
Exploring the Mechanisms Underlying Drug-Induced Fractures Using the Japanese Adverse Drug Event Reporting Database

 ,
,
Abstract
:1. Introduction
2. Results
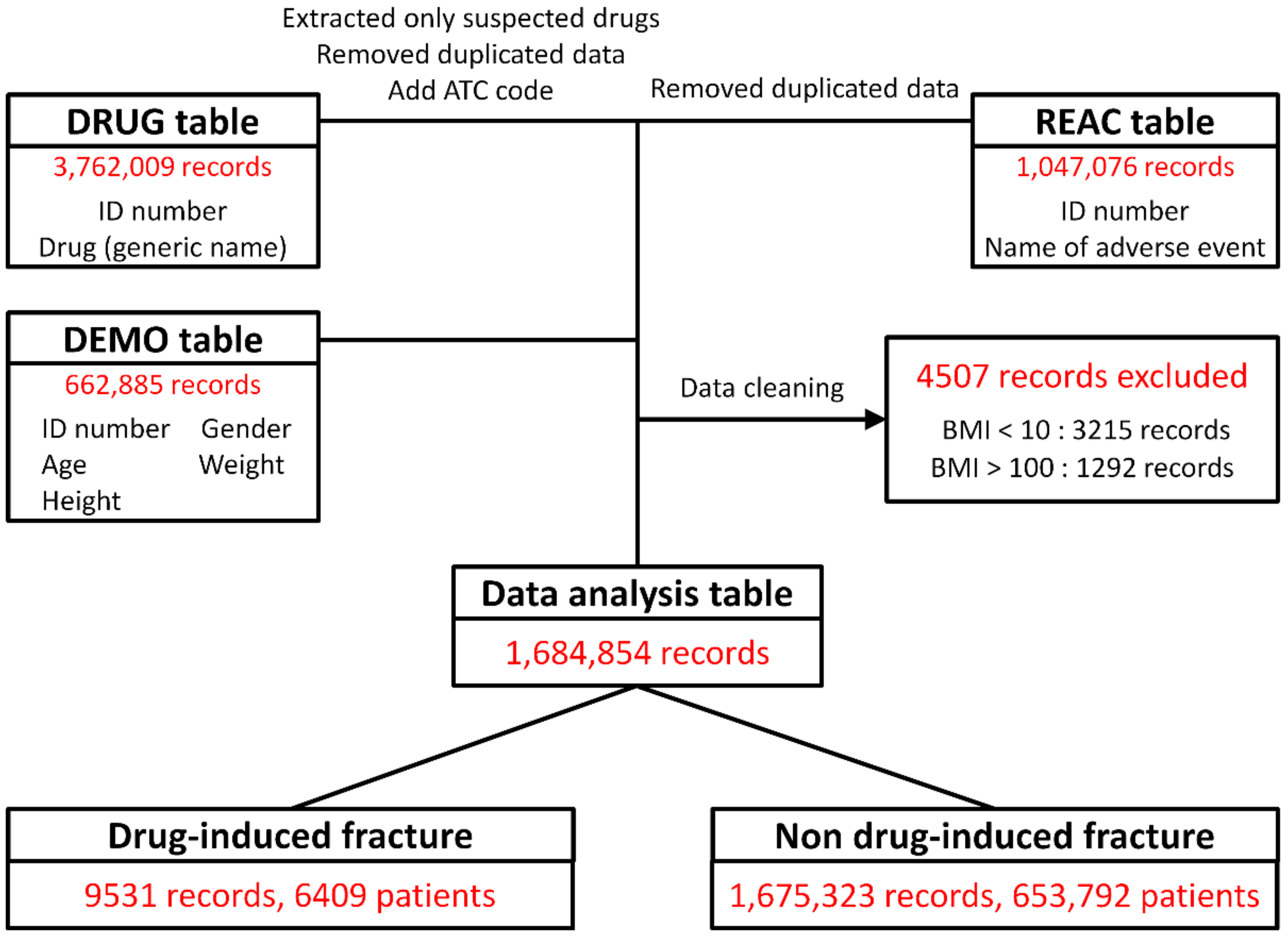
2.1. Construction of Data Analysis Tables
2.2. Sites of Drug-Induced Fractures
2.3. Association between Patient Characteristics and Drug-Induced Fractures
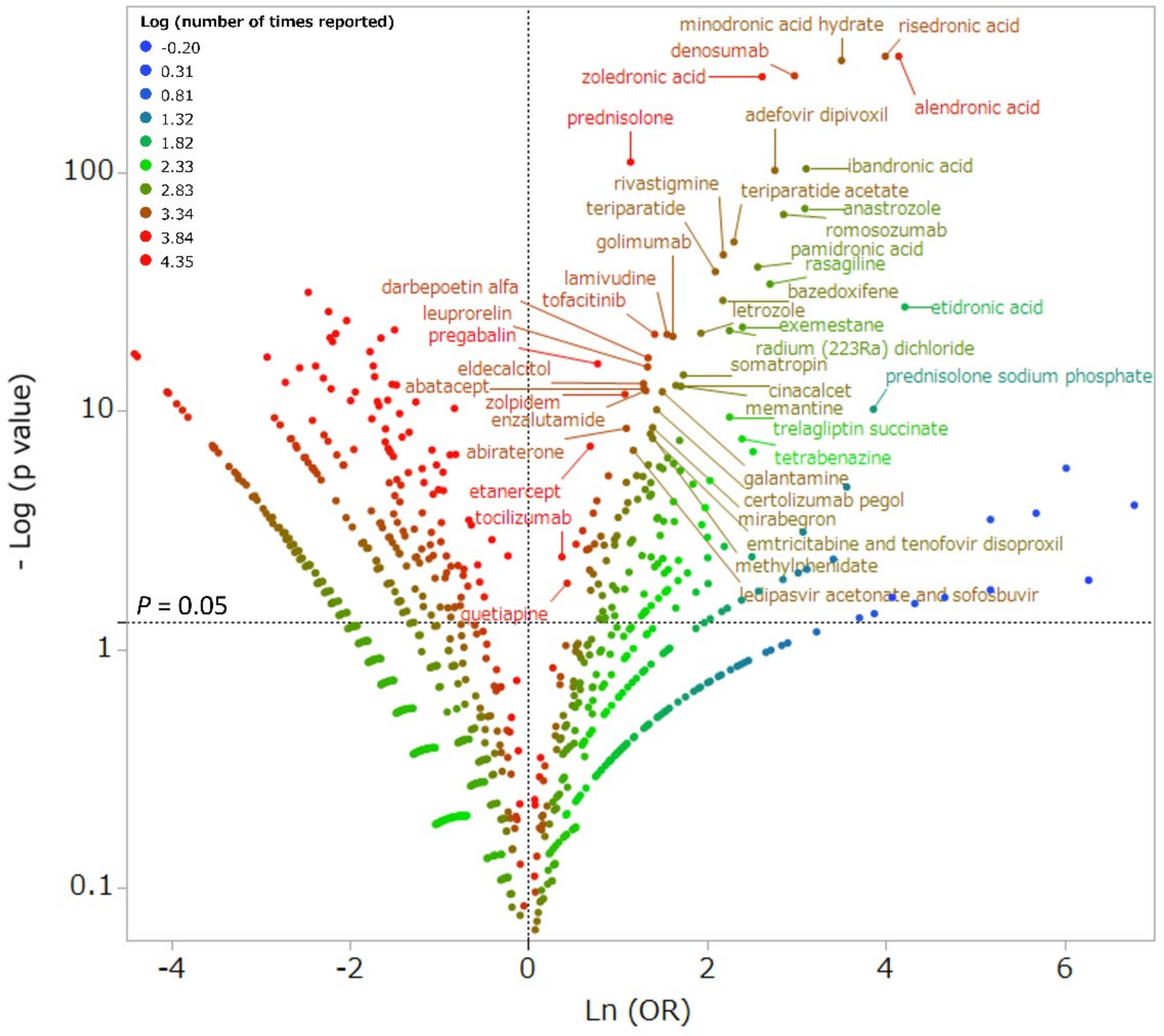
2.4. Association between Drug Use and Drug-Induced Fractures
2.5. Independent Risk Factors for Drug-Induced Fracture by Multiple Logistic Regression Analysis
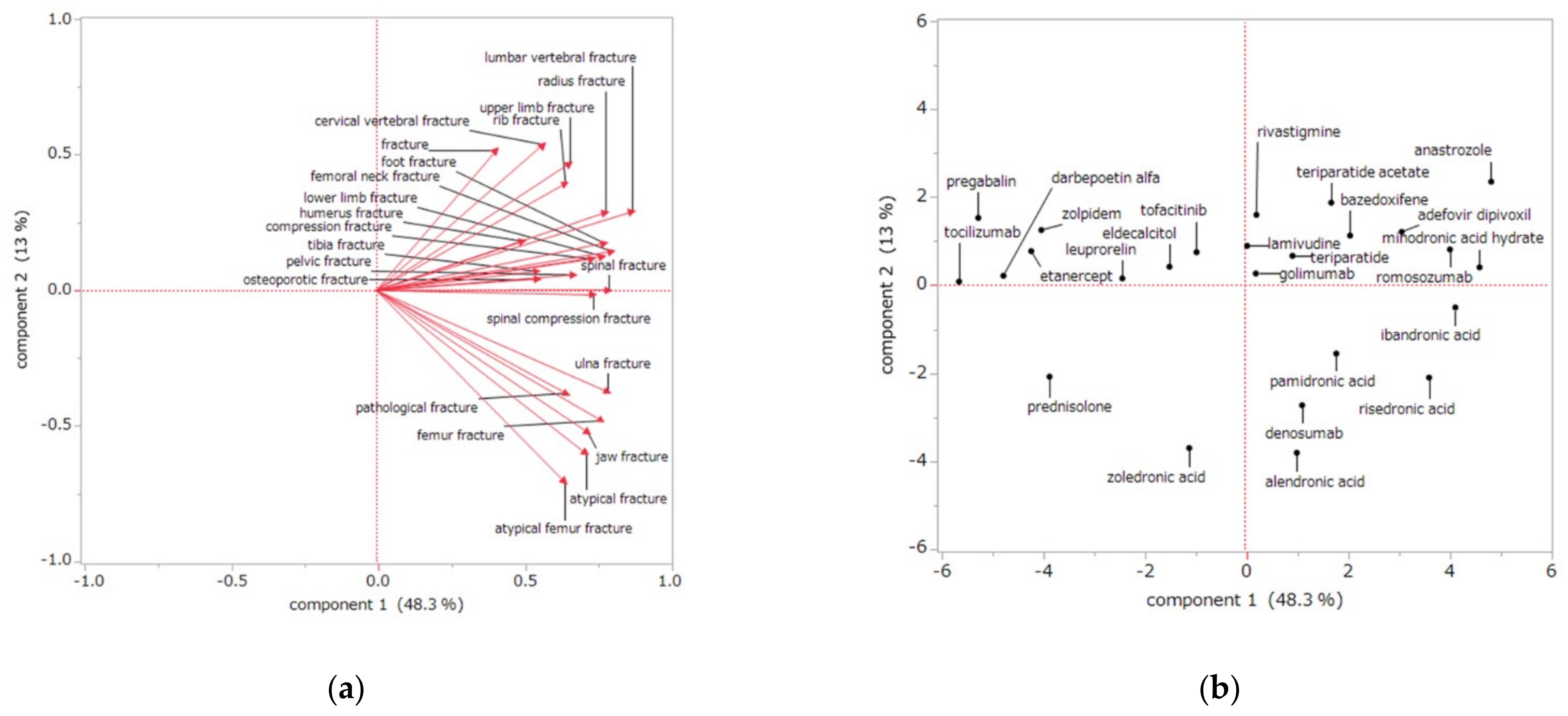
2.6. Association between Drug Use and the Drug-Induced Fracture Site by Principal Component Analysis
3. Discussion
3.1. Drug-Induced Fracture Sites
3.2. Risk Factors for Drug-Induced Fractures
3.3. Association between Drug Use and the Drug-Induced Fracture Site
3.4. Limitations
4. Materials and Methods
4.1. JADER Database and the Selection of Data for Analysis
4.2. Association between Patient Characteristics and Drug-Induced Fracture by Single Regression Analysis
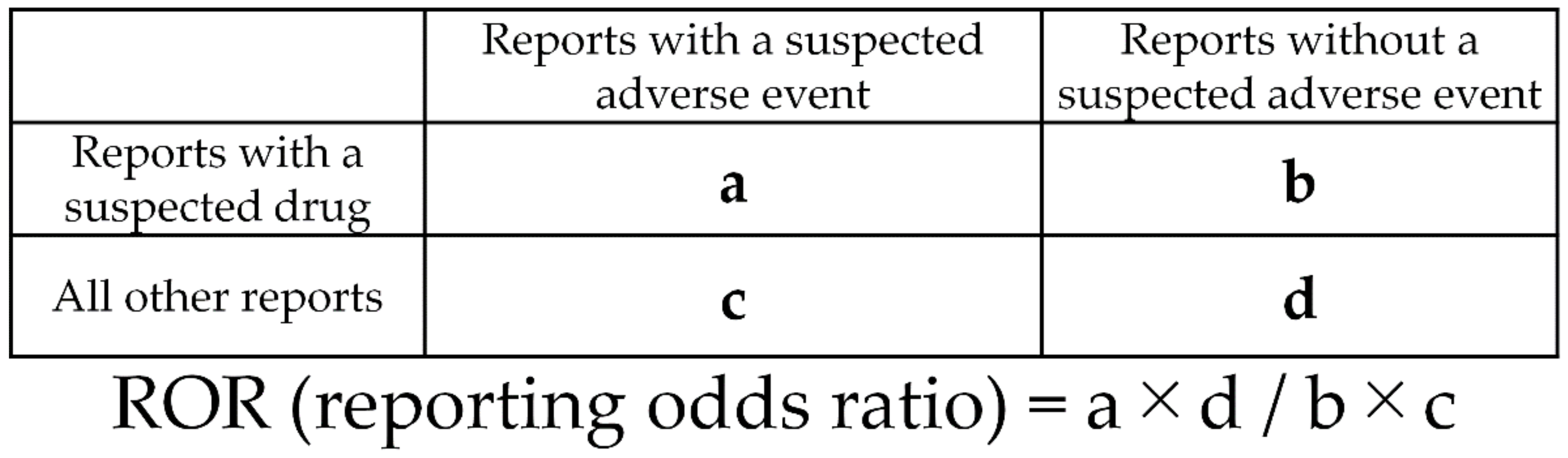
4.3. Association between Drug Use and Drug-Induced Fractures by Single Regression Analysis
4.4. Associated between Patient Characteristics and Drug-Induced Fracture by Multiple Logistic Regression Analysis
4.5. Association between Drug Use and Drug-Induced Fracture Site by Principal Component Analysis
4.6. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Stone, K.L.; Seeley, D.G.; Lui, L.Y.; Cauley, J.A.; Ensrud, K.; Browner, W.S.; Nevitt, M.C.; Cummings, S.R.; Osteoporotic Fractures Research Group. BMD at multiple sites and risk of fracture of multiple types: Long-term results from the Study of Osteoporotic Fractures. J. Bone Miner. Res. 2003, 18, 1947–1954. [Google Scholar] [CrossRef] [PubMed]
- Parkkari, J.; Kannus, P.; Palvanen, M.; Natri, A.; Vainio, J.; Aho, H.; Vuori, I.; Järvinen, M. Majority of hip fractures occur as a result of a fall and impact on the greater trochanter of the femur: A prospective controlled hip fracture study with 206 consecutive patients. Calcif. Tissue Int. 1999, 65, 183–187. [Google Scholar] [CrossRef] [PubMed]
- Palvanen, M.; Kannus, P.; Parkkari, J.; Pitkäjärvi, T.; Pasanen, M.; Vuori, I.; Järvinen, M. The injury mechanisms of osteoporotic upper extremity fractures among older adults: A controlled study of 287 consecutive patients and their 108 controls. Osteoporos. Int. 2000, 11, 822–831. [Google Scholar] [CrossRef] [PubMed]
- NIH Consensus Development Panel on Osteoporosis Prevention, Diagnosis, and Therapy. Osteoporosis prevention, diagnosis, and therapy. JAMA 2001, 285, 785–795. [Google Scholar] [CrossRef]
- Thorell, K.; Ranstad, K.; Midlöv, P.; Borgquist, L.; Halling, A. Is use of fall risk-increasing drugs in an elderly population associated with an increased risk of hip fracture, after adjustment for multimorbidity level: A cohort study. BMC Geriatr. 2014, 14, 131. [Google Scholar] [CrossRef] [Green Version]
- Toriumi, S.; Kobayashi, A.; Uesawa, Y. Comprehensive Study of the Risk Factors for Medication-Related Osteonecrosis of the Jaw Based on the Japanese Adverse Drug Event Report Database. Pharmaceuticals 2020, 13, 467. [Google Scholar] [CrossRef]
- Hirooka, T.; Yamada, M. Evaluation of AEs risk using the “Japanese Adverse Drug Event Report database” of PMDA. In Proceedings of the SAS User General Assembly, Tokyo, Japan, 1–3 December 2012; pp. 263–270. [Google Scholar]
- Odvina, C.V.; Zerwekh, J.E.; Rao, D.S.; Maalouf, N.; Gottschalk, F.A.; Pak, C.Y. Severely suppressed bone turnover: A potential complication of alendronate therapy. J. Clin. Endocrinol. Metab. 2005, 90, 1294–1301. [Google Scholar] [CrossRef]
- Shane, E.; Burr, D.; Abrahamsen, B.; Adler, R.A.; Brown, T.D.; Cheung, A.M.; Cosman, F.; Curtis, J.R.; Dell, R.; Dempster, D.W.; et al. Atypical subtrochanteric and diaphyseal femoral fractures: Second report of a task force of the American Society for Bone and Mineral Research. J. Bone Miner. Res. 2014, 29, 1–23. [Google Scholar] [CrossRef] [Green Version]
- Ruggiero, S.L.; Dodson, T.B.; Fantasia, J.; Goodday, R.; Aghaloo, T.; Mehrotra, B.; O’Ryan, F.; American Association of Oral and Maxillofacial Surgeons. American Association of Oral and Maxillofacial Surgeons position paper on medication-related osteonecrosis of the jaw—2014 update. J. Oral. Maxillofac. Surg. 2014, 72, 1938–1956. [Google Scholar] [CrossRef]
- FitzGerald, G.; Boonen, S.; Compston, J.E.; Pfeilschifter, J.; LaCroix, A.Z.; Hosmer, D.W., Jr.; Hooven, F.H.; Gehlbach, S.H.; GLOW Investigators. Differing risk profiles for individual fracture sites: Evidence from the Global Longitudinal Study of Osteoporosis in Women (GLOW). J. Bone Miner. Res. 2012, 27, 1907–1915. [Google Scholar] [CrossRef]
- Johnell, O.; Kanis, J.A. An estimate of the worldwide prevalence, mortality and disability associated with hip fracture. Osteoporos. Int. 2004, 15, 897–902. [Google Scholar] [CrossRef]
- Abrahamsen, B.; van Staa, T.; Ariely, R.; Olson, M.; Cooper, C. Excess mortality following hip fracture: A systematic epidemiological review. Osteoporos. Int. 2009, 20, 1633–1650. [Google Scholar] [CrossRef]
- Fujiwara, S.; Kasagi, F.; Masunari, N.; Naito, K.; Suzuki, G.; Fukunaga, M. Fracture prediction from bone mineral density in Japanese men and women. J. Bone Miner. Res. 2003, 18, 1547–1553. [Google Scholar] [CrossRef]
- Suzuki, Y.; Nawata, H.; Soen, S.; Fujiwara, S.; Nakayama, H.; Tanaka, I.; Ozono, K.; Sagawa, A.; Takayanagi, R.; Tanaka, H.; et al. Guidelines on the management and treatment of glucocorticoid-induced osteoporosis of the Japanese Society for Bone and Mineral Research: 2014 update. J. Bone Miner. Metab. 2014, 32, 337–350. [Google Scholar] [CrossRef]
- Arai, K.; Hanyu, T.; Sugitani, H.; Murai, T.; Fujisawa, J.; Nakazono, K.; Kondo, N.; Endo, N. Risk factors for vertebral fracture in menopausal or postmenopausal Japanese women with rheumatoid arthritis: A cross-sectional and longitudinal study. J. Bone Miner. Metab. 2006, 24, 118–124. [Google Scholar] [CrossRef]
- Kragh Ekstam, A.; Elmståhl, S. Do fall-risk-increasing drugs have an impact on mortality in older hip fracture patients? A population-based cohort study. Clin. Interv. Aging 2016, 29, 489–496. [Google Scholar] [CrossRef] [Green Version]
- Iki, M.; Fujita, Y.; Tamaki, J.; Kouda, K.; Yura, A.; Kadowaki, E.; Sato, Y.; Moon, J.S.; Okamoto, N.; Kurumatani, N.; et al. Design and baseline characteristics of a prospective cohort study for determinants of osteoporotic fracture in community-dwelling elderly Japanese men: The Fujiwara-kyo osteoporosis risk in men (FORMEN) study. BMC Musculoskelet. Disord. 2009, 10, 165. [Google Scholar] [CrossRef] [Green Version]
- Yoshimura, N.; Hashimoto, T.; Sakata, K.; Morioka, S.; Kasamatsu, T.; Cooper, C. Biochemical markers of bone turnover and bone loss at the lumbar spine and femoral neck: The Taiji study. Calcif. Tissue Int. 1999, 65, 198–202. [Google Scholar] [CrossRef]
- Zenke, Y.; Ikeda, S.; Fukuda, F.; Tanaka, M.; Tanaka, H.; Hirano, F.; Sakai, A. Study of Atypical Femoral Fracture Cases Coupled in a Multicenter Study. J. UOEH 2016, 38, 207–214. [Google Scholar] [CrossRef] [Green Version]
- Taormina, D.P.; Marcano, A.I.; Karia, R.; Egol, K.A.; Tejwani, N.C. Symptomatic atypical femoral fractures are related to underlying hip geometry. Bone 2014, 63, 1–6. [Google Scholar] [CrossRef]
- Velasco, S.; Kim, S.; Bleakney, R.; Jamal, S.A. The clinical characteristics of patients with hip fractures in typical locations and atypical femoral fractures. Arch. Osteoporos. 2014, 9, 171. [Google Scholar] [CrossRef]
- De Laet, C.; Kanis, J.A.; Odén, A.; Johanson, H.; Johnell, O.; Delmas, P.; Eisman, J.A.; Kroger, H.; Fujiwara, S.; Garnero, P.; et al. Body mass index as a predictor of fracture risk: A meta-analysis. Osteoporos. Int. 2005, 16, 1330–1338. [Google Scholar] [CrossRef]
- Russell, R.G. Bisphosphonates: The first 40 years. Bone 2011, 49, 2–19. [Google Scholar] [CrossRef]
- Feldstein, A.C.; Black, D.; Perrin, N.; Rosales, A.G.; Friess, D.; Boardman, D.; Dell, R.; Santora, A.; Chandler, J.M.; Rix, M.M.; et al. Incidence and demography of femur fractures with and without atypical features. J. Bone Miner. Res. 2012, 27, 977–986. [Google Scholar] [CrossRef]
- Cummings, S.R.; San Martin, J.; McClung, M.R.; Siris, E.S.; Eastell, R.; Reid, I.R.; Delmas, P.; Zoog, H.B.; Austin, M.; Wang, A.; et al. Denosumab for prevention of fractures in postmenopausal women with osteoporosis. N. Engl. J. Med. 2009, 361, 756–765. [Google Scholar] [CrossRef] [Green Version]
- Fizazi, K.; Carducci, M.; Smith, M.; Damião, R.; Brown, J.; Karsh, L.; Milecki, P.; Shore, N.; Rader, M.; Wang, H.; et al. Denosumab versus zoledronic acid for treatment of bone metastases in men with castration-resistant prostate cancer: A randomised, double-blind study. Lancet 2011, 377, 813–822. [Google Scholar] [CrossRef] [Green Version]
- Thompson, R.N.; Armstrong, C.L.; Heyburn, G. Bilateral atypical femoral fractures in a patient prescribed denosumab—A case report. Bone 2014, 61, 44–47. [Google Scholar] [CrossRef]
- Schilcher, J.; Aspenberg, P. Atypical fracture of the femur in a patient using denosumab—A case report. Acta Orthop. 2014, 85, 6–7. [Google Scholar] [CrossRef] [Green Version]
- Takahashi, M.; Ozaki, Y.; Kizawa, R.; Masuda, J.; Sakamaki, K.; Kinowaki, K.; Umezu, T.; Kondoh, C.; Tanabe, Y.; Tamura, N.; et al. Atypical femoral fracture in patients with bone metastasis receiving denosumab therapy: A retrospective study and systematic review. BMC Cancer 2019, 19, 980. [Google Scholar] [CrossRef] [Green Version]
- Limones, A.; Sáez-Alcaide, L.M.; Díaz-Parreño, S.A.; Helm, A.; Bornstein, M.M.; Molinero-Mourelle, P. Medication-related osteonecrosis of the jaws (MRONJ) in cancer patients treated with denosumab VS. zoledronic acid: A systematic review and meta-analysis. Med. Oral. Patol. Oral. Cir. Bucal. 2020, 25, e326–e336. [Google Scholar] [CrossRef]
- Brown, T.T.; Qaqish, R.B. Antiretroviral therapy and the prevalence of osteopenia and osteoporosis: A meta-analytic review. AIDS 2006, 20, 2165–2174. [Google Scholar] [CrossRef] [PubMed]
- Borderi, M.; Gibellini, D.; Vescini, F.; De Crignis, E.; Cimatti, L.; Biagetti, C.; Tampellini, L.; Re, M.C. Metabolic bone disease in HIV infection. AIDS 2009, 23, 1297–1310. [Google Scholar] [CrossRef] [PubMed]
- Brown, T.T.; McComsey, G.A.; King, M.S.; Qaqish, R.B.; Bernstein, B.M.; da Silva, B.A. Loss of bone mineral density after antiretroviral therapy initiation, independent of antiretroviral regimen. J. Acquir. Immune Defic. Syndr. 2009, 51, 554–561. [Google Scholar] [CrossRef] [PubMed]
- Van Staa, T.P.; Leufkens, H.G.; Cooper, C. The epidemiology of corticosteroid-induced osteoporosis: A meta-analysis. Osteoporos. Int. 2002, 13, 777–787. [Google Scholar] [CrossRef] [Green Version]
- Kanis, J.A.; Johansson, H.; Oden, A.; Johnell, O.; de Laet, C.; Melton, L.J., III; Tenenhouse, A.; Reeve, J.; Silman, A.J.; Pols, H.A.; et al. A meta-analysis of prior corticosteroid use and fracture risk. J. Bone Miner. Res. 2004, 19, 893–899. [Google Scholar] [CrossRef]
- American College of Rheumatology Task Force on Osteoporosis Guidelines. Recommendations for the prevention and treatment of glucocorticoid-induced osteoporosis. Arthritis Rheum. 1996, 39, 1791–1801. [Google Scholar] [CrossRef]
- Walsh, L.J.; Wong, C.A.; Pringle, M.; Tattersfield, A.E. Use of oral corticosteroids in the community and the prevention of secondary osteoporosis: A cross sectional study. BMJ 1996, 313, 344–346. [Google Scholar] [CrossRef] [Green Version]
- Manolagas, S.C.; Weinstein, R.S. New developments in the pathogenesis and treatment of steroid-induced osteoporosis. J. Bone Miner. Res. 1999, 14, 1061–1066. [Google Scholar] [CrossRef]
- Weinstein, R.S.; Jilka, R.L.; Parfitt, A.M.; Manolagas, S.C. Inhibition of osteoblastogenesis and promotion of apoptosis of osteoblasts and osteocytes by glucocorticoids. Potential mechanisms of their deleterious effects on bone. J. Clin. Investig. 1998, 102, 274–282. [Google Scholar] [CrossRef] [Green Version]
- Weinstein, R.S.; Chen, J.R.; Powers, C.C.; Stewart, S.A.; Landes, R.D.; Bellido, T.; Jilka, R.L.; Parfitt, A.M.; Manolagas, S.C. Promotion of osteoclast survival and antagonism of bisphosphonate-induced osteoclast apoptosis by glucocorticoids. J. Clin. Investig. 2002, 109, 1041–1048. [Google Scholar] [CrossRef]
- Mazziotti, G.; Angeli, A.; Bilezikian, J.P.; Canalis, E.; Giustina, A. Glucocorticoid-induced osteoporosis: An update. Trends Endocrinol. Metab. 2006, 17, 144–149. [Google Scholar] [CrossRef]
- Van Geel, T.A.; Geusens, P.P.; Winkens, B.; Sels, J.P.; Dinant, G.J. Measures of bioavailable serum testosterone and estradiol and their relationships with muscle mass, muscle strength and bone mineral density in postmenopausal women: A cross-sectional study. Eur. J. Endocrinol. 2009, 160, 681–687. [Google Scholar] [CrossRef] [Green Version]
- Goss, P.E.; Ingle, J.N.; Pritchard, K.I.; Robert, N.J.; Muss, H.; Gralow, J.; Gelmon, K.; Whelan, T.; Strasser-Weippl, K.; Rubin, S.; et al. Extending Aromatase-Inhibitor Adjuvant Therapy to 10 Years. N. Engl. J. Med. 2016, 375, 209–219. [Google Scholar] [CrossRef] [Green Version]
- Walsh, J.S.; Eastell, R. Osteoporosis in men. Nat. Rev. Endocrinol. 2013, 9, 637–645. [Google Scholar] [CrossRef]
- De Groot, M.H.; van Campen, J.P.; Moek, M.A.; Tulner, L.R.; Beijnen, J.H.; Lamoth, C.J. The effects of fall-risk-increasing drugs on postural control: A literature review. Drugs Aging 2013, 30, 901–920. [Google Scholar] [CrossRef]
- Seppala, L.J.; Wermelink, A.M.A.T.; de Vries, M.; Ploegmakers, K.J.; van de Glind, E.M.M.; Daams, J.G.; van der Velde, N.; EUGMS task and Finish group on fall-risk-increasing drugs. Fall-Risk-Increasing Drugs: A Systematic Review and Meta-Analysis: II. Psychotropics. J. Am. Med. Dir. Assoc. 2018, 19, 371.e11–371.e17. [Google Scholar] [CrossRef] [Green Version]
- Woolcott, J.C.; Richardson, K.J.; Wiens, M.O.; Patel, B.; Marin, J.; Khan, K.M.; Marra, C.A. Meta-analysis of the impact of 9 medication classes on falls in elderly persons. Arch. Intern. Med. 2009, 169, 1952–1960. [Google Scholar] [CrossRef] [Green Version]
- Pariente, A.; Dartigues, J.F.; Benichou, J.; Letenneur, L.; Moore, N.; Fourrier-Réglat, A. Benzodiazepines and injurious falls in community dwelling elders. Drugs Aging 2008, 25, 61–70. [Google Scholar] [CrossRef]
- Matinolli, M.; Korpelainen, J.T.; Sotaniemi, K.A.; Myllylä, V.V.; Korpelainen, R. Recurrent falls and mortality in Parkinson’s disease: A prospective two-year follow-up study. Acta Neurol. Scand. 2011, 123, 193–200. [Google Scholar] [CrossRef]
- Allcock, L.M.; Rowan, E.N.; Steen, I.N.; Wesnes, K.; Kenny, R.A.; Burn, D.J. Impaired attention predicts falling in Parkinson’s disease. Parkinsonism Relat. Disord. 2009, 15, 110–115. [Google Scholar] [CrossRef]
- Yeung, E.Y.H.; Cavanna, A.E. Sleep Attacks in Patients with Parkinson’s Disease on Dopaminergic Medications: A Systematic Review. Mov. Disord. Clin. Pract. 2014, 1, 1307–1316. [Google Scholar] [CrossRef] [Green Version]
- Paus, S.; Brecht, H.M.; Köster, J.; Seeger, G.; Klockgether, T.; Wüllner, U. Sleep attacks, daytime sleepiness, and dopamine agonists in Parkinson’s disease. Mov. Disord. 2003, 18, 659–667. [Google Scholar] [CrossRef]
- Homann, C.N.; Wenzel, K.; Suppan, K.; Ivanic, G.; Kriechbaum, N.; Crevenna, R.; Ott, E. Sleep attacks in patients taking dopamine agonists: Review. BMJ 2002, 324, 1483–1487. [Google Scholar] [CrossRef] [Green Version]
- Sánchez, A.; Blanco, R. Osteonecrosis of the jaw (ONJ) and atypical femoral fracture (AFF) in an osteoporotic patient chronically treated with bisphosphonates. Osteoporos. Int. 2017, 28, 1145–1147. [Google Scholar] [CrossRef] [PubMed]
- Tan, S.H.; Saseendar, S.; Tan, B.H.; Pawaskar, A.; Kumar, V.P. Ulnar fractures with bisphosphonate therapy: A systematic review of published case reports. Osteoporos. Int. 2015, 26, 421–429. [Google Scholar] [CrossRef]
- Abe, K.; Kimura, H.; Yamamoto, N.; Shimozaki, S.; Higuchi, T.; Taniguchi, Y.; Uto, T.; Tsuchiya, H. Treatment strategy for atypical ulnar fracture due to severely suppressed bone turnover caused by long-term bisphosphonate therapy: A case report and literature review. BMC Musculoskelet. Disord. 2020, 21, 802. [Google Scholar] [CrossRef]
- Manolagas, S.C. Corticosteroids and fractures: A close encounter of the third cell kind. J. Bone Miner. Res. 2000, 15, 1001–1005. [Google Scholar] [CrossRef]
- Furuya, M.; Kikuta, J.; Fujimori, S.; Seno, S.; Maeda, H.; Shirazaki, M.; Uenaka, M.; Mizuno, H.; Iwamoto, Y.; Morimoto, A.; et al. Direct cell-cell contact between mature osteoblasts and osteoclasts dynamically controls their functions in vivo. Nat. Commun. 2018, 9, 300. [Google Scholar] [CrossRef]
- Eastell, R.; Adams, J.E.; Coleman, R.E.; Howell, A.; Hannon, R.A.; Cuzick, J.; Mackey, J.R.; Beckmann, M.W.; Clack, G. Effect of anastrozole on bone mineral density: 5-year results from the anastrozole, tamoxifen, alone or in combination trial 18233230. J. Clin. Oncol. 2008, 26, 1051–1057. [Google Scholar] [CrossRef]
- Kang, D.Y.; Park, S.; Rhee, C.W.; Kim, Y.J.; Choi, N.K.; Lee, J.; Park, B.J. Zolpidem use and risk of fracture in elderly insomnia patients. J. Prev. Med. Public Health 2012, 45, 219–226. [Google Scholar] [CrossRef]
- Pharmaceutical and Medical Devices Agency. Available online: https://www.pmda.go.jp/safety/info-services/drugs/adr-info/suspected-adr/0005.html (accessed on 25 January 2021).
- Lumini, A.; Nanni, L. Convolutional Neural Networks for ATC Classification. Curr. Pharm. Des. 2018, 24, 4007–4012. [Google Scholar] [CrossRef] [PubMed]
- MedDRA Japanese Maintenance Organization. Available online: https://www.pmrj.jp/jmo/php/indexj.php (accessed on 25 January 2021).
- Nagai, J.; Uesawa, Y.; Shimamura, R.; Kagaya, H. Characterization of the Adverse Effects Induced by Acetaminophen and Nonsteroidal Anti-Inflammatory Drugs Based on the Analysis of the Japanese Adverse Drug Event Report Database. Clin. J. Pain 2017, 33, 667–675. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Watanabe, H.; Matsushita, Y.; Watanabe, A.; Maeda, T.; Nukui, K.; Ogawa, Y.; Sawa, J.; Maeda, H. Early detection of important safety information. Jpn. J. Biomet. 2004, 25, 37–60. [Google Scholar] [CrossRef]
- Kan, Y.; Nagai, J.; Uesawa, Y. Evaluation of antibiotic-induced taste and smell disorders using the FDA adverse event reporting system database. Sci. Rep. 2021, 11, 9625. [Google Scholar] [CrossRef]
- Chen, J.J.; Wang, S.J.; Tsai, C.A.; Lin, C.J. Selection of differentially expressed genes in microarray data analysis. Pharm. J. 2007, 7, 212–220. [Google Scholar] [CrossRef]
- Kurosaki, K.; Uesawa, Y. Molecular Initiating Events Associated with Drug-Induced Liver Malignant Tumors: An Integrated Study of the FDA Adverse Event Reporting System and Toxicity Predictions. Biomolecules 2021, 11, 944. [Google Scholar] [CrossRef]
- Hosoya, R.; Uesawa, Y.; Ishii-Nozawa, R.; Kagaya, H. Analysis of factors associated with hiccups based on the Japanese Adverse Drug Event Report database. PLoS ONE 2017, 12, e0172057. [Google Scholar] [CrossRef] [Green Version]
- Jolliffe, I.T. Principal Component Analysis, 2nd ed.; Springer: New York, NY, USA, 2002; ISBN 978-0-387-95442-4. [Google Scholar]
- Okunaka, M.; Kano, D.; Matsui, R.; Kawasaki, T.; Uesawa, Y. Comprehensive Analysis of Chemotherapeutic Agents that Induce Infectious Neutropenia. Pharmaceuticals 2021, 14, 681. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Adverse Event | Reporting Times | Reporting Ratio (%) |
|---|---|---|
| Atypical femur fracture | 1653 | 17.3% |
| Fracture | 1550 | 16.3% |
| Femur fracture | 1366 | 14.3% |
| Spinal compression fracture | 1059 | 11.1% |
| Femoral neck fracture | 619 | 6.5% |
| Compression fracture | 355 | 3.7% |
| Rib fracture | 261 | 2.7% |
| Lumbar vertebral fracture | 217 | 2.3% |
| Humerus fracture | 199 | 2.1% |
| Pelvic fracture | 197 | 2.1% |
| Spinal fracture | 142 | 1.5% |
| Pathological fracture | 129 | 1.4% |
| Radius fracture | 128 | 1.3% |
| Foot fracture | 113 | 1.2% |
| Atypical fracture | 111 | 1.2% |
| Upper limb fracture | 106 | 1.1% |
| Jaw fracture | 92 | 1.0% |
| Osteoporotic fracture | 79 | 0.8% |
| Lower limb fracture | 76 | 0.8% |
| Tibia fracture | 76 | 0.8% |
| Cervical vertebral fracture | 74 | 0.8% |
| Ulna fracture | 74 | 0.8% |
| Clavicle fracture | 67 | 0.7% |
| Ankle fracture | 67 | 0.7% |
| Thoracic vertebral fracture | 66 | 0.7% |
| Hip fracture | 64 | 0.7% |
| Facial bones fracture | 60 | 0.6% |
| Multiple fractures | 55 | 0.6% |
| Hand fracture | 50 | 0.5% |
| Wrist fracture | 37 | 0.4% |
| Skull fracture | 37 | 0.4% |
| Stress fracture | 36 | 0.4% |
| Patella fracture | 36 | 0.4% |
| Scapula fracture | 28 | 0.3% |
| Fibula fracture | 28 | 0.3% |
| Traumatic fracture | 27 | 0.3% |
| Ilium fracture | 26 | 0.3% |
| Sternal fracture | 22 | 0.2% |
| Fractured sacrum | 18 | 0.2% |
| Avulsion fracture | 16 | 0.2% |
| Skull fractured base | 14 | 0.1% |
| Comminuted fracture | 13 | 0.1% |
| Fracture delayed union | 12 | 0.1% |
| Forearm fracture | 11 | 0.1% |
| Fracture nonunion | 9 | 0.1% |
| Fracture pain | 8 | 0.1% |
| Limb fracture | 8 | 0.1% |
| Complicated fracture | 8 | 0.1% |
| Open reduction of fracture | 6 | 0.1% |
| Periprosthetic fracture | 6 | 0.1% |
| Lisfranc fracture | 5 | 0.1% |
| Internal fixation of fracture | 4 | <0.1% |
| Open fracture | 3 | <0.1% |
| Fractured coccyx | 3 | <0.1% |
| Acetabulum fracture | 2 | <0.1% |
| Epiphyseal fracture | 1 | <0.1% |
| Sacroiliac fracture | 1 | <0.1% |
| Fractured skull depressed | 1 | <0.1% |
| Patient Characteristics | Drug-Induced Fracture (9531) | Non–Drug-Induced Fracture (1,675,323) | p-Value |
|---|---|---|---|
| Sex # (male; female) | 2530; 6533 (9063) | 837,777; 785,685 (1,623,462) | <0.001 ### |
| Age † | 69.1 ± 17.4 (8239) | 59.5 ± 21.5 (1,565,208) | <0.001 *** |
| Height (cm) † | 154.0 ± 12.6 (2369) | 157.2 ± 18.3 (703,033) | <0.001 *** |
| Weight (kg) † | 52.1 ± 13.7 (2721) | 54.5 ± 16.3 (821,264) | <0.001 *** |
| BMI † | 22.2 ± 4.5 (2286) | 21.9 ± 4.5 (680,578) | 0.010 ** |
| Risk Factor | Drug Class | Odds Ratio | 95% Confidence Interval | p-Value |
|---|---|---|---|---|
| etidronic acid | drugs affecting bone structure and mineralization | 189.01 | 73.21–487.95 | <0.001 ** |
| trientine | other alimentary tract and metabolism products | 164.48 | 19.57–1382.36 | <0.001 ** |
| dolutegravir | direct acting antivirals | 151.14 | 63.90–357.50 | <0.001 ** |
| abacavir | direct acting antivirals | 123.71 | 37.41–409.03 | <0.001 ** |
| prednisolone sodium phosphate | corticosteroids | 106.92 | 12.67–902.28 | <0.001 ** |
| alendronic acid | drugs affecting bone structure and mineralization | 78.13 | 66.18–92.25 | <0.001 ** |
| adefovir dipivoxil | direct acting antivirals | 71.83 | 51.25–100.68 | <0.001 ** |
| laninamivir | direct acting antivirals | 63.91 | 33.37–122.41 | <0.001 ** |
| abacavir sulfate and lamivudine | direct acting antivirals | 60.8 | 18.93–195.25 | <0.001 ** |
| minodronic acid hydrate | drugs affecting bone structure and mineralization | 59.15 | 44.62–78.41 | <0.001 ** |
| risedronic acid | drugs affecting bone structure and mineralization | 59.14 | 46.46–75.29 | <0.001 ** |
| radium (223Ra) dichloride | other therapeutic radiopharmaceuticals | 53.77 | 31.62–91.44 | <0.001 ** |
| cepharanthine | isoquinoline alkaloids | 51.53 | 12.01–221.06 | <0.001 ** |
| tetrabenazine | other nervous system drugs | 45.02 | 21.90–92.55 | <0.001 ** |
| denosumab | drugs affecting bone structure and mineralization | 44.12 | 35.96–54.14 | <0.001 ** |
| L-aspartate potassium | potassium | 40.9 | 17.75–94.25 | <0.001 ** |
| nafarelin | hypothalamic hormones | 36.81 | 4.90–276.58 | 0.001 * |
| ropinirole | dopaminergic agents | 33.28 | 14.49–76.42 | <0.001 ** |
| lamivudine | direct acting antivirals | 33.03 | 18.86–57.86 | <0.001 ** |
| ibandronic acid | drugs affecting bone structure and mineralization | 32.76 | 20.59–52.12 | <0.001 ** |
| clostridium butyricum | antidiarrheal microorganisms | 30.21 | 14.05–64.95 | <0.001 ** |
| interferon beta-1a | immunostimulants | 30.19 | 4.07–224.02 | 0.001 * |
| anastrozole | hormone antagonists and related agents | 29.22 | 17.50–48.77 | <0.001 ** |
| trelagliptin succinate | blood glucose lowering drugs, excl. insulins | 28.21 | 12.31–64.64 | <0.001 ** |
| incadronate disodium hydrate | drugs affecting bone structure and mineralization | 27.8 | 6.63–116.61 | <0.001 ** |
| emtricitabine and tenofovir disoproxil | direct acting antivirals | 26.95 | 3.68–197.42 | 0.001 * |
| teneligliptin and canagliflozin | blood glucose lowering drugs, excl. insulins | 26.36 | 8.25–84.31 | <0.001 ** |
| tafamidis | other nervous system drugs | 24.85 | 7.84–78.76 | <0.001 ** |
| methylphenidate | psychostimulants, agents used for adhd and nootropics | 23.69 | 7.48–74.98 | <0.001 ** |
| zoledronic acid | drugs affecting bone structure and mineralization | 23.67 | 18.27–30.67 | <0.001 ** |
| romosozumab | drugs affecting bone structure and mineralization | 23.64 | 12.80–43.66 | <0.001 ** |
| ritonavir | direct acting antivirals | 22.23 | 3.05–161.95 | 0.002 * |
| calcium L-aspartate hydrate | calcium | 20.87 | 7.60–57.35 | <0.001 ** |
| somatropin | anterior pituitary lobe hormones and analogues | 19.05 | 8.40–43.20 | <0.001 ** |
| pamidronic acid | drugs affecting bone structure and mineralization | 18.98 | 10.05–35.85 | <0.001 ** |
| etelcalcetide | anti-parathyroid agents | 18.95 | 6.98–51.44 | <0.001 ** |
| exemestane | hormone antagonists and related agents | 16.66 | 7.80–35.57 | <0.001 ** |
| memantine | anti-dementia drugs | 16.11 | 9.55–27.17 | <0.001 ** |
| rasagiline | dopaminergic agents | 15.96 | 5.86–43.44 | <0.001 ** |
| leuprorelin | hormones and related agents | 14.94 | 9.43–23.67 | <0.001 ** |
| certolizumab pegol | immunosuppressants | 14.42 | 7.12–29.23 | <0.001 ** |
| tofacitinib | immunosuppressants | 14.09 | 10.43–19.04 | <0.001 ** |
| abiraterone | hormone antagonists and related agents | 14.05 | 7.68–25.71 | <0.001 ** |
| tenofovir alafenamide | direct acting antivirals | 13.95 | 3.43–56.67 | <0.001 ** |
| perampanel | antiepileptics | 13.87 | 3.41–56.45 | <0.001 ** |
| methylprednisolone | corticosteroids | 13.55 | 8.83–20.80 | <0.001 ** |
| teriparatide | parathyroid hormones and analogues | 13.36 | 5.90–30.25 | <0.001 ** |
| goserelin | hormones and related agents | 13.22 | 5.88–29.75 | <0.001 ** |
| paliperidone | antipsychotics | 12.61 | 4.67–34.01 | <0.001 ** |
| entacapone | dopaminergic agents | 12.6 | 4.00–39.70 | <0.001 ** |
| letrozole | hormone antagonists and related agents | 12.43 | 6.38–24.23 | <0.001 ** |
| tramadol | opioids | 12.29 | 6.32–23.91 | <0.001 ** |
| raloxifene | other sex hormones and modulators of the genital system | 11.99 | 6.71–21.41 | <0.001 ** |
| eszopiclone | hypnotics and sedatives | 11.07 | 2.72–45.00 | 0.001 * |
| istradefylline | other antiparkinson drugs | 11 | 2.70–44.75 | 0.001 * |
| fluticasone furoate and vilanterol trifenatate | adrenergics, inhalants | 10.56 | 1.46–76.28 | 0.019 * |
| zopiclone | hypnotics and sedatives | 10.17 | 4.52–22.87 | <0.001 ** |
| aripiprazole hydrate | antipsychotics | 9.89 | 2.44–40.08 | 0.001 * |
| suvorexant | hypnotics and sedatives | 9.75 | 4.01–23.69 | <0.001 ** |
| hydrocortisone | corticosteroids | 8.79 | 2.17–35.60 | 0.002 * |
| levodopa and benserazide hydrochloride | dopaminergic agents | 8.51 | 2.71–26.72 | <0.001 ** |
| pioglitazone | blood glucose lowering drugs, excl. insulins | 8.43 | 5.19–13.70 | <0.001 ** |
| rotigotine | dopaminergic agents | 8.34 | 1.15–60.30 | <0.001 ** |
| alogliptin | blood glucose lowering drugs, excl. insulins | 8.13 | 3.84–17.22 | <0.001 ** |
| golimumab | immunosuppressants | 8.09 | 4.75–13.78 | <0.001 ** |
| prednisolone | corticosteroids | 8.08 | 6.73–9.70 | <0.001 ** |
| pramipexole | dopaminergic agents | 7.93 | 3.27–19.23 | <0.001 ** |
| enzalutamide | hormone antagonists and related agents | 7.64 | 3.78–15.42 | <0.001 ** |
| teriparatide acetate | parathyroid hormones and analogues | 7.64 | 4.18–13.96 | <0.001 ** |
| cinacalcet | anti-parathyroid agents | 6.9 | 2.20–21.63 | 0.001 * |
| buprenorphine | opioids | 6.83 | 1.69–27.64 | 0.007 * |
| salmeterol xinafoate and fluticasone propionate | corticosteroids | 6.64 | 1.65–26.78 | 0.008 * |
| bazedoxifene | other sex hormones and modulators of the genital system | 6.57 | 2.09–20.62 | 0.001 * |
| betamethasone | corticosteroids | 6.46 | 2.67–15.64 | <0.001 ** |
| ledipasvir acetonate and sofosbuvir | direct acting antivirals | 6.41 | 2.86–14.40 | <0.001 ** |
| eldecalcitol | vitamin a and d, incl. combinations of the two | 6.39 | 3.67–11.12 | <0.001 ** |
| galantamine | anti-dementia drugs | 6.36 | 2.83–14.31 | <0.001 ** |
| alprazolam | anxiolytics | 6.24 | 2.32–16.76 | <0.001 ** |
| rivastigmine | anti-dementia drugs | 5.86 | 2.17–15.77 | 0.001 * |
| zolpidem | hypnotics and sedatives | 5.85 | 3.02–11.31 | <0.001 ** |
| urapidil | antiadrenergic agents, peripherally acting | 5.74 | 0.80–41.38 | 0.083 |
| brotizolam | hypnotics and sedatives | 5.67 | 2.68–11.97 | <0.001 ** |
| pregabalin | antiepileptics | 5.55 | 3.85–8.00 | <0.001 ** |
| sofosbuvir | direct acting antivirals | 5 | 2.06–12.09 | <0.001 ** |
| carbidopa hydrate and levodopa | dopaminergic agents | 4.29 | 1.38–13.41 | 0.012 * |
| donepezil | anti-dementia drugs | 4.15 | 1.96–8.77 | <0.001 ** |
| tramadol hydrochloride and acetaminophen | opioids | 3.85 | 1.59–9.31 | 0.003 * |
| mirogabalin besylate | other analgesics and antipyretics | 3.77 | 0.53–27.07 | 0.187 |
| darbepoetin alfa | other antianemic preparations | 3.75 | 1.40–10.04 | 0.009 * |
| alfacalcidol | vitamin a and d, incl. combinations of the two | 3.48 | 1.30–9.34 | 0.013 * |
| duloxetine | antidepressants | 3.09 | 1.28–7.47 | 0.012 * |
| tocilizumab | immunosuppressants | 3.06 | 1.77–5.30 | <0.001 ** |
| methoxy polyethylene glycol-epoetin beta | other antianemic preparations | 2.73 | 0.68–10.98 | 0.157 |
| clozapine | antipsychotics | 2.34 | 0.58–9.41 | 0.23 |
| ramelteon | hypnotics and sedatives | 2.32 | 0.32–16.57 | 0.402 |
| aliskiren | other agents acting on the renin-angiotensin system | 2.28 | 0.32–16.31 | 0.41 |
| paliperidone palmitate | antipsychotics | 2.27 | 0.32–16.17 | 0.414 |
| abatacept | immunosuppressants | 2.25 | 0.72–7.02 | 0.161 |
| quetiapine | antipsychotics | 1.89 | 0.61–5.87 | 0.274 |
| mirabegron | urologicals | 1.64 | 0.23–11.72 | 0.62 |
| etanercept | immunosuppressants | 1.56 | 0.74–3.29 | 0.24 |
| ixazomib | other antineoplastic agents | 1.18 | 0.29–4.72 | 0.818 |
| female | ― | 2.05 | 1.86–2.26 | <0.001 ** |
| Unit Odds Ratio | ||||
| Risk Factor | Odds Ratio | 95% Confidence Interval | p-Value | |
| age | ― | 1.02 | 1.01–1.02 | <0.001 ** |
| BMI | ― | 1.02 | 1.01–1.03 | <0.001 ** |
| Range Odds Ratio | ||||
| Risk Factor | Odds Ratio | 95% Confidence Interval | p-Value | |
| age | ― | 5.59 | 4.21–7.43 | <0.001 ** |
| BMI | ― | 5.49 | 2.64–11.45 | <0.001 ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Toriumi, S.; Kobayashi, A.; Sueki, H.; Yamamoto, M.; Uesawa, Y. Exploring the Mechanisms Underlying Drug-Induced Fractures Using the Japanese Adverse Drug Event Reporting Database. Pharmaceuticals 2021, 14, 1299. https://doi.org/10.3390/ph14121299
Toriumi S, Kobayashi A, Sueki H, Yamamoto M, Uesawa Y. Exploring the Mechanisms Underlying Drug-Induced Fractures Using the Japanese Adverse Drug Event Reporting Database. Pharmaceuticals. 2021; 14(12):1299. https://doi.org/10.3390/ph14121299
Chicago/Turabian StyleToriumi, Shinya, Akinobu Kobayashi, Hitoshi Sueki, Munehiro Yamamoto, and Yoshihiro Uesawa. 2021. "Exploring the Mechanisms Underlying Drug-Induced Fractures Using the Japanese Adverse Drug Event Reporting Database" Pharmaceuticals 14, no. 12: 1299. https://doi.org/10.3390/ph14121299