
Similar Piperacillin/Tazobactam Target Attainment in Obese versus Nonobese Patients despite Differences in Interstitial Tissue Fluid Pharmacokinetics

 , , , ,
, , , ,  ,
,
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Design and Patient Population
2.2. Bioanalysis of Piperacillin Concentrations
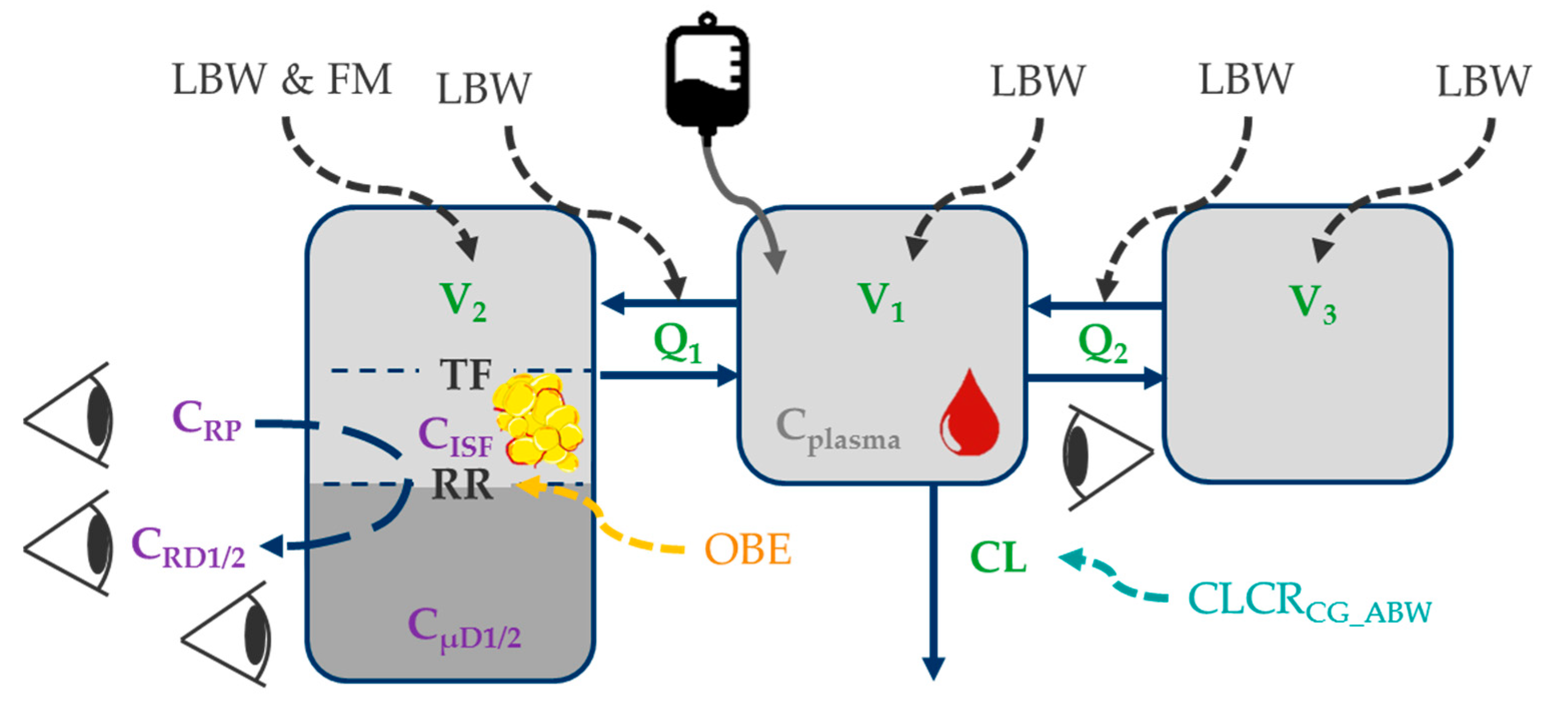
2.3. Population Pharmacokinetic Model and Identification of Body Size Descriptors
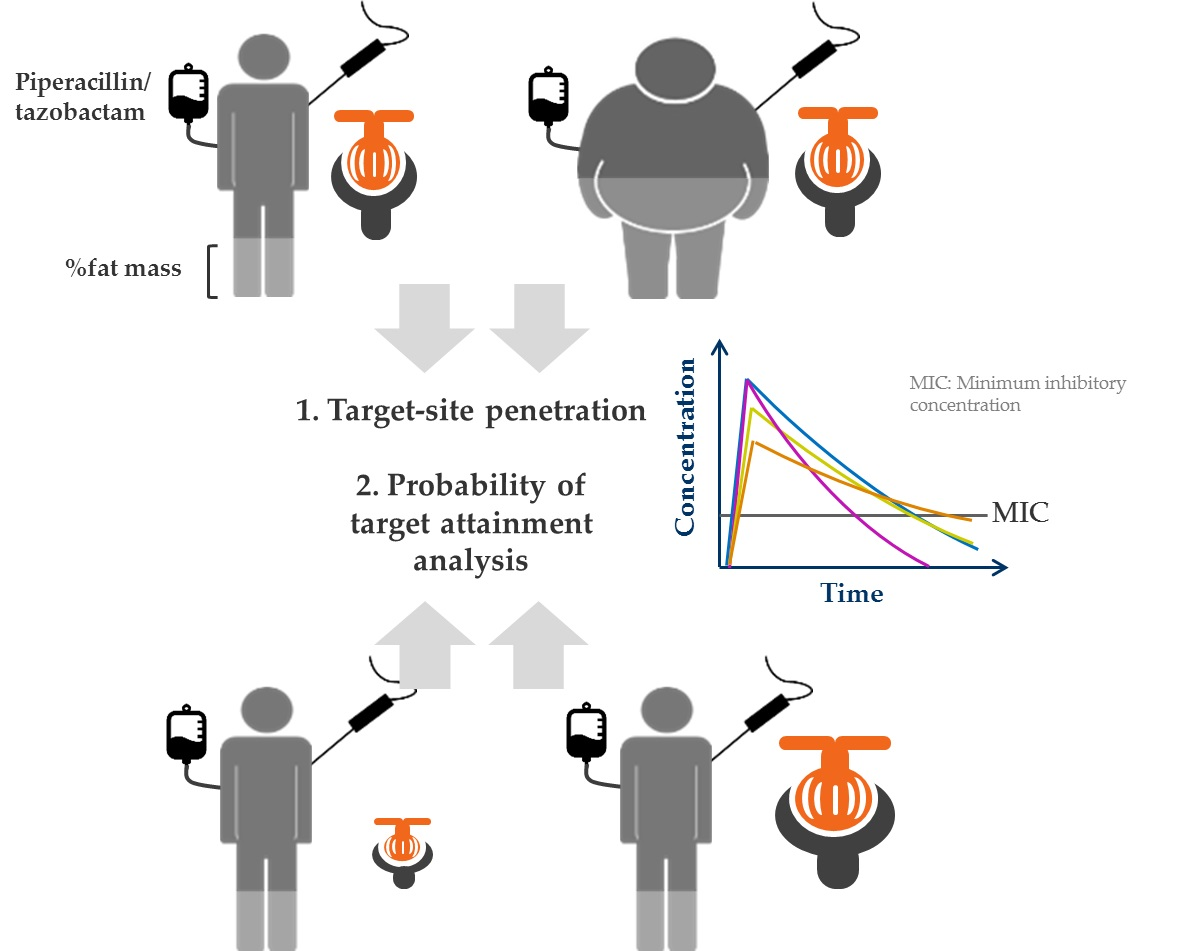
2.4. Target-Site Penetration in Obese and Nonobese Patients
- (1)
- Nonobese, healthy renal function patient
- (2)
- Morbidly obese, healthy renal function patient
- (3)
- Nonobese, renally impaired patient
- (4)
- Nonobese, hyperfiltration patient
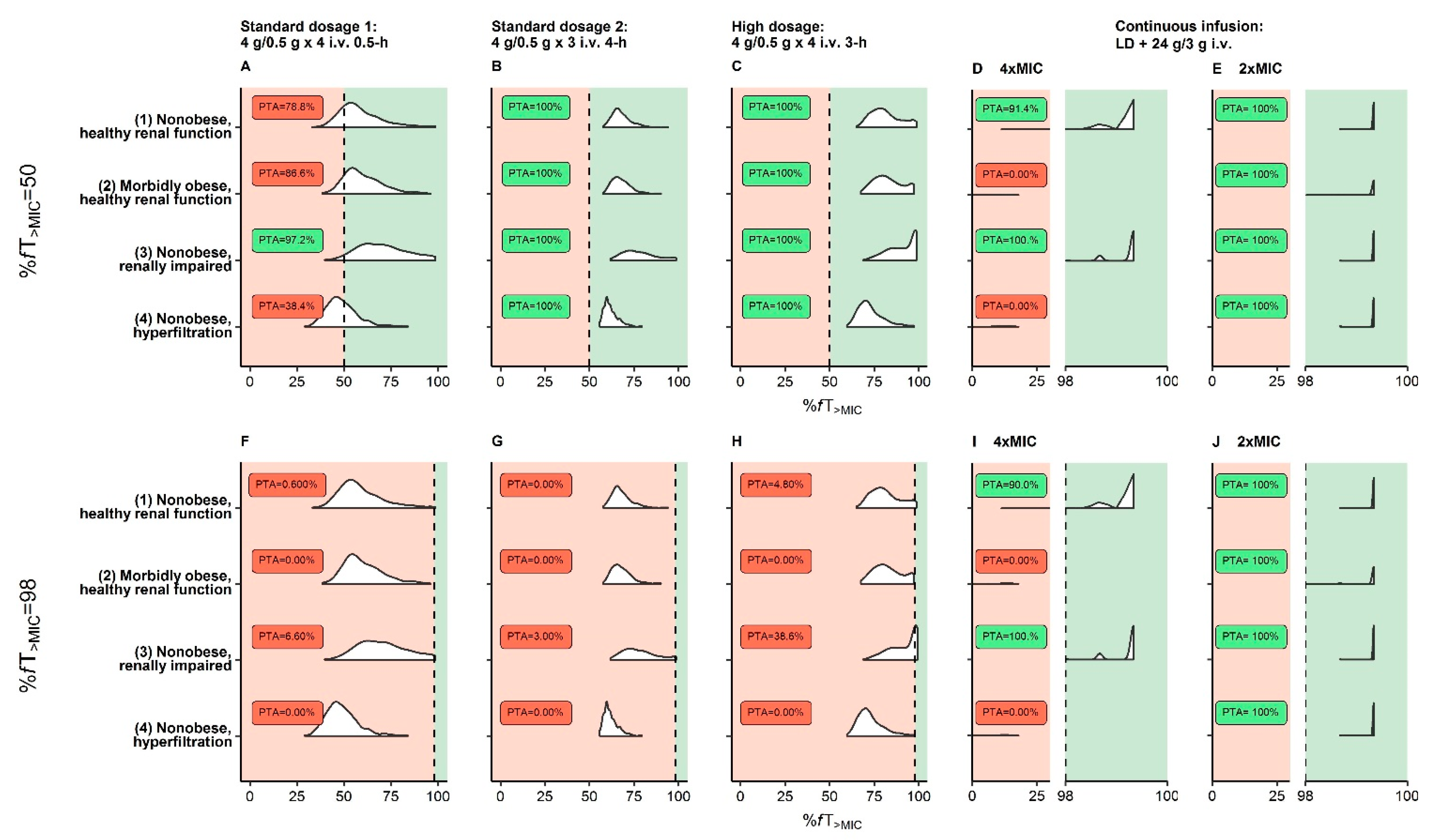
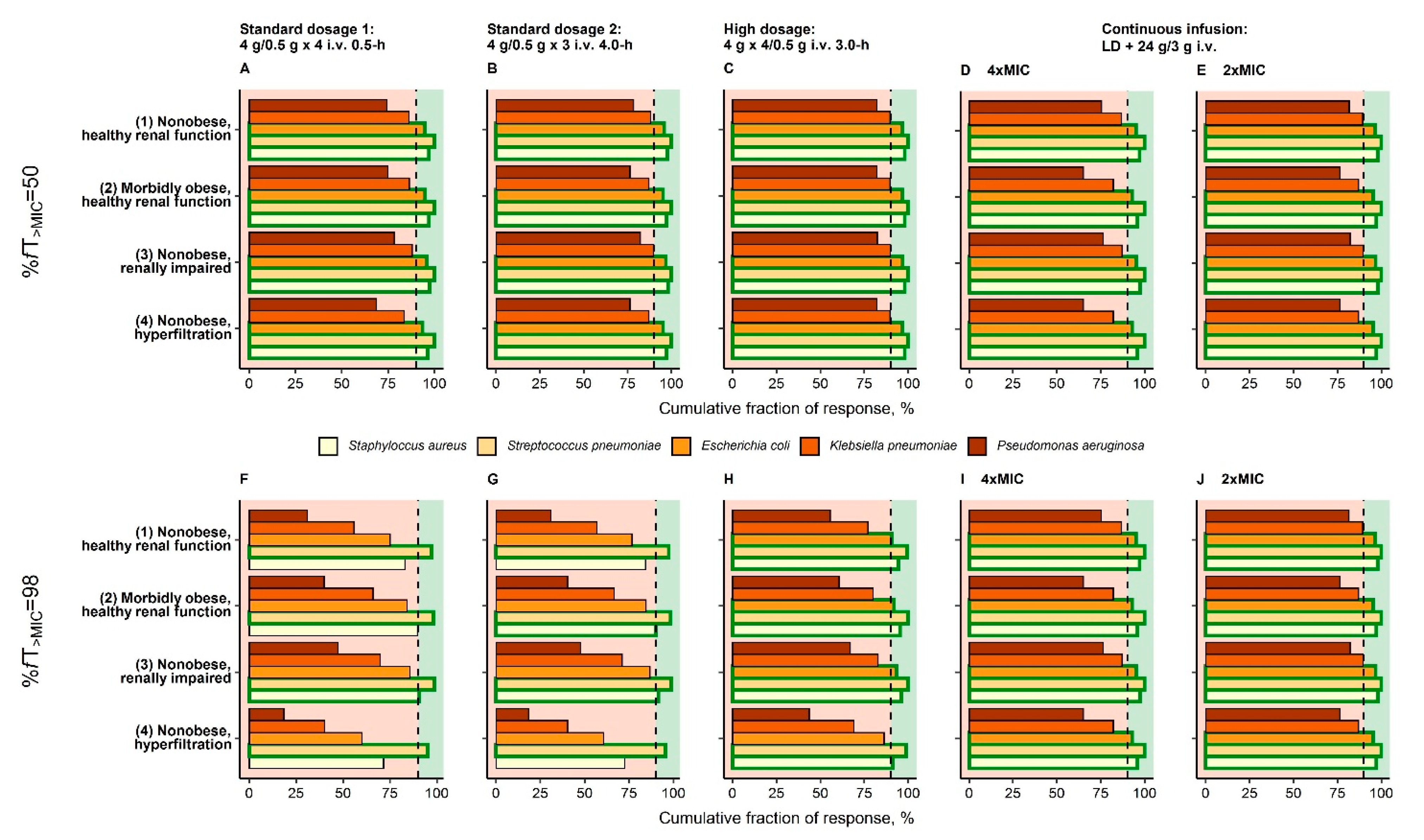
2.5. Evaluation of Clinically Relevant Piperacillin/Tazobactam Dosing Regimens
3. Results
3.1. Patient Population
3.2. Population Pharmacokinetic Model and Identification of Body Size Descriptors
3.3. Target-Site Penetration in Obese and Nonobese Patients
3.4. Evaluation of Clinically Relevant Piperacillin/Tazobactam Dosing Regimens
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Blüher, M. Obesity: Global epidemiology and pathogenesis. Nat. Rev. Endocrinol. 2019, 15, 288–298. [Google Scholar] [CrossRef]
- Hales, C.M.; Carroll, M.D.; Fryar, C.D.; Ogden, C.L. Prevalence of Obesity and Severe Obesity Among Adults: United States, 2017–2018. NCHS Data Brief 2020, 360, 1–8. [Google Scholar]
- Ward, Z.J.; Bleich, S.N.; Cradock, A.L.; Barrett, J.L.; Giles, C.M.; Flax, C.; Long, M.W.; Gortmaker, S.L. Projected U.S. State-Level Prevalence of Adult Obesity and Severe Obesity. N. Engl. J. Med. 2019, 381, 2440–2450. [Google Scholar] [CrossRef] [PubMed]
- Löfgren, M.; Poromaa, I.S.; Stjerndahl, J.H.; Renström, B. Postoperative infections and antibiotic prophylaxis for hysterectomy in Sweden: A study by the Swedish National Register for Gynecologic Surgery. Acta Obstet. Gynecol. Scand. 2004, 83, 1202–1207. [Google Scholar] [CrossRef]
- Olsen, M.A.; Mayfield, J.; Lauryssen, C.; Polish, L.B.; Jones, M.; Vest, J.; Fraser, V. Risk factors for surgical site infection in spinal surgery. J. Neurosurg. Spine 2003, 98, 149–155. [Google Scholar] [CrossRef] [Green Version]
- Baik, I.; Curhan, G.C.; Rimm, E.B.; Bendich, A.; Willett, W.C.; Fawzi, W.W. A Prospective Study of Age and Lifestyle Factors in Relation to Community-Acquired Pneumonia in US Men and Women. Arch. Intern. Med. 2000, 160, 3082–3088. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McDonald, S.P.; Collins, J.F.; Rumpsfeld, M.; Johnson, D.W. Obesity is a Risk Factor for Peritonitis in the Australian and New Zealand Peritoneal Dialysis Patient Populations. Perit. Dial. Int. 2004, 24, 340–346. [Google Scholar] [CrossRef]
- Alobaid, A.S.; Hites, M.; Lipman, J.; Taccone, F.S.; Roberts, J.A. Effect of obesity on the pharmacokinetics of antimicrobials in critically ill patients: A structured review. Int. J. Antimicrob. Agents 2016, 47, 259–268. [Google Scholar] [CrossRef]
- Ehmann, L.; Zoller, M.; Minichmayr, I.K.; Scharf, C.; Huisinga, W.; Zander, J.; Kloft, C. Development of a dosing algorithm for meropenem in critically ill patients based on a population pharmacokinetic/pharmacodynamic analysis. Int. J. Antimicrob. Agents 2019, 43, 309–317. [Google Scholar] [CrossRef]
- Busse, D.; Simon, P.; Schmitt, L.; Petroff, D.; Dorn, C.; Dietrich, A.; Zeitlinger, M.; Huisinga, W.; Michelet, R.; Wrigge, H.; et al. Comparative Plasma and Target-Site Pharmacokinetics of Meropenem Demonstrate the Need for Increasing Dose and Infusion Duration in Obese and Non-Obese Patients. Clin. Pharmacokinet. 2021. accepted. [Google Scholar]
- Keizer, R.J.; Ter Heine, R.; Frymoyer, A.; Lesko, L.J.; Mangat, R.; Goswami, S. Model-Informed Precision Dosing at the Bedside: Scientific Challenges and Opportunities. CPT Pharmacomet. Syst. Pharmacol. 2018, 7, 785–787. [Google Scholar] [CrossRef]
- Kluwe, F.; Michelet, R.; Mueller-Schoell, A.; Maier, C.; Klopp-Schulze, L.; Van Dyk, M.; Mikus, G.; Huisinga, W.; Kloft, C. Perspectives on Model-Informed Precision Dosing in the Digital Health Era: Challenges, Opportunities, and Recommendations. Clin. Pharmacol. Ther. 2021, 109, 29–36. [Google Scholar] [CrossRef]
- Gin, A.; Dilay, L.; A Karlowsky, J.; Walkty, A.; Rubinstein, E.; Zhanel, G.G. Piperacillin-tazobactam: A β-lactam/β-lactamase inhibitor combination. Expert Rev. Anti Infect. Ther. 2007, 5, 365–383. [Google Scholar] [CrossRef] [PubMed]
- Chung, E.K.; Cheatham, S.C.; Fleming, M.R.; Healy, D.P.; Shea, K.M.; Kays, M.B. Population pharmacokinetics and pharmacodynamics of piperacillin and tazobactam administered by prolonged infusion in obese and nonobese patients. J. Clin. Pharmacol. 2015, 55, 899–908. [Google Scholar] [CrossRef]
- Drawz, S.M.; Bonomo, R.A. Three decades of beta-lactamase inhibitors. Clin. Microbiol. Rev. 2010, 23, 160–201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lodise, T.P.; Lomaestro, B.M.; Drusano, G.L. Application of antimicrobial pharmacodynamic concepts into clinical practice: Focus on β-lactam antibiotics. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2006, 26, 1320–1332. [Google Scholar] [CrossRef]
- Kim, M.-K.; Xuan, D.; Quintiliani, R.; Nightingale, C.H.; Nicolau, D.P. Pharmacokinetic and pharmacodynamic profile of high dose extended interval piperacillin–tazobactam. J. Antimicrob. Chemother. 2001, 48, 259–267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guilhaumou, R.; Benaboud, S.; Bennis, Y.; Dahyot-Fizelier, C.; Dailly, E.; Gandia, P.; Goutelle, S.; Lefeuvre, S.; Mongardon, N.; Roger, C.; et al. Optimization of the treatment with beta-lactam antibiotics in critically ill patients—Guidelines from the French Society of Pharmacology and Therapeutics (Société Française de Pharmacologie et Thérapeutique—SFPT) and the French Society of Anaesthesia and. Crit. Care 2019, 23, 104. [Google Scholar] [CrossRef] [Green Version]
- Pea, F.; Viale, P. Pharmacodynamics of antibiotics to treat multidrug-resistant Gram-positive hospital infections. Expert Rev. Anti Infect. Ther. 2007, 5, 255–270. [Google Scholar] [CrossRef]
- Cojutti, P.; Sartor, A.; Righi, E.; Scarparo, C.; Bassetti, M.; Pea, F. Population Pharmacokinetics of High-Dose Continuous-Infusion Meropenem and Considerations for Use in the Treatment of Infections Due to KPC-Producing Klebsiella pneumoniae. Antimicrob. Agents Chemother. 2017, 61, e00794-17. [Google Scholar] [CrossRef] [Green Version]
- Pea, F.; Viale, P.; Cojutti, P.G.; Furlanut, M. Dosing nomograms for attaining optimum concentrations of meropenem by continuous infusion in critically ill patients with severe gram-negative infections: A pharmacokinetics/pharmacodynamics-based approach. Antimicrob. Agents Chemother. 2012, 56, 6343–6348. [Google Scholar] [CrossRef] [Green Version]
- Mouton, J.W.; den Hollander, J.G. Killing of Pseudomonas aeruginosa during continuous and intermittent infusion of ceftazidime in an in vitro pharmacokinetic model. Antimicrob. Agents Chemother. 1994, 38, 931–936. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, G.; Brinkman, A.; Benefield, R.J.; Carlier, M.; De Waele, J.J.; El Helali, N.; Frey, O.; Harbarth, S.; Huttner, A.; McWhinney, B.; et al. An international, multicentre survey of β-lactam antibiotic therapeutic drug monitoring practice in intensive care units. J. Antimicrob. Chemother. 2014, 69, 1416–1423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- EMA. Guideline on the Use of Pharmacokinetics and Pharmacodynamics in the Development of Antibacterial Medicinal Products; EMA: Amsterdam, The Netherlands, 2017.
- Ehmann, L.; Simon, P.; Busse, D.; Petroff, D.; Dorn, C.; Huisinga, W.; Dietrich, A.; Zeitlinger, M.; Wrigge, H.; Kloft, C. Risk of target non-attainment in obese compared to non-obese patients in calculated linezolid therapy. Clin. Microbiol. Infect. 2020, 26, 1222–1228. [Google Scholar] [CrossRef] [PubMed]
- Dorn, C.; Petroff, D.; Neumann, N.; Kratzer, A.; El-Najjar, N.; Dietrich, A.; Kloft, C.; Zeitlinger, M.; Kees, M.G.; Kees, F.; et al. Plasma and tissue pharmacokinetics of fosfomycin in morbidly obese and non-obese surgical patients: A controlled clinical trial. J. Antimicrob. Chemother. 2019, 74, 2335–2340. [Google Scholar] [CrossRef]
- Simon, P.; Petroff, D.; Busse, D.; Heyne, J.; Girrbach, F.; Dietrich, A.; Kratzer, A.; Zeitlinger, M.; Kloft, C.; Kees, F.; et al. Meropenem plasma and interstitial soft tissue concentrations in obese and nonobese patients-a controlled clinical trial. Antibiot 2020, 9, 931. [Google Scholar] [CrossRef] [PubMed]
- Alobaid, A.S.; Wallis, S.C.; Jarrett, P.; Starr, T.; Stuart, J.; Lassig-Smith, M.; Mejia, J.L.O.; Roberts, M.S.; Roger, C.; Udy, A.A.; et al. Population Pharmacokinetics of Piperacillin in Nonobese, Obese, and Morbidly Obese Critically Ill Patients. Antimicrob. Agents Chemother. 2017, 61, e01276-16. [Google Scholar] [CrossRef] [Green Version]
- Cheatham, S.C.; Fleming, M.R.; Healy, D.P.; Chung, C.E.; Shea, K.M.; Humphrey, M.L.; Kays, M.B. Steady-state pharmacokinetics and pharmacodynamics of piperacillin and tazobactam administered by prolonged infusion in obese patients. Int. J. Antimicrob. Agents 2013, 41, 52–56. [Google Scholar] [CrossRef]
- Jung, B.; Mahul, M.; Breilh, D.; Legeron, R.; Signe, J.; Jean-Pierre, H.; Uhlemann, A.-C.; Molinari, N.; Jaber, S. Repeated Piperacillin-Tazobactam Plasma Concentration Measurements in Severely Obese Versus Nonobese Critically Ill Septic Patients and the Risk of Under—and Overdosing*. Crit. Care Med. 2017, 45, e470–e478. [Google Scholar] [CrossRef]
- Simon, P.; Petroff, D.; Dorn, C.; Ehmann, L.; Kloft, C.; Prettin, C.; Dietrich, A.; Zeitlinger, M.; Kees, F.; Wrigge, H. Measurement of soft tissue drug concentrations in morbidly obese and non-obese patients—A prospective, parallel group, open-labeled, controlled, phase IV, single center clinical trial. Contemp. Clin. Trials Commun. 2019, 15, 100375. [Google Scholar] [CrossRef] [PubMed]
- Burau, D.; Petroff, D.; Simon, P.; Ehmann, L.; Weiser, C.; Dorn, C.; Kratzer, A.; Wrigge, H.; Kloft, C. Drug combinations and impact of experimental conditions on relative recovery in in vitro microdialysis investigations. Eur. J. Pharm. Sci. 2019, 127, 252–260. [Google Scholar] [CrossRef]
- Busse, D.; Simon, P.; Michelet, R.; Ehmann, L.; Mehner, F.; Dorn, C.; Kratzer, A.; Huisinga, W.; Wrigge, H.; Petroff, D.; et al. Quantification of microdialysis related variability in humans: Clinical trial design recommendations. Eur. J. Pharm. Sci. 2021, 157, 105607. [Google Scholar] [CrossRef]
- Plock, N.; Kloft, C. Microdialysis-Theoretical background and recent implementation in applied life-sciences. Eur. J. Pharm. Sci. 2005, 25, 1–24. [Google Scholar] [CrossRef]
- Dorn, C.; Petroff, D.; Walther, S.; Kees, M.G.; Kratzer, A.; Kees, F.; Kloft, C.; Zeitlinger, M.; Wrigge, H.; Simon, P.; et al. Pharmacokinetics and subcutaneous tissue distribution of piperacillin in obese and non-obese surgical patients following a single dose of piperacillin/tazobactam. Int. J. Antimicrob. Agents 2021. in submission. [Google Scholar]
- US Food and Drug Administration. DRAFT Guidance for Industry Population Pharmacokinetics; Silver Spring, MD, USA, 2019. Available online: https://www.fda.gov/media/128793/download (accessed on 10 July 2021).
- Tunblad, K.; Hammarlund-Udenaes, M.; Jonsson, E.N. An integrated model for the analysis of pharmacokinetic data from microdialysis experiments. Pharm. Res. 2004, 21, 1698–1707. [Google Scholar] [CrossRef] [PubMed]
- Busse, D.; Schaeftlein, A.; Solms, A.; Ilia, L.; Michelet, R.; Zeitlinger, M.; Huisinga, W.; Kloft, C. Which Analysis Approach Is Adequate to Leverage Clinical Microdialysis Data? A Quantitative Comparison to Investigate Exposure and Reponse Exemplified by Levofloxacin. Pharm. Res. 2021, 38, 381–395. [Google Scholar] [CrossRef] [PubMed]
- Post, T.M.; Freijer, J.I.; Ploeger, B.A.; Danhof, M. Extensions to the Visual Predictive Check to facilitate model performance evaluation. J. Pharmacokinet. Pharmacodyn. 2008, 35, 185–202. [Google Scholar] [CrossRef] [Green Version]
- Janmahasatian, S.; Duffull, S.B.; Ash, S.; Ward, L.; Byrne, N.; Green, B. Quantification of lean bodyweight. Clin. Pharmacokinet. 2005, 44, 1051–1065. [Google Scholar] [CrossRef]
- Mosteller, R.D. Simplified Calculation of Body-Surface Area. N. Engl. J. Med. 1987, 317, 1098. [Google Scholar] [CrossRef]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F.; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]
- Grams, M.E.; Chow, E.; Segev, D.L.; Coresh, J. Lifetime Incidence of CKD Stages 3–5 in the United States. Am. J. Kidney Dis. 2013, 62, 245–252. [Google Scholar] [CrossRef] [Green Version]
- Holford, N.H.G.; Anderson, B.J. Allometric size: The scientific theory and extension to normal fat mass. Eur. J. Pharm. Sci. 2017, 109, S59–S64. [Google Scholar] [CrossRef]
- World Health Organization. Body Mass Index-BMI 2021. Available online: http://www.euro.who.int/en/health-topics/disease-prevention/nutrition/a-healthy-lifestyle/body-mass-index-bmi (accessed on 10 February 2021).
- Verbraecken, J.; Van de Heyning, P.; De Backer, W.; Van Gaal, L. Body surface area in normal-weight, overweight, and obese adults. A comparison study. Metabolism 2006, 55, 515–524. [Google Scholar] [CrossRef]
- Pai, M.P. Estimating the Glomerular Filtration Rate in Obese Adult Patients for Drug Dosing. Adv. Chronic Kidney Dis. 2010, 17, e53–e62. [Google Scholar] [CrossRef]
- Cachat, F.; Combescure, C.; Cauderay, M.J.; Girardin, E.; Chehade, H. A Systematic Review of Glomerular Hyperfiltration Assessment and Definition in the Medical Literature. Clin. J. Am. Soc. Nephrol. 2015, 10, 382–389. [Google Scholar] [CrossRef] [PubMed]
- European Committee on Antimicrobial Susceptibility Testing. Breakpoint Tables for Interpretation of MICs and Zone Diameters, Version 11.0, 2021. 2021. Available online: http://www.eucast.org/fileadmin/src/media/PDFs/EUCAST_files/Breakpoint_tables/v_8.0_Breakpoint_Tables.pdf (accessed on 9 June 2021).
- Mouton, J.W.; Dudley, M.N.; Cars, O.; Derendorf, H.; Drusano, G.L. Standardization of pharmacokinetic/pharmacodynamic (PK/PD) terminology for anti-infective drugs: An update. J. Antimicrob. Chemother. 2005, 55, 601–607. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, A.; Kuti, J.L.; Nicolau, D.P. Probability of pharmacodynamic target attainment with standard and prolonged-infusion antibiotic regimens for empiric therapy in adults with hospital-acquired pneumonia. Clin. Ther. 2009, 31, 2765–2778. [Google Scholar] [CrossRef]
- Koomanachai, P.; Bulik, C.C.; Kuti, J.L.; Nicolau, D.P. Pharmacodynamic modeling of intravenous antibiotics against gram-negative bacteria collected in the United States. Clin. Ther. 2010, 32, 766–779. [Google Scholar] [CrossRef]
- Anderson, B.J.; Holford, N.H.G. Mechanism-based concepts of size and maturity in pharmacokinetics. Annu. Rev. Pharmacol. Toxicol. 2008, 48, 303–332. [Google Scholar] [CrossRef] [PubMed]
- Huisinga, W.; Solms, A.; Fronton, L.; Pilari, S. Modeling Interindividual Variability in Physiologically Based Pharmacokinetics and Its Link to Mechanistic Covariate Modeling. CPT Pharmacomet. Syst. Pharmacol. 2012, 1, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Meng, L.; Mui, E.; Holubar, M.K.; Deresinski, S.C. Comprehensive guidance for antibiotic dosing in obese adults. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2017, 37, 1415–1431. [Google Scholar] [CrossRef] [PubMed]
- Winter, M.A.; Guhr, K.N.; Berg, G.M. Impact of various body weights and serum creatinine concentrations on the bias and accuracy of the Cockcroft-Gault equation. Pharmacotherapy 2012, 32, 604–612. [Google Scholar] [CrossRef] [PubMed]
- Stefansson, V.T.N.; Schei, J.; Jenssen, T.G.; Melsom, T.; Eriksen, B.O. Central obesity associates with renal hyperfiltration in the non-diabetic general population: A cross-sectional study. BMC Nephrol. 2016, 17, 172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tokunaga, A.; Miyamoto, H.; Fumoto, S.; Nishida, K. Effect of renal ischaemia/reperfusion-induced acute kidney injury on pharmacokinetics of midazolam in rats. J. Pharm. Pharmacol. 2019, 71, 1792–1799. [Google Scholar] [CrossRef]
- Pilari, S.; Huisinga, W. Lumping of physiologically-based pharmacokinetic models and a mechanistic derivation of classical compartmental models. J. Pharmacokinet. Pharmacodyn. 2010, 37, 365–405. [Google Scholar] [CrossRef] [PubMed]
- Sturm, A.W.; Allen, N.; Rafferty, K.D.; Fish, D.N.; Toschlog, E.; Newell, M.; Waibel, B. Pharmacokinetic analysis of piperacillin administered with tazobactam in critically ill, morbidly obese surgical patients. Pharmacotherapy 2014, 34, 28–35. [Google Scholar] [CrossRef] [PubMed]
- Hites, M.; Taccone, F.S.; Wolff, F.; Cotton, F.; Beumier, M.; De Backer, D.; Roisin, S.; Lorent, S.; Surin, R.; Seyler, L.; et al. Case-control study of drug monitoring of β-lactams in obese critically ill patients. Antimicrob. Agents Chemother. 2013, 57, 708–715. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cojutti, P.; Pai, M.P.; Pea, F. Population pharmacokinetics and dosing considerations for the use of linezolid in overweight and obese adult patients. Clin. Pharmacokinet. 2018, 57, 989–1000. [Google Scholar] [CrossRef]
- Pai, M.P.; Cojutti, P.G.; Pea, F. Levofloxacin Dosing Regimen in Severely Morbidly Obese Patients (BMI ≥ 40 kg/m2) Should be Guided by Creatinine Clearance Estimates Based on Ideal Body Weight and Optimized by Therapeutic Drug Monitoring. Clin. Pharmacokinet. 2014, 53, 753–762. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Reference Patients | BMI [kg/m2] | Total Body Weight [kg] | Lean Body Weight [kg] a | Fat Mass [kg] b | %Fat Mass c | BSA [m2] d | CLCRCG_ABW [mL/min] |
|---|---|---|---|---|---|---|---|
| (1) Nonobese, healthy renal function | 22.6 | 70.0 I | 52.6 | 17.4 | 24.8 | 1.85 | 90 III |
| (2) Morbidly obese, healthy renal function | 40.0 II | 127 | 76.8 | 50.2 | 39.5 | 2.49 | 130 IV |
| (3) Nonobese, renally impaired | 22.6 | 70.0 | 52.6 | 17.4 | 24.8 | 1.85 | 45.0 V |
| (4) Nonobese, hyperfiltration | 22.6 | 70.0 | 52.6 | 17.4 | 24.8 | 1.85 | 130 VI |
| Dosing Regimen | Dose Piperacillin [g]/ Tazobactam [g] | Dosing Interval [h] | Infusion Length [h] | Loading Dose 1 Piperacillin [g]/ Tazobactam [g] | Daily Dose Piperacillin [g]/ Tazobactam [g] |
|---|---|---|---|---|---|
| “Standard dosage 1” 2 | 4/0.5 | 6 | 0.5 | - | 16/2 |
| “Standard dosage 2” 2 | 4/0.5 | 8 | 4 | - | 12/1.5 |
| “High dosage” 2 | 4/0.5 | 6 | 3 | - | 16/2 |
| “Continuous infusion” | 24/3 | 24 | 24 | 4/0.5 | 28/3.5 3 |
| Characteristic | Full Population (n = 30) * | Obese Subpopulation (n = 15) * | Nonobese Subpopulation (n = 15) * |
|---|---|---|---|
| Sex, male | 12 (40.0%) | 6 (40.0%) | 6 (40.0%) |
| Total body weight [kg] | 96.0 (77.0–123) | 122 (109–147) | 75.0 (67.0–84.0) |
| Lean body weight [kg] a | 55.5 (46.9–71.8) | 64.7 (54.5–83.3) | 45.8 (42.4–61.1) |
| Fat mass [kg] b | 39.3 (25.2–63.3) | 64.2 (53.0–72.3) | 25.2 (22.8–27.8) |
| Percent fat mass, % c | 39.9 (34.4–48.6) | 48.6 (46.2–53.7) | 34.0 (27.4–38.5) |
| BMI [kg/m2] | 33.4 (26.5–44.8) | 45.7 (40.1–48.3) | 26.4 (24.7–28.1) |
| Serum creatinine conc. [µmol/L] | 70.6 (59.2–86.0) | 79.1 (61.0–88.0) | 70.0 (57.6–86.0) |
| CLCRCG_ABW [mL/min] | 110 (82.1–130) | 131 (113–144) | 89.8 (75.1–106) |
| Serum albumin conc. [g/L] | 45.6 (43.1–46.9) | 45.6 (44.0–46.9) | 45.9 (42.1–47.7) |
| Total bilirubin conc. [µM] | 6.20 (3.70–9.00) | 7.70 (4.30–11.6) | 5.90 (3.50–6.30) |
| Arterial hypertension | 17 (56.7%) | 14 (93.3%) | 3 (20.0%) |
| Diabetes mellitus type 2 | 6 (20.0%) | 4 (26.7%) | 2 (13.3%) |
| Steatohepatitis | 8 (26.7%) | 8 (53.3%) | 0 (0.00%) |
| Vasopressors d | 18 (60.0%) | 8 (53.3%) | 10 (66.7%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Busse, D.; Simon, P.; Petroff, D.; Dorn, C.; Schmitt, L.; Bindellini, D.; Kratzer, A.; Dietrich, A.; Zeitlinger, M.; Huisinga, W.; et al. Similar Piperacillin/Tazobactam Target Attainment in Obese versus Nonobese Patients despite Differences in Interstitial Tissue Fluid Pharmacokinetics. Pharmaceutics 2021, 13, 1380. https://doi.org/10.3390/pharmaceutics13091380
Busse D, Simon P, Petroff D, Dorn C, Schmitt L, Bindellini D, Kratzer A, Dietrich A, Zeitlinger M, Huisinga W, et al. Similar Piperacillin/Tazobactam Target Attainment in Obese versus Nonobese Patients despite Differences in Interstitial Tissue Fluid Pharmacokinetics. Pharmaceutics. 2021; 13(9):1380. https://doi.org/10.3390/pharmaceutics13091380
Chicago/Turabian StyleBusse, David, Philipp Simon, David Petroff, Christoph Dorn, Lisa Schmitt, Davide Bindellini, Alexander Kratzer, Arne Dietrich, Markus Zeitlinger, Wilhelm Huisinga, and et al. 2021. "Similar Piperacillin/Tazobactam Target Attainment in Obese versus Nonobese Patients despite Differences in Interstitial Tissue Fluid Pharmacokinetics" Pharmaceutics 13, no. 9: 1380. https://doi.org/10.3390/pharmaceutics13091380