
Intra-Articular Leukocyte-Rich Platelet-Rich Plasma versus Intra-Articular Hyaluronic Acid in the Treatment of Knee Osteoarthritis: A Meta-Analysis of 14 Randomized Controlled Trials



Abstract
:1. Introduction
2. Results
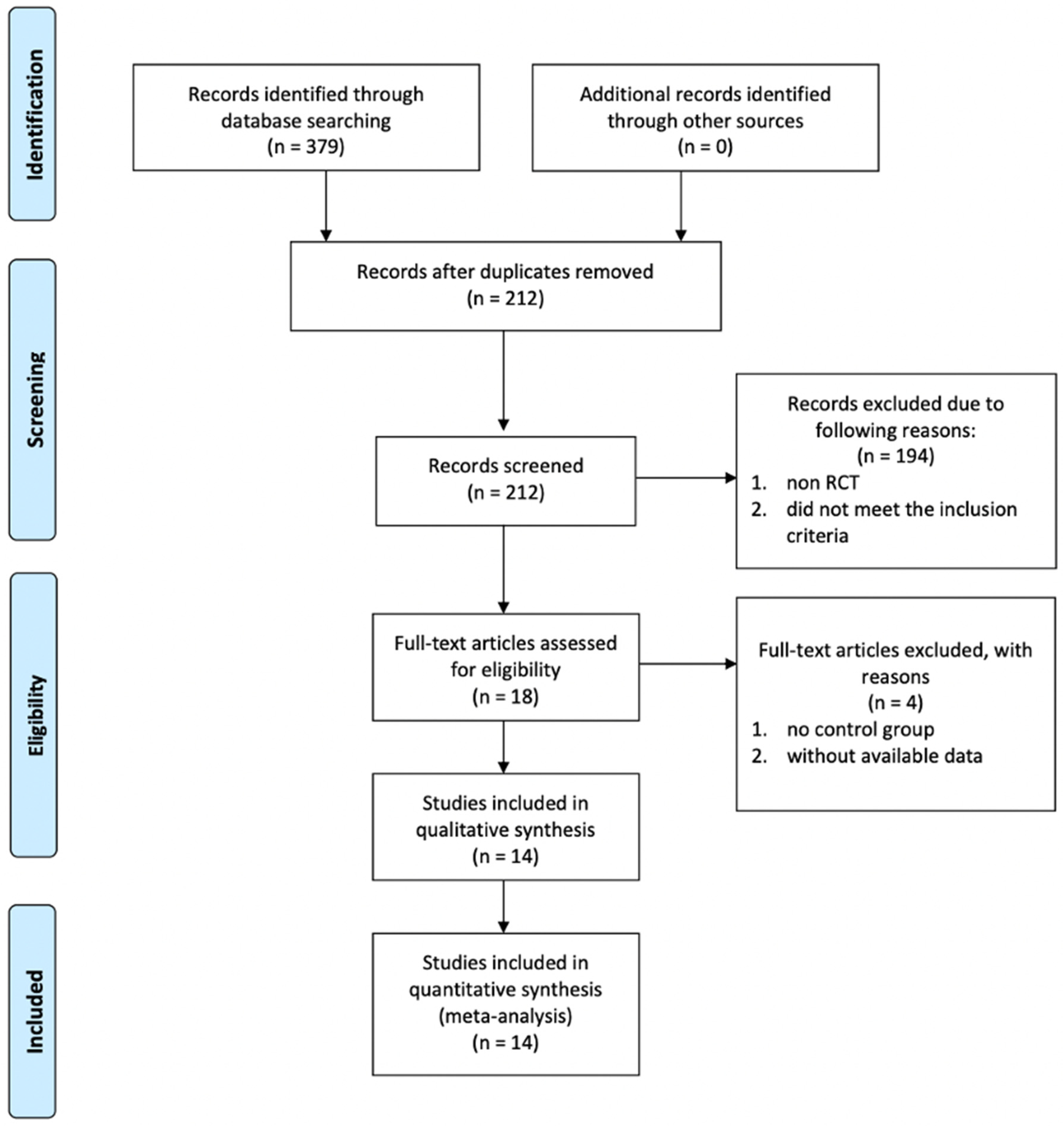
2.1. Literature Search
2.2. Main Characteristics of Included Studies
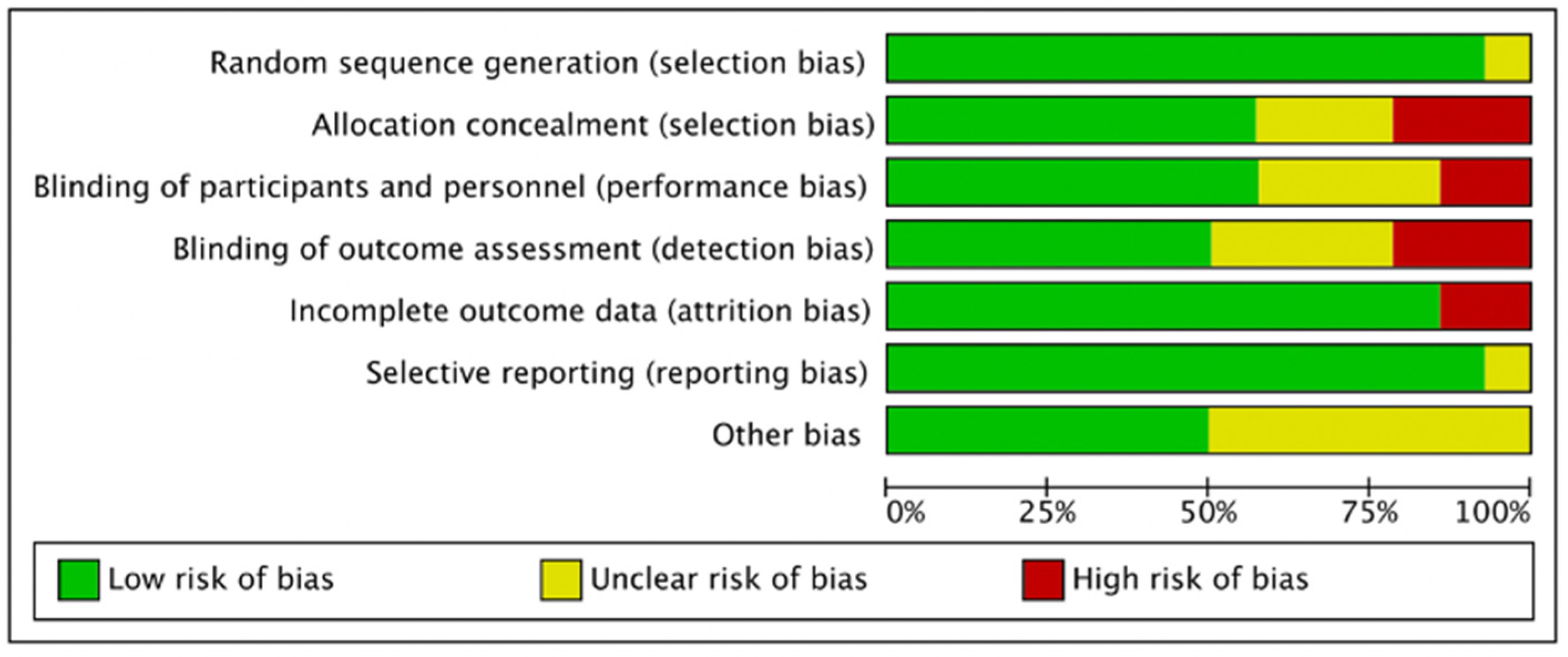
2.3. Quality of the Studies
2.4. Outcomes of the Meta-Analysis
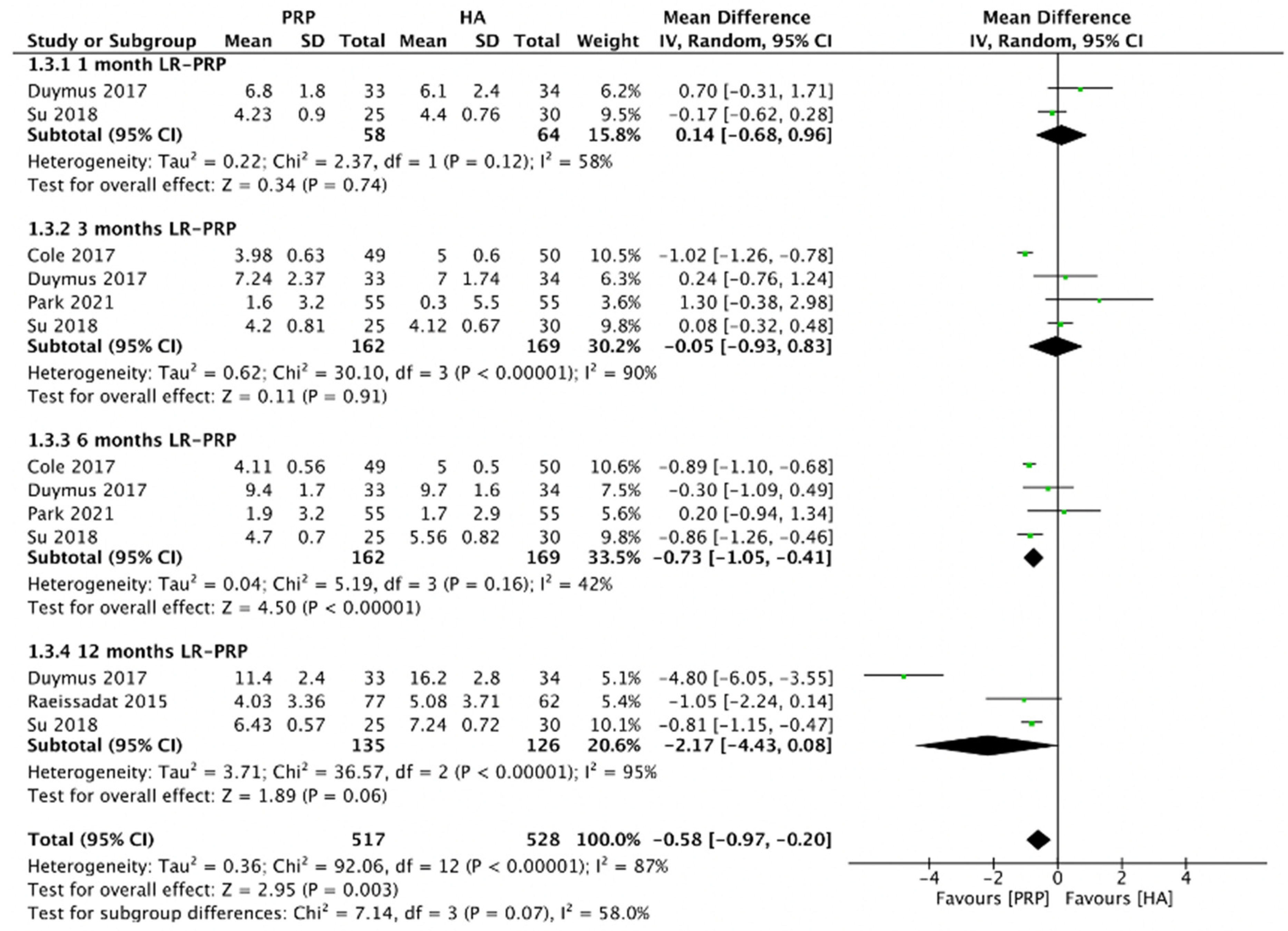
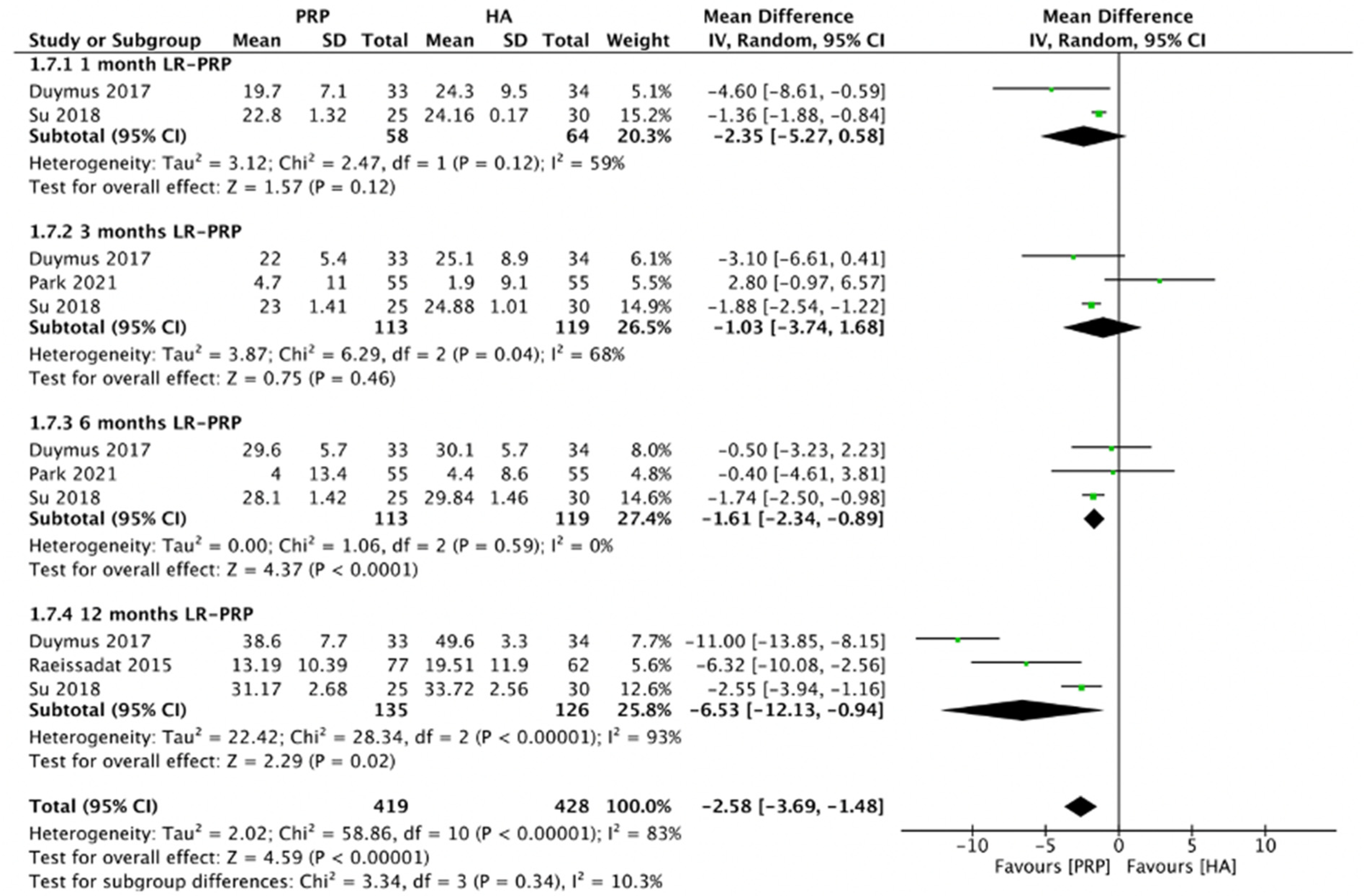
2.4.1. WOMAC Total Scores (LR-PRP)
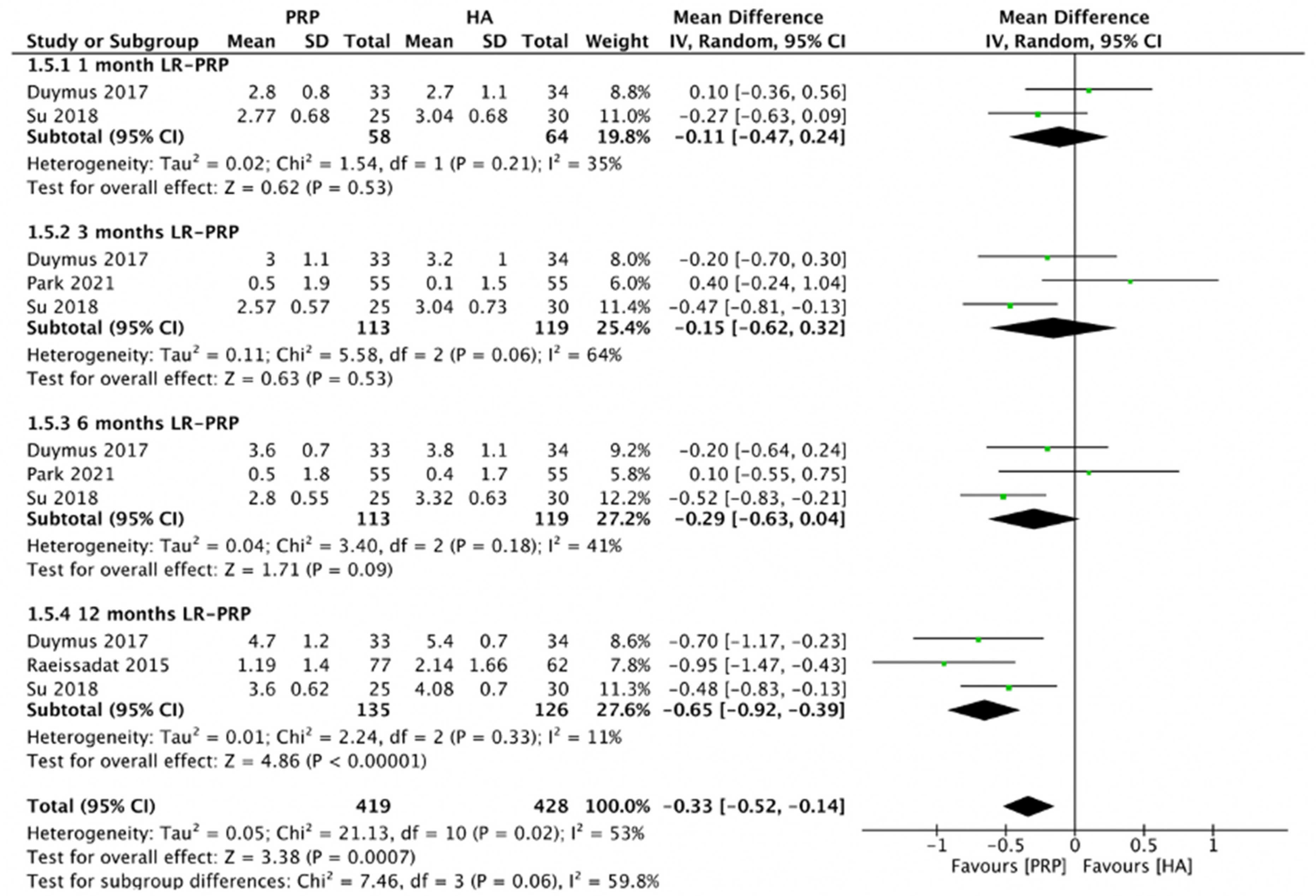
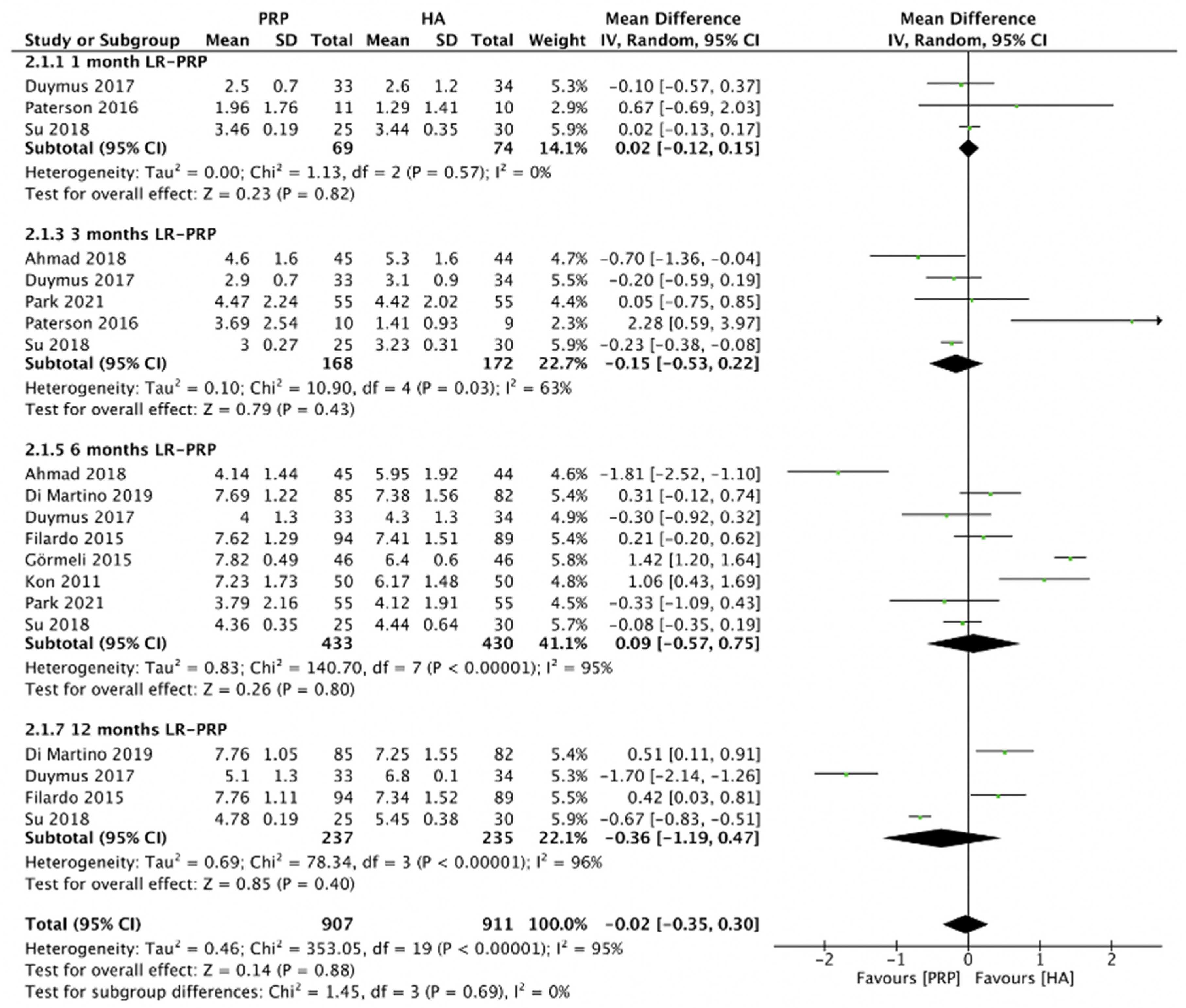
2.4.2. WOMAC Pain Scores (LR-PRP)
2.4.3. WOMAC Stiffness Scores (LR-PRP)
2.4.4. WOMAC Physical Function Scores (LR-PRP)
2.4.5. VAS Score (LR-PRP)
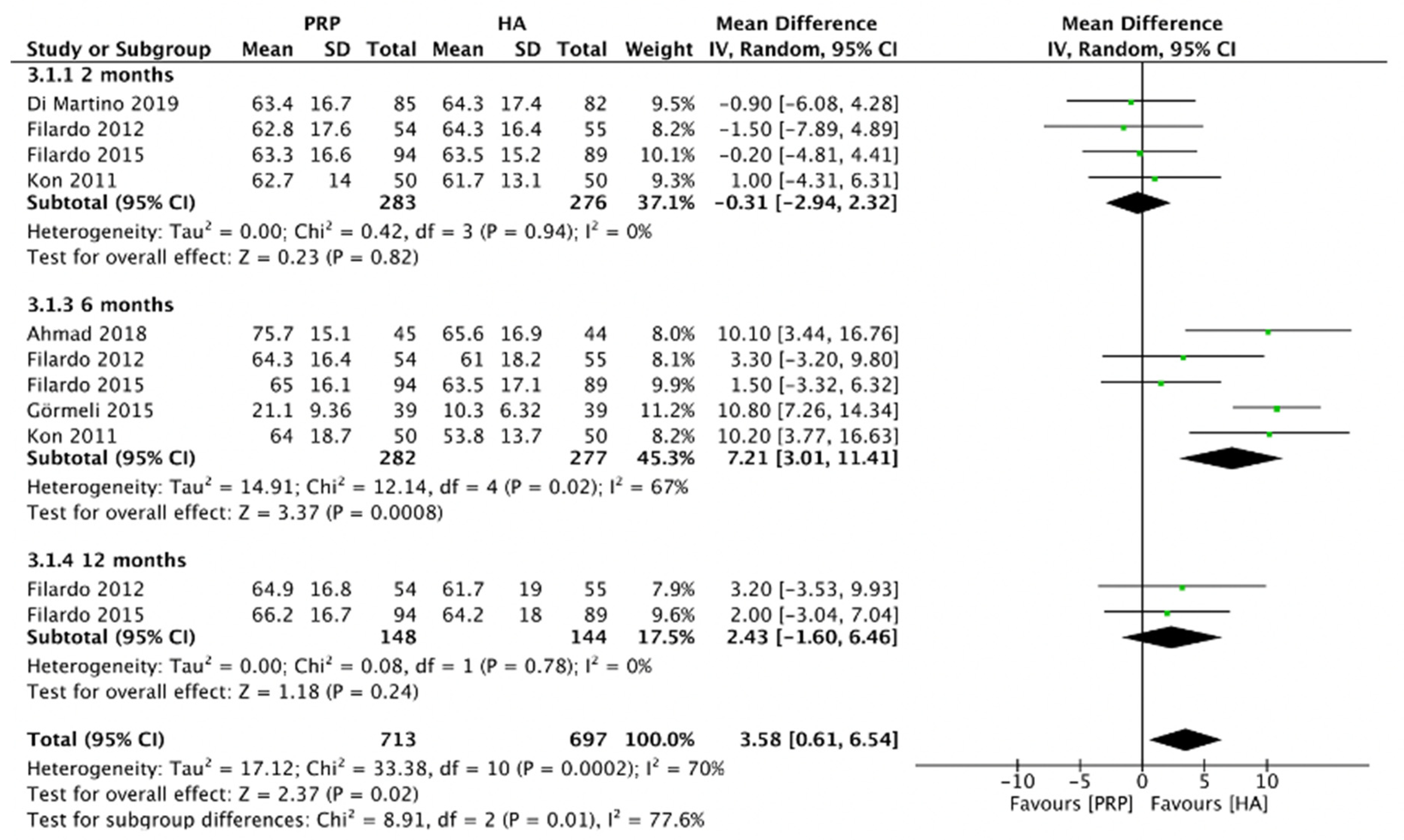
2.4.6. IKDC Score (LR-PRP)
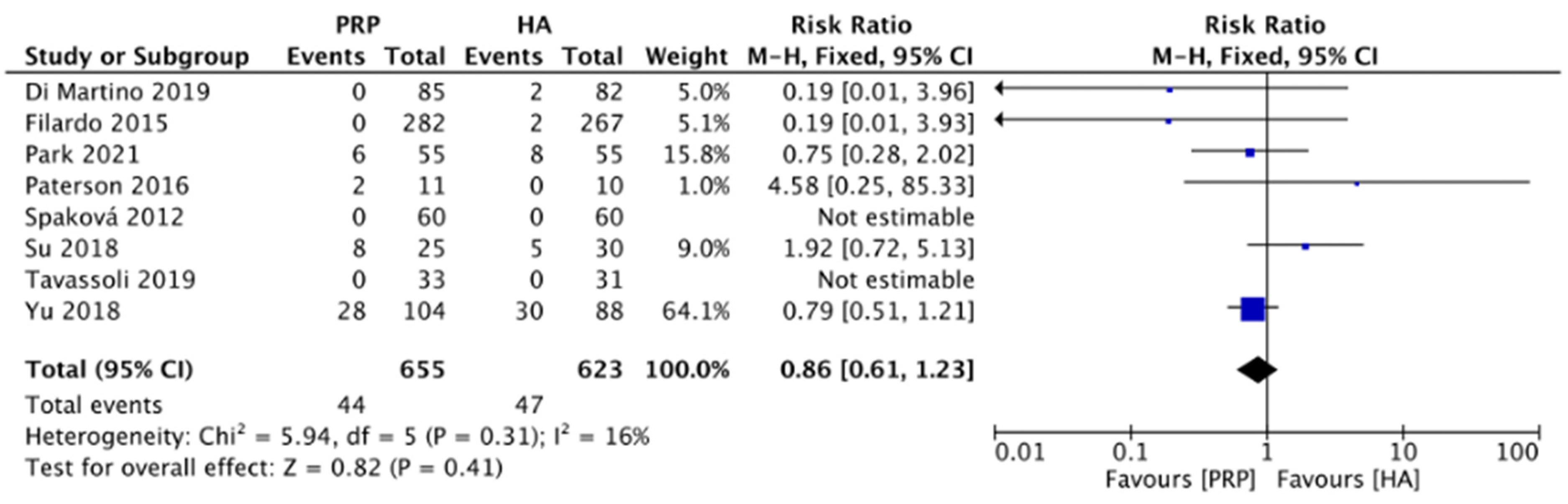
2.4.7. Adverse Events (LR-PRP)
3. Discussion
4. Materials and Methods
4.1. Systematic Search for Trials
4.2. Inclusion Criteria
4.3. Exclusion Criteria
4.4. Risk of Bias Assessment and Data Extraction
4.5. Data Analysis
5. Limitations and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Alden, K.J.; Harris, S.; Hubbs, B.; Kot, K.; Istwan, N.B.; Mason, D. Micronized Dehydrated Human Amnion Chorion Membrane Injection in the Treatment of Knee Osteoarthritis—A Large Retrospective Case Series. J. Knee Surg. 2021, 34, 841–845. [Google Scholar] [CrossRef] [PubMed]
- Prodromos, C.C.; Finkle, S.; Dawes, A.; Dizon, A. Intra-Articular Laser Treatment Plus Platelet Rich Plasma (PRP) Significantly Reduces Pain in Many Patients Who Had Failed Prior PRP Treatment. Medicines 2019, 6, 75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spreafico, A.; Chellini, F.; Frediani, B.; Bernardini, G.; Niccolini, S.; Serchi, T.; Collodel, G.; Paffetti, A.; Fossombroni, V.; Galeazzi, M.; et al. Biochemical investigation of the effects of human platelet releasates on human articular chondrocytes. J. Cell. Biochem. 2009, 108, 1153–1165. [Google Scholar] [CrossRef] [PubMed]
- Bowman, S.; Awad, M.E.; Hamrick, M.W.; Hunter, M.; Fulzele, S. Recent advances in hyaluronic acid based therapy for osteoarthritis. Clin. Transl. Med. 2018, 7, 6. [Google Scholar] [CrossRef] [Green Version]
- Dai, W.L.; Zhou, A.G.; Zhang, H.; Zhang, J. Efficacy of Platelet-Rich Plasma in the Treatment of Knee Osteoarthritis: A Meta-analysis of Randomized Controlled Trials. Arthroscopy 2017, 33, 659–670.e651. [Google Scholar] [CrossRef]
- Tang, J.Z.; Nie, M.J.; Zhao, J.Z.; Zhang, G.C.; Zhang, Q.; Wang, B. Platelet-rich plasma versus hyaluronic acid in the treatment of knee osteoarthritis: A meta-analysis. J. Orthop. Surg. Res. 2020, 15, 403. [Google Scholar] [CrossRef]
- Braun, H.J.; Kim, H.J.; Chu, C.R.; Dragoo, J.L. The effect of platelet-rich plasma formulations and blood products on human synoviocytes: Implications for intra-articular injury and therapy. Am. J. Sports Med. 2014, 42, 1204–1210. [Google Scholar] [CrossRef] [Green Version]
- Belk, J.W.; Kraeutler, M.J.; Houck, D.A.; Goodrich, J.A.; Dragoo, J.L.; McCarty, E.C. Platelet-Rich Plasma Versus Hyaluronic Acid for Knee Osteoarthritis: A Systematic Review and Meta-analysis of Randomized Controlled Trials. Am. J. Sports Med. 2021, 49, 249–260. [Google Scholar] [CrossRef]
- Filardo, G.; Kon, E.; Di Martino, A.; Di Matteo, B.; Merli, M.L.; Cenacchi, A.; Fornasari, P.M.; Marcacci, M. Platelet-rich plasma vs hyaluronic acid to treat knee degenerative pathology: Study design and preliminary results of a randomized controlled trial. BMC Musculoskelet. Disord. 2012, 13, 229. [Google Scholar] [CrossRef] [Green Version]
- Di Martino, A.; Di Matteo, B.; Papio, T.; Tentoni, F.; Selleri, F.; Cenacchi, A.; Kon, E.; Filardo, G. Platelet-Rich Plasma Versus Hyaluronic Acid Injections for the Treatment of Knee Osteoarthritis: Results at 5 Years of a Double-Blind, Randomized Controlled Trial. Am. J. Sports Med. 2019, 47, 347–354. [Google Scholar] [CrossRef]
- Kon, E.; Mandelbaum, B.; Buda, R.; Filardo, G.; Delcogliano, M.; Timoncini, A.; Fornasari, P.M.; Giannini, S.; Marcacci, M. Platelet-rich plasma intra-articular injection versus hyaluronic acid viscosupplementation as treatments for cartilage pathology: From early degeneration to osteoarthritis. Arthroscopy 2011, 27, 1490–1501. [Google Scholar] [CrossRef] [PubMed]
- Spakova, T.; Rosocha, J.; Lacko, M.; Harvanova, D.; Gharaibeh, A. Treatment of knee joint osteoarthritis with autologous platelet-rich plasma in comparison with hyaluronic acid. Am. J. Phys. Med. Rehabil. 2012, 91, 411–417. [Google Scholar] [CrossRef] [PubMed]
- Filardo, G.; Di Matteo, B.; Di Martino, A.; Merli, M.L.; Cenacchi, A.; Fornasari, P.; Marcacci, M.; Kon, E. Platelet-Rich Plasma Intra-articular Knee Injections Show No Superiority Versus Viscosupplementation: A Randomized Controlled Trial. Am. J. Sports Med. 2015, 43, 1575–1582. [Google Scholar] [CrossRef] [PubMed]
- Gormeli, G.; Gormeli, C.A.; Ataoglu, B.; Colak, C.; Aslanturk, O.; Ertem, K. Multiple PRP injections are more effective than single injections and hyaluronic acid in knees with early osteoarthritis: A randomized, double-blind, placebo-controlled trial. Knee Surg. Sports Traumatol. Arthrosc. 2017, 25, 958–965. [Google Scholar] [CrossRef]
- Raeissadat, S.A.; Rayegani, S.M.; Hassanabadi, H.; Fathi, M.; Ghorbani, E.; Babaee, M.; Azma, K. Knee Osteoarthritis Injection Choices: Platelet- Rich Plasma (PRP) Versus Hyaluronic Acid (A one-year randomized clinical trial). Clin. Med. Insights Arthritis Musculoskelet. Disord. 2015, 8, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Paterson, K.L.; Nicholls, M.; Bennell, K.L.; Bates, D. Intra-articular injection of photo-activated platelet-rich plasma in patients with knee osteoarthritis: A double-blind, randomized controlled pilot study. BMC Musculoskelet. Disord. 2016, 17, 67. [Google Scholar] [CrossRef] [Green Version]
- Duymus, T.M.; Mutlu, S.; Dernek, B.; Komur, B.; Aydogmus, S.; Kesiktas, F.N. Choice of intra-articular injection in treatment of knee osteoarthritis: Platelet-rich plasma, hyaluronic acid or ozone options. Knee Surg. Sports Traumatol. Arthrosc. 2017, 25, 485–492. [Google Scholar] [CrossRef]
- Ahmad, H.S.; Farrag, S.E.; Okasha, A.E.; Kadry, A.O.; Ata, T.B.; Monir, A.A.; Shady, I. Clinical outcomes are associated with changes in ultrasonographic structural appearance after platelet-rich plasma treatment for knee osteoarthritis. Int. J. Rheum. Dis. 2018, 21, 960–966. [Google Scholar] [CrossRef]
- Su, K.; Bai, Y.; Wang, J.; Zhang, H.; Liu, H.; Ma, S. Comparison of hyaluronic acid and PRP intra-articular injection with combined intra-articular and intraosseous PRP injections to treat patients with knee osteoarthritis. Clin. Rheumatol. 2018, 37, 1341–1350. [Google Scholar] [CrossRef]
- Yu, W.; Xu, P.; Huang, G.; Liu, L. Clinical therapy of hyaluronic acid combined with platelet-rich plasma for the treatment of knee osteoarthritis. Exp. Ther. Med. 2018, 16, 2119–2125. [Google Scholar] [CrossRef] [Green Version]
- Tavassoli, M.; Janmohammadi, N.; Hosseini, A.; Khafri, S.; Esmaeilnejad-Ganji, S.M. Single- and double-dose of platelet-rich plasma versus hyaluronic acid for treatment of knee osteoarthritis: A randomized controlled trial. World J. Orthop. 2019, 10, 310–326. [Google Scholar] [CrossRef] [PubMed]
- Park, Y.B.; Kim, J.H.; Ha, C.W.; Lee, D.H. Clinical Efficacy of Platelet-Rich Plasma Injection and Its Association With Growth Factors in the Treatment of Mild to Moderate Knee Osteoarthritis: A Randomized Double-Blind Controlled Clinical Trial As Compared With Hyaluronic Acid. Am. J. Sports Med. 2021, 49, 487–496. [Google Scholar] [CrossRef] [PubMed]
- Cole, B.J.; Karas, V.; Hussey, K.; Pilz, K.; Fortier, L.A. Hyaluronic Acid Versus Platelet-Rich Plasma: A Prospective, Double-Blind Randomized Controlled Trial Comparing Clinical Outcomes and Effects on Intra-articular Biology for the Treatment of Knee Osteoarthritis. Am. J. Sports Med. 2017, 45, 339–346. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.P.C.; Hsu, C.C.; Huang, S.C.; Lin, M.Y.; Chen, J.L.; Lin, S.Y. The application of thermal oscillation method to augment the effectiveness of autologous platelet rich plasma in treating elderly patients with knee osteoarthritis. Exp. Gerontol. 2020, 142, 111120. [Google Scholar] [CrossRef] [PubMed]
- Gong, H.; Li, K.; Xie, R.; Du, G.; Li, L.; Wang, S.; Yin, J.; Gu, J.; Wang, P.; Chen, M.; et al. Clinical therapy of platelet-rich plasma vs hyaluronic acid injections in patients with knee osteoarthritis: A systematic review and meta-analysis of randomized double-blind controlled trials. Medicine 2021, 100, e25168. [Google Scholar] [CrossRef] [PubMed]
- Dong, Y.; Zhang, B.; Yang, Q.; Zhu, J.; Sun, X. The effects of platelet-rich plasma injection in knee and hip osteoarthritis: A meta-analysis of randomized controlled trials. Clin. Rheumatol. 2021, 40, 263–277. [Google Scholar] [CrossRef]
- Le, A.D.K.; Enweze, L.; DeBaun, M.R.; Dragoo, J.L. Current Clinical Recommendations for Use of Platelet-Rich Plasma. Curr. Rev. Musculoskelet. Med. 2018, 11, 624–634. [Google Scholar] [CrossRef]
- Sundman, E.A.; Cole, B.J.; Fortier, L.A. Growth Factor and Catabolic Cytokine Concentrations Are Influenced by the Cellular Composition of Platelet-Rich Plasma. Am. J. Sport Med. 2011, 39, 2135–2140. [Google Scholar] [CrossRef]
- Simental-Mendia, M.; Vilchez-Cavazos, J.; Pena-Martinez, V.M.; Said-Fernandez, S.; Lara-Arias, J.; Martinez-Rodriguez, H.G. Leukocyte-poor platelet-rich plasma is more effective than the conventional therapy with acetaminophen for the treatment of early knee osteoarthritis. Arch. Orthop. Trauma Surg. 2016, 136, 1723–1732. [Google Scholar] [CrossRef]
- Uchiyama, R.; Toyoda, E.; Maehara, M.; Wasai, S.; Omura, H.; Watanabe, M.; Sato, M. Effect of Platelet-Rich Plasma on M1/M2 Macrophage Polarization. Int. J. Mol. Sci. 2021, 22, 2336. [Google Scholar] [CrossRef]
- Higgins, J.P.; Green, S. Cochrane Collaboration. Cochrane Handbook for Systematic Reviews of Interventions; Wiley-Blackwell: Chichester, UK; Hoboken, NJ, USA, 2008. [Google Scholar]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Health Care Interventions: Explanation and Elaboration. Ann. Intern. Med. 2009, 151, W65–W94. [Google Scholar] [CrossRef] [PubMed] [Green Version]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Included Trials | Study Type | Group | Patients | Age (Years, PRP/HA) | Gender (Male/Female, N) | Stage of Knee OA (Kellgren and Lawrence Classification) | Outcome Measurements | Follow-Up Period (Months) |
|---|---|---|---|---|---|---|---|---|
| Kon et al., 2011 (Italy) [11] | RCT | LR-PRP HA | 50 50 | 50.6 ± 13.8 54.9 ± 12.6 | 30/20 25/25 | 0–4 | EQ-VAS, IKDC, adverse events | 2, 6 |
| Filardo et al., 2012 (Italy) [9] | RCT | LR-PRP HA | 54 55 | 55 58 | 37/17 31/24 | 0–3 | IKDC | 2, 6, 12 |
| Spaková et al., 2012 (Slovakia) [12] | RCT | LR-PRP HA | 60 60 | 52.80 ± 12.43 53.20 ± 14.53 | 33/27 31/29 | 1–3 | WOMAC, adverse events | 3, 6 |
| Filardo et al., 2015 (Italy) [13] | RCT | LR-PRP HA | 94 89 | 53.32 ± 13.2 57.55 ± 11.8 | 60/34 52/37 | 0–3 | EQ-VAS, IKDC, adverse events | 2, 6, 12 |
| Görmeli et al., 2015 (Turkey) [14] | RCT | LR-PRP HA | 39 39 | 53.8 ± 23.1 53.5 ± 14 | 16/23 17/22 | 0–4 | EQ-VAS, IKDC | 6 |
| Raeissadat et al., 2015 (Iran) [15] | RCT | LR-PRP HA | 77 62 | 56.85 ± 9.13 61.13 ± 7.48 | 8/69 15/47 | 1–4 | WOMAC | 12 |
| Paterson et al., 2016 (Australia) [16] | RCT | LR-PRP HA | 11 10 | 49.91 ± 13.72 52.70 ± 10.30 | 8/3 7/3 | 2–3 | VAS, adverse effects | 1, 3 |
| Duymus et al., 2017 (Turkey) [17] | RCT | LR-PRP HA | 33 34 | 60.4 ± 5.1 60.3 ± 9.1 | 1/32 1/33 | 2–3 | WOMAC, VAS | 1, 3, 6, 12 |
| Ahmad et al., 2018 (Egypt) [18] | RCT | LR-PRP HA | 45 44 | 56.2 ± 6.8 56.8 ± 7.4 | 14/31 14/30 | 1–3 | VAS, IKDC | 3, 6 |
| Su et al., 2018 (China) [19] | RCT | LR-PRP HA | 25 30 | 54.16 ± 6.56 53.13 ± 6.41 | 11/14 12/18 | 2–3 | WOMAC, VAS, adverse effects | 1, 3, 6, 12, 18 |
| Yu et al., 2018 (China) [20] | RCT | LR-PRP HA | 104 88 | 46.2 ± 8.6 51.5 ± 9.3 | 50/54 48/40 | Not specified | WOMAC, adverse effects | 12 |
| Di Martino et al., 2019 (Italy) [10] | RCT | LR-PRP HA | 85 82 | 52.7 ± 13.2 57.5 ± 11.7 | 53/32 47/35 | 0–3 | EQ-VAS, IKDC, adverse events | 2, 6, 12, 24 |
| Tavassoli et al., 2019 (Italy) [21] | RCT | LR-PRP HA | 28 27 | 66.04 ± 7.58 63.30 ± 8.87 | 6/22 8/19 | Ahlbäck classification:1–5 | WOMAC, VAS, adverse effects | 1, 2, 3 |
| Park et al., 2021 (South Korea) [22] | RCT | LR-PRP HA | 55 55 | 60.6 ± 8.2 62.3 ± 9.6 | 16/39 8/47 | 1–3 | WOMAC, VAS, adverse effects | 1.5, 3, 6 |
| Included Trials | LR-PRP | HA | |||||
|---|---|---|---|---|---|---|---|
| Dosage (mL) | Intervals (Weeks) | Injection Times | Dosage | Molecular Weight (kDa) | Intervals (Weeks) | Injection Times | |
| Kon et al., 2011 (Italy) [11] | 5 | 2 | 3 | 30 mg/2 mL | 500–2900 | NA | 1 |
| Filardo et al., 2012 (Italy) [9] | 5 | 1 | 3 | 30 mg/2 mL | >1500 | 1 | 3 |
| Spaková et al., 2012 (Slovakia) [12] | 3 | 1 | 3 | NA | Not mentioned | 1 | 3 |
| Filardo et al., 2015 (Italy) [13] | 5 | 1 | 3 | 30 mg/2 mL | >1500 | 1 | 3 |
| Görmeli et al., 2015 (Turkey) [14] | 5 | 1 | 3 | 30 mg/2 mL | Not mentioned | 1 | 3 |
| Raeissadat et al., 2015 (Iran) [15] | 4–6 | 4 | 2 | 20 mg/2 mL | 500–730 | 1 | 3 |
| Paterson et al., 2016 (Australia) [16] | 3 | 1 | 3 | 3 | Not mentioned | 1 | 3 |
| Duymus et al., 2017 (Turkey) [17] | 5 | 4 | 2 | 40 mg/2 mL | 1600 | 4 | 1 |
| Ahmad et al., 2018 (Egypt) [18] | 4 | 2 | 3 | 20 mg/2 mL | Not mentioned | 2 | 3 |
| Su et al., 2018 (China) [19] | 6 | 2 | 2 | 2 mL | 600–1500 | 1 | 5 |
| Yu et al., 2018 (China) [20] | 2–14 | 1 | 4 | 0.1–0.3 mg | Not mentioned | 1 | 4 |
| Di Martino et al., 2019 (Italy) [10] | 5 | 1 | 3 | 30 mg/2 mL | >1500 | 1 | 3 |
| Tavassoli et al., 2019 (Italy) [21] | 4–6 | 3 | 2 | 30 mg/2 mL | 500–730 | 1 | 4 |
| Park et al., 2021 (South Korea) [22] | 3 | NA | 1 | 30 mg/3 mL | >10,000 | NA | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peng, Y.-N.; Chen, J.-L.; Hsu, C.-C.; Chen, C.P.C.; Suputtitada, A. Intra-Articular Leukocyte-Rich Platelet-Rich Plasma versus Intra-Articular Hyaluronic Acid in the Treatment of Knee Osteoarthritis: A Meta-Analysis of 14 Randomized Controlled Trials. Pharmaceuticals 2022, 15, 974. https://doi.org/10.3390/ph15080974
Peng Y-N, Chen J-L, Hsu C-C, Chen CPC, Suputtitada A. Intra-Articular Leukocyte-Rich Platelet-Rich Plasma versus Intra-Articular Hyaluronic Acid in the Treatment of Knee Osteoarthritis: A Meta-Analysis of 14 Randomized Controlled Trials. Pharmaceuticals. 2022; 15(8):974. https://doi.org/10.3390/ph15080974
Chicago/Turabian StylePeng, Yu-Ning, Jean-Lon Chen, Chih-Chin Hsu, Carl P. C. Chen, and Areerat Suputtitada. 2022. "Intra-Articular Leukocyte-Rich Platelet-Rich Plasma versus Intra-Articular Hyaluronic Acid in the Treatment of Knee Osteoarthritis: A Meta-Analysis of 14 Randomized Controlled Trials" Pharmaceuticals 15, no. 8: 974. https://doi.org/10.3390/ph15080974