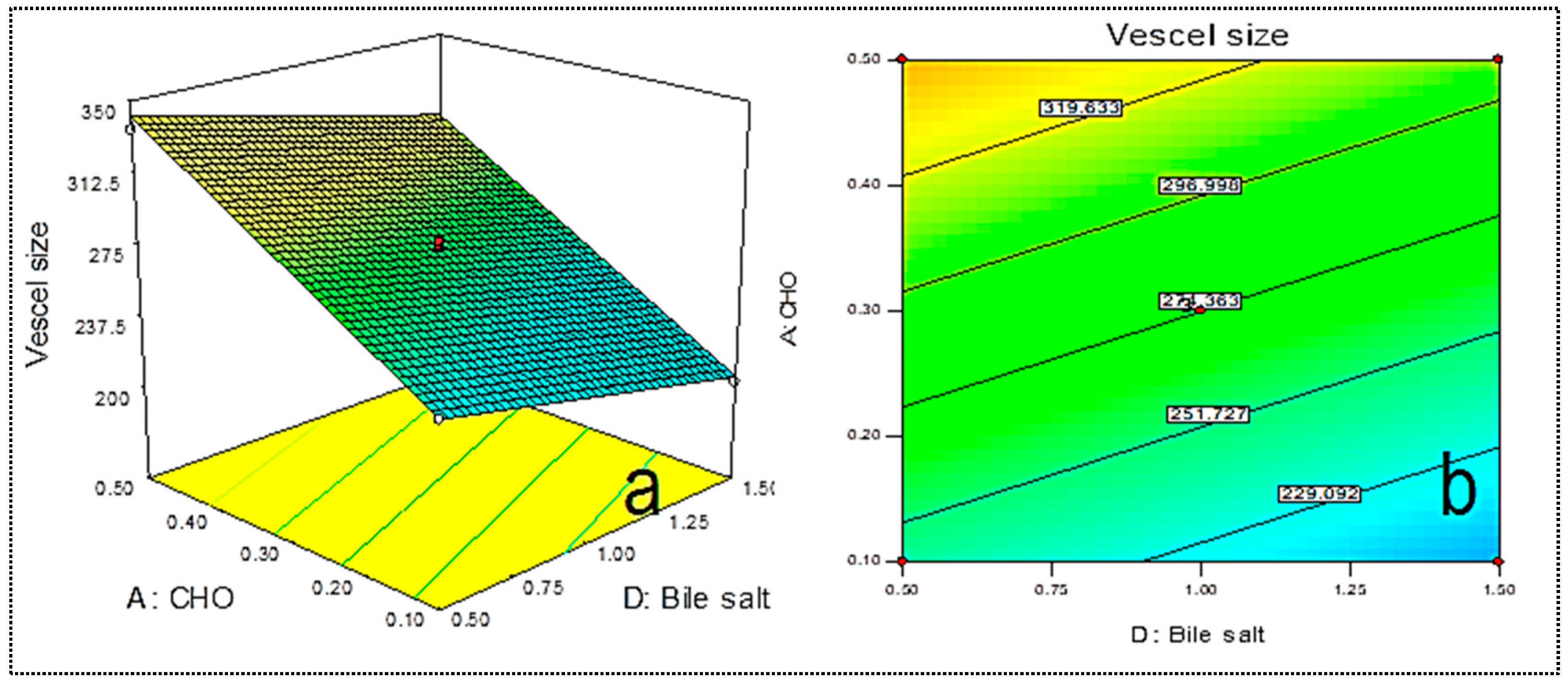
3.2. Effect of Independent Variables over Vesicle Size (R1)
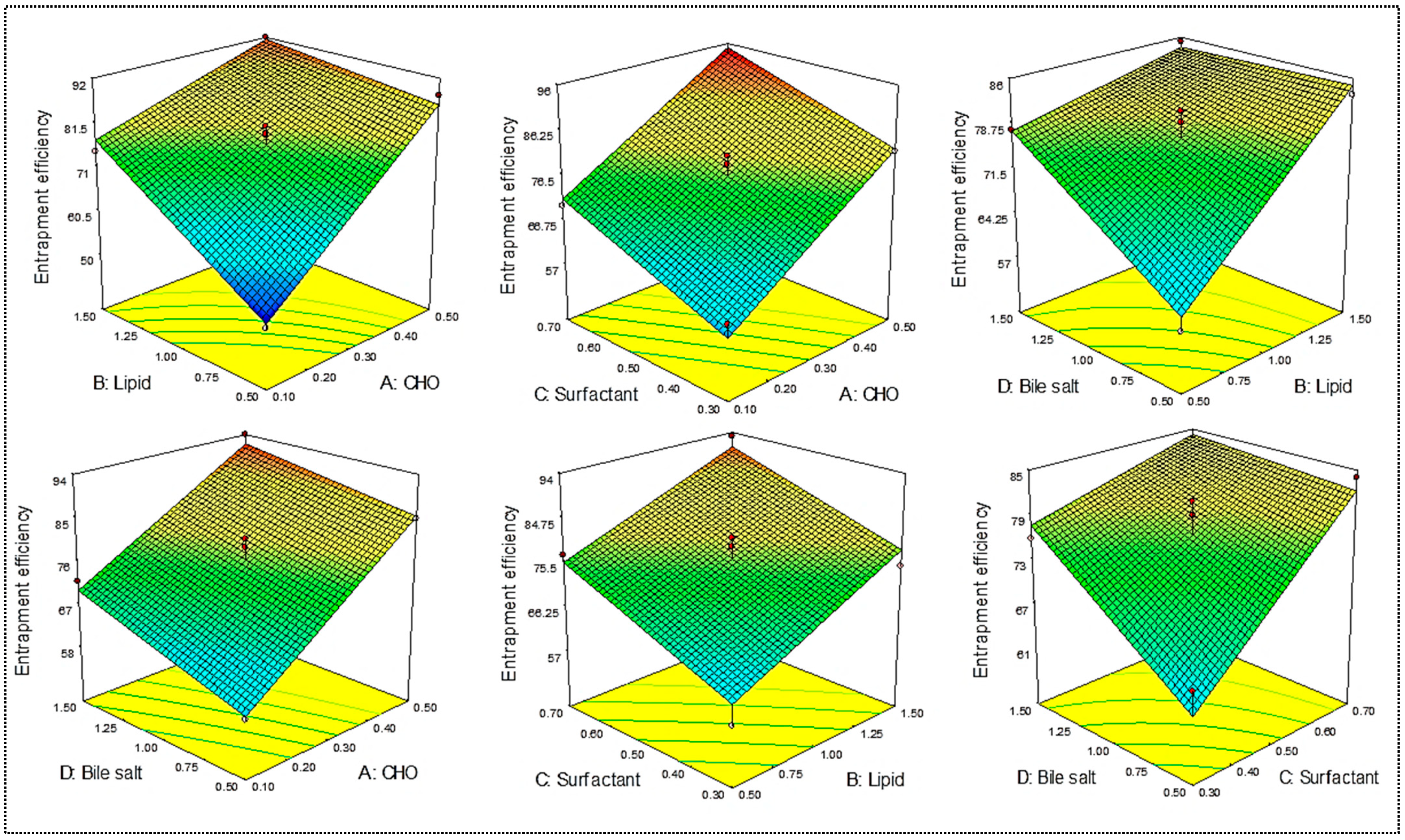
3.3. Effect of Independent Variables (A, B, C, D) on Entrapment Efficiency (R2)
3.4. Optimized Formulation (DC-BMs-opt)
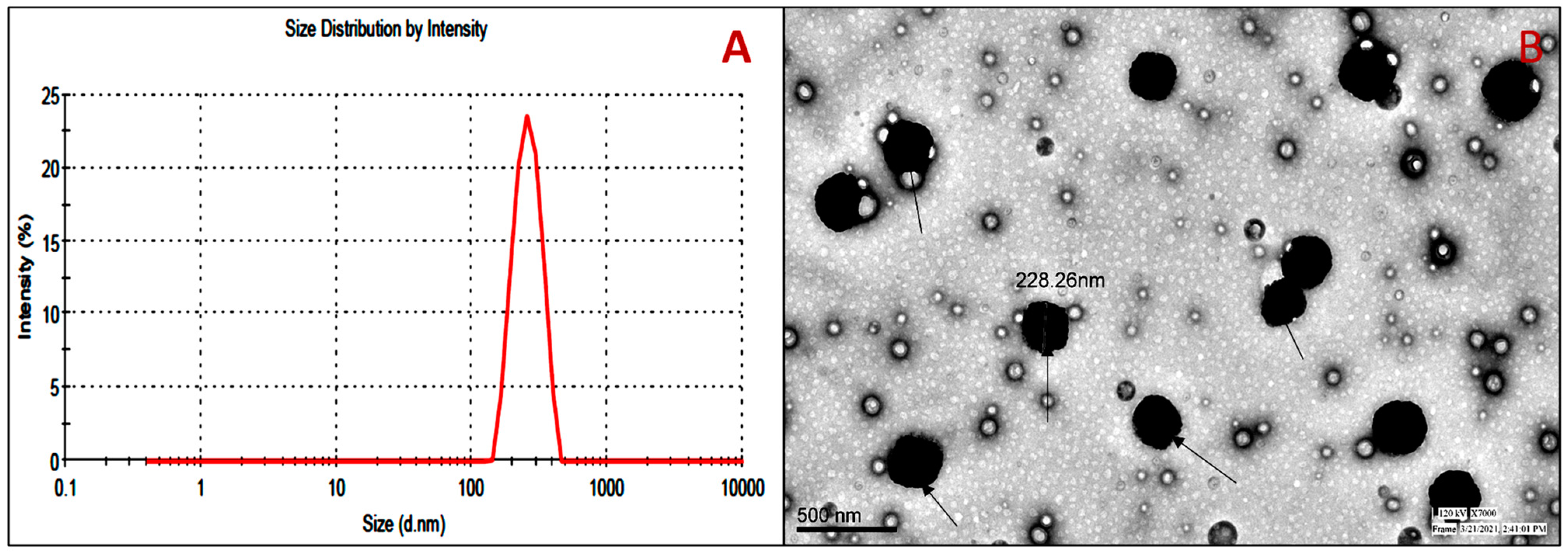
3.5. Vesicle Evaluation
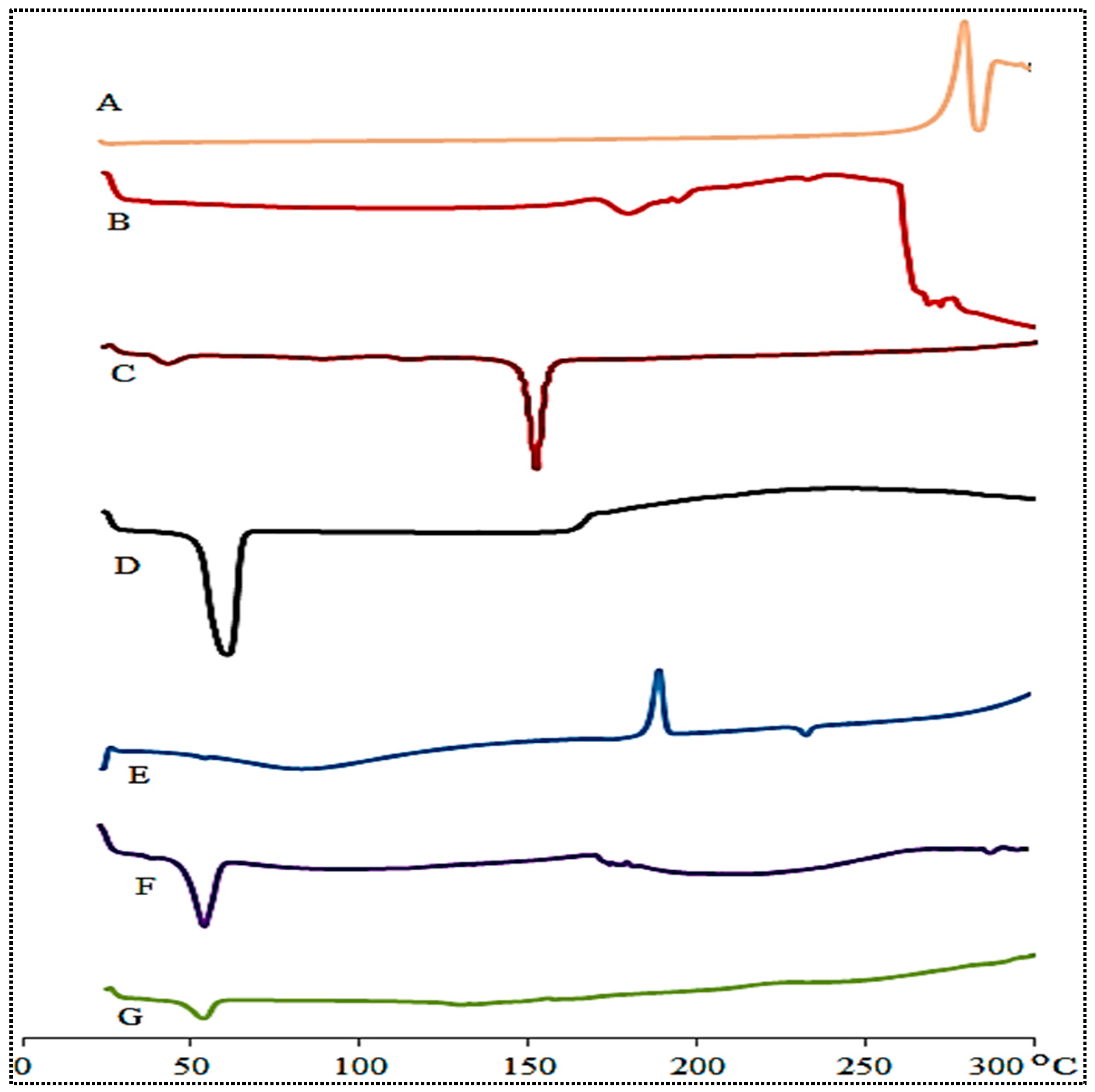
3.6. Thermal Analysis
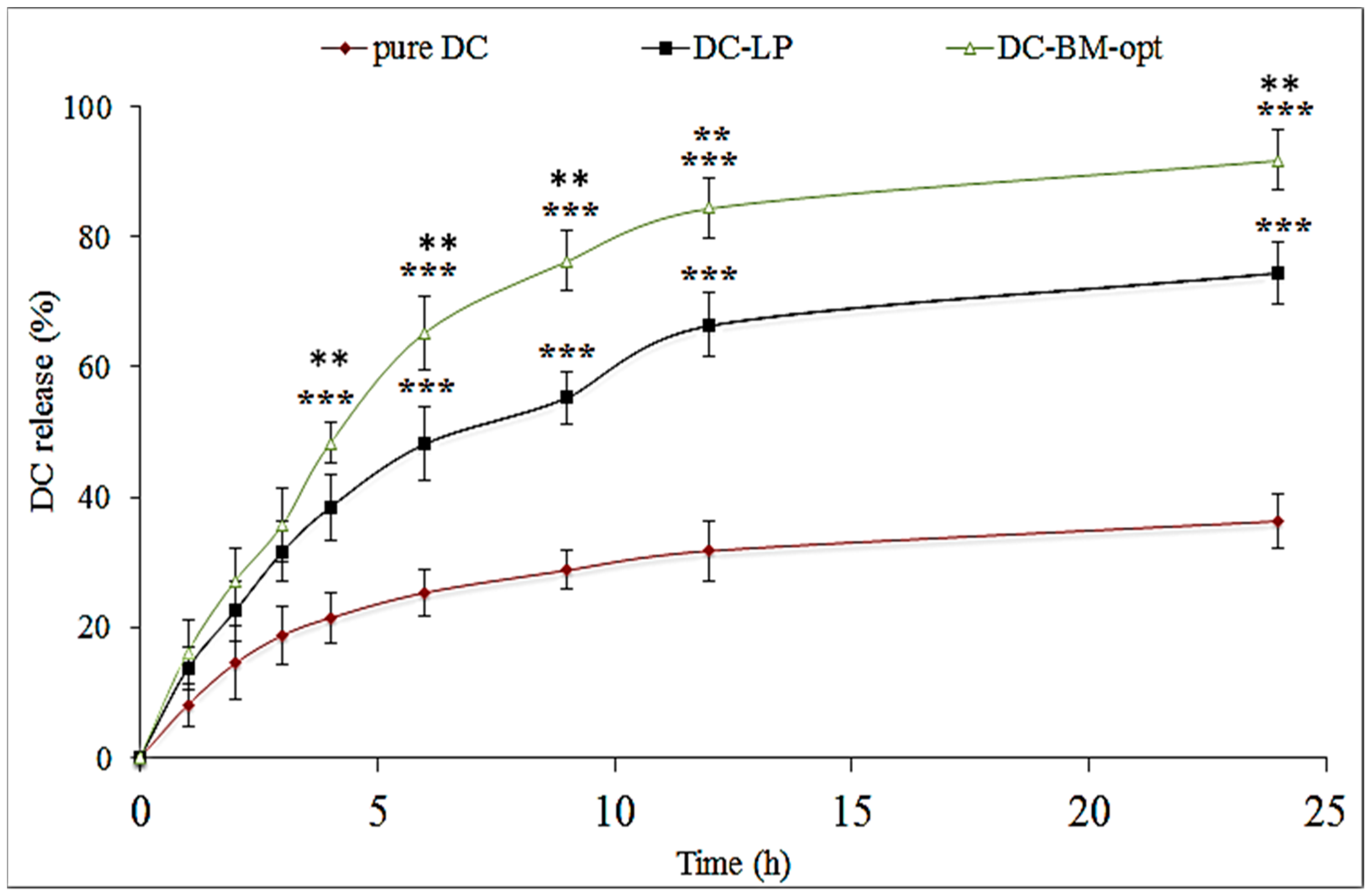
3.7. In Vitro Drug Release
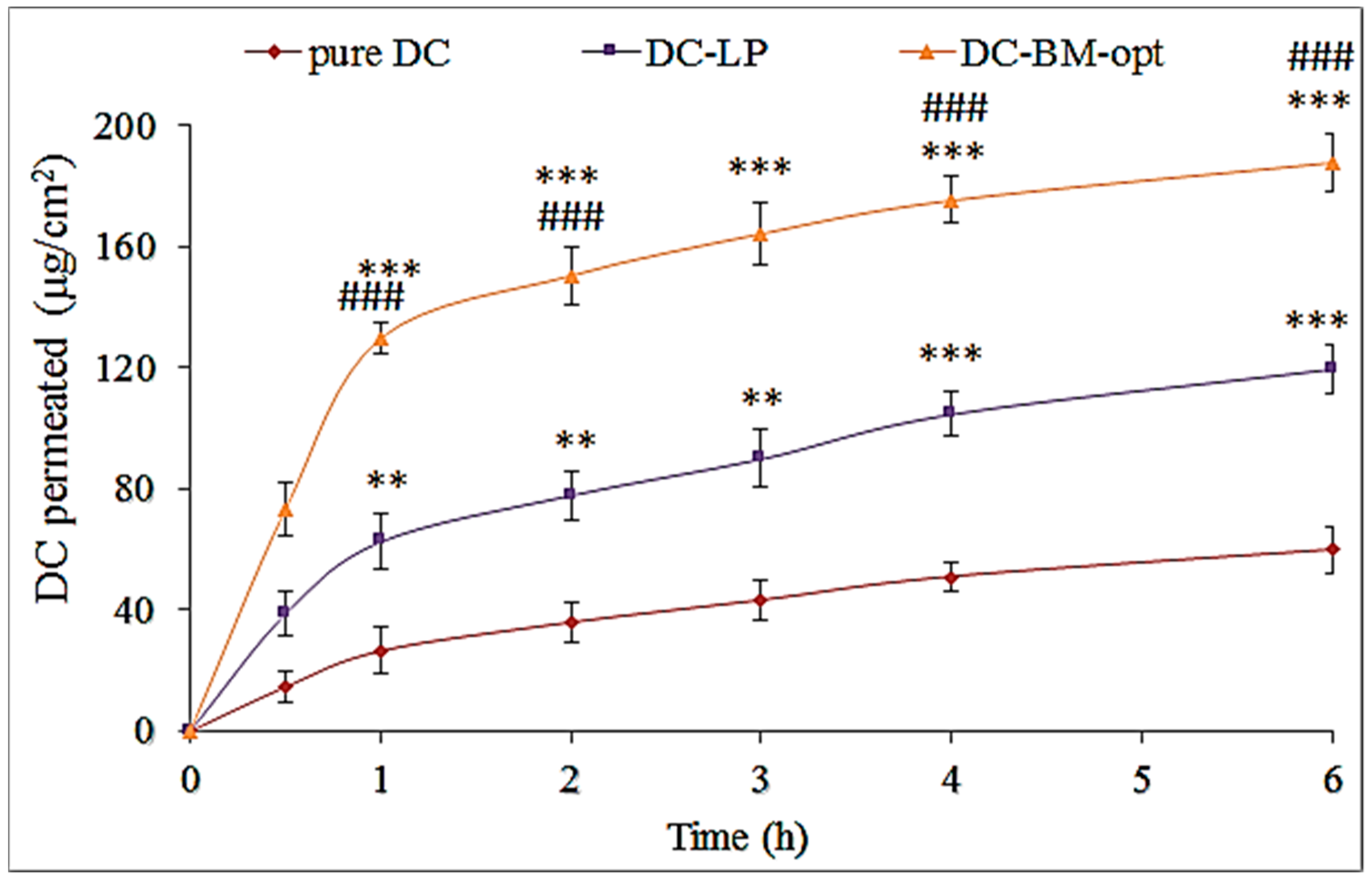
3.8. Ex Vivo Permeation Study
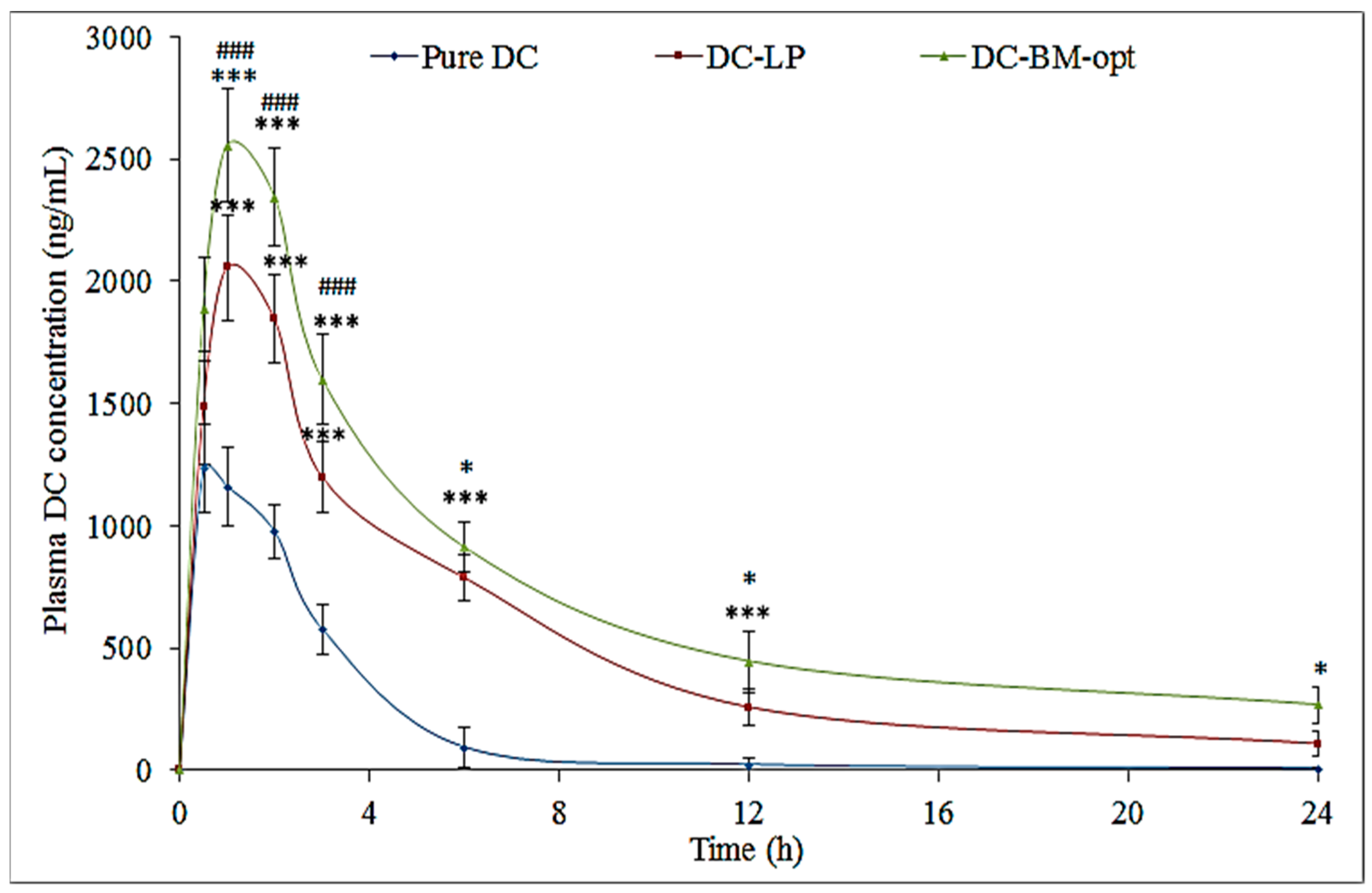
3.9. Bioavailability Study
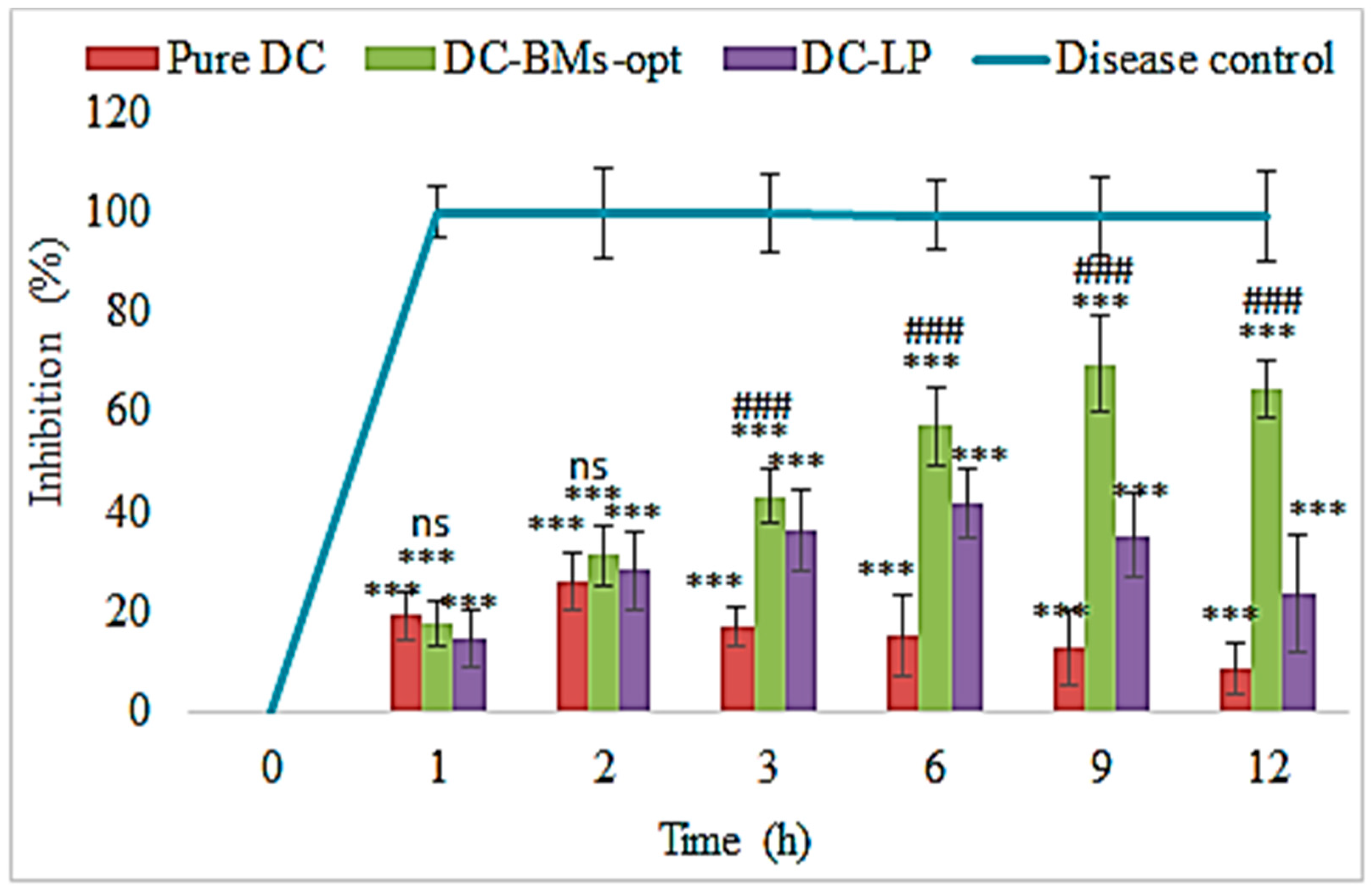
3.10. Pharmacodynamic Study
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Arias, J.L.; Lopez-Viota, M.; López-Viota, J.; Delgado, A.V. Development of iron/ethylcellulose (core/shell) nanoparticles loaded with diclofenac sodium for arthritis treatment. Int. J. Pharm. 2009, 382, 270–276. [Google Scholar] [CrossRef] [PubMed]
- Roth, S.H. Nonsteroidal anti-inflammatory drug gastropathy: New avenues for safety. Clin. Interv. Aging 2011, 6, 125–131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhatia, N.; Katkar, K.; Ashtekar, S. Formulation and evaluation of co-prodrug of flurbiprofen and methocarbamol. Asian J. Pharm. Sci. 2016, 11, 449–458. [Google Scholar] [CrossRef] [Green Version]
- Narayanan, D.; Pillai, G.J.; Nair, S.V.; Menon, D. Effect of formulation parameters on pharmacokinetics, pharmacodynamics, and safety of diclofenac nanomedicine. Drug Deliv. Transl. Res. 2019, 9, 867–878. [Google Scholar] [CrossRef] [PubMed]
- Akbari, J.; Saeedi, M.; Morteza-Semnani, K.; Hashemi, S.M.H.; Babaei, A.; Eghbali, M.; Mohammadi, M.; Rostamkalaei, S.S.; Asare-Addo, K.; Nokhodchi, A. Innovative topical niosomal gel formulation containing diclofenac sodium (niofenac). J. Drug Target. 2022, 30, 108–117. [Google Scholar] [CrossRef] [PubMed]
- Sala, M.; Locher, F.; Bonvallet, M.; Agusti, G.; Elaissari, A.; Fessi, H. Diclofenac Loaded Lipid Nanovesicles Prepared by Double Solvent Displacement for Skin Drug Delivery. Pharm. Res. 2017, 34, 1908–1924. [Google Scholar] [CrossRef] [PubMed]
- Gaur, P.K.; Purohit, S.; Kumar, Y.; Mishra, S.; Bhandari, A. Preparation, characterization and permeation studies of a nanovesicular system containing diclofenac for transdermal delivery. Pharm. Dev. Technol. 2014, 19, 48–54. [Google Scholar] [CrossRef]
- Dianzani, C.; Foglietta, F.; Ferrara, B.; Rosa, A.C.; Muntoni, E.; Gasco, P.; Della Pepa, C.; Canaparo, R.; Serpe, L. Solid lipid nanoparticles delivering anti-inflammatory drugs to treat inflammatory bowel disease: Effects in an in vivo model. World J. Gastroenterol. 2017, 23, 4200–4210. [Google Scholar] [CrossRef]
- Bhalekar, M.R.; Madgulkar, A.R.; Desale, P.S.; Marium, G. Formulation of piperine solid lipid nanoparticles (SLN) for treatment of rheumatoid arthritis. Drug Dev. Ind. Pharm. 2017, 43, 1003–1010. [Google Scholar] [CrossRef]
- Zewail, M.; Nafee, N.; Helmy, M.W.; Boraie, N. Coated nanostructured lipid carriers targeting the joints–An effective and safe approach for the oral management of rheumatoid arthritis. Int. J. Pharm. 2019, 567, 118447. [Google Scholar] [CrossRef]
- Mohanty, S.; Sahoo, A.K.; Konkimalla, V.B.; Pal, A.; Si, S.C. Naringin in Combination with Isothiocyanates as Liposomal Formulations Potentiates the Anti-inflammatory Activity in Different Acute and Chronic Animal Models of Rheumatoid Arthritis. ACS Omega 2020, 5, 28319–28332. [Google Scholar] [CrossRef]
- Al-Mahallawi, A.M.; Abdelbary, A.A.; Aburahma, M.H. Investigating the potential of employing bilosomes as a novel vesicular carrier for transdermal delivery of tenoxicam. Int. J. Pharm. 2015, 485, 329–340. [Google Scholar] [CrossRef]
- Saifi, Z.; Rizwanullah, M.; Mir, S.R.; Amin, S. Bilosomes nanocarriers for improved oral bioavailability of acyclovir: A complete characterization through in vitro, ex-vivo and in vivo assessment. J. Drug Deliv. Sci. Technol. 2020, 57, 101634. [Google Scholar] [CrossRef]
- Bnyan, R.; Khan, I.; Ehtezazi, T.; Saleem, I.; Gordon, S.; O’Neill, F.; Roberts, M. Surfactant Effects on Lipid-Based Vesicles Properties. J. Pharm. Sci. 2018, 107, 1237–1246. [Google Scholar] [CrossRef] [PubMed]
- Shukla, A.; Mishra, V.; Kesharwani, P. Bilosomes in the context of oral immunization: Development, challenges and opportunities. Drug Discov. Today 2016, 21, 888–899. [Google Scholar] [CrossRef] [PubMed]
- Jain, S.; Indulkar, A.; Harde, H.; Agrawal, A.K. Oral mucosal immunization using glucomannosylated bilosomes. J. Biomed. Nanotechnol. 2014, 10, 932–947. [Google Scholar] [CrossRef] [PubMed]
- Guan, P.; Lu, Y.; Qi, J.; Niu, M.; Lian, R.; Hu, F.; Wu, W. Enhanced oral bioavailability of cyclosporine A by liposomes containing a bile salt. Int. J. Nanomed. 2011, 6, 965–974. [Google Scholar]
- Naguib, M.J.; Kamel, A.M.; Negmeldin, A.T.; Elshafeey, A.H.; Elsayed, I. Molecular docking and statistical optimization of taurocholate-stabilized galactose anchored bilosomes for the enhancement of sofosbuvir absorption and hepatic relative targeting efficiency. Drug Deliv. 2020, 27, 996–1009. [Google Scholar] [CrossRef]
- Deng, F.; Bae, Y.H. Bile acid transporter-mediated oral drug delivery. J. Control. Release 2020, 327, 100–116. [Google Scholar] [CrossRef]
- Niu, M.; Lu, Y.; Hovgaard, L.; Guan, P.; Tan, Y.; Lian, R.; Qi, J.; Wu, W. Hypoglycemic activity and oral bioavailability of insulin-loaded liposomes containing bile salts in rats: The effect of cholate type, particle size and administered dose. Eur. J. Pharm. Biopharm. 2012, 2, 265–272. [Google Scholar] [CrossRef]
- Shukla, A.; Singh, B.; Katare, O.P. Significant systemic and mucosal immune response induced on oral delivery of diphtheria toxoid using nano-bilosomes. Br. J. Pharmacol. 2011, 164, 820–827. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shukla, A.; Khatri, K.; Gupta, P.N.; Goyal, A.K.; Mehta, A.; Vyas, S.P. Oral immunization against hepatitis B using bile salt stabilized vesicles (bilosomes). J. Pharm. Pharm. Sci. 2008, 11, 59–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zakaria, M.Y.; Fayad, E.; Althobaiti, F.; Zaki, I.; Abu Almaaty, A.H. Statistical optimization of bile salt deployed nanovesicles as a potential platform for oral delivery of piperine: Accentuated antiviral and anti-inflammatory activity in MERS-CoV challenged mice. Drug Deliv. 2021, 28, 1150–1165. [Google Scholar] [CrossRef]
- El Taweel, M.M.; Aboul-Einien, M.H.; Kassem, M.A.; Elkasabgy, N.A. Intranasal Zolmitriptan-Loaded Bilosomes with Extended Nasal Mucociliary Transit Time for Direct Nose to Brain Delivery. Pharmaceutics 2021, 13, 1828. [Google Scholar] [CrossRef] [PubMed]
- Ammar, H.; Ghorab, M.; Kamel, R.; Salama, A.H. A trial for the design and optimization of pH-sensitive microparticles for intestinal delivery of cinnarizine. Drug Deliv. Transl. Res. 2016, 6, 195–209. [Google Scholar] [CrossRef]
- Bhattacharya, S.S.; Banerjee, S.; Ghosh, A.K.; Chattopadhyay, P.; Verma, A.; Ghosh, A. A RP-HPLC method for quantification of diclofenac sodium released from biological macromolecules. Int. J. Biol. Macromol. 2013, 58, 354–359. [Google Scholar] [CrossRef] [PubMed]
- Albash, R.; Elmahboub, Y.; Baraka, K.; Abdellatif, M.M.; Alaa-Eldin, A.A. Ultra-deformable liposomes containing terpenes (terpesomes) loaded fenticonazole nitrate for treatment of vaginal candidiasis: Box-Behnken design optimization, comparative ex vivo and in vivo studies. Drug Deliv. 2020, 27, 1514–1523. [Google Scholar] [CrossRef]
- Shaker, S.; Gardouh, A.R.; Ghorab, M.M. Factors affecting liposomes particle size prepared by ethanol injection method. Res. Pharm. Sci. 2017, 12, 346–352. [Google Scholar] [CrossRef]
- Wu, Y.N.; Xu, Y.L.; Sun, W.X. Preparation and particle size controlling of papain nanoliposomes. J. Shanghai Jiaotong Univ. Agric. Sci. 2007, 25, 105–109. [Google Scholar]
- Taghizadeh, S.M.; Bajgholi, S. A new liposomal-drug-in-adhesive patch for transdermal delivery of sodium diclofenac. J. Biomater. Nanobiotechnol. 2011, 2, 576–581. [Google Scholar] [CrossRef] [Green Version]
- Waglewska, E.; Pucek-Kaczmarek, A.; Bazylińska, U. Novel Surface-Modified Bilosomes as Functional and Biocompatible Nanocarriers of Hybrid Compounds. Nanomaterials 2020, 10, 2472. [Google Scholar] [CrossRef] [PubMed]
- Albash, R.; El-Nabarawi, M.A.; Refai, H.; Abdelbary, A.A. Tailoring of PEGylated bilosomes for promoting the transdermal delivery of olmesartan medoxomil: In-vitro characterization, ex-vivo permeation and in-vivo assessment. Int. J. Nanomed. 2019, 14, 6555–6574. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fahmy, A.M.; Hassan, M.; El-Setouhy, D.A.; Tayel, S.A.; Al-Mahallawi, A.M. Statistical optimization of hyaluronic acid enriched ultradeformable elastosomes for ocular delivery of voriconazole via Box-Behnken design: In vitro characterization and in vivo evaluation. Drug Deliv. 2021, 28, 77–86. [Google Scholar] [CrossRef] [PubMed]
- Rushmi, Z.T.; Akter, N.; Mow, R.J.; Afroz, M.; Kazi, M.; de Matas, M.; Rahman, M.; Shariare, M.H. The impact of formulation attributes and process parameters on black seed oil loaded liposomes and their performance in animal models of analgesia. Saudi Pharm. J. 2017, 25, 404–412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shivhare, U.D.; Ambulkar, D.U.; Mathur, V.B.; Bhusari, K.P.; Godbole, M.D. Formulation and evaluation of pentoxifylline liposome formulation. Digest J. Nanomater. Biostruct. 2009, 4, 857–862. [Google Scholar]
- Maritim, S.; Boulas, P.; Lin, Y. Comprehensive analysis of liposome formulation parameters and their influence on encapsulation, stability and drug release in glibenclamide liposomes. Int. J. Pharm. 2021, 592, 120051. [Google Scholar] [CrossRef]
- Sun, J.; Deng, Y.; Wang, S.; Cao, J.; Gao, X.; Dong, X. Liposomes incorporating sodium deoxycholate for hexamethylmelamine (HMM) oral delivery: Development, characterization, and in vivo evaluation. Drug Deliv. 2010, 17, 164–170. [Google Scholar] [CrossRef]
- Danaei, M.; Dehghankhold, M.; Ataei, S.; Hasanzadeh Davarani, F.; Javanmard, R.; Dokhani, A.; Khorasani, S.; Mozafari, M.R. Impact of Particle Size and Polydispersity Index on the Clinical Applications of Lipidic Nanocarrier Systems. Pharmaceutics 2018, 10, 57. [Google Scholar] [CrossRef] [Green Version]
- Ozturk, A.A.; Namlı, İ.; Güleç, K.; Kıyan, H.T. Diclofenac sodium loaded PLGA nanoparticles for inflammatory diseases with high anti-inflammatory properties at low dose: Formulation, characterization and in vivo HET-CAM analysis. Microvasc. Res. 2020, 130, 103991. [Google Scholar] [CrossRef]
- Wu, I.Y.; Bala, S.; Basnet, N.S.; Cagno, M.P. Interpreting non-linear drug diffusion data: Utilizing Korsmeyer-Peppas model to study drug release from liposomes. Eur. J. Pharm. Sci. 2019, 138, 105026. [Google Scholar] [CrossRef]
- Shanmugam, S.; Song, C.K.; Sriraman, S.N.; Baskaran, R.; Yong, C.S.; Choi, H.G.; Kim, D.D.; Woo, J.S.; Yoo, B.K. Physicochemical Characterization and Skin Permeation of Liposome Formulations Containing Clindamycin Phosphate. Arch. Pharm. Res. 2009, 32, 1067–1075. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Lee, J.; Choi, Y. Skin permeation enhancement of ascorbyl palmitate by liposomal hydrogel (lipogel) formulation and electrical assistance. Biol. Pharm. Bull. 2007, 30, 393–396. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elnaggar, Y.S. Multifaceted applications of bile salts in pharmacy: An emphasis on nanomedicine. Int. J. Nanomed. 2015, 10, 3955–3971. [Google Scholar] [CrossRef] [PubMed] [Green Version]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Code | Formulation Factor | Responses | ||||
|---|---|---|---|---|---|---|
| CHO (A; %) | Lipid (B; %) | Surfactant (C; %) | Bile Salt (D; %) | Vesicle Size (nm; R1) | Entrapment Efficiency (%; R2) | |
| 1 | 0.1 | 0.5 | 0.5 | 1 | 169.34 | 50.23 |
| 2 | 0.5 | 0.5 | 0.5 | 1 | 284.53 | 88.23 |
| 3 | 0.1 | 1.5 | 0.5 | 1 | 275.34 | 75.43 |
| 4 | 0.5 | 1.5 | 0.5 | 1 | 380.14 | 92.32 |
| 5 | 0.3 | 1 | 0.3 | 0.5 | 328.12 | 65.02 |
| 6 | 0.3 | 1 | 0.7 | 0.5 | 260.34 | 84.12 |
| 7 | 0.3 | 1 | 0.3 | 1.5 | 291.65 | 76.32 |
| 8 | 0.3 | 1 | 0.7 | 1.5 | 218.54 | 81.32 |
| 9 | 0.1 | 1 | 0.5 | 0.5 | 243.45 | 58.43 |
| 10 | 0.5 | 1 | 0.5 | 0.5 | 335.27 | 85.12 |
| 11 | 0.1 | 1 | 0.5 | 1.5 | 203.16 | 72.02 |
| 12 | 0.5 | 1 | 0.5 | 1.5 | 297.65 | 94.03 |
| 13 | 0.3 | 0.5 | 0.3 | 1 | 248.24 | 57.23 |
| 14 | 0.3 | 1.5 | 0.3 | 1 | 357.00 | 75.12 |
| 15 | 0.3 | 0.5 | 0.7 | 1 | 200.43 | 77.32 |
| 16 | 0.3 | 1.5 | 0.7 | 1 | 298.14 | 93.11 |
| 17 | 0.1 | 1 | 0.3 | 1 | 256.76 | 60.23 |
| 18 | 0.5 | 1 | 0.3 | 1 | 345.65 | 81.87 |
| 19 | 0.1 | 1 | 0.7 | 1 | 194.54 | 70.21 |
| 20 | 0.5 | 1 | 0.7 | 1 | 290.00 | 90.24 |
| 21 | 0.3 | 0.5 | 0.5 | 0.5 | 242.87 | 57.25 |
| 22 | 0.5 | 1 | 0.7 | 1 | 341.54 | 83.51 |
| 23 | 0.3 | 0.5 | 0.5 | 1.5 | 210.00 | 77.87 |
| 24 | 0.3 | 1.5 | 0.5 | 1.5 | 306.23 | 85.23 |
| 25 | 0.3 | 1 | 0.5 | 1 | 270.21 | 79.01 |
| 26 | 0.3 | 1 | 0.5 | 1 | 270.43 | 79.09 |
| 27 | 0.3 | 1 | 0.5 | 1 | 269.36 | 80.87 |
| Source | Vesicle Size (VS) | Entrapment Efficiency (EE) |
|---|---|---|
| Model | Linear | 2F1 |
| Adjusted R2 | 0.9900 | 0.9318 |
| R2 | 0.9915 | 0.9580 |
| Predicted R2 | 0.9867 | 0.8781 |
| %CV | 1.96 | 4.10 |
| Adequate precision | 85.98 | 21.95 |
| SD | 5.37 | 3.14 |
| Vesicle Size (VS) | |||||
|---|---|---|---|---|---|
| Source | Sum of Squares | Mean Square | F-Value | p-Value Prob > F | Remark |
| Model (2nd order) | 74,666.22 | 18,666.55 | 646.03 | <0.0001 | Significant |
| A-CHO | 29,058.51 | 29,058.51 | 1005.69 | <0.0001 | -- |
| B-Lipid | 30,284.67 | 30,284.67 | 1048.13 | <0.0001 | -- |
| C-Surfactant | 11,128.26 | 11,128.26 | 385.14 | <0.0001 | -- |
| D-Bile salt | 4194.78 | 4194.784 | 145.17 | <0.0001 | -- |
| Residual | 635.66 | 28.89394 | -- | -- | -- |
| Lack of Fit | 631.00 | 31.55001 | 13.52 | 0.0710 | NS |
| Pure Error | 4.66 | 2.333333 | -- | -- | -- |
| Total | 75,301.89 | -- | -- | -- | -- |
| Entrapment efficiency (EE) | |||||
| Model | 3599.88 | 359.98 | 36.53 | <0.0001 | Significant |
| A-CHO | 1779.01 | 1779.01 | 180.54 | <0.0001 | -- |
| B-Lipid | 778.43 | 778.43 | 79.00 | <0.0001 | -- |
| C-Surfactant | 544.05 | 544.05 | 55.21 | <0.0001 | -- |
| D-Bile salt | 239.41 | 239.41 | 24.29 | 0.0002 | -- |
| AB | 110.25 | 110.25 | 11.18 | 0.0041 | -- |
| AC | 0.66 | 0.66 | 0.06 | 0.7985 | -- |
| AD | 6.25 | 6.25 | 0.63 | 0.4374 | -- |
| BC | 1.22 | 1.22 | 0.12 | 0.7294 | -- |
| BD | 91.58 | 91.58 | 9.29 | 0.0077 | -- |
| CD | 49 | 49 | 4.97 | 0.0404 | -- |
| Residual | 157.65 | 9.85 | -- | -- | -- |
| Lack of Fit | 155.44 | 11.10 | 10.04 | 0.0942 | NS |
| Pure Error | 2.21 | 1.105 | -- | -- | -- |
| Total | 3757.54 | -- | -- | -- | -- |
| Type of Model | R2 |
|---|---|
| Zero model | 0.7344 |
| First order | 0.9257 |
| Higuchi model | 0.7744 |
| Korsmeyer–Peppas | 0.9354, n = 0.58 |
| Hixon–Crowell model | 0.8673 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zafar, A.; Alruwaili, N.K.; Imam, S.S.; Yasir, M.; Alsaidan, O.A.; Alquraini, A.; Rawaf, A.; Alsuwayt, B.; Anwer, M.K.; Alshehri, S.; et al. Development and Optimization of Nanolipid-Based Formulation of Diclofenac Sodium: In Vitro Characterization and Preclinical Evaluation. Pharmaceutics 2022, 14, 507. https://doi.org/10.3390/pharmaceutics14030507
Zafar A, Alruwaili NK, Imam SS, Yasir M, Alsaidan OA, Alquraini A, Rawaf A, Alsuwayt B, Anwer MK, Alshehri S, et al. Development and Optimization of Nanolipid-Based Formulation of Diclofenac Sodium: In Vitro Characterization and Preclinical Evaluation. Pharmaceutics. 2022; 14(3):507. https://doi.org/10.3390/pharmaceutics14030507
Chicago/Turabian StyleZafar, Ameeduzzafar, Nabil K Alruwaili, Syed Sarim Imam, Mohd Yasir, Omar Awad Alsaidan, Ali Alquraini, Alenazy Rawaf, Bader Alsuwayt, Md. Khalid Anwer, Sultan Alshehri, and et al. 2022. "Development and Optimization of Nanolipid-Based Formulation of Diclofenac Sodium: In Vitro Characterization and Preclinical Evaluation" Pharmaceutics 14, no. 3: 507. https://doi.org/10.3390/pharmaceutics14030507