The Role of Monoclonal Antibodies in the First-Line Treatment of Transplant-Ineligible Patients with Newly Diagnosed Multiple Myeloma

 ,
,
Abstract
:1. Introduction
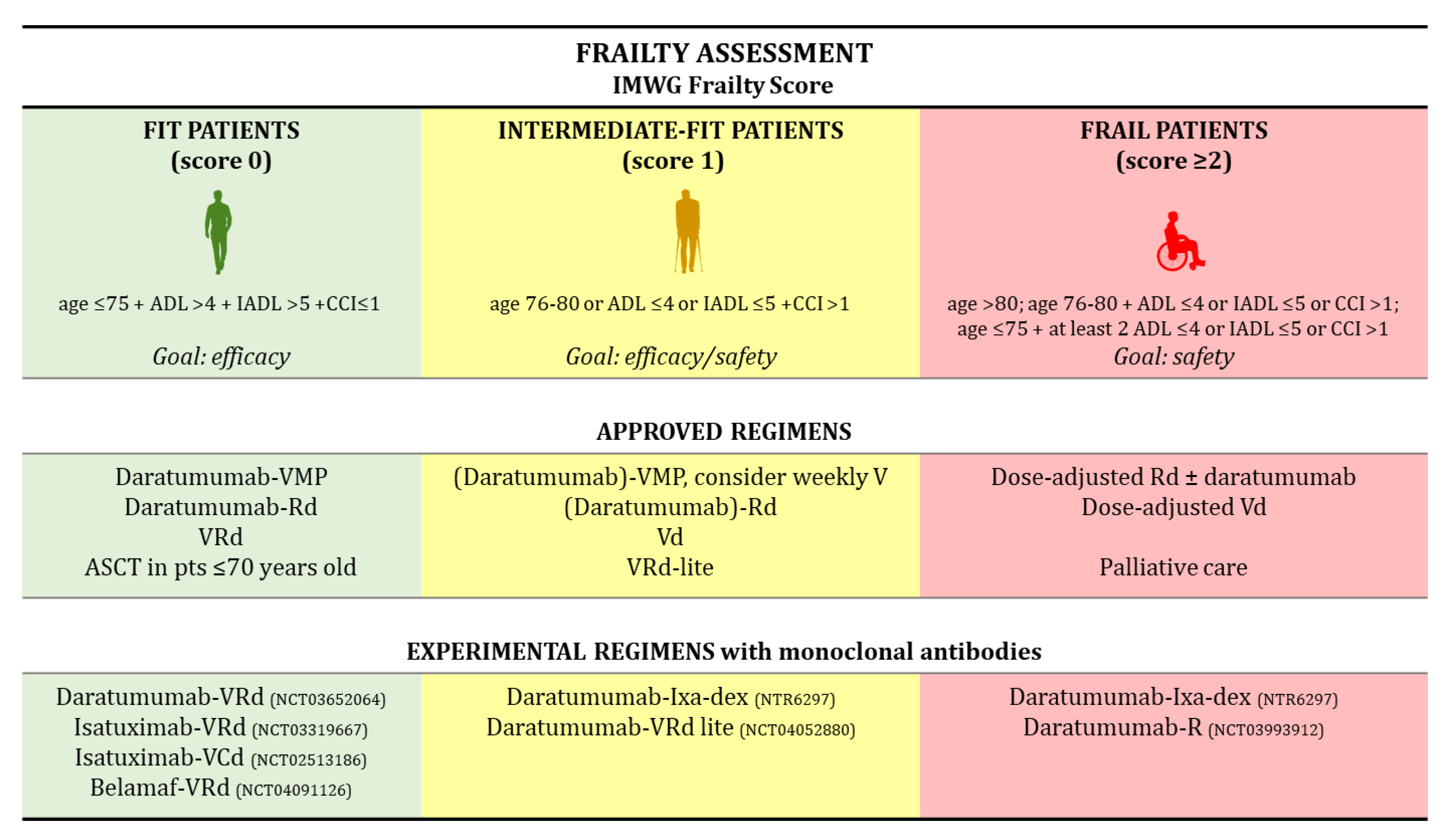
2. How to Choose Therapy in NTE NDMM Patients
3. Monoclonal Antibodies in Elderly Patients: Data about Feasibility
3.1. Data on Relapsed/Refractory (RR)MM Patients
3.2. Data on NDMM Patients
4. Clinical Trials Evaluating MAb-Based Treatments in NTE MM Patients
4.1. New Standards of Care for NTE Patients
4.2. New Combinations under Evaluation in Clinical Trials
4.2.1. Daratumumab-Based Regimens
4.2.2. Isatuximab-Based Regimens
4.2.3. Elotuzumab-Based Regimens
4.2.4. Pembrolizumab-Based Regimens
5. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Kazandjian, D. Multiple myeloma epidemiology and survival: A unique malignancy. Semin. Oncol. 2016, 43, 676–681. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Cancer Institute Surveillance, Epidemiology, and End Results Program. Myeloma—Cancer Stat Facts. Available online: https://seer.cancer.gov/statfacts/html/mulmy.html (accessed on 25 September 2020).
- Moreau, P.; San Miguel, J.; Sonneveld, P.; Mateos, M.V.; Zamagni, E.; Avet-Loiseau, H.; Hajek, R.; Dimopoulos, M.A.; Ludwig, H.; Einsele, H.; et al. Multiple myeloma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2017, 28, iv52–iv61. [Google Scholar] [CrossRef] [PubMed]
- Vaxman, I.; Visram, A.; Kumar, S.; Dispenzieri, A.; Buadi, F.; Dingli, D.; Lacy, M.; Muchtar, E.; Kapoor, P.; Hogan, W.; et al. Autologous stem cell transplantation for multiple myeloma patients aged ≥ 75 treated with novel agents. Bone Marrow Transplant. 2020. [Google Scholar] [CrossRef] [PubMed]
- Munshi, P.N.; Vesole, D.; Jurczyszyn, A.; Zaucha, J.M.; St. Martin, A.; Davila, O.; Agrawal, V.; Badawy, S.M.; Battiwalla, M.; Chhabra, S.; et al. Age no bar: A CIBMTR analysis of elderly patients undergoing autologous hematopoietic cell transplantation for multiple myeloma. Cancer 2020, 126, 5077–5087. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S.K.; Rajkumar, S.V.; Dispenzieri, A.; Lacy, M.Q.; Hayman, S.R.; Buadi, F.K.; Zeldenrust, S.R.; Dingli, D.; Russell, S.J.; Lust, J.A.; et al. Improved survival in multiple myeloma and the impact of novel therapies. Blood 2008, 111, 2516–2520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schaapveld, M.; Visser, O.; Siesling, S.; Schaar, C.G.; Zweegman, S.; Vellenga, E. Improved survival among younger but not among older patients with Multiple Myeloma in the Netherlands, a population-based study since 1989. Eur. J. Cancer 2010, 46, 160–169. [Google Scholar] [CrossRef]
- Turesson, I.; Velez, R.; Kristinsson, S.Y.; Landgren, O. Patterns of improved survival in patients with multiple myeloma in the twenty-first century: A population-based study. J. Clin. Oncol. 2010, 28, 830–834. [Google Scholar] [CrossRef] [Green Version]
- Costa, L.J.; Brill, I.K.; Omel, J.; Godby, K.; Kumar, S.K.; Brown, E.E. Recent trends in multiple myeloma incidence and survival by age, race, and ethnicity in the United States. Blood Adv. 2017, 1, 282–287. [Google Scholar] [CrossRef]
- Nandakumar, B.; Binder, M.; Dispenzieri, A.; Kapoor, P.; Buadi, F.; Gertz, M.A.; Lacy, M.; Dingli, D.; Hwa, L.; Leung, N.; et al. Continued improvement in survival in multiple myeloma (MM) including high-risk patients. J. Clin. Oncol. 2019, 37. Abstract #8039 [ASCO 2019 Meeting]. [Google Scholar] [CrossRef]
- Bonello, F.; Mina, R.; Boccadoro, M.; Gay, F. Therapeutic monoclonal antibodies and antibody products: Current practices and development in multiple myeloma. Cancers 2020, 12, 15. [Google Scholar] [CrossRef] [Green Version]
- D’agostino, M.; Innorcia, S.; Boccadoro, M.; Bringhen, S. Monoclonal antibodies to treat multiple myeloma: A dream come true. Int. J. Mol. Sci. 2020, 21, 8192. [Google Scholar] [CrossRef] [PubMed]
- D’Agostino, M.; Boccadoro, M.; Smith, E.L. Novel immunotherapies for multiple myeloma. Curr. Hematol. Malig. Rep. 2017, 12, 344–357. [Google Scholar] [CrossRef] [PubMed]
- Gay, F.; D’Agostino, M.; Giaccone, L.; Genuardi, M.; Festuccia, M.; Boccadoro, M.; Bruno, B. Immuno-oncologic approaches: CAR-T cells and checkpoint inhibitors. Clin. Lymphoma Myeloma Leuk. 2017, 17, 471–478. [Google Scholar] [CrossRef] [PubMed]
- Mateos, M.V.; Dimopoulos, M.A.; Cavo, M.; Suzuki, K.; Jakubowiak, A.; Knop, S.; Doyen, C.; Lucio, P.; Nagy, Z.; Kaplan, P.; et al. Daratumumab plus bortezomib, melphalan, and prednisone for untreated myeloma. N. Engl. J. Med. 2018, 378, 518–528. [Google Scholar] [CrossRef]
- Facon, T.; Kumar, S.; Plesner, T.; Orlowski, R.Z.; Moreau, P.; Bahlis, N.; Basu, S.; Nahi, H.; Hulin, C.; Quach, H.; et al. Daratumumab plus lenalidomide and dexamethasone for untreated myeloma. N. Engl. J. Med. 2019, 380, 2104–2115. [Google Scholar] [CrossRef]
- Larocca, A.; Dold, S.M.; Zweegman, S.; Terpos, E.; Wäsch, R.; D’Agostino, M.; Scheubeck, S.; Goldschmidt, H.; Gay, F.; Cavo, M.; et al. Patient-centered practice in elderly myeloma patients: An overview and consensus from the European Myeloma Network (EMN). Leukemia 2018, 32, 1697–1712. [Google Scholar] [CrossRef]
- Salvini, M.; D’Agostino, M.; Bonello, F.; Boccadoro, M.; Bringhen, S. Determining treatment intensity in elderly patients with multiple myeloma. Expert Rev. Anticancer Ther. 2018, 18, 917–930. [Google Scholar] [CrossRef]
- Mina, R.; Bringhen, S.; Wildes, T.M.; Zweegman, S.; Rosko, A.E. Approach to the older adult with multiple myeloma. Am. Soc. Clin. Oncol. Educ. B. 2019, 39, 500–518. [Google Scholar] [CrossRef]
- Clegg, A.; Young, J.; Iliffe, S.; Rikkert, M.O.; Rockwood, K. Frailty in elderly people. Lancet 2013, 381, 752–762. [Google Scholar] [CrossRef] [Green Version]
- Pawlyn, C.; Cairns, D.; Kaiser, M.; Striha, A.; Jones, J.; Shah, V.; Jenner, M.; Drayson, M.; Owen, R.; Gregory, W.; et al. The relative importance of factors predicting outcome for myeloma patients at different ages: Results from 3894 patients in the Myeloma XI trial. Leukemia 2020, 34, 604–612. [Google Scholar] [CrossRef] [Green Version]
- Cook, G.; Larocca, A.; Facon, T.; Zweegman, S.; Engelhardt, M. Defining the vulnerable patient with myeloma—a frailty position paper of the European Myeloma Network. Leukemia 2020, 34, 2285–2294. [Google Scholar] [CrossRef] [PubMed]
- Palumbo, A.; Bringhen, S.; Mateos, M.-V.; Larocca, A.; Facon, T.; Kumar, S.; Offidani, M.; McCarthy, P.; Evangelista, A.; Lonial, S.; et al. Geriatric assessment predicts survival and toxicities in elderly myeloma patients: An International Myeloma Working Group report. Blood 2015, 125, 2068–2074. [Google Scholar] [CrossRef]
- Facon, T.; Dimopoulos, M.A.; Meuleman, N.; Belch, A.; Mohty, M.; Chen, W.M.; Kim, K.; Zamagni, E.; Rodriguez-Otero, P.; Renwick, W.; et al. A simplified frailty scale predicts outcomes in transplant-ineligible patients with newly diagnosed multiple myeloma treated in the FIRST (MM-020) trial. Leukemia 2020, 34, 224–233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cook, G.; Royle, K.L.; Pawlyn, C.; Hockaday, A.; Shah, V.; Kaiser, M.F.; Brown, S.R.; Gregory, W.M.; Child, J.A.; Davies, F.E.; et al. A clinical prediction model for outcome and therapy delivery in transplant-ineligible patients with myeloma (UK Myeloma Research Alliance Risk Profile): A development and validation study. Lancet Haematol. 2019, 6, e154–e166. [Google Scholar] [CrossRef] [Green Version]
- Bringhen, S.; D’Agostino, M.; Paris, L.; Ballanti, S.; Pescosta, N.; Spada, S.; Pezzatti, S.; Grasso, M.; Rota-Scalabrini, D.; de Rosa, L.; et al. Lenalidomide-based induction and maintenance in elderly newly diagnosed multiple myeloma patients: Updated results of the EMN01 randomized trial. Haematologica 2020, 105, 1937–1947. [Google Scholar] [CrossRef] [Green Version]
- Bonello, F.; Boccadoro, M.; Larocca, A. Diagnostic and therapeutic challenges in the management of intermediate and frail elderly multiple myeloma patients. Cancers 2020, 12, 3106. [Google Scholar] [CrossRef]
- Stege, C.A.M.; Nasserinejad, K.; van der Spek, E.; Van Kampen, R.J.W.; Sohne, M.; Thielen, N.; Bilgin, Y.; De Waal, E.G.M.; Ludwig, I.; Leijs, M.B.L.; et al. Efficacy and tolerability of ixazomib, daratumumab and low dose dexamethasone (ixa dara dex) in unfit and frail newly diagnosed multiple myeloma (NDMM) patients; Results of the interim efficacy analysis of the phase II HOVON 143 study. Blood 2019, 134. Abstract #695 [ASH 2019 61st Meeting]. [Google Scholar] [CrossRef]
- Mateos, M.-V.; Spencer, A.; Nooka, A.K.; Pour, L.; Weisel, K.; Cavo, M.; Laubach, J.P.; Cook, G.; Iida, S.; Benboubker, L.; et al. Daratumumab-based regimens are highly effective and well tolerated in relapsed or refractory multiple myeloma regardless of patient age: Subgroup analysis of the phase 3 CASTOR and POLLUX studies. Haematologica 2020, 105, 468–477. [Google Scholar] [CrossRef] [Green Version]
- Schjesvold, F.H.; Richardson, P.G.; Facon, T.; Alegre, A.; Spencer, A.; Jurczyszyn, A.; Sunami, K.; Frenzel, L.; Min, C.-K.; Guillonneau, S.; et al. Isatuximab plus pomalidomide and dexamethasone in elderly patients with relapsed/refractory multiple myeloma: ICARIA-MM subgroup analysis. Haematologica 2020. [Google Scholar] [CrossRef]
- San-Miguel, J.; Iida, S.; Blade, J.; Mateos, M.-V.; Lee, J.-J.; Garg, M.; Hungria, V.; Beksac, M.; Spicka, I.; Knop, S.; et al. Daratumumab plus bortezomib-melphalan-prednisone (VMP) in elderly (≥75 years of age) patients with newly diagnosed multiple myeloma ineligible for transplantation (ALCYONE). HemaSpehere 2018, 2, 5, [Abstract #S107-EHA 2018 23rd Congress]. [Google Scholar]
- Usmani, S.Z.; Facon, T.; Kumar, S.; Plesner, T.; Moreau, P.; Basu, S.; Nahi, H.; Macro, M.; Quach, H.; Perrot, A.; et al. Impact of age on efficacy and safety of daratumumab in combination with lenalidomide and dexamethasone (D-Rd) in patients (pts) with transplant-ineligible newly diagnosed multiple myeloma (NDMM): MAIA. J. Clin. Oncol. 2019, 37. Abstract #8035 [ASCO 2019 Annual Meeting]. [Google Scholar] [CrossRef]
- Takamatsu, H.; Iida, S.; Shibayama, H.; Shibayama, K.; Yamazaki, H.; Suzuki, K. Daratumumab, lenalidomide, and dexamethasone in Japanese patients with transplant-ineligible newly diagnosed multiple myeloma: A phase 1b study. Int. J. Hematol. 2020, 111, 692–701. [Google Scholar] [CrossRef] [PubMed]
- Fujisaki, T.; Ishikawa, T.; Takamatsu, H.; Suzuki, K.; Min, C.K.; Lee, J.H.; Wang, J.; Carson, R.; Crist, W.; Qi, M.; et al. Daratumumab plus bortezomib, melphalan, and prednisone in East Asian patients with non-transplant multiple myeloma: Subanalysis of the randomized phase 3 ALCYONE trial. Ann. Hematol. 2019, 98, 2805–2814. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lonial, S.; Dimopoulos, M.; Palumbo, A.; White, D.; Grosicki, S.; Spicka, I.; Walter-Croneck, A.; Moreau, P.; Mateos, M.-V.; Magen, H.; et al. Elotuzumab therapy for relapsed or refractory multiple myeloma. N. Engl. J. Med. 2015, 373, 621–631. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trudel, S.; Moreau, P.; Touzeau, C. Update on elotuzumab for the treatment of relapsed/refractory multiple myeloma: Patients’ selection and perspective. Onco. Targets. Ther. 2019, 12, 5813–5822. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kubo, K.; Hori, M.; Ohta, K.; Handa, H.; Hatake, K.; Matsumoto, M.; Hagiwara, S.; Ohashi, K.; Nakaseko, C.; Suzuki, K.; et al. Elotuzumab plus lenalidomide and dexamethasone for newly diagnosed multiple myeloma: A randomized, open-label, phase 2 study in Japan. Int. J. Hematol. 2020, 111, 65–74. [Google Scholar] [CrossRef]
- Mateos, M.V.; Cavo, M.; Blade, J.; Dimopoulos, M.A.; Suzuki, K.; Jakubowiak, A.; Knop, S.; Doyen, C.; Lucio, P.; Nagy, Z.; et al. Overall survival with daratumumab, bortezomib, melphalan, and prednisone in newly diagnosed multiple myeloma (ALCYONE): A randomised, open-label, phase 3 trial. Lancet 2020, 395, 132–141. [Google Scholar] [CrossRef]
- Bahlis, N.; Facon, T.; Usmani, S.Z.; Kumar, S.K.; Plesner, T.; Orlowski, R.Z.; Touzeau, C.; Basu, S.; Nahi, H.; Hulin, C.; et al. daratumumab plus lenalidomide and dexamethasone (D-Rd) Versus lenalidomide and dexamethasone (Rd) in patients with newly diagnosed multiple myeloma (NDMM) ineligible for transplant: Updated analysis of maia. Blood 2019, 134. Abstract #1875 [ASH 2019 61st Meeting]. [Google Scholar] [CrossRef]
- Usmani, S.Z.; Ailawadhi, S.; Sexton, R.; Hoering, A.; Lipe, B.; Hita, S.; Durie, B.G.; Zonder, J.A.; Dhodapkar, M.V.; Callander, N.S.; et al. Primary analysis of the randomized phase II trial of bortezomib, lenalidomide, dexamthasone with/without elotuzumab for newly diagnosed, high-risk multiple myeloma (SWOG-1211). J. Clin. Oncol. 2020, 38. Abstract #8507 [ASCO 2020 Annual Meeting]. [Google Scholar] [CrossRef]
- Ocio, E.M.; Rodriguez Otero, P.; Bringhen, S.; Oliva, S.; Nogai, A.; Attal, M.; Moreau, P.; Kanagavel, D.; Fitzmaurice, T.F.; Wu, J.; et al. Preliminary results from a phase I study of isatuximab (ISA) in combination with bortezomib, lenalidomide, dexamethasone (VRd), and in patients with newly diagnosed multiple myeloma (NDMM) non-eligible for transplant. Blood 2018, 132. Abstract #595 [ASH 2018 60th Meeting]. [Google Scholar] [CrossRef]
- Ocio, E.M.; Bringhen, S.; Oliva, S.; Rodriguez-Otero, P.; Kanagavel, D.; Oprea, C.; Wei, V.; Doroumian, S.; Martinez-Lopez, J. A Phase Ib study of isatuximab in combination with bortezomib, cyclophosphamide, and dexamethasone (VCDI) in patients with newly diagnosed multiple myeloma non-eligible for transplantation. Blood 2017, 130. Abstract #3160 [ASH 2017 59th Annual Meeting]. [Google Scholar] [CrossRef]
- Ocio, E.M.; Rodríguez Otero, P.; Bringhen, S.; Oliva, S.; Nogai, A.; Attal, M.; Moreau, P.; Martinez-Lopez, J.; Le Roux, N.; Macé, S.; et al. Updates from a phase Ib study of isatuximab (Isa), bortezomib (V) and dexamethasone (D) plus cyclophosphamide (C) or lenalidomide (R) in transplant-ineligible, newly diagnosed multiple myeloma (NDMM). J. Clin. Oncol. 2020, 38. Abstract #8529 [ASCO 2020 Annual Meeting]. [Google Scholar] [CrossRef]
- Durie, B.G.M.; Kumar, S.K.; Usmani, S.Z.; Nonyane, B.A.S.; Ammann, E.M.; Lam, A.; Kobos, R.; Maiese, E.M.; Facon, T. Daratumumab-lenalidomide-dexamethasone vs standard-of-care regimens: Efficacy in transplant-ineligible untreated myeloma. Am. J. Hematol. 2020, 95, 1486–1494. [Google Scholar] [CrossRef] [PubMed]
- Bristol-Myers Squibb Company Press Release. Bristol Myers Squibb Reports Primary Results of ELOQUENT-1 Study Evaluating Empliciti (elotuzumab) Plus Revlimid (lenalidomide) and Dexamethasone in Patients with Newly Diagnosed, Untreated Multiple Myeloma. Available online: https://news.bms.com/press-release/corporatefinancial-news/bristol-myers-squibb-reports-primary-results-eloquent-1-study- (accessed on 29 July 2020).
- Chari, A.; Martinez-Lopez, J.; Mateos, M.-V.; Bladé, J.; Benboubker, L.; Oriol, A.; Arnulf, B.; Rodriguez-Otero, P.; Pineiro, L.; Jakubowiak, A.; et al. Daratumumab plus carfilzomib and dexamethasone in patients with relapsed or refractory multiple myeloma. Blood 2019, 134, 421–431. [Google Scholar] [CrossRef] [Green Version]
- Xu, X.S.; Moreau, P.; Usmani, S.Z.; Lonial, S.; Jakubowiak, A.; Oriol, A.; Krishnan, A.; Bladé, J.; Luo, M.; Sun, Y.N.; et al. Split first dose administration of intravenous daratumumab for the treatment of multiple myeloma (MM): Clinical and population pharmacokinetic analyses. Adv. Ther. 2020, 37, 1464–1478. [Google Scholar] [CrossRef] [Green Version]
- Weisel, K.; Asemissen, A.M.; Schieferdecker, A.; Besemer, B.; Zago, M.; Mann, C.; Lutz, R.; Benner, A.; Tichy, D.; Bokemeyer, C.; et al. Isatuximab, Carfilzomib, Lenalidomide and Dexamethasone (I-KRd) in front-line treatment of high-risk Multiple Myeloma: Results of the Safety Run-In cohort in the phase II, multicenter GMMG-CONCEPT trial. Clin. Lymphoma Myeloma Leuk. 2019, 19, e17, [Abstract #OAB–023, 17th IMW 2019]. [Google Scholar] [CrossRef]
- Weisel, K.; Asemissen, A.M.; Besemer, B.; Haenel, M.; Blau, I.W.; Goerner, M.; Ko, Y.-D.; Dürig, J.; Staib, P.; Mann, C.; et al. Depth of response to isatuximab, carfilzomib, lenalidomide, and dexamethasone (Isa-KRd) in front-line treatment of high-risk multiple myeloma: Interim analysis of the GMMG-CONCEPT trial. J. Clin. Oncol. 2020, 38. Abstract #8508 [ASCO 2020 Annual Meeting]. [Google Scholar] [CrossRef]
- Mateos, M.V.; Orlowski, R.Z.; Ocio, E.M.; Rodríguez-Otero, P.; Reece, D.; Moreau, P.; Munshi, N.; Avigan, D.E.; Siegel, D.S.; Ghori, R.; et al. Pembrolizumab combined with lenalidomide and low-dose dexamethasone for relapsed or refractory multiple myeloma: Phase I KEYNOTE-023 study. Br. J. Haematol. 2019, 186, e117–e121. [Google Scholar] [CrossRef] [Green Version]
- Badros, A.; Hyjek, E.; Ma, N.; Lesokhin, A.; Dogan, A.; Rapoport, A.P.; Kocoglu, M.; Lederer, E.; Philip, S.; Milliron, T.; et al. Pembrolizumab, pomalidomide, and low-dose dexamethasone for relapsed/refractory multiple myeloma. Blood 2017, 130, 1189–1197. [Google Scholar] [CrossRef] [Green Version]
- Usmani, S.Z.; Schjesvold, F.; Oriol, A.; Karlin, L.; Cavo, M.; Rifkin, R.M.; Yimer, H.A.; LeBlanc, R.; Takezako, N.; McCroskey, R.D.; et al. Pembrolizumab plus lenalidomide and dexamethasone for patients with treatment-naive multiple myeloma (KEYNOTE-185): A randomised, open-label, phase 3 trial. Lancet Haematol. 2019, 6, e448–e458. [Google Scholar] [CrossRef]
- Larocca, A.; Salvini, M.; De Paoli, L.; Cascavilla, N.; Benevolo, G.; Galli, M.; Montefusco, V.; di Toritto, T.C.; Baraldi, A.; Spada, S.; et al. Efficacy and feasibility of dose/schedule-adjusted Rd-R vs. continuous Rd in elderly and intermediate-fit newly diagnosed multiple myeloma (NDMM) patients: RV-MM-PI-0752 phase III randomized study. Blood 2018, 132. Abstract #305 [ASH 2018 60th Meeting]. [Google Scholar] [CrossRef]
- Barr, H.; Dempsey, J.; Waller, A.; Huang, Y.; Williams, N.; Sharma, N.; Benson, D.M.; Rosko, A.E.; Efebera, Y.A.; Hofmeister, C.C. Ninety-minute daratumumab infusion is safe in multiple myeloma. Leukemia 2018, 32, 2495–2518. [Google Scholar] [CrossRef] [PubMed]
- Mateos, M.V.; Nahi, H.; Legiec, W.; Grosicki, S.; Vorobyev, V.; Spicka, I.; Hungria, V.; Korenkova, S.; Bahlis, N.; Flogegard, M.; et al. Subcutaneous versus intravenous daratumumab in patients with relapsed or refractory multiple myeloma (COLUMBA): A multicentre, open-label, non-inferiority, randomised, phase 3 trial. Lancet Haematol. 2020, 7, e370–e380. [Google Scholar] [CrossRef]
- Usmani, S.Z.; Nahi, H.; Mateos, M.V.; van de Donk, N.W.C.J.; Chari, A.; Kaufman, J.L.; Moreau, P.; Oriol, A.; Plesner, T.; Benboubker, L.; et al. Subcutaneous delivery of daratumumab in relapsed or refractory multiple myeloma. Blood 2019, 134, 668–677. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mian, H.S.; Fiala, M.A.; Wildes, T.M. Burden of treatment among older adults with newly diagnosed multiple myeloma. Clin. Lymphoma Myeloma Leuk. 2020. [Google Scholar] [CrossRef]
- Drayson, M.T.; Bowcock, S.; Planche, T.; Iqbal, G.; Pratt, G.; Yong, K.; Wood, J.; Raynes, K.; Higgins, H.; Dawkins, B.; et al. Levofloxacin prophylaxis in patients with newly diagnosed myeloma (TEAMM): A multicentre, double-blind, placebo-controlled, randomised, phase 3 trial. Lancet Oncol. 2019, 20, 1760–1772. [Google Scholar] [CrossRef] [Green Version]
- Lonial, S.; Lee, H.C.; Badros, A.; Trudel, S.; Nooka, A.K.; Chari, A.; Abdallah, A.O.; Callander, N.; Lendvai, N.; Sborov, D.; et al. Belantamab mafodotin for relapsed or refractory multiple myeloma (DREAMM-2): A two-arm, randomised, open-label, phase 2 study. Lancet Oncol. 2020, 21, 207–221. [Google Scholar] [CrossRef]


{kind=link}
| a. Efficacy | |||||||
| Trial | N pts | Treatment | OR (%) | CR/VGPR (%) | MRD neg (%) | mPFS [95% CI] (Months) | mOS [95% CI] (Months) |
| ALCYONE [38] | 706 | Dara-VMP | 90.9 | 43/71 | 28 | 36.4 | 78.0 |
| vs. | vs. | vs. | vs. | vs. | vs. | ||
| VMP | 73.9 | 25/50 | 7 | 19.3 | 67.9 | ||
| MAIA [16,39] | 737 | Dara-Rd | 93 | 50/81 | 24.2 | NR | NR |
| vs. | vs. | vs. | vs. | vs. | vs. | ||
| Rd | 82 | 27/55 | 7.3 | 33.8 | NR | ||
| HOVON 143 [28] | 46 | Dara-Ixa-dex | - | 9-month PFS rates: | 9-month OS rates: | ||
| interm.-fit | 87 | 0/39 | 78 (55–90) | 100 | |||
| vs. | vs. | vs. | vs. | vs. | |||
| frail pts | 78 | 4/26 | 61 (38–77) | 83 (60–93) | |||
| SWOG-1211 [40] | 103 | Elo-VRd | - | - | - | 31 | 68 |
| vs. | vs. | vs. | |||||
| VRd | 34 | NR | |||||
| TCD13983 [41,42,43] | 44 | Isa-VRd | 100 | 41/52 | 30.8 | NR | - |
| vs. | vs. | vs. | vs. | vs. | |||
| Isa-VCd | 93.3 | 59 | 33.3 | NR | |||
| b. Safety | |||||||
| Trial | N pts | Treatment | Total Discontinuation (%) | Discontinuation due to AE (%) | Discontinuation due to Death (%) | Grade 3–4 Hematologic Toxicities: Neutropenia/Anemia (%) | Grade 3–4 Non-Hematologic Toxicities: Infections (%) |
| ALCYONE [38] | 706 | Dara-VMP | - | 7 | 24 | 40/15 | 22 |
| vs. | vs. | vs. | vs. | vs. | |||
| VMP | 9 | 36 | 39/20 | 15 | |||
| MAIA [16,39] | 737 | Dara-Rd | 39 | 9 | 23 | 51/14 | 36 |
| vs. | vs. | vs. | vs. | vs. | vs. | ||
| Rd | 64 | 18 | 28 | 35.3/21 | 27 | ||
| HOVON 143 [28] | 46 | Dara-Ixa-dex | |||||
| Interm.-fit | 30 | 4 | 0 | 8/- | 9 | ||
| vs. | vs. | vs. | vs. | vs. | vs. | ||
| frail pts | 39 | 0 | 13 | 17/- | 9 | ||
| SWOG-1211 [40] | 103 | Elo-VRd | - | - | - | - | 16 |
| vs. | vs. | ||||||
| VRd | 8 | ||||||
| TCD13983 [41,42,43] | 22 | Isa-VRd | 14 | 9 | 5 | 12.5% | 27 |
| Drug Class | Concerns in Elderly Patients | Opportunities in Elderly Patients | Possible Future Directions |
|---|---|---|---|
| Anti-CD38 mAbs | IRRs, slight increase of infection risk | Synergy with other MM backbone treatments, easy to combine | Part of standard-of-care regimens for virtually all NTE NDMM patients? |
| Anti-SLAMF7 mAbs | Low efficacy | Very good safety, easy to combine | Exploration of their use in new combination therapies? With other immune therapies? |
| Checkpoint inhibitors | immune-mediated AEs, infections | Possible synergy with IMiD-based backbones | Suboptimal as compared with available alternatives. |
| ADCs | Corneal events | High efficacy as single agent, feasible combination with other MM backbone treatments | Exploration of their use in combination with other backbone MM treatments? |
| BiAbs | CRS, neurotoxicity, infections | Very high efficacy as single agent | Consolidation therapy in fit, MRD-positive, NTE NDMM patients? |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bonello, F.; Grasso, M.; D’Agostino, M.; Celeghini, I.; Castellino, A.; Boccadoro, M.; Bringhen, S. The Role of Monoclonal Antibodies in the First-Line Treatment of Transplant-Ineligible Patients with Newly Diagnosed Multiple Myeloma. Pharmaceuticals 2021, 14, 20. https://doi.org/10.3390/ph14010020
Bonello F, Grasso M, D’Agostino M, Celeghini I, Castellino A, Boccadoro M, Bringhen S. The Role of Monoclonal Antibodies in the First-Line Treatment of Transplant-Ineligible Patients with Newly Diagnosed Multiple Myeloma. Pharmaceuticals. 2021; 14(1):20. https://doi.org/10.3390/ph14010020
Chicago/Turabian StyleBonello, Francesca, Mariella Grasso, Mattia D’Agostino, Ivana Celeghini, Alessia Castellino, Mario Boccadoro, and Sara Bringhen. 2021. "The Role of Monoclonal Antibodies in the First-Line Treatment of Transplant-Ineligible Patients with Newly Diagnosed Multiple Myeloma" Pharmaceuticals 14, no. 1: 20. https://doi.org/10.3390/ph14010020