
Real-World Comparative Evaluation of Add-On Glucagon-like Peptide 1 Receptor Agonist in Type 2 Diabetes Treated with or without Insulin
 and
and
Abstract
:1. Introduction
2. Results
3. Discussion
4. Material and Methods
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Khan, M.A.B.; Hashim, M.J.; King, J.K.; Govender, R.D.; Mustafa, H.; Al Kaabi, J. Epidemiology of Type 2 Diabetes—Global Burden of Disease and Forecasted Trends. J. Epidemiol. Glob. Health 2020, 10, 107–111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, H.; Saeedi, P.; Karuranga, S.; Pinkepank, M.; Ogurtsova, K.; Duncan, B.B.; Stein, C.; Basit, A.; Chan, J.C.; Mbanya, J.C.; et al. IDF Diabetes Atlas: Global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res. Clin. Pract. 2022, 183, 109119. [Google Scholar] [CrossRef] [PubMed]
- Shah, N.; Abdalla, M.A.; Deshmukh, H.; Sathyapalan, T. Therapeutics for type-2 diabetes mellitus: A glance at the recent inclusions and novel agents under development for use in clinical practice. Ther. Adv. Endocrinol. Metab. 2021, 12, 20420188211042145. [Google Scholar] [CrossRef] [PubMed]
- Martínez, M.S.; Manzano, A.; Olivar, L.C.; Nava, M.; Salazar, J.; D’Marco, L.; Ortiz, R.; Chacín, M.; Guerrero-Wyss, M.; de Bravo, M.C.; et al. The Role of the α Cell in the Pathogenesis of Diabetes: A World beyond the Mirror. Int. J. Mol. Sci. 2021, 22, 9504. [Google Scholar] [CrossRef]
- Lu, J.M. The Role of Glucagon-Like Peptide-1 Receptor Agonists in Type 2 Diabetes in Asia. Adv. Ther. 2019, 36, 798–805. [Google Scholar] [CrossRef]
- Kristensen, S.L.; Rørth, R.; Jhund, P.S.; Docherty, K.F.; Sattar, N.; Preiss, D.; Køber, L.; Petrie, M.C.; McMurray, J.J.V. Cardiovascular, mortality, and kidney outcomes with GLP-1 receptor agonists in patients with type 2 diabetes: A systematic review and meta-analysis of cardiovascular outcome trials. Lancet Diabetes Endocrinol. 2019, 7, 776–785. [Google Scholar] [CrossRef]
- Marso, S.P.; Daniels, G.H.; Brown-Frandsen, K.; Kristensen, P.; Mann, J.F.E.; Nauck, M.A.; Nissen, S.E.; Pocock, S.; Poulter, N.R.; Ravn, L.S.; et al. LEADER Steering Committee; LEADER Trial Investigators. Liraglutide and Cardiovascular Outcomes in Type 2 Diabetes. N. Engl. J. Med. 2016, 375, 311–322. [Google Scholar] [CrossRef] [Green Version]
- Marso, S.P.; Bain, S.C.; Consoli, A.; Eliaschewitz, F.G.; Jódar, E.; Leiter, L.A.; Lingvay, I.; Rosenstock, J.; Seufert, J.; Warren, M.L.; et al. SUSTAIN-6 Investigators. Semaglutide and Cardiovascular Outcomes in Patients with Type 2 Diabetes. N. Engl. J. Med. 2016, 375, 1834–1844. [Google Scholar] [CrossRef] [Green Version]
- Gerstein, H.C.; Colhoun, H.M.; Dagenais, G.R.; Diaz, R.; Lakshmanan, M.; Pais, P.; Probstfield, J.; Riesmeyer, J.S.; Riddle, M.C.; Rydén, L.; et al. REWIND Investigators. Dulaglutide and cardiovascular outcomes in type 2 diabetes (REWIND): A double-blind, randomised placebo-controlled trial. Lancet 2019, 394, 121–130. [Google Scholar] [CrossRef]
- American Diabetes Association Professional Practice Committee; Draznin, B.; Aroda, V.R.; Bakris, G.; Benson, G.; Brown, F.M.; Freeman, R.; Green, J.; Huang, E.; Isaacs, D.; et al. 9. Pharmacologic Approaches to Glycemic Treatment: Standards of Medical Care in Diabetes-2022. Diabetes Care 2022, 45, S125–S143. [Google Scholar] [CrossRef]
- Filippatos, T.D.; Panagiotopoulou, T.V.; Elisaf, M.S. Adverse Effects of GLP-1 Receptor Agonists. Rev. Diabet. Stud. 2014, 11, 202–230. [Google Scholar] [CrossRef] [Green Version]
- He, L.; Wang, J.; Ping, F.; Yang, N.; Huang, J.; Li, Y. Association of Glucagon-Like Peptide-1 Receptor Agonist Use With Risk of Gallbladder and Biliary Diseases: A Systematic Review and Meta-analysis of Randomized Clinical Trials. JAMA Intern. Med. 2022, 182, 513–519. [Google Scholar] [CrossRef]
- Lipowsky, C.; Sze, L.; Krull, I.; Brändle, M. Liraglutide as add-on therapy to insulin in type 2 diabetes mellitus: A retrospective, observational study from a daily clinical practice setting in Switzerland. Diabetes Ther. 2015, 6, 41–47. [Google Scholar] [CrossRef] [Green Version]
- Blonde, L.; Russell-Jones, D. The safety and efficacy of liraglutide with or without oral antidiabetic drug therapy in type 2 diabetes: An overview of the LEAD 1–5 studies. Diabetes Obes. Metab. 2009, 11, 26–34. [Google Scholar] [CrossRef]
- Lee, J.; Cho, Y.K.; Kim, H.S.; Jung, C.H.; Park, J.-Y.; Lee, W.J. Dulaglutide as an Add-on to Insulin in Type 2 Diabetes; Clinical Efficacy and Parameters Affecting the Response in Real-World Practice. Diabetes Metab. Syndr. Obes. Targets Ther. 2019, 12, 2745–2753. [Google Scholar] [CrossRef] [Green Version]
- Rhinehart, A.S. Adding GLP-1 Receptor Agonist Therapy to Basal Insulin for Postprandial Glucose Control. Clin. Diabetes 2015, 33, 73–75. [Google Scholar] [CrossRef] [Green Version]
- Gyorffy, J.B.; Keithler, A.N.; Wardian, J.L.; Zarzabal, L.A.; Rittel, A.; True, M.W. The Impact of GLP-1 Receptor Agonists on Patients with Diabetes on Insulin Therapy. Endocr. Pract. 2019, 25, 935–942. [Google Scholar] [CrossRef]
- Buse, J.B.; Wexler, D.J.; Tsapas, A.; Rossing, P.; Mingrone, G.; Mathieu, C.; D’Alessio, D.A.; Davies, M.J. 2019 update to: Management of hyperglycaemia in type 2 diabetes, 2018. A consensus report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetologia 2020, 63, 221–228. [Google Scholar] [CrossRef] [Green Version]
- Aroda, V.R.; González-Galvez, G.; Grøn, R.; Halladin, N.; Haluzík, M.; Jermendy, G.; Kok, A.; Őrsy, P.; Sabbah, M.; Sesti, G.; et al. Durability of insulin degludec plus liraglutide versus insulin glargine U100 as initial injectable therapy in type 2 diabetes (DUAL VIII): A multicentre, open-label, phase 3b, randomised controlled trial. Lancet Diabetes Endocrinol. 2019, 7, 596–605. [Google Scholar] [CrossRef]
- U.K. Prospective Diabetes Study Group. U.K. prospective diabetes study 16. Overview of 6 years’ therapy of type II diabetes: A progressive disease. Diabetes 1995, 44, 1249–1258. [Google Scholar] [CrossRef]
- Poitout, V.; Robertson, R.P. Minireview: Secondary beta-cell failure in type 2 diabetes--a convergence of glucotoxicity and lipotoxicity. Endocrinology 2002, 143, 339–342. [Google Scholar] [CrossRef] [PubMed]
- Hanefeld, M. Use of insulin in type 2 diabetes: What we learned from recent clinical trials on the benefits of early insulin initiation. Diabetes Metab. 2014, 40, 391–399. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wysham, C.; Shubrook, J. Beta-cell failure in type 2 diabetes: Mechanisms, markers, and clinical implications. Postgrad. Med. 2020, 132, 676–686. [Google Scholar] [CrossRef] [PubMed]
- Matthews, D.R.; Cull, C.A.; Stratton, I.M.; Holman, R.R.; Turner, R.C. UKPDS 26: Sulphonylurea failure in non-insulin-dependent diabetic patients over six years. UK Prospective Diabetes Study (UKPDS) Group. Diabet. Med. 1998, 15, 297–303. [Google Scholar] [CrossRef]
- Kaneto, H.; Kimura, T.; Shimoda, M.; Obata, A.; Sanada, J.; Fushimi, Y.; Nakanishi, S.; Mune, T.; Kaku, K. Favorable Effects of GLP-1 Receptor Agonist against Pancreatic β-Cell Glucose Toxicity and the Development of Arteriosclerosis: “The Earlier, the Better” in Therapy with Incretin-Based Medicine. Int. J. Mol. Sci. 2021, 22, 7917. [Google Scholar] [CrossRef]
- Jones, A.G.; McDonald, T.J.; Shields, B.M.; Hill, A.V.; Hyde, C.J.; Knight, B.A.; Hattersley, A.T. PRIBA Study Group. Markers of β-Cell Failure Predict Poor Glycemic Response to GLP-1 Receptor Agonist Therapy in Type 2 Diabetes. Diabetes Care. 2016, 39, 250–257. [Google Scholar] [CrossRef] [Green Version]
- Esposito, K.; Mosca, C.; Brancario, C.; Chiodini, P.; Ceriello, A.; Giugliano, D. GLP-1 receptor agonists and HBA1c target of <7% in type 2 diabetes: Meta-analysis of randomized controlled trials. Curr. Med. Res. Opin. 2011, 27, 1519–1528. [Google Scholar]
- Babenko, A.Y.; Savitskaya, D.A.; Kononova, Y.A.; Trofimova, A.Y.; Simanenkova, A.V.; Vasilyeva, E.Y.; Shlyakhto, E.V. Predictors of Effectiveness of Glucagon-Like Peptide-1 Receptor Agonist Therapy in Patients with Type 2 Diabetes and Obesity. J. Diabetes Res. 2019, 2019, 1365162. [Google Scholar] [CrossRef]
- Imai, K.; Tsujimoto, T.; Goto, A.; Goto, M.; Kishimoto, M.; Yamamoto-Honda, R.; Noto, H.; Kajio, H.; Noda, M. Prediction of response to GLP-1 receptor agonist therapy in Japanese patients with type 2 diabetes. Diabetol. Metab. Syndr. 2014, 6, 110. [Google Scholar] [CrossRef] [Green Version]
- Kozawa, J.; Inoue, K.; Iwamoto, R.; Kurashiki, Y.; Okauchi, Y.; Kashine, S.; Kitamura, T.; Maeda, N.; Okita, K.; Iwahashi, H.; et al. Liraglutide is effective in type 2 diabetic patients with sustained endogenous insulin-secreting capacity. J. Diabetes Investig. 2012, 3, 294–297. [Google Scholar] [CrossRef] [Green Version]
- Nuttall, F.Q. Body Mass Index: Obesity, BMI, and Health: A Critical Review. Nutr. Today 2015, 50, 117–128. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association Professional Practice Committee; Draznin, B.; Aroda, V.R.; Bakris, G.; Benson, G.; Brown, F.M.; Freeman, R.; Green, J.; Huang, E.; Isaacs, D.; et al. Glycemic Targets: Standards of Medical Care in Diabetes-2022. Diabetes Care 2022, 45, S83–S96. [Google Scholar]



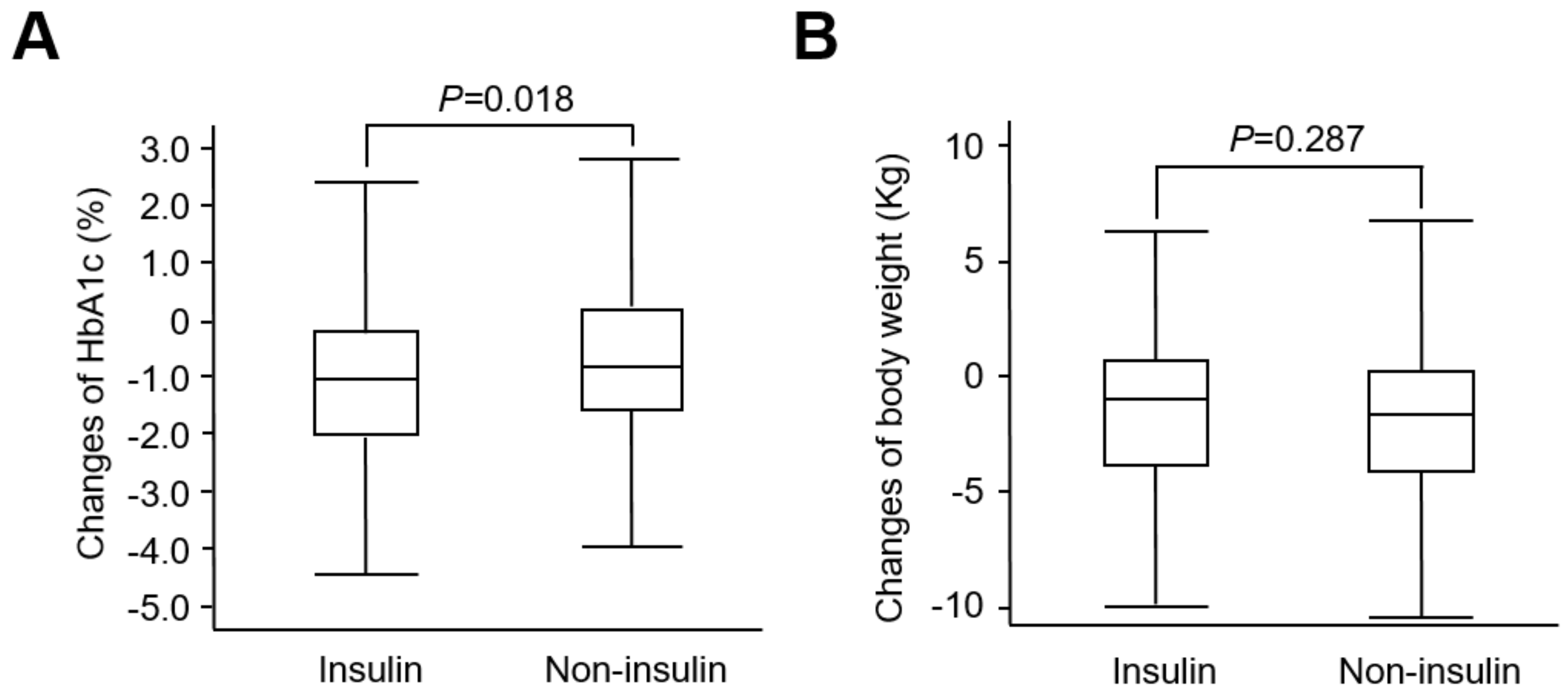{kind=link}
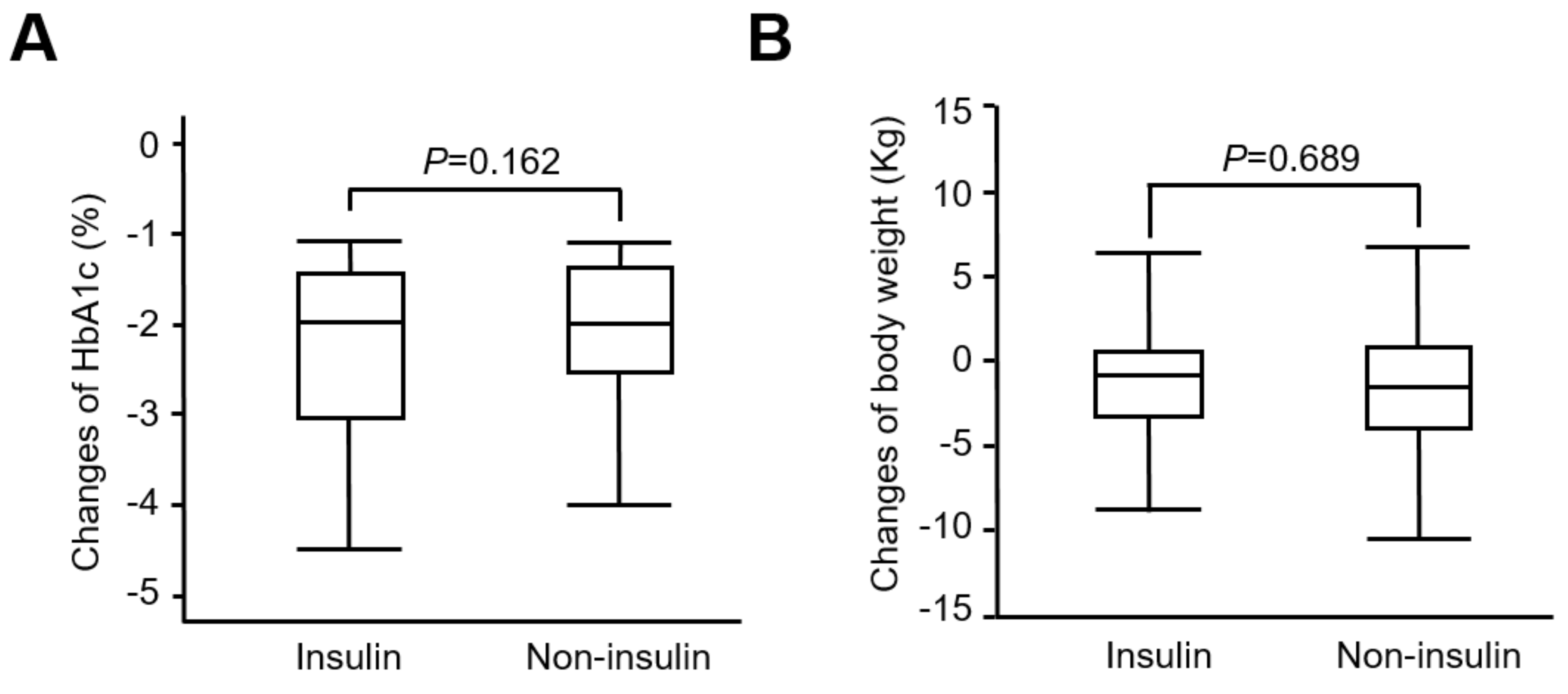{kind=link}
| Insulin User | Non-Insulin User | p-Value (Insulin User vs. Non-Insulin User) | |
|---|---|---|---|
| Number | 147 | 211 | |
| Age (years) | 56.7 ± 13.1 | 50.6 ± 12.9 | <0.001 |
| Male (%) | 51 | 51 | NS |
| DM duration (years) | 12.1 ± 7.1 | 8.7 ± 6.5 | <0.001 |
| BW (kg) | 77.2± 16.0 | 83.7 ± 16.1 | <0.001 |
| BMI (kg/m2) | 29.4 ± 5.2 | 31.3± 5.3 | 0.001 |
| SBP (mmHg) | 136 ± 18 | 135 ± 16 | NS |
| DBP (mmHg) | 81 ± 10 | 82 ± 10 | NS |
| Enrollment into “Diabetes Shared Care Program” (%) | 86 | 91 | NS |
| Comorbidities | |||
| Cerebrovascular disease (%) | 19 | 17 | NS |
| Coronary artery disease (%) | 19 | 17 | NS |
| Stroke (%) | 11 | 9 | NS |
| Peripheral artery disease (%) | 0 | 1 | NS |
| Congestive heart failure (%) | 3 | 7 | NS |
| Biochemical data | |||
| Fasting plasma glucose (mg/dL) | 186.01 ± 72.88 | 174.98 ± 55.87 | 0.12 |
| A1C (%) | 9.50 ± 1.70 | 8.84 ± 1.60 | <0.001 |
| Creatinine (mg/dL) | 1.15 ± 1.60 | 0.83 ± 0.43 | 0.007 |
| Estimated GFR (ml/min/1.73 m2) < 45 (%) | 16 | 6 | 0.002 |
| ALT (U/L) | 36 ± 28 | 43 ± 26 | 0.017 |
| Urinary albumin-to-creatinine ratio (mg/g) | 604 ± 1136 | 274 ± 747 | 0.001 |
| Total cholesterol (mg/dL) | 158.8 ± 38.2 | 167.0 ± 42.8 | NS |
| Triglyceride (mg/dL) | 191.8 ± 207.8 | 203.2 ± 164.1 | NS |
| HDL-C (mg/dL) | 44.6 ± 13.6 | 44.0 ± 11.6 | NS |
| LDL-C (mg/dL) | 95.6 ± 32.34 | 98.3 ± 32.4 | NS |
| Other anti-diabetes medications | |||
| Metformin (%) | 72 | 91 | <0.001 |
| Insulin secretagogues (%) | 42 | 72 | <0.001 |
| Pioglitazone (%) | 14 | 12 | NS |
| Acarbose (%) | 10 | 8 | NS |
| DPP-4 inhibitor (%) | 1 | 3 | NS |
| SGLT-2 inhibitor (%) | 5 | 8 | NS |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chou, H.-W.; Cheng, K.-P.; Lin, A.-C.; Hung, H.-C.; Lin, C.-H.; Wang, C.-C.; Wu, H.-T.; Ou, H.-Y. Real-World Comparative Evaluation of Add-On Glucagon-like Peptide 1 Receptor Agonist in Type 2 Diabetes Treated with or without Insulin. Pharmaceuticals 2022, 15, 1569. https://doi.org/10.3390/ph15121569
Chou H-W, Cheng K-P, Lin A-C, Hung H-C, Lin C-H, Wang C-C, Wu H-T, Ou H-Y. Real-World Comparative Evaluation of Add-On Glucagon-like Peptide 1 Receptor Agonist in Type 2 Diabetes Treated with or without Insulin. Pharmaceuticals. 2022; 15(12):1569. https://doi.org/10.3390/ph15121569
Chicago/Turabian StyleChou, Hsuan-Wen, Kai-Pi Cheng, An-Chi Lin, Hao-Chang Hung, Ching-Han Lin, Chih-Chen Wang, Hung-Tsung Wu, and Horng-Yih Ou. 2022. "Real-World Comparative Evaluation of Add-On Glucagon-like Peptide 1 Receptor Agonist in Type 2 Diabetes Treated with or without Insulin" Pharmaceuticals 15, no. 12: 1569. https://doi.org/10.3390/ph15121569