Changes in the Sodium Content of New Zealand Processed Foods: 2003–2013



Abstract
:1. Introduction
2. Experimental Section
2.1. Data Sources, Food Groups and Categories
- (1)
- Were major contributors to population sodium intakes [15]
- (2)
- Included a wide range of sodium contents across the food category; a wide range of sodium contents indicates the potential or feasibility for producing lower sodium products, i.e., sodium reduction
- (3)
- Displayed a NIP (a new Food Standards Code came into effect in 2002 requiring almost all packaged food to display a NIP) [16]. In 2003, some food products did not yet meet these requirements as companies were still working towards the requirements of the new Code (e.g., sausages)
2.2. Data Cleaning and Matching

{kind=link}
| Sodium content 2003 (mg 100 g−1) | Sodium content 2013 (mg 100 g−1) | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N | % total foods * | Mean | SD | Median | Min | Max | N | % total foods * | Mean | SD | Median | Min | Max | ||
| Bread | All | 45 | 14% | 472 | 61 | 450 | 350 | 600 | 104 | 12% | 410 | 68 | 410 | 380 | 630 |
| White | 17 | 5% | 516 | 52 | 515 | 450 | 600 | 23 | 3% | 433 | 62 | 410 | 346 | 630 | |
| Whole Meal/Grain | 28 | 9% | 445 | 51 | 450 | 350 | 540 | 81 | 9% | 403 | 68 | 410 | 1 | 530 | |
| Breakfast cereals$ | All | 109 | 34% | 348 | 275 | 289 | 6 | 933 | 176 | 20% | 215 | 183 | 205 | 1 | 780 |
| Childrens’ | 34 | 11% | 574 | 286 | 577 | 6 | 933 | 42 | 5% | 358 | 229 | 378 | 2 | 780 | |
| Museli | 22 | 7% | 111 | 125 | 61 | 14 | 479 | 47 | 5% | 64 | 81 | 43 | 4 | 479 | |
| Other | 44 | 14% | 303 | 216 | 286 | 10 | 714 | 74 | 8% | 211 | 133 | 215 | 1 | 520 | |
| Wheat Biscuits & Bites | 9 | 3% | 297 | 76 | 280 | 205 | 437 | 13 | 1% | 317 | 54 | 300 | 235 | 410 | |
| Butter, Margarine & Dairy Blends | All | 50 | 15% | 474 | 135 | 400 | 360 | 772 | 58 | 7% | 421 | 139 | 360 | 1 | 700 |
| Butter | 7 | 2% | 480 | 0 | 480 | 480 | 480 | 11 | 1% | 579 | 47 | 600 | 480 | 600 | |
| Dairy Blends | 6 | 2% | 467 | 123 | 400 | 390 | 700 | 9 | 1% | 394 | 34 | 400 | 360 | 470 | |
| Margarine | 37 | 11% | 474 | 150 | 380 | 360 | 772 | 38 | 4% | 382 | 140 | 360 | 1 | 700 | |
| Canned Corned Beef | All | 10 | 3% | 770 | 265 | 750 | 463 | 1369 | 11 | 1% | 718 | 164 | 750 | 460 | 920 |
| Canned Salmon | All | 9 | 3% | 347 | 195 | 425 | 80 | 600 | 32 | 4% | 364 | 134 | 369 | 59 | 580 |
| Canned Spaghetti | All | 9 | 3% | 474 | 127 | 460 | 370 | 800 | 13 | 1% | 370 | 125 | 390 | 1 | 505 |
| Canned Vegetables | All | 39 | 12% | 241 | 174 | 270 | 0 | 780 | 116 | 13% | 200 | 137 | 185 | 0 | 583 |
| Asparagus | 7 | 2% | 289 | 23 | 280 | 280 | 340 | 7 | 1% | 238 | 62 | 240 | 120 | 310 | |
| Baked Beans | 9 | 3% | 445 | 194 | 365 | 270 | 780 | 22 | 2% | 384 | 124 | 415 | 0 | 583 | |
| Beetroot | 4 | 1% | 273 | 157 | 335 | 40 | 380 | 12 | 1% | 234 | 67 | 237 | 70 | 330 | |
| Creamed Corn | 7 | 2% | 167 | 55 | 150 | 140 | 290 | 8 | 1% | 194 | 65 | 165 | 130 | 300 | |
| Tomatoes | 7 | 2% | 90 | 89 | 60 | 0 | 190 | 56 | 6% | 120 | 96 | 128 | 0 | 350 | |
| Whole Corn Kernels | 5 | 2% | 94 | 52 | 110 | 5 | 140 | 11 | 1% | 185 | 90 | 162 | 2 | 340 | |
| Cheese ^ | All | 15 | 5% | 661 | 56 | 630 | 590 | 800 | 59 | 7% | 673 | 61 | 670 | 315 | 760 |
| Crackers | All | 37 | 11% | 637 | 369 | 610 | 8 | 1390 | 316 | 36% | 604 | 367 | 594 | 0 | 1810 |
| Total | 323 | 436 | 263 | 430 | 0 | 1390 | 885 | 433 | 304 | 400 | 0 | 1810 | |||
2.3. Statistical Analysis
3. Results
3.1. Sodium Content of Food Groups and Categories in 2003 and 2013
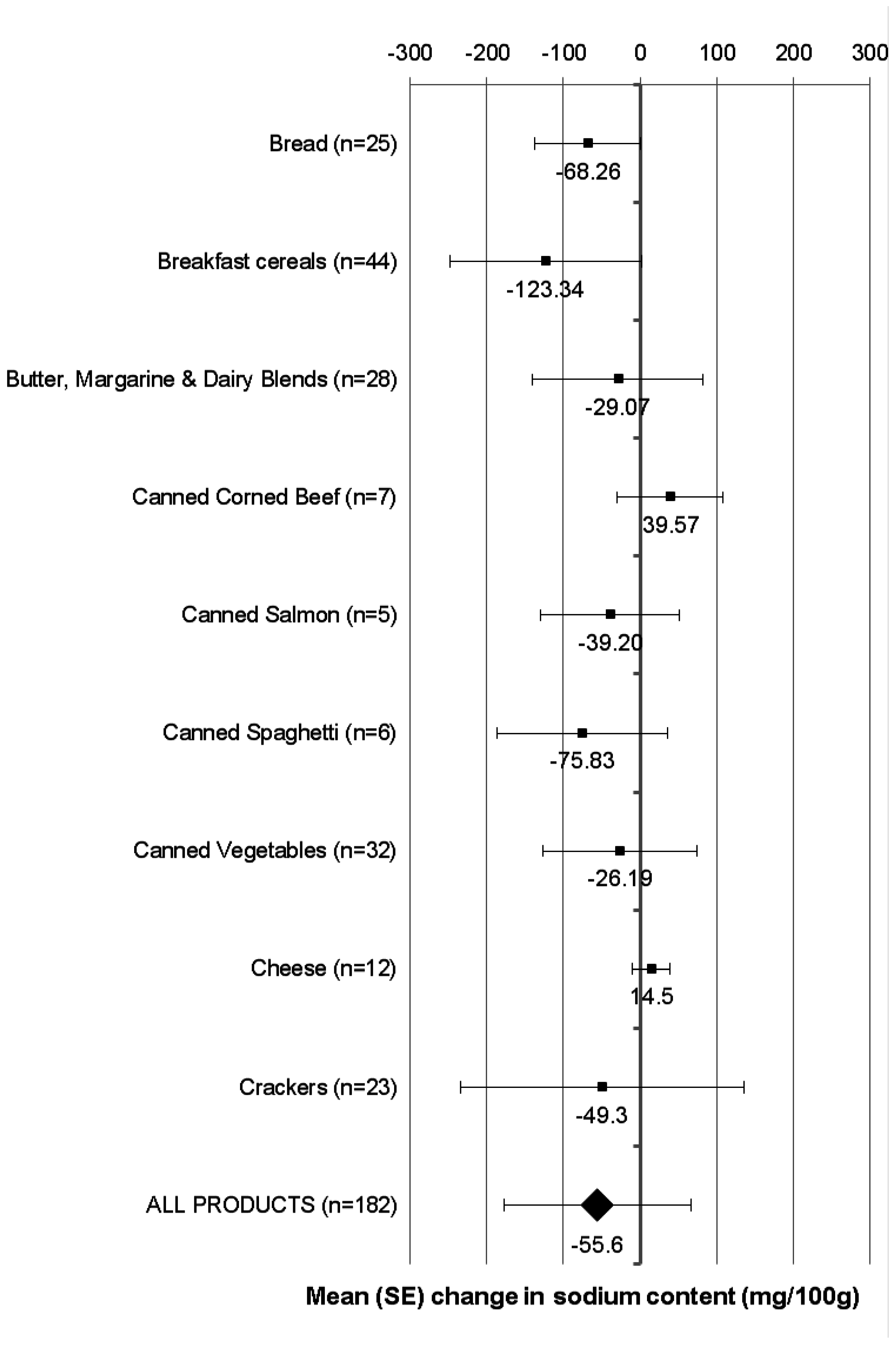
3.2. Change in Sodium Content of Matched Products Available for Sale in Both 2003 and 2013

3.3. Sodium Content of Private Label and Branded Products in 2003 and 2013
4. Discussion
| Sodium Content 2003 (mg (100 g)−1) | Sodium Content 2013 (mg (100 g)−1) | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N | Mean | SD | Median | Min | Max | N | Mean | SD | Median | Min | Max | ||
| Bread | Branded | 29 | 463 | 59 | 450 | 350 | 560 | 85 | 408 | 73 | 410 | 1 | 630 |
| Private Label | 16 | 488 | 65 | 490 | 366 | 600 | 19 | 416 | 34 | 410 | 366 | 503 | |
| Breakfast cereals $ | Branded | 73 | 320 | 247 | 289 | 6 | 920 | 146 | 201 | 167 | 191 | 1 | 725 |
| Private Label | 36 | 406 | 320 | 294 | 7 | 933 | 30 | 279 | 237 | 280 | 3 | 780 | |
| Butter, margarine, and dairy blends | Branded | 36 | 421 | 89 | 380 | 360 | 700 | 52 | 414 | 136 | 360 | 1 | 700 |
| Private Label | 14 | 608 | 142 | 575 | 377 | 772 | 6 | 486 | 157 | 475 | 339 | 680 | |
| Canned corned beef | Branded | 9 | 772 | 281 | 750 | 463 | 1369 | 8 | 645 | 128 | 637 | 460 | 820 |
| Private Label | 1 | 750 | . | 750 | 750 | 750 | 3 | 910 | 9 | 905 | 905 | 920 | |
| Canned salmon | Branded | 6 | 297 | 227 | 273 | 80 | 600 | 24 | 373 | 124 | 375 | 76 | 580 |
| Private Label | 3 | 445 | 39 | 468 | 400 | 468 | 8 | 337 | 165 | 367 | 59 | 538 | |
| Canned spaghetti | Branded | 3 | 420 | 40 | 420 | 380 | 460 | 10 | 345 | 130 | 385 | 1 | 455 |
| Private Label | 6 | 502 | 151 | 460 | 370 | 800 | 3 | 453 | 58 | 465 | 390 | 505 | |
| Canned vegetables | Branded | 25 | 223 | 166 | 190 | 0 | 740 | 79 | 208 | 146 | 185 | 0 | 583 |
| Private Label | 14 | 273 | 190 | 280 | 10 | 780 | 37 | 185 | 113 | 168 | 5 | 440 | |
| Cheese ^ | Branded | 7 | 669 | 72 | 670 | 590 | 800 | 42 | 672 | 69 | 685 | 315 | 760 |
| Private Label | 8 | 653 | 41 | 630 | 620 | 710 | 17 | 676 | 34 | 668 | 620 | 740 | |
| Crackers | Branded | 33 | 632 | 384 | 610 | 8 | 1390 | 277 | 605 | 378 | 600 | 0 | 1810 |
| Private Label | 4 | 678 | 238 | 690 | 410 | 920 | 39 | 598 | 284 | 553 | 100 | 1370 | |
| ALL PRODUCTS | Branded | 221 | 421 | 269 | 400 | 0 | 1390 | 723 | 436 | 312 | 400 | 0 | 1810 |
| Private Label | 102 | 468 | 247 | 475 | 7 | 933 | 162 | 417 | 265 | 400 | 3 | 1370 | |
5. Conclusions
Supplementary Files
Supplementary File 1Acknowledgments
Author Contributions
Conflicts of Interest
References
- Lim, S.S.; Vos, T.; Flaxman, A.D.; Danaei, G.; Shibuya, K.; Adair-Rohani, H.; AlMazroa, M.A.; Amann, M.; Anderson, H.R.; Andrews, K.G.; et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012, 380, 2224–2260. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Guideline: Sodium Intake for Adults and Children. Available online: http://www.who.int/nutrition/publications/guidelines/sodium_intake_printversion.pdf (accessed on 18 February 2013).
- Sadler, K.; Nicholson, S.; Steer, T.; Gill, V.; Bates, B.; Tipping, S.; Cox, L.; Lennox, A.; Prentice, A. National Diet and Nutrition Survey—Assessment of Dietary Sodium in Adults (Aged 19 to 64 years) in England, 2011; Department of Health: London, United Kingdom, 2012.
- United States Department of Agriculture, Food Surveys Research Group. Sodium intake of the US population. In What We Eat in America, NHANES 2007–2008; 2011. Available online: www.ars.usda.gov/ba/bhnrc/fsrg (accessed on 22 May 2015). [Google Scholar]
- Slimani, N.; Deharveng, G.; Southgate, D.A.T.; Biessy, C.; Chajès, V.; van Bakel, M.M.E.; Boutron-Ruault, M.C.; McTaggart, A.; Grioni, S.; Verkaik-Kloosterman, J.; et al. Contribution of highly industrially processed foods to the nutrient intakes and patterns of middle-aged populations in the European Prospective Investigation into Cancer and Nutrition study. Eur. J. Clin. Nutr. 2009, 63, S206–S225. [Google Scholar] [CrossRef] [PubMed]
- Mason, H.; Shoaibi, A.; Ghandour, R.; O’Flaherty, M.; Capewell, S.; Khatib, R.; Jabr, S.; Unal, B.; Sözmen, K.; Arfa, C.; et al. A cost effectiveness analysis of salt reduction policies to reduce coronary heart disease in four Eastern Mediterranean countries. PLoS ONE 2014, 9, e84445. [Google Scholar] [CrossRef] [PubMed]
- Barton, P.; Andronis, L.; Briggs, A.; McPherson, K.; Capewell, S. Effectiveness and cost effectiveness of cardiovascular disease prevention in whole populations: Modelling study. Br. Med. J. 2011, 343, d4044. [Google Scholar] [CrossRef]
- Smith-Spangler, C.M.; Juusola, J.L.; Enns, E.A.; McPherson, K.; Capewell, S. Population strategies to decrease sodium intake and the burden of cardiovascular disease: A cost-effectiveness analysis. Ann. Int. Med. 2010, 1552, 481–487. [Google Scholar] [CrossRef]
- Kontis, V.; Mathers, C.D.; Rehm, J.; Stevens, G.A.; Shield, K.D.; Bonita, R.; Riley, L.M.; Poznyak, V.; Beaglehole, R.; Ezzati, M. Contribution of six risk factors to achieving the 25 × 25 non-communicable disease mortality reduction target: A modelling study. Lancet 2014. [Google Scholar] [CrossRef]
- Webster, J.L.; Trieu, K.; Dunford, E.; Hawkes, C. Target salt 2025: A global overview of national programs to encourage the food industry to reduce salt in foods. Nutrients 2014, 6, 3274–3287. [Google Scholar] [CrossRef] [PubMed]
- Eyles, H.; Webster, J.L.; Jebb, S.A.; Capelin, C.; Neal, B.; Ni, M.C. Impact of the UK voluntary sodium reduction targets on the sodium content of processed foods from 2006 to 2011: Analysis of household consumer panel data. Prev. Med. 2013, 57, 555–560. [Google Scholar] [CrossRef] [PubMed]
- Heart Foundation Tick Programme. Available online: http://www.heartfoundation.org.nz/healthy-living/healthy-eating/heart-foundation-tick/what-is-the-tick (accessed on 5 March 2015).
- Heart Foundation of New Zealand. HeartSAFE: Industry Commitment to Sodium Reduction. 2014. Available online: http://www.heartfoundation.org.nz/programmes-resources/food-industry-and-hospitality/heartsafe/industry-commitment-to-sodium-reduction (accessed on 27 May 2014).
- Monro, D.; Young, L.; Wilson, J.; Chisholm, A. The sodium content of low cost and private label foods; Implications for public health. J. N. Z. Diet. Assoc. 2004, 58, 4–10. [Google Scholar]
- Ministry of Health; University of Auckland. Nutrition and the Burden of Disease: New Zealand 1997–2011; Ministry of Health: Wellington, New Zealand, 2003.
- Food Standards Australia New Zealand. Nutrition Information User Guide to Standard 1.2.8 Nutrition Information Requirements. Available online: http://www.foodstandards.govt.nz/code/userguide/pages/nutritioninformation1406.aspx (accessed on 27 February 2015).
- National Institute for Health Innovation. Nutritrack: Reformulation of Processed Foods to Promote Health. Available online: http://nihi.auckland.ac.nz/page/current-research/our-nutrition-and-physical-activity-research/nutritrack-reformulation-processe (accessed on 12 February 2013).
- Global Market Information Database, 2014 version; Euromonitor International: London, UK, 2014.
- Eyles, H.; Ni Mhhurchu, C. Potential for electronic household food purchase data to enhance population nutrition monitoring. N. Z. Med. J. 2014, 127, 68–71. [Google Scholar] [PubMed]
- Australian Bureau of Statistics. Australian Social Trends; Australian Bureau of Statistics: Canberra, Australia, 2006.
- Statistics New Zealand. Household Economic Survey: Year Ended June 2013; Statistics New Zealand: Wellington, New Zealand, 2013.
- Young, L.; Swinburn, B. Impact of the Pick the Tick food information programme on the salt content of food in New Zealand. Health Prom. Int. 2002, 17, 13–19. [Google Scholar] [CrossRef]
- Beaglehole, R.; Bonita, R.; Ezzati, M.; Alleyne, G.; Dain, K.; Kishore, S.P.; Horton, R. NCD Countdown 2025: Accountability for the 25 × 25 NCD mortality reduction target. Lancet 2014, 384, 105–107. [Google Scholar] [CrossRef] [PubMed]
- Wyness, L.A.; Butriss, J.L.; Stanner, S.A. Reducing the population’s sodium intake: The UK Food Standards Agency’s salt reduction programme. Public Health Nutr. 2012, 15, 254–261. [Google Scholar] [CrossRef] [PubMed]
- Trevena, H.; Neal, B.; Dunford, E.; Wu, J.H.Y. An evaluation of the effects of the Australian Food and Health Dialogue targets on the sodium content of bread, breakfast cereals, and processed meats. Nutrients 2014, 6, 3802–3817. [Google Scholar] [CrossRef] [PubMed]
- Woodward, E.; Eyles, H.; Ni Mhurchu, C. Key opportunities for sodium reduction in New Zealand processed foods. Aust. N. Z. J. Public Health 2012, 36, 84–89. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Monro, D.; Mhurchu, C.N.; Jiang, Y.; Gorton, D.; Eyles, H. Changes in the Sodium Content of New Zealand Processed Foods: 2003–2013. Nutrients 2015, 7, 4054-4067. https://doi.org/10.3390/nu7064054
Monro D, Mhurchu CN, Jiang Y, Gorton D, Eyles H. Changes in the Sodium Content of New Zealand Processed Foods: 2003–2013. Nutrients. 2015; 7(6):4054-4067. https://doi.org/10.3390/nu7064054
Chicago/Turabian StyleMonro, David, Cliona Ni Mhurchu, Yannan Jiang, Delvina Gorton, and Helen Eyles. 2015. "Changes in the Sodium Content of New Zealand Processed Foods: 2003–2013" Nutrients 7, no. 6: 4054-4067. https://doi.org/10.3390/nu7064054