
Epidemiological Trends of Trans-Boundary Tick-Borne Encephalitis in Europe, 2000–2019

 , , ,
, , ,
Abstract
:1. Introduction
2. Factors Affecting TBEV Transmission
3. Migration of TBE Subtypes

{kind=link}
{kind=link}
{kind=link}
| Year | Country | Altitude (Meters above Sea Level) | Conditions |
|---|---|---|---|
| 1950 | Bosnia Herzegovina | <800 | [49] |
| 1957 | Scotland | 700 | [49] |
| 1960 | Bosnia Herzegovina | 900 | [48,49] |
| 1980 | Czech Republic | 700–750 | Krkonose mountainous area [50] |
| 1997 | Italy | <1300 | Presence of limestone and vegetation cover with thermophile deciduous forests and high densities of roe deer [51] |
| 1990s | Scotland | ≥700 | [49,52] |
| 2001 | Scotland | 1100 | [49,52] |
| 2002 | Czech Republic | 1180 | Krkonose mountainous area [50] |
| 2006 | Czech Republic | 1250 | Krkonose mountainous area [50] |
| 2008 | Austria | >1500 | Alpine pasture [53] |
| 2008 | Greece | >600 | Arid parts of Europe typical of the Mediterranean |
| 2010 | Bosnia Herzegovina | 1190 | [49] |
| 2013 | Spain | 2000 | Atlantic influence (i.e., greater humidity) [49] |
| Switzerland | 1450 | Mountainside [49] |
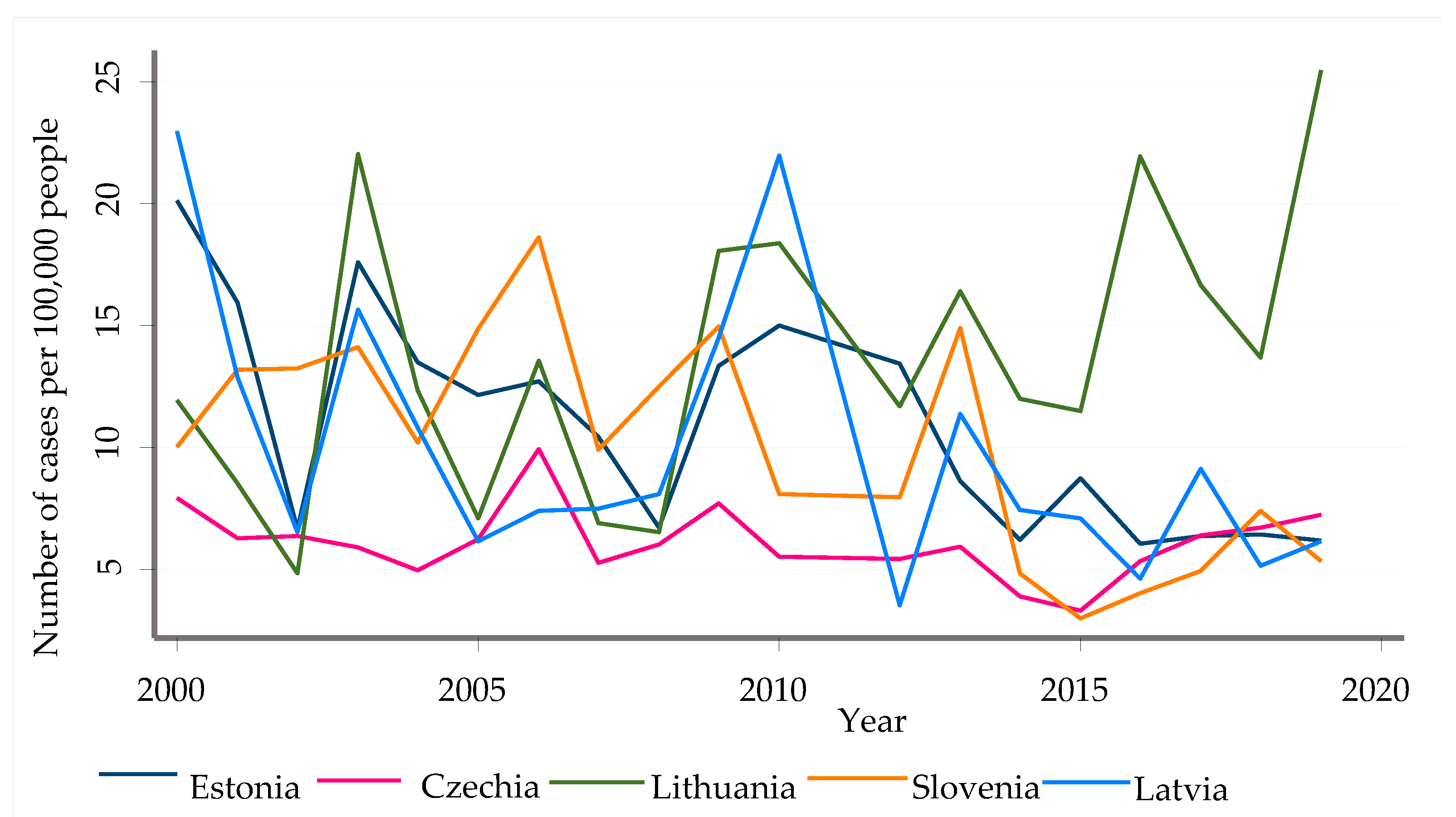
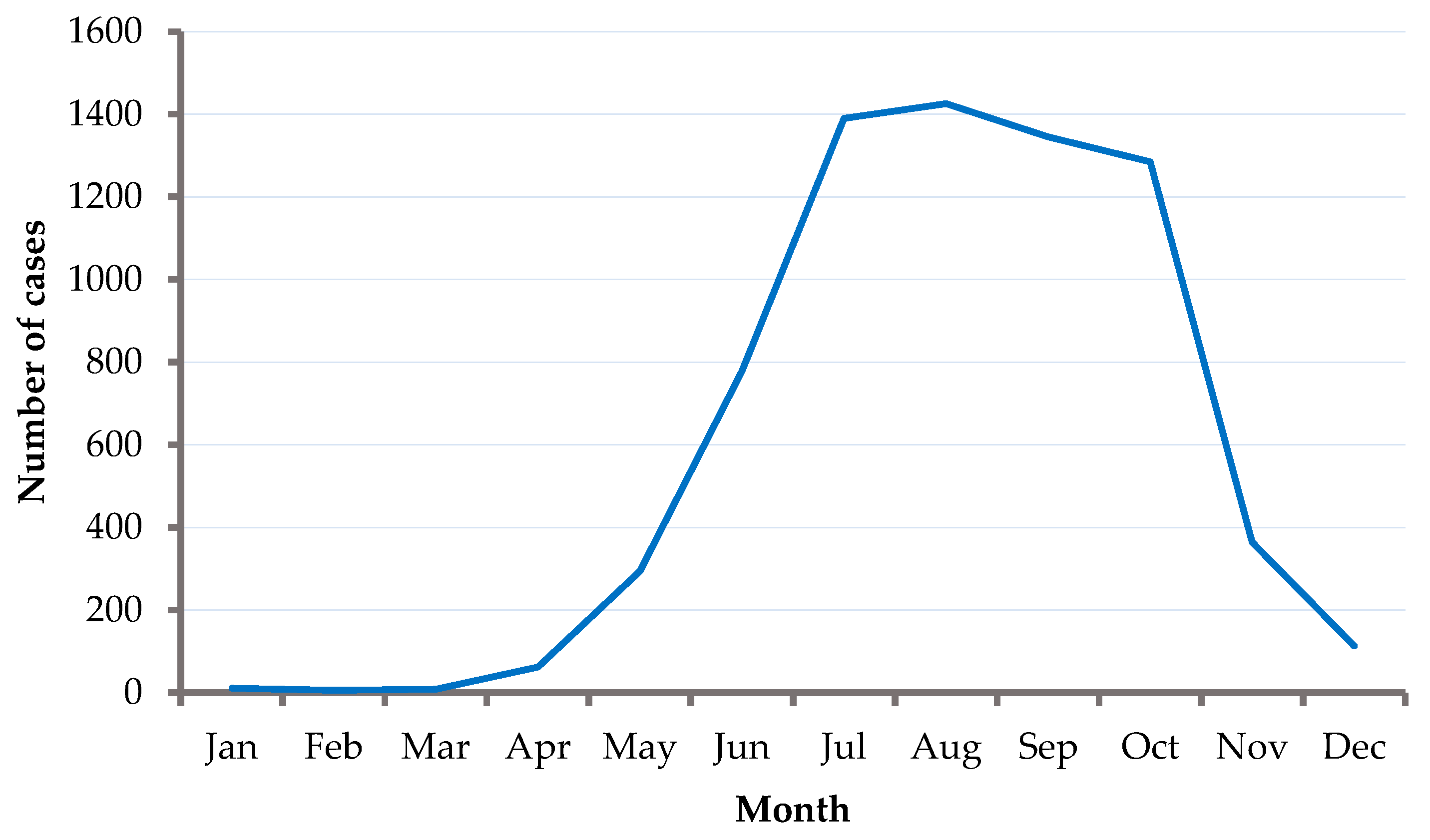
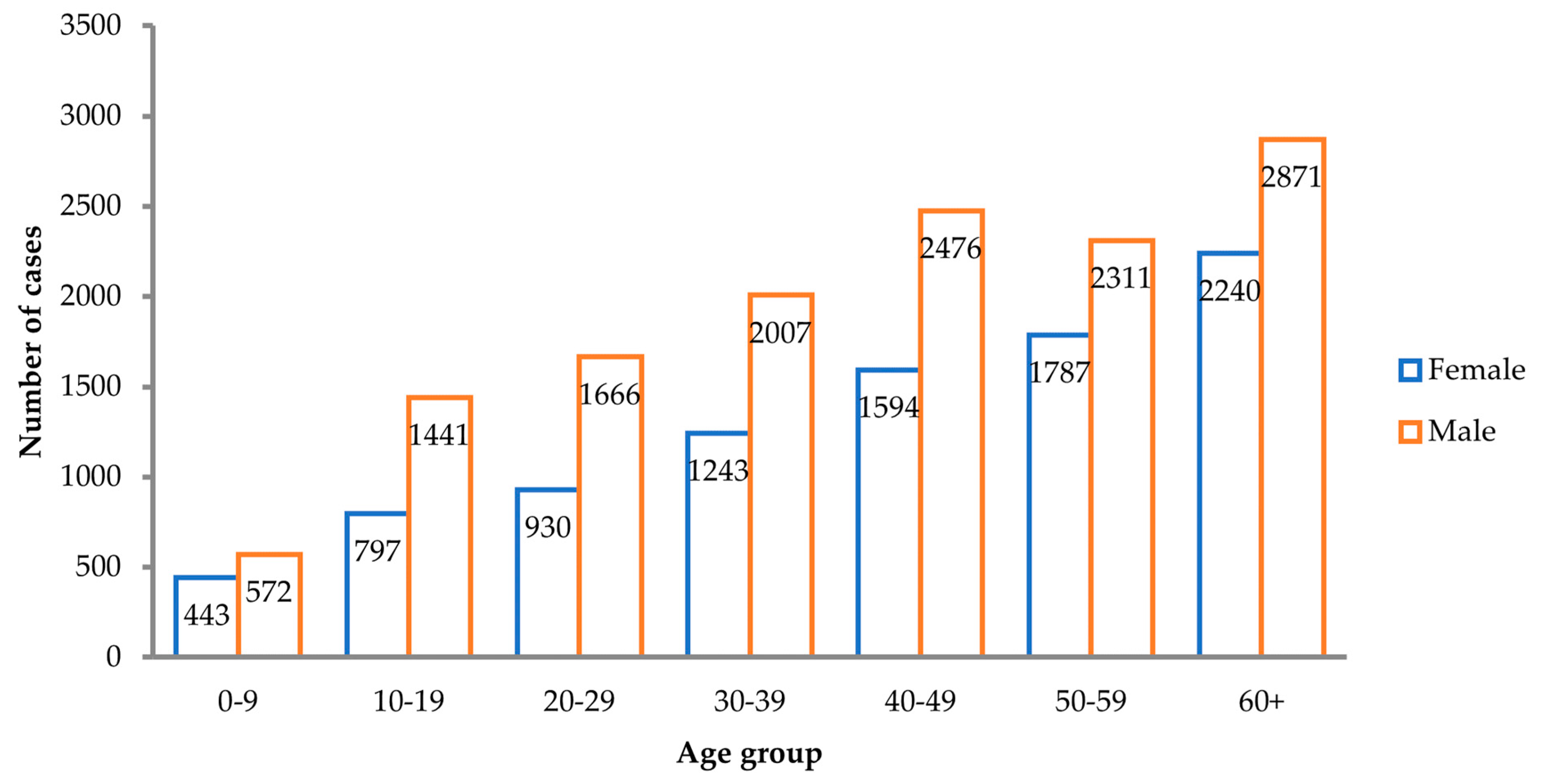
4. Epidemiological Trends of TBE, 2000–2019
5. Conclusions
Author Contributions
Funding
 This study was conducted as part of a project that received funding from the European Union’s Horizon 2020 Research and Innovation Programme, under the Marie Skłodowska-Curie grant agreement No 754432, and the Polish Ministry of Science and Higher Education, from financial resources for science in 2018–2023 granted for the implementation of an international co-financed project. The study was also partially financed by the National Science Centre, Poland, 2017/26/E/NZ6/00277.
This study was conducted as part of a project that received funding from the European Union’s Horizon 2020 Research and Innovation Programme, under the Marie Skłodowska-Curie grant agreement No 754432, and the Polish Ministry of Science and Higher Education, from financial resources for science in 2018–2023 granted for the implementation of an international co-financed project. The study was also partially financed by the National Science Centre, Poland, 2017/26/E/NZ6/00277.Institutional Review Board Statement
Conflicts of Interest
Consent for Publication
References
- Deviatkin, A.A.; Kholodilov, I.S.; Vakulenko, Y.A.; Karganova, G.G.; Lukashev, A.N. Tick-Borne Encephalitis Virus: An Emerging Ancient Zoonosis? Viruses 2020, 12, 247. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lipowski, D.; Popiel, M.; Perlejewski, K.; Nakamura, S.; Bukowska-Osko, I.; Rzadkiewicz, E.; Dzieciatkowski, T.; Milecka, A.; Wenski, W.; Ciszek, M.; et al. A Cluster of Fatal Tick-Borne Encephalitis Virus Infection in Organ Transplant Setting. J. Infect. Dis. 2017, 215, 896–901. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lindquist, L.; Vapalahti, O. Tick-Borne Encephalitis. Lancet 2008, 371, 1861–1871. [Google Scholar] [CrossRef]
- Estrada-Peña, A.; de la Fuente, J. The Ecology of Ticks and Epidemiology of Tick-Borne Viral Diseases. Antivir. Res. 2014, 108, 104–128. [Google Scholar] [CrossRef]
- Estrada-Peña, A.; Farkas, R.; Jaenson, T.G.T.; Koenen, F.; Madder, M.; Pascucci, I.; Salman, M.; Tarrés-Call, J.; Jongejan, F. Association of Environmental Traits with the Geographic Ranges of Ticks (Acari: Ixodidae) of Medical and Veterinary Importance in the Western Palearctic. A Digital Data Set. Exp. Appl. Acarol. 2013, 59, 351–366. [Google Scholar] [CrossRef] [Green Version]
- European Centre for Disease Prevention and Control. Epidemiological Situation of Tick-Borne Encephalitis in the European Union and European Free Trade Association Countries; ECDC: Stockholm, Sweden, 2012. [Google Scholar]
- Michelitsch, A.; Wernike, K.; Klaus, C.; Dobler, G.; Beer, M. Exploring the Reservoir Hosts of Tick-Borne Encephalitis Virus. Viruses 2019, 11, 669. [Google Scholar] [CrossRef] [Green Version]
- Bakhvalova, V.N.; Potapova, O.F.; Panov, V.V.; Morozova, O.V. Vertical Transmission of Tick-Borne Encephalitis Virus between Generations of Adapted Reservoir Small Rodents. Virus Res. 2009, 140, 172–178. [Google Scholar] [CrossRef]
- Karbowiak, G.; Biernat, B. The Role of Particular Tick Developmental Stages in the Circulation of Tick-Borne Pathogens Affecting Humans in Central Europe. 2. Tick-Borne Encephalitis Virus. Ann. Parasitol. 2016, 62, 3–9. [Google Scholar] [CrossRef]
- Klaus, C.; Gethmann, J.; Hoffmann, B.; Ziegler, U.; Heller, M.; Beer, M. Tick Infestation in Birds and Prevalence of Pathogens in Ticks Collected from Different Places in Germany. Parasitol. Res. 2016, 115, 2729–2740. [Google Scholar] [CrossRef] [Green Version]
- Dai, X.; Shang, G.; Lu, S.; Yang, J.; Xu, J. A New Subtype of Eastern Tick-Borne Encephalitis Virus Discovered in Qinghai-Tibet Plateau, China. Emerg. Microbes Infect. 2018, 7, 74. [Google Scholar] [CrossRef]
- Holding, M.; Dowall, S.D.; Medlock, J.M.; Carter, D.P.; McGinley, L.; Curran-French, M.; Pullan, S.T.; Chamberlain, J.; Hansford, K.M.; Baylis, M.; et al. Detection of New Endemic Focus of Tick-Borne Encephalitis Virus (TBEV), Hampshire/Dorset Border, England, September 2019. Eurosurveillance 2019, 24, 1900658. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bogovic, P. Tick-Borne Encephalitis: A Review of Epidemiology, Clinical Characteristics, and Management. WJCC 2015, 3, 430. [Google Scholar] [CrossRef] [PubMed]
- Pulkkinen, L.; Butcher, S.; Anastasina, M. Tick-Borne Encephalitis Virus: A Structural View. Viruses 2018, 10, 350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruzek, D.; Avšič Županc, T.; Borde, J.; Chrdle, A.; Eyer, L.; Karganova, G.; Kholodilov, I.; Knap, N.; Kozlovskaya, L.; Matveev, A.; et al. Tick-Borne Encephalitis in Europe and Russia: Review of Pathogenesis, Clinical Features, Therapy, and Vaccines. Antivir. Res. 2019, 164, 23–51. [Google Scholar] [CrossRef] [PubMed]
- Zlobin, V.I.; Pogodina, V.V.; Kahl, O. A Brief History of the Discovery of Tick-Borne Encephalitis Virus in the Late 1930s (Based on Reminiscences of Members of the Expeditions, Their Colleagues, and Relatives). Ticks Tick-Borne Dis. 2017, 8, 813–820. [Google Scholar] [CrossRef] [PubMed]
- Barrett, P.N.; Schober-Bendixen, S.; Ehrlich, H.J. History of TBE Vaccines. Vaccine 2003, 21, S41–S49. [Google Scholar] [CrossRef]
- Randolph, S.E. Ticks Are Not Insects: Consequences of Contrasting Vector Biology for Transmission Potential. Parasitol. Today 1998, 14, 186–192. [Google Scholar] [CrossRef]
- Hartemink, N.A.; Randolph, S.E.; Davis, S.A.; Heesterbeek, J.A.P. The Basic Reproduction Number for Complex Disease Systems: Defining R0 for Tick-Borne Infections. Am. Nat. 2008, 171, 743–754. [Google Scholar] [CrossRef] [Green Version]
- Kahl, O.; Alidousti, I. Bodies of Liquid Water as a Source of Water Gain for Ixodes Ricinus Ticks (Acari: Ixodidae). Exp. Appl. Acarol. 1997, 21, 731–746. [Google Scholar] [CrossRef]
- Hrnjaković Cvjetković, I.; Cvjetković, D.; Patić, A.; Radovanov, J.; Kovacević, G.; Milosević, V. TICK-BORNE ENCEPHALITIS VIRUS INFECTION IN HUMANS. Med. Pregl. 2016, 69, 93–98. [Google Scholar] [CrossRef] [Green Version]
- A Clear and Present Danger: Tick-Borne Diseases in Europe. Available online: http://www.medscape.com/viewarticle/717730 (accessed on 29 July 2020).
- Randolph, S.E. Ticks and Tick-Borne Disease Systems in Space and from Space. In Advances in Parasitology; Remote Sensing and Geographical Information Systems in Epidemiology; Academic Press: Cambridge, MA, USA, 2000; Volume 47, pp. 217–243. [Google Scholar]
- Gray, J.S.; Dautel, H.; Estrada-Peña, A.; Kahl, O.; Lindgren, E. Effects of Climate Change on Ticks and Tick-Borne Diseases in Europe. Interdiscip. Perspect. Infect. Dis. 2009, 2009, 593232. [Google Scholar] [CrossRef]
- Jaenson, T.G.; Hjertqvist, M.; Bergström, T.; Lundkvist, Å. Why Is Tick-Borne Encephalitis Increasing? A Review of the Key Factors Causing the Increasing Incidence of Human TBE in Sweden. Parasites Vectors 2012, 5, 184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ostfeld, R.S.; Brunner, J.L. Climate Change and Ixodes Tick-Borne Diseases of Humans. Philos. Trans. R. Soc. B Biol. Sci. 2015, 370, 20140051. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ogden, N.H.; Lindsay, L.R.; Beauchamp, G.; Charron, D.; Maarouf, A.; O’Callaghan, C.J.; Waltner-Toews, D.; Barker, I.K. Investigation of Relationships Between Temperature and Developmental Rates of Tick Ixodes Scapularis (Acari: Ixodidae) in the Laboratory and Field. J. Med. Entomol. 2004, 41, 622–633. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nieto, N.C.; Holmes, E.A.; Foley, J.E. Survival Rates of Immature Ixodes Pacificus (Acari: Ixodidae) Ticks Estimated Using Field-Placed Enclosures. J. Vector Ecol. 2010, 35, 43–49. [Google Scholar] [CrossRef]
- Randolph, S.E. To What Extent Has Climate Change Contributed to the Recent Epidemiology of Tick-Borne Diseases? Vet. Parasitol. 2010, 167, 92–94. [Google Scholar] [CrossRef]
- Radzišauskienė, D.; Žagminas, K.; Ašoklienė, L.; Jasionis, A.; Mameniškienė, R.; Ambrozaitis, A.; Jančorienė, L.; Jatužis, D.; Petraitytė, I.; Mockienė, E. Epidemiological Patterns of Tick-borne Encephalitis in Lithuania and Clinical Features in Adults in the Light of the High Incidence in Recent Years: A Retrospective Study. Eur. J. Neurol. 2018, 25, 268–274. [Google Scholar] [CrossRef] [Green Version]
- Kerbo, N.; Donchenko, I.; Kutsar, K.; Vasilenko, V. Tickborne Encephalitis Epidemiology in Estonia, 1950–2004. Wkly. Releases 2005, 10, 2740. [Google Scholar] [CrossRef]
- Kriz, B.; Maly, M.; Benes, C.; Daniel, M. Epidemiology of Tick-Borne Encephalitis in the Czech Republic 1970–2008. Vector Borne Zoonotic Dis. 2012, 12, 994–999. [Google Scholar] [CrossRef] [Green Version]
- Tick-Borne Encephalitis—Annual Epidemiological Report for 2018. Available online: https://www.ecdc.europa.eu/en/publications-data/tick-borne-encephalitis-annual-epidemiological-report-2018 (accessed on 30 December 2020).
- Amicizia, D.; Domnich, A.; Panatto, D.; Lai, P.L.; Cristina, M.L.; Avio, U.; Gasparini, R. Epidemiology of Tick-Borne Encephalitis (TBE) in Europe and Its Prevention by Available Vaccines. Hum. Vaccin. Immunother. 2013, 9, 1163–1171. [Google Scholar] [CrossRef] [Green Version]
- Blomqvist, G.; Näslund, K.; Svensson, L.; Beck, C.; Valarcher, J.F. Mapping Geographical Areas at Risk for Tick-Borne Encephalitis (TBE) by Analysing Bulk Tank Milk from Swedish Dairy Cattle Herds for the Presence of TBE Virus–Specific Antibodies. Acta Vet. Scand. 2021, 63, 16. [Google Scholar] [CrossRef] [PubMed]
- Pettersson, J.H.-O.; Golovljova, I.; Vene, S.; Jaenson, T.G.T. Prevalence of Tick-Borne Encephalitis Virus in Ixodes Ricinus Ticks in Northern Europe with Particular Reference to Southern Sweden. Parasites Vectors 2014, 7, 102. [Google Scholar] [CrossRef] [Green Version]
- Hartemink, N.; Takken, W. Trends in Tick Population Dynamics and Pathogen Transmission in Emerging Tick-Borne Pathogens in Europe: An Introduction. Exp. Appl. Acarol. 2016, 68, 269–278. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knap, N.; Avšič-Županc, T. Factors Affecting the Ecology of Tick-Borne Encephalitis in Slovenia. Epidemiol. Infect. 2015, 143, 2059–2067. [Google Scholar] [CrossRef]
- Süss, J.; Kahl, O.; Aspöck, H.; Hartelt, K.; Vaheri, A.; Oehme, R.; Hasle, G.; Dautel, H.; Kunz, C.; Kupreviciene, N.; et al. Tick-Borne Encephalitis in the Age of General Mobility; Springer: Berlin/Heidelberg, Germany, 2010; pp. 94–100. [Google Scholar]
- Egyed, L.; Rónai, Z.; Dán, Á. Hungarian Tick-Borne Encephalitis Viruses Isolated from a 0.5-Ha Focus Are Closely Related to Finnish Strains. Ticks Tick-Borne Dis. 2018, 9, 1064–1068. [Google Scholar] [CrossRef]
- Jääskeläinen, A.E.; Sironen, T.; Murueva, G.B.; Subbotina, N.; Alekseev, A.N.; Castrén, J.; Alitalo, I.; Vaheri, A.; Vapalahti, O. Tick-Borne Encephalitis Virus in Ticks in Finland, Russian Karelia and Buryatia. J. Gen. Virol. 2010, 91, 2706–2712. [Google Scholar] [CrossRef]
- Yurchenko, O.O.; Dubina, D.O.; Vynograd, N.O.; Gonzalez, J.-P. Partial Characterization of Tick-Borne Encephalitis Virus Isolates from Ticks of Southern Ukraine. Vector Borne Zoonotic Dis. 2017, 17, 550–557. [Google Scholar] [CrossRef] [Green Version]
- Agergaard, C.N.; Rosenstierne, M.W.; Bødker, R.; Rasmussen, M.; Andersen, P.H.S.; Fomsgaard, A. New Tick-Borne Encephalitis Virus Hot Spot in Northern Zealand, Denmark, October 2019. Eurosurveillance 2019, 24, 1900639. [Google Scholar] [CrossRef]
- Frimmel, S.; Krienke, A.; Riebold, D.; Loebermann, M.; Littmann, M.; Fiedler, K.; Klaus, C.; Süss, J.; Reisinger, E.C. Tick-Borne Encephalitis Virus Habitats in North East Germany: Reemergence of TBEV in Ticks after 15 Years of Inactivity. Available online: https://www.hindawi.com/journals/bmri/2014/308371/ (accessed on 8 January 2021).
- Makenov, M.; Karan, L.; Shashina, N.; Akhmetshina, M.; Zhurenkova, O.; Kholodilov, I.; Karganova, G.; Smirnova, N.; Grigoreva, Y.; Yankovskaya, Y.; et al. First Detection of Tick-Borne Encephalitis Virus in Ixodes Ricinus Ticks and Their Rodent Hosts in Moscow, Russia. Ticks Tick-Borne Dis. 2019, 10, 101265. [Google Scholar] [CrossRef]
- Randolph, S.E. Dynamics of Tick-Borne Disease Systems: Minor Role of Recent Climate Change. Rev. Sci. Tech. 2008, 27, 367. [Google Scholar] [CrossRef]
- Randolph, S. Predicting the Risk of Tick-Borne Diseases. Int. J. Med. Microbiol. 2002, 291, 6–10. [Google Scholar] [CrossRef]
- Randolph, S.E.; Rogers, D.J. Fragile Transmission Cycles of Tick-Borne Encephalitis Virus May Be Disrupted by Predicted Climate Change. Proc. Biol. Sci. 2000, 267, 1741–1744. [Google Scholar] [CrossRef] [Green Version]
- Daniel, M.; Danielová, V.; Kříž, B.; Jirsa, A.; Nožička, J. Shift of the Tick Ixodes Ricinus and Tick-Borne Encephalitis to Higher Altitudes in Central Europe. Eur. J. Clin. Microbiol. Infect. Dis. 2003, 22, 327–328. [Google Scholar] [CrossRef]
- Tick-Borne Encephalitis Virus Expansion to Higher Altitudes Correlated with Climate Warming—ScienceDirect. Available online: https://www.sciencedirect.com/science/article/pii/S1438422108000398 (accessed on 15 January 2021).
- Rizzoli, A.; Merler, S.; Furlanello, C.; Genchi, C. Geographical Information Systems and Bootstrap Aggregation (Bagging) of Tree-Based Classifiers for Lyme Disease Risk Prediction in Trentino, Italian Alps. J. Med. Entomol. 2002, 39, 485–492. [Google Scholar] [CrossRef]
- Medlock, J.M.; Hansford, K.M.; Bormane, A.; Derdakova, M.; Estrada-Peña, A.; George, J.-C.; Golovljova, I.; Jaenson, T.G.; Jensen, J.-K.; Jensen, P.M.; et al. Driving Forces for Changes in Geographical Distribution of Ixodes Ricinus Ticks in Europe. Parasites Vectors 2013, 6, 1. [Google Scholar] [CrossRef] [Green Version]
- Cagnacci, F.; Focardi, S.; Heurich, M.; Stache, A.; Hewison, A.J.M.; Morellet, N.; Kjellander, P.; Linnell, J.D.C.; Mysterud, A.; Neteler, M.; et al. Partial Migration in Roe Deer: Migratory and Resident Tactics Are End Points of a Behavioural Gradient Determined by Ecological Factors. Oikos 2011, 120, 1790–1802. [Google Scholar] [CrossRef]
- Kaaijk, P.; Luytjes, W. Are We Prepared for Emerging Flaviviruses in Europe? Challenges for Vaccination. Hum. Vaccines Immunother. 2018, 14, 337–344. [Google Scholar] [CrossRef] [Green Version]
- Riccardi, N.; Antonello, R.M.; Luzzati, R.; Zajkowska, J.; Bella, S.D.; Giacobbe, D.R. Tick-Borne Encephalitis in Europe: A Brief Update on Epidemiology, Diagnosis, Prevention, and Treatment. Eur. J. Intern. Med. 2019, 62, 1–6. [Google Scholar] [CrossRef]
- Taba, P.; Schmutzhard, E.; Forsberg, P.; Lutsar, I.; Ljøstad, U.; Mygland, Å.; Levchenko, I.; Strle, F.; Steiner, I. EAN Consensus Review on Prevention, Diagnosis and Management of Tick-Borne Encephalitis. Eur. J. Neurol. 2017, 24, 1214-e61. [Google Scholar] [CrossRef]
- Kollaritsch, H.; Paulke-Korinek, M.; Holzmann, H.; Hombach, J.; Bjorvatn, B.; Barrett, A. Vaccines and Vaccination against Tick-Borne Encephalitis. Expert Rev. Vaccines 2012, 11, 1103–1119. [Google Scholar] [CrossRef]
- Lindblom, P.; Wilhelmsson, P.; Fryland, L.; Matussek, A.; Haglund, M.; Sjöwall, J.; Vene, S.; Nyman, D.; Forsberg, P.; Lindgren, P.-E. Factors Determining Immunological Response to Vaccination against Tick-Borne Encephalitis Virus in Older Individuals. PLoS ONE 2014, 9, e100860. [Google Scholar] [CrossRef] [PubMed]



| Year | Number of Countries | Number of Confirmed Cases | Number of Confirmed Cases/100,000 Population |
|---|---|---|---|
| 2000 | 12 | 2629 | 7.02 |
| 2001 | 14 | 2497 | 5.07 |
| 2002 | 14 | 1952 | 3.19 |
| 2003 | 14 | 3225 | 6.15 |
| 2004 | 14 | 2481 | 4.33 |
| 2005 | 15 | 2651 | 3.71 |
| 2006 | 15 | 3756 | 4.94 |
| 2007 | 15 | 2267 | 3.27 |
| 2008 | 16 | 2513 | 3.15 |
| 2009 | 16 | 3513 | 5.07 |
| 2010 | 16 | 3155 | 5.06 |
| 2012 | 21 | 2149 | 2.34 |
| 2013 | 22 | 2904 | 3.03 |
| 2014 | 24 | 1985 | 1.75 |
| 2015 | 24 | 1908 | 1.75 |
| 2016 | 25 | 2680 | 2.14 |
| 2017 | 25 | 2916 | 2.22 |
| 2018 | 26 | 3092 | 2.07 |
| 2019 | 25 | 3246 | 2.57 |
| Total | 51519 |
| Country | Number of Years | Confirmed Cases | IR/100,000 | Age-Adjusted IR/100,000 (2012–2019) |
|---|---|---|---|---|
| Czechia | 19 | 12055 | 6.14 | 5.50 |
| Lithuania | 19 | 8178 | 13.66 | 15.64 |
| Germany | 19 | 6089 | 0.41 | 0.43 |
| Latvia | 19 | 4184 | 9.95 | 6.60 |
| Poland | 19 | 3933 | 0.54 | 0.41 |
| Slovenia | 19 | 3877 | 10.12 | 6.34 |
| Sweden | 19 | 3345 | 2.48 | 2.85 |
| Estonia | 19 | 2761 | 10.86 | 7.73 |
| Slovakia | 19 | 1734 | 1.69 | 2.15 |
| Austria | 19 | 1562 | 0.97 | 1.10 |
| Switzerland | 11 | 1302 | . | . |
| Hungary | 19 | 878 | 0.46 | 0.24 |
| Finland | 19 | 787 | 0.77 | 1.07 |
| Italy | 18 | 312 | 0.03 | 0.03 |
| Croatia | 8 | 189 | 0.56 | 0.53 |
| Norway | 19 | 186 | 0.20 | 0.30 |
| France | 8 | 67 | 0.01 | 0.01 |
| Romania | 19 | 26 | 0.01 | 0.01 |
| Netherlands | 4 | 16 | . | . |
| Belgium | 8 | 14 | 0.02 | 0.02 |
| United Kingdom | 8 | 9 | 0.00 | 0.00 |
| Denmark | 1 | 4 | 0.07 | 0.07 |
| Bulgaria | 6 | 4 | 0.01 | 0.01 |
| Greece | 8 | 4 | 0.00 | 0.01 |
| Luxembourg | 6 | 1 | 0.03 | 0.03 |
| Ireland | 8 | 1 | 0.00 | 0.00 |
| Spain | 8 | 1 | 0.00 | 0.00 |
| Total | 51519 | 3.26 ** | 2.19 ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wondim, M.A.; Czupryna, P.; Pancewicz, S.; Kruszewska, E.; Groth, M.; Moniuszko-Malinowska, A. Epidemiological Trends of Trans-Boundary Tick-Borne Encephalitis in Europe, 2000–2019. Pathogens 2022, 11, 704. https://doi.org/10.3390/pathogens11060704
Wondim MA, Czupryna P, Pancewicz S, Kruszewska E, Groth M, Moniuszko-Malinowska A. Epidemiological Trends of Trans-Boundary Tick-Borne Encephalitis in Europe, 2000–2019. Pathogens. 2022; 11(6):704. https://doi.org/10.3390/pathogens11060704
Chicago/Turabian StyleWondim, Mulugeta A., Piotr Czupryna, Sławomir Pancewicz, Ewelina Kruszewska, Monika Groth, and Anna Moniuszko-Malinowska. 2022. "Epidemiological Trends of Trans-Boundary Tick-Borne Encephalitis in Europe, 2000–2019" Pathogens 11, no. 6: 704. https://doi.org/10.3390/pathogens11060704