
Very Low-Calorie Ketogenic Diet: A Potential Application in the Treatment of Hypercortisolism Comorbidities


Dipartimento di Promozione della Salute, Materno-Infantile, Medicina Interna e Specialistica di Eccellenza “G. D’Alessandro” (PROMISE), Sezione di Malattie Endocrine, del Ricambio e della Nutrizione, Università di Palermo, 90127 Palermo, Italy
*
Author to whom correspondence should be addressed.
Nutrients 2022, 14(12), 2388; https://doi.org/10.3390/nu14122388
Submission received: 3 May 2022
/
Revised: 3 June 2022
/
Accepted: 8 June 2022
/
Published: 9 June 2022
(This article belongs to the Section Nutrition and Metabolism)
Abstract
:A very low-calorie ketogenic diet (VLCKD) is characterized by low daily caloric intake (less than 800 kcal/day), low carbohydrate intake (<50 g/day) and normoproteic (1–1.5 g of protein/kg of ideal body weight) contents. It induces a significant weight loss and an improvement in lipid parameters, blood pressure, glycaemic indices and insulin sensitivity in patients with obesity and type 2 diabetes mellitus. Cushing’s syndrome (CS) is characterized by an endogenous or exogenous excess of glucocorticoids and shows many comorbidities including cardiovascular disease, obesity, type 2 diabetes mellitus and lipid disorders. The aim of this speculative review is to provide an overview on nutrition in hypercortisolism and analyse the potential use of a VLCKD for the treatment of CS comorbidities, analysing the molecular mechanisms of ketogenesis.
1. Introduction
Cushing’s syndrome is characterized by an exogenous or endogenous excess of glucocorticoids (GCs) resulting in a combination of metabolic disorders, including visceral obesity, type 2 diabetes mellitus, dyslipidaemia and cardiovascular disease. Nutrition has an important role in the management of obesity, diabetes mellitus and cardiovascular disease and may be used as an additional treatment of the metabolic comorbidities in patients with CS waiting to undergo neurosurgery or to reach pharmacologically biochemical remission.
Traditional methods of weight loss include various types of low-calorie diets calculated on a calorie range of between 800 and 1500 Kcal per day, although calorie requirements vary from individual to individual, so the goal of weight loss can also be achieved with a higher calorie amount [1]. A VLCKD is a nutritional approach characterized by low daily caloric intake (less than 800 kcal/day), low carbohydrate (<50 g/day) and normoproteic (1–1.5 g of protein/kg of ideal body weight) contents [2,3]. This dietogenic protocol leads to the production of ketones, which are then used by other tissues such as the central nervous system, skeletal muscle and heart for energy production [4].
A VLCKD has been reported to induce a significant weight loss and improvement in lipid parameters, glycaemic indices and insulin sensitivity, beyond an improvement in neurological and respiratory disorders [5,6,7,8,9,10]. Currently, there are no studies evaluating the effects of a VLCKD and CS; therefore, this area needs further investigation.
Thus, the aim of this speculative review is to focus on the current evidence of nutrition and cortisol levels and the beneficial effects of a VLCKD on metabolic complications and its potential application in patients with hypercortisolism for the treatment of its comorbidities.
2. Cushing’s Syndrome
CS is characterized by an excess of GCs that can be exogenous due to a chronic intake of corticosteroids or endogenous owing to the pituitary or adrenal hyperproduction of ACTH or cortisol, respectively. Rarely, the endogenous form can result from an extra-pituitary ACTH-secreting tumour (ectopic CS) [11].
CS is associated with increased mortality and a high risk of cardiovascular disease due to the presence of several comorbidities [12,13,14,15,16]. Comorbidities of CS include metabolic syndrome, characterized by systemic arterial hypertension, visceral obesity, impaired glucose metabolism and dyslipidaemia, polycystic ovary syndrome (PCOS), musculoskeletal disorders, such as myopathy, osteoporosis and skeletal fractures, infections, neuropsychiatric disorders, such as impaired cognitive function, depression or mania, impaired reproductive and sexual function and dermatological manifestations, represented mainly by acne, hirsutism and alopecia [14,15,16,17,18].
The therapeutic approach consists of surgery as the first-line therapy. When patients refuse surgery or it is contraindicated or when a relapse occurs, other therapeutic options including medical therapy, radiotherapy or bilateral adrenalectomy should be evaluated [19,20]. Medical therapy mainly consists of drugs directly inhibiting pituitary ACTH secretion, such as pasireotide and cabergoline, or adrenal steroidogenesis inhibitors such as metyrapone, ketoconazole, osilodrostat, mitotane and etomidate [21,22]. Another medical drug is the glucocorticoid receptor (GR) antagonist mifepristone, which impairs cortisol binding to GR and mainly acts on clinical comorbidities [23]. However, obtaining remission in CS is not always possible and sometimes it is necessary to combine the treatment options. In addition, these patients tend to show the metabolic comorbidities for a long time, sometimes even in the remission phase, and therefore a nutritional approach to improve metabolism should be started.
Nutrition and Cushing’s Syndrome
Generally speaking, patients with CS need a low sodium, high-protein and high-calcium diet to prevent muscle and bone loss, respectively. However, an interesting and complex relationship exists between diet macronutrients and cortisol [24].
Meal macronutrients have a strong influence on cortisol concentrations, reducing or increasing their levels [25,26,27,28]. Long-standing studies have shown that fasting and starvation are associated with an increase in serum, salivary and urinary free cortisol levels and inadequate suppression of cortisol after a low dose dexamethasone test [29,30,31,32]. However, to what degree caloric restriction cortisol levels increased was not ascertained in any study [33,34].
The sympathetic nervous system (SNS) and hypothalamic–pituitary–adrenal axis (HPA) are strictly involved in stress management. An unhealthy behaviour (consumption of highly rich carbohydrate food, chronic stress and reduced sleep) may stimulate cortisol secretion with the development of obesity in subjects who are predisposed for it [35]. By contrast, calorie-restricted diets inducing a decrease in cortisol values are associated with weight loss and reduced chronic inflammation [36].
There are a few clinical studies evaluating the effects of calorie restriction on cortisol levels.
Stimson et al. evaluated the effects of a high-fat/low-carb diet vs. a moderate-fat/moderate-carb diet on cortisol metabolism in obese men [37]. They showed that a lower carb diet was able to regenerate cortisol by increasing the enzyme 11-β-hydroxysteroid dehydrogenase type 1 (11β-HSD1) that activates cortisol and reducing the enzymes (5-alpha and 5-beta reductase) that inactivate cortisol. Other improvements seen in the lower carb group were greater weight loss and improvements in glucose and insulin levels. The regeneration of cortisol in the low-carb group was independent of the difference in caloric intake between the low-carb and the high-carb group, meaning that the number of calories consumed was not a factor in the positive changes seen; rather, it was the carb ratio in the diet that made the difference.
Another study by the same authors showed that dietary macronutrients have different effects on cortisol production [38]. They conducted a study on eight lean men and observed the effects of carbohydrate, high-protein and fat meals on insulin and cortisol levels, showing that all these meals stimulate a rise in cortisol levels, in different ways. Indeed, carbohydrates stimulate both the adrenal cortisol secretion and the extra-adrenal cortisol regeneration mediated by 11β-HSD1, which is present in the liver, adipose tissue and brain, and regenerate cortisol from cortisone releasing it into the bloodstream. By contrast, high-protein and fat meals stimulate adrenal cortisol secretion to a greater degree than extra-adrenal regeneration. The extra-adrenal cortisol regeneration is strictly related to the increase in insulin levels.
Interestingly, a meta-analysis conducted on 13 studies analysed the effects of fasting, a very low-calorie diet (VLCD) and a low-calorie diet (LCD) on serum cortisol levels [39]. This meta-analysis only included studies that evaluated serum cortisol levels, while it excluded those based on salivary or urinary cortisol levels, in order to avoid heterogeneity of the studies. The results of the meta-analysis showed that short-term calorie restriction was more associated with an increase in cortisol values, compared to a VLCD and LCD, which, in turn, had no long-term effects on serum cortisol values and were less stressful than fasting. In addition, carbohydrate restriction was associated with a decrease in insulin concentration, leading to extra-adrenal cortisol synthesis [39].
Furthermore, some amino acids, such as tryptophan, can lead to a decrease in cortisol levels [40]. Similarly, supplementation with phospholipids at the dose of at least 400 mg/day also results in a reduction in cortisol levels [41]. In addition, other nutrients including vitamin B6 and B12, folic acid, lithium, taurine, fermented milk products and sprouts of brown rice, barley and beans, which stimulate the GABAergic system, in turn, can reduce the secretion of CRH, leading to a decrease in cortisol levels [24,41,42,43].
3. Ketogenic Diet
The ketogenic diet (KD) was used for the first time for the treatment of epilepsy in 1921 [44]. Its use was proposed to mimic the effects of fasting. The KD is a high-fat, low carbohydrate, normocaloric diet. It is characterized by a 4:1 ratio of fat to protein, plus carbohydrates and about 90% of calories are provided by fats (Table 1). In the scenario of the use of a KD, we can identify some variants, the low-calorie ketogenic diet (LCKD) with a calorie intake of 800–1200 Kcal/day and the very-low-calorie ketogenic diet (VLCKD) with a calorie intake of less than 800 Kcal/day (Table 1) [45].
Biochemistry of Ketogenesis
The process of ketogenesis depends on a reduction in glucose intake and the production of ketone bodies, to boost the mechanisms of the beta-oxidation of fatty acids [46]. The biochemical process takes place in the liver (also to a small extent in the kidney), and becomes very intense in conditions of reduced glucose availability, such as fasting, or in certain pathological conditions, such as diabetes mellitus, due to the lack of antiketogenic activity of the hormone insulin. Metabolism in these circumstances is predominantly dependent on the oxidation of fatty acids from the catabolism of storage lipids.
From a biochemical point of view, the process depends on the inhibition of the glycolytic pathway, which normally guarantees an adequate share of pyruvate and oxaloacetate, used in the Krebs cycle [47]. Under conditions of a lack of glucose, pyruvate and oxaloacetate are used as substrates in hepatic gluconeogenesis to ensure adequate blood glucose levels. By contrast, fatty acids are transported into mitochondria via carnitine palmitoyltransferase (CPT-1), and then broken down into acetyl-coenzyme-A (CoA) by beta-oxidation. The mechanism by which an adequate amount of CoA is ensured is through the reaction between the excess acetyl-CoA molecules that accumulate in the mitochondria, resulting in condensation reactions. Ketogenesis then starts, leading to the formation of ketone bodies: acetoacetate, beta-hydroxybutyrate and acetone [48]. The most important enzyme in this process is beta-hydroxy-methylglutaryl-CoA synthetase.
The process of ketogenesis is regulated at three levels: free fatty acid production, the hepatic flow of free fatty acids towards esterification or beta-oxidation and the regulation of acetyl-CoA towards oxidation in the Krebs cycle or condensation in ketogenesis. The most important of these steps is regulation of the circulating free fatty acids. These can be regarded as the precursors of ketone bodies. The intensity of ketogenesis is closely related to the proportion of circulating free fatty acids, mainly from adipose tissue. Endocrine and metabolic factors that regulate lipolysis also regulate ketogenesis. Adrenaline, glucagon and pituitary hormones stimulate both lipolysis and ketogenesis, while insulin inhibits the formation of ketone bodies [49].
The ketone bodies produced can be used by the heart, muscle and brain for oxidative purposes, to obtain energy [50]. The kidney can also use ketone bodies to a small extent, although in this case they are mainly eliminated in the urine.
Under healthy conditions, with an adequate intake of carbohydrate-containing foods, the proportion of plasma ketone bodies is 0.3–2 mg/100 mL. If hepatic production exceeds peripheral utilization capacity, a condition of accumulation in the blood (ketosis) occurs, with increased elimination of ketone bodies in the urine (ketonuria). Ketosis, given the acid nature of ketone bodies, can develop into ketoacidosis, one of the most serious complications of type 1 diabetes mellitus [51]. However, ketoacidosis only occurs in conditions of a severe lack of glucose or total insulinopenia since the body has homeostatic pH maintenance activities such as an increased production of NH4+ ammonium ions and bicarbonates to prevent the evolution towards acidosis [52].
We can define the state of ketosis induced by ketogenesis as ‘controlled’ or physiological ketosis, in which the pH is not altered. Furthermore, in healthy individuals, the increase in circulating ketone bodies stimulates increased insulin secretion, which on the one hand inhibits hepatic ketogenesis and the mobilization of free fatty acids from adipose tissue, and on the other hand promotes the increased elimination of ketone bodies through urine.
Ketosis is also promoted by a sedentary lifestyle. Exercise leads to the increased muscular production of enzymes (thiophorase and acetoacetyl-CoA thiolase), which promote the uptake of ketone bodies [53]. During fasting, or during a VLCKD, glycaemic levels are maintained in a normal range thanks to the glucostatic function of the liver, both through mobilization from the hepatic glycogen reserve and through the process of gluconeogenesis. Low levels of exogenous glucose lead to a reduction in the amount of insulin produced by the pancreas, and an increase in the production of glucagon, responsible for activating enzyme glycogen phosphorylase, which is essential for the production of glucose from glycogen. In this condition, if peripheral tissues were to use only glucose from the liver, glycogen reserves would be rapidly depleted, so the various organs direct their metabolism towards alternative energy sources, such as ketones. This metabolic shift is caused not only by a reduction in the share of exogenous glucose intake, but also by a reduction in the insulin/glucagon ratio and increased production of adrenaline, which result in the reduced inhibition of lipolysis in adipose tissue. This leads to an increase in the levels of circulating free fatty acids and the enhanced beta-oxidation of fatty acids, which in turn activates ketogenesis [53]. Ketogenesis, whether under conditions of prolonged fasting or glucose deficiency, is a saving mechanism that limits the depletion of glycogen reserves. Some tissues in ketosis mainly use ketone bodies, thus saving glucose and ensuring a reserve for noble, glucose-dependent organs. The sparing effect is not only on glucose metabolism but also on amino acid catabolism since ketosis leads to an inhibition of alpha-keto acid dehydrogenase from the transamination of branched amino acids [54]. The degradation of muscle proteins is therefore counteracted. Triiodothyronine activity is also reduced, leading to a reduction in basal metabolism and protein degradation. A ketogenic diet, however, normally guarantees a protein intake greater than the minimum requirements.
4. VLCKD
A VLCKD is characterized by, approximately, a 44–43–13% ratio of lipids, proteins and carbohydrates, respectively, and the total energy intake is less than or equal to 800 kcal [55,56,57,58,59,60].
In a VLCKD, the process of using ketone bodies as an energy source derived from fatty acids is much more intense, with increased use of these energy sources by tissues such as the heart, kidney, skeletal muscle and central nervous system. Physiologically, acetyl-CoA fuses with oxaloacetate derived from glycolytic processes. Under conditions of slowed glycolysis, such as during a VLCKD, the oxaloacetate produced is preferentially used for neoglucogenetic processes, while the cetyl-CoA molecules derived from the beta-oxidation of fatty acids are used for the production of ketone bodies. The VLCKD is the model with the greatest availability of acetyl-CoA [61,62].
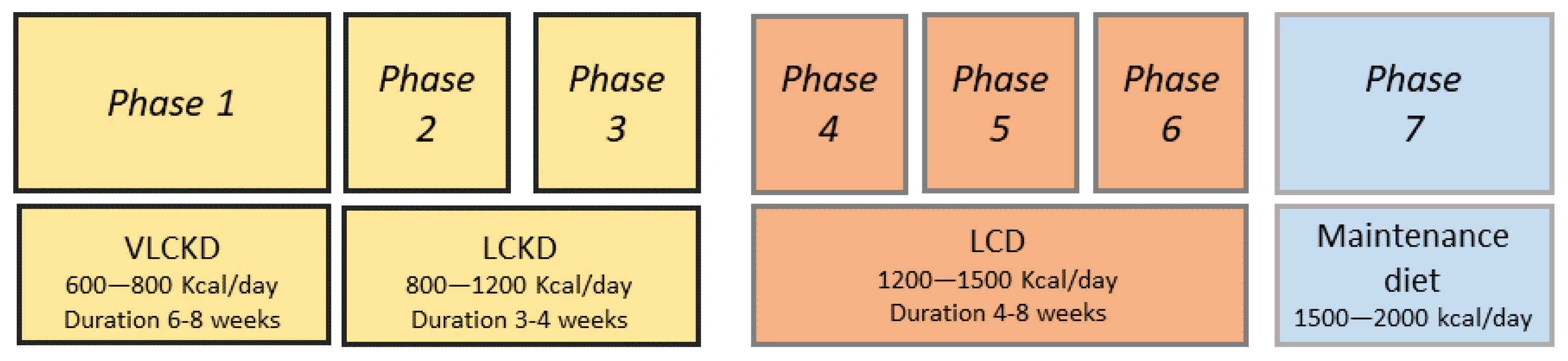
A VLCKD plan is normally divided into several phases, with an initial pure ketogenic period of 6–8 weeks (Figure 1).
Protein preparations containing 18 g of proteins, 4 g of carbohydrates and 3 g of fats may be used initially, but these are gradually discontinued with the introduction of natural protein foods. In phase 1 of the VLCKD, patients are educated to eat high biological value protein preparations five times a day and vegetables with a low glycaemic index. In phase 2, natural proteins including meat/egg/fish are introduced in place of one of the protein preparations at lunch or dinner. In phase 3, natural proteins are introduced in place of the second protein preparation. At the end of the VLCKD, carbohydrates are gradually reintroduced, starting with foods with a lower glycaemic index including fruit and milk products (Phase 4), followed by foods with a moderate glycaemic index such as legumes (Phase 5) and a high glycaemic index (bread, pasta and cereals—Phase 6). This dietetic plan corresponds to an LCD with a daily calorie intake ranging from 1200 to 1500 Kcal/day. At the end of phases 4–6, the patient must be re-educated in order to be able to have a maintenance diet of approximately 1500–2000 Kcal/day and avoid regaining lost weight [58,63].
In a VLCKD, insulin levels are reduced, while glucagon levels increase, and after a few days, circulating levels of free fatty acids and ketone bodies rise. The success of a VLCKD depends not only on the anorectic power of ketone bodies but also on the contribution of certain hormones produced in higher concentrations, such as neuropeptide Y, cholecystokinin and ghrelin. In addition, carbohydrate reduction leads to the rapid consumption of hepatic triglycerides and increased intrahepatic beta-oxidation [64].
4.1. Indications and Contraindications of VLCKD
A VLCKD is mainly known for fast weight loss due to the anorectic power of ketone bodies, which reduce the sense of hunger and prevent environmental factors leading to dietary failure. Weight loss can also be optimally achieved by other dietary therapy models, but some indications for the use of the VLCKD include obesity (BMI ≥ 30 kg/m2), overweight with metabolic complications (BMI ranging from 25 to 29.9 kg/m2) and type 2 diabetes mellitus [65,66,67,68]. Other indications include dyslipidaemia, polycystic ovary syndrome (PCOS), metabolic syndrome and non-endocrine disorders such as asthma, epilepsy, some neurodegenerative disorders, obstructive sleep apnoea syndrome and locomotor system disorders [6,69,70,71,72]. In addition, a VLCKD may be indicated in the pre-operative phase, both for bariatric surgery and for other types of surgery requiring rapid weight loss [73]. In these conditions, adjusting protein requirements promotes weight loss by preventing immune function deficits through protein intake control.
Finally, a further use of this dietary model concerns competitive sporting activity since an increased protein intake allows muscle mass to be maintained and performance to be improved.
Equally important are the contraindications to the VLCKD, which currently include type 1 diabetes mellitus, chronic kidney disease, where the protein intake must be adjusted to the renal function parameters, severe hepatic failure due to the predominant beta-oxidation of fatty acids in the liver, cardiac insufficiency, previous stroke, pregnancy and lactation, active neoplasms, severe psychiatric disorders, developmental age and elderly people (relative contraindication) [74,75,76].
4.2. Adverse Events of VLCKD
The VLCKD establishes a state of controlled ketosis. This dietary model requires medical monitoring both at the start of the dietary plan, by means of a careful clinical history and assessment of the subject’s state of health, and during the course of the dietary therapy, in order to avoid vitamin deficiencies or electrolyte imbalances that may be associated with the loss of ketone bodies in the urine. This diet may give rise to certain transitory side-effects, such as headaches (due to an increase in circulating ketone bodies), which can be managed by taking analgesic drugs, and halitosis [77]. Other effects are orthostatic hypotension, tachycardia, dehydration, hypoglycaemia, constipation, diarrhoea, nausea, urolithiasis, gallstones, hyperuricemia and muscle weakness [78,79,80,81,82]. The elimination of negatively charged ketone bodies in the urine results in an increased passive loss of positively charged ions such as sodium. This is one of the main reasons why the VLCKD is not suitable in cases of severe heart failure. Supplements of calcium, selenium, zinc, vitamin D and oral alkalis can reduce the incidence of nutritional deficiencies and kidney stones [83]. H2-blockers or proton pump inhibitors may be prescribed to prevent gastrointestinal dysmotility and gastroesophageal reflux [79]. In addition, high-fibre vegetables, sufficient fluids and, if necessary, carbohydrate-free laxatives are recommended to overcome constipation.
4.3. VLCKD and Cushing’s Syndrome
Little is known about the effects of a VLCKD on cortisol levels. Indeed, a VLCKD causing a decrease in glucose values may result in an acute increase in cortisol levels to counteract hypoglycaemia stimulating the gluconeogenesis process [83]. However, a prolonged state of ketosis may probably determine a balanced secretion of cortisol, without significant increases. A diet full of high glycaemic index foods can generate a stress condition in the body and favour the deposition of visceral fat and cortisol secretion, leading to a vicious circle. By contrast, a balanced diet has been reported to change body composition and reduce chronic inflammation, acting on cortisol secretion.
A recent study conducted in 30 obese males showed a significant decrease in salivary cortisol after 8 weeks of a VLCKD compared to the baseline [36]. In addition, these authors suggested that a VLCKD was associated with a significant decrease in serum cortisol by reducing cortisol-binding proteins.
Although currently the mechanisms associated with a reduction in serum cortisol values during VLCKD are not fully known, we may hypothesize that a VLCKD, by reducing visceral fat, lowers the expression of 11β-HSD1, mainly expressed in visceral adipose tissue, that catalyses the conversion of corticosterone in cortisol and enhances the 11β-HSD2 that inactivates the cortisol in cortisone.
Currently, there are no clinical studies evaluating the effects of a VLCKD in patients with CS. However, we hypothesize that a VLCKD may be an effective treatment strategy for CS comorbidities including obesity, diabetes mellitus, cardiovascular disease, dyslipidaemia, PCOS and chronic inflammation. Indeed, a VLCKD induces weight loss, reducing visceral fat, by lowering appetite [84] and lipogenesis and increasing lipolysis [85,86]. A VLCKD reduces glucose and insulin levels, improving insulin sensitivity and leading to an improvement in glycaemic control for patients with type 2 diabetes mellitus and an improvement in gonadal function in women (PCOS) [87,88,89,90].
Ketogenesis is associated with a reduction in blood pressure values, which can be attributed in part to the natriuretic effect of ketone bodies [91]. Controlled ketogenesis, which leads to a reduction in excess myocardial lipid content and is also involved in the pharmacodynamic processes of some therapies, is a favourable mechanism for cardiovascular health. In this context, it is important to mention inhibitors of renal sodium-glucose co-transporter type 2 (SGLT2-inhibitors), which, in addition to causing natriuresis and glycosuria, promote a shift towards ketogenesis and a 38% decrease in cardiovascular mortality [92]. The process of ketogenesis has recently been investigated as one of the possible mechanisms associated with the success of SGLT-2 inhibitors on cardiovascular health. Some of these effects appear to be related to the inhibitory action of ketone bodies on the sympathetic nervous system [93]. These effects are metabolic adaptation mechanisms related to the pharmacological induction of glycosuria. In particular, empagliflozin has been shown to promote an increase in endogenous glucose production in response to glycosuria, an increase in lipolysis, fatty acid beta-oxidation and ketogenesis, demonstrated by measuring circulating beta-hydroxy-butyrate levels [94,95].
5. Conclusions
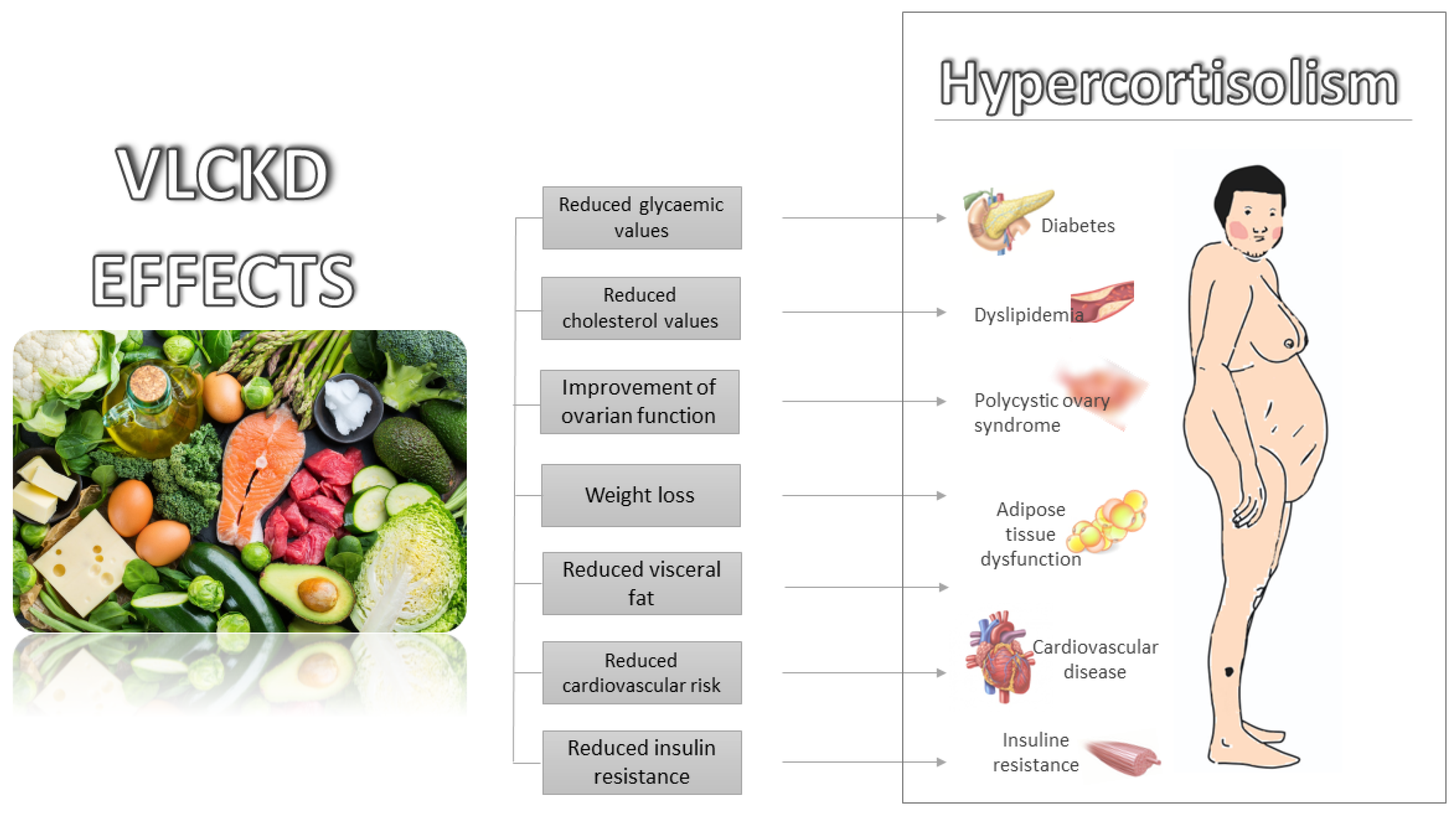
It is currently widely known that a VLCKD has beneficial effects on obesity, diabetes mellitus, cardiovascular disease and the improvement of insulin resistance. All these conditions are present in patients with CS. Currently, there are no clinical studies on the use of a VLCKD in patients with hypercortisolism for the treatment of its comorbidities. However, based on the above-mentioned metabolic favourable effects of a VLCKD, it can be hypothesized that it may be successfully employed for the treatment of CS comorbidities (Figure 2).
To confirm our hypotheses, prospective larger studies on the use of a VLCKD in patients with CS should be performed.
Author Contributions
Conceptualization, V.G., F.E. and R.A.; investigation, V.G. and F.E.; writing—original draft preparation, V.G., F.E. and R.A.; writing—review and editing, V.G. and C.G.; supervision, C.G.; project administration, C.G. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
We thank Gailor for the revision of the language.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Kirkpatrick, C.F.; Bolick, J.P.; Kris-Etherton, P.M.; Sikand, G.; Aspry, K.E.; Soffer, D.E.; Willard, K.E.; Maki, K.C. Review of current evidence and clinical recommendations on the effects of low-carbohydrate and very-low-carbohydrate (including ketogenic) diets for the management of body weight and other cardiometabolic risk factors: A scientific statement from the National Lipid Association Nutrition and Lifestyle Task Force. J. Clin. Lipidol. 2019, 13, 689–711.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muscogiuri, G.; El Ghoch, M.; Colao, A.; Hassapidou, M.; Yumuk, V.; Busetto, L.; Obesity Management Task Force (OMTF) of the European Association for the Study of Obesity (EASO). European Guidelines for Obesity Management in Adults with a Very Low-Calorie Ketogenic Diet: A Systematic Review and Meta-Analysis. Obes. Fact. 2021, 14, 222–245. [Google Scholar] [CrossRef] [PubMed]
- Muscogiuri, G.; Barrea, L.; Laudisio, D.; Pugliese, G.; Salzano, C.; Savastano, S.; Colao, A. The management of very low-calorie ketogenic diet in obesity outpatient clinic: A practical guide. J. Transl. Med. 2019, 17, 356. [Google Scholar] [CrossRef] [PubMed]
- Kolb, H.; Kempf, K.; Röhling, M.; Lenzen-Schulte, M.; Schloot, N.C.; Martin, S. Ketone bodies: From enemy to friend and guardian angel. BMC Med. 2021, 19, 313. [Google Scholar] [CrossRef] [PubMed]
- Boden, G.; Sargrad, K.; Homko, C.; Mozzoli, M.; Stein, T.P. Effect of a low-carbohydrate diet on appetite, blood glucose levels, and insulin resistance in obese patients with type 2 diabetes. Ann. Intern. Med. 2005, 142, 403–411. [Google Scholar] [CrossRef]
- Dashti, H.M.; Mathew, T.C.; Khadada, M.; Al-Mousawi, M.; Talib, H.; Asfar, S.K.; Behbahani, A.I.; Al-Zaid, N.S. Beneficial effects of ketogenic diet in obese diabetic subjects. Mol. Cell. Biochem. 2007, 302, 249–256. [Google Scholar] [CrossRef]
- Gupta, L.; Khandelwal, D.; Kalra, S.; Gupta, P.; Dutta, D.; Aggarwal, S. Ketogenic diet in endocrine disorders: Current perspectives. J. Postgrad. Med. 2017, 63, 242–251. [Google Scholar] [CrossRef]
- Barañano, K.W.; Hartman, A.L. The ketogenic diet: Uses in epilepsy and other neurologic illnesses. Curr. Treat. Options Neurol. 2008, 10, 410–419. [Google Scholar] [CrossRef]
- Thammongkol, S.; Vears, D.F.; Bicknell-Royle, J.; Nation, J.; Draffin, K.; Stewart, K.G.; Ingrid, E.; Scheffer, E.; Mackay, M.T. Efficacy of the ketogenic diet: Which epilepsies respond? Epilepsia 2012, 53, e55–e59. [Google Scholar] [CrossRef]
- Rubini, A.; Bosco, G.; Lodi, A.; Cenci, L.; Parmagnani, A.; Grimaldi, K.; Zhongjin, Y.; Paoli, A. Effects of twenty days of the ketogenic diet on metabolic and respiratory parameters in healthy subjects. Lung 2015, 193, 939–945. [Google Scholar] [CrossRef] [Green Version]
- Pivonello, R.; De Martino, M.C.; Iacuaniello, D.; Simeoli, C.; Muscogiuri, G.; Carlomagno, F.; De Leo, M.; Cozzolino, A.; Colao, A. Metabolic Alterations and Cardiovascular Outcomes of Cortisol Excess. Front. Horm. Res. 2016, 46, 54–56. [Google Scholar] [CrossRef] [PubMed]
- Nieman, L.K. Hypertension and Cardiovascular Mortality in Patients with Cushing Syndrome. Endocrinol. Metab. Clin. N. Am. 2019, 48, 717–725. [Google Scholar] [CrossRef] [PubMed]
- Barbot, M.; Zilio, M.; Scaroni, C. Cushing’s syndrome: Overview of clinical presentation, diagnostic tools and complications. Best Pract. Res. Clin. Endocrinol. Metab. 2020, 34, 101380. [Google Scholar] [CrossRef] [PubMed]
- Giordano, C.; Guarnotta, V.; Pivonello, R.; Amato, M.C.; Simeoli, C.; Ciresi, A.; Cozzolino, A.; Colao, A. Is diabetes in Cushing’s syndrome only a consequence of hypercortisolism? Eur. J. Endocrinol. 2013, 170, 311–319. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ragnarsson, O. Cushing’s syndrome—Disease monitoring: Recurrence, surveillance with biomarkers or imaging studies. Best Pract. Res. Clin. Endocrinol. Metab. 2020, 34, 101382. [Google Scholar] [CrossRef] [PubMed]
- Ferriere, A.; Tabarin, A. Cushing’s syndrome: Treatment and new therapeutic approaches. Best Pract. Res. Clin. Endocrinol. Metab. 2020, 34, 101381. [Google Scholar] [CrossRef] [PubMed]
- Guarnotta, V.; Prinzi, A.; Pitrone, M.; Pizzolanti, G.; Giordano, C. Circulating Irisin Levels as a Marker of Osteosarcopenic-Obesity in Cushing’s Disease. Diabetes Metab. Syndr. Obes. 2020, 13, 1565–1574. [Google Scholar] [CrossRef]
- Braun, L.T.; Vogel, F.; Reincke, M. Long-term morbidity and mortality in patients with Cushing’s syndrome. J. Neuroendocrinol. 2022, 4, e13113. [Google Scholar] [CrossRef]
- Castinetti, F. Medical management of Cushing’s disease: When and how? J. Neuroendocrinol. 2022, 15, e13120. [Google Scholar] [CrossRef]
- Pivonello, R.; Ferrigno, R.; De Martino, M.C.; Simeoli, C.; Di Paola, N.; Pivonello, C.; Barba, L.; Negri, M.; De Angelis, C.; Colao, A. Medical Treatment of Cushing’s Disease: An Overview of the Current and Recent Clinical Trials. Front. Endocrinol. 2020, 11, 648. [Google Scholar] [CrossRef]
- Tritos, N.A. Adrenally Directed Medical Therapies for Cushing Syndrome. J. Clin. Endocrinol. Metab. 2021, 106, 16–25. [Google Scholar] [CrossRef] [PubMed]
- Brown, D.R.; East, H.E.; Eilerman, B.S.; Gordon, M.B.; King, E.E.; Knecht, L.A.; Salke, B.; Samson, S.L.; Yuen, K.C.J.; Yau, H. Clinical management of patients with Cushing syndrome treated with mifepristone: Consensus recommendations. Clin. Diabetes Endocrinol. 2020, 6, 18. [Google Scholar] [CrossRef] [PubMed]
- Stachowicz, M.; Lebiedzińska, A. The effect of diet components on the level of cortisol. Eur. Food Res. Technol. 2016, 242, 2001–2009. [Google Scholar] [CrossRef] [Green Version]
- Lemmens, S.; Born, J.M.; Martens, E.A.; Martens, M.J.; Westerterp Plantenga, M.S. Influence of consumption of a high-protein vs. high-carbohydrate meal on the physiological cortisol and psychological mood response in men and women. PLoS ONE 2011, 6, e16826. [Google Scholar] [CrossRef] [PubMed]
- Peeters, F.; Nicholson, N.A.; Berkhof, J. Cortisol responses to daily events in major depressive disorder. Psychosom. Med. 2003, 65, 836–841. [Google Scholar] [CrossRef] [Green Version]
- Martens, M.J.; Rutters, F.; Lemmens, S.G.; Born, J.M.; Westerterp-Plantenga, M.S. Effects of single macronutrients on serum cortisol concentrations in normal weight men. Physiol. Behav. 2010, 101, 563–567. [Google Scholar] [CrossRef]
- Bray, G.A.; Most, M.; Rood, J.; Redmann, S.; Smith, S.R. Hormonal responses to a fast-food meal compared with nutritionally comparable meals of different composition. Ann. Nutr. Metab. 2007, 51, 163–171. [Google Scholar] [CrossRef]
- Galvao-Teles, A.; Graves, L.; Burke, C.W.; Fotherby, K.; Fraser, R. Free cortisol in obesity; effect of fasting. Acta Endocrinol. 1976, 81, 321–329. [Google Scholar] [CrossRef]
- Edelstein, C.K.; Roy-Byrne, P.; Fawzy, F.I.; Dornfeld, L. Effects of weight loss on the dexamethasone suppression test. Am. J. Psychiatry 1983, 140, 338–341. [Google Scholar] [CrossRef]
- Berger, M.P.K.; Doerr, P.; Krieg, C.; von Zersseen, D. Influence of weight loss on the dexamethasone suppression test. Arch. Gen. Psychiatry 1983, 19, 585–586. [Google Scholar] [CrossRef]
- Tomiyama, A.J.; Mann, T.; Vinas, D.; Hunger, J.M.; Dejager, J.; Taylor, S.E. Low calorie dieting increases cortisol. Psychosom. Med. 2010, 72, 357–364. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dubuc, G.R.; Phinney, S.D.; Stern, J.S.; Havel, P.J. Changes of serum leptin and endocrine and metabolic parameters after 7 days of energy restriction in men and women. Metab. Clin. Exp. 1998, 47, 429–434. [Google Scholar] [CrossRef] [Green Version]
- Pasiakos, S.M.; Caruso, C.M.; Kellogg, M.D.; Kramer, F.M.; Lieberman, H.R. Appetite and endocrine regulators of energy balance after 2 days of energy restriction: Insulin, leptin, ghrelin, and DHEA-S. Obesity 2011, 19, 1124–1130. [Google Scholar] [CrossRef] [PubMed]
- van der Valk, E.S.; Savas, M.; van Rossum, E.F.C. Stress and obesity: Are there more susceptible individuals? Curr. Obes. Rep. 2018, 7, 193–203. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valenzano, A.; Polito, R.; Trimigno, V.; Di Palma, A.; Moscatelli, F.; Corso, G.; Sessa, F.; Salerno, M.; Montana, A.; Di Nunno, N.; et al. Effects of very low calorie ketogenic diet on the orexinergic system, visceral adipose tissue, and ROS production. Antioxidants 2019, 8, 643. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Polito, R.; Messina, G.; Valenzano, A.; Scarinci, A.; Villano, I.; Monda, M.; Cibelli, G.; Porro, C.; Pisanelli, D.; Monda, V.; et al. The Role of Very Low Calorie Ketogenic Diet in Sympathetic Activation through Cortisol Secretion in Male Obese Population. J. Clin. Med. 2021, 10, 4230. [Google Scholar] [CrossRef]
- Stimson, R.H.; Johnstone, A.M.; Homer, N.Z.; Wake, D.J.; Morton, N.M.; Andrew, R.; Lobley, G.E.; Walker, B.R. Dietary macronutrient content alters cortisol metabolism independently of body weight changes in obese men. J. Clin. Endocrinol. Metab. 2007, 92, 4480–4484. [Google Scholar] [CrossRef] [Green Version]
- Stimson, R.H.; Mohd-Shukri, N.A.; Bolton, J.L.; Andrew, R.; Reynolds, R.M.; Walker, B.R. The postprandial rise in plasma cortisol in men is mediated by macronutrient-specific stimulation of adrenal and extra-adrenal cortisol production. J. Clin. Endocrinol. Metab. 2014, 99, 160–168. [Google Scholar] [CrossRef] [Green Version]
- Nakamura, Y.; Walker, B.R.; Ikuta, T. Systematic review and meta-analysis reveals acutely elevated plasma cortisol following fasting but not less severe calorie restriction. Stress 2016, 19, 151–157. [Google Scholar] [CrossRef]
- Capello, A.E.; Marcus, C.R. Effect of sub chronic tryptophan supplementation on stress-induced cortisol and appetite in subjects differing in 5-HTTLPR genotype and trait neuroticism. Psychoneuroendocrinology 2014, 45, 96–107. [Google Scholar] [CrossRef]
- Starks, M.A.; Starks, S.L.; Kingsley, M.; Purpura, M.; Jager, R. The effects of phosphatidylserine on endocrine response to moderate intensity exercise. J. Int. Soc. Sports Nutr. 2008, 5, 11–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miklos, I.H.; Kovacs, K.J. GABAergic innervation of corticotropin-releasing hormone (CRH)-secreting parvocellular neurons and its plasticity as demonstrated by quantitative immunoelectron micorscopy. Neuroscience 2002, 113, 581–592. [Google Scholar] [CrossRef]
- Song, Z.; Hatton, G.I. Taurine and the control of basal hor mone release from rat neurophysis. Exp. Neurol. 2003, 183, 330–337. [Google Scholar] [CrossRef]
- Wilder, R.M. The effects of ketonemia on the course of epilepsy. Mayo Clin. Proc. 1921, 2, 307–308. [Google Scholar]
- Sukkar, S.G.; Muscaritoli, M. A Clinical Perspective of Low Carbohydrate Ketogenic Diets: A Narrative Review. Front. Nutr. 2021, 8, 642628. [Google Scholar] [CrossRef]
- Leonard, T. The physiology of ketosis and the ketogenic diet. S. Afr. J. Anaesth. Analg. 2020, 26, S94–S97. [Google Scholar] [CrossRef]
- Dhillon, K.K.; Gupta, S. Biochemistry, Ketogenesis. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Jensen, N.J.; Wodschow, H.Z.; Nilsson, M. Effects of ketone bodies on brain metabolism and function in neurodegenerative diseases. Int. J. Mol. Sci. 2020, 21, 8767. [Google Scholar] [CrossRef]
- Williams, M.S.; Turos, E. The Chemistry of the Ketogenic Diet: Updates and Opportunities in Organic Synthesis. Int. J. Mol. Sci. 2021, 22, 5230. [Google Scholar] [CrossRef]
- Fedorovich, S.V.; Voronina, P.P.; Waseem, T.V. Ketogenic diet versus ketoacidosis: What determines the influence of ketone bodies on neurons? Neural Regen. Res. 2018, 13, 2060–2063. [Google Scholar] [CrossRef]
- Kanikarla-Marie, P.; Jain, S.K. Hyperketonemia and ketosis increase the risk of complications in type 1 diabetes. Free Radic. Biol. Med. 2016, 95, 268–277. [Google Scholar] [CrossRef] [Green Version]
- Ashtary-Larky, D.; Bagheri, R.; Bavi, H.; Baker, J.; Moro, T.; Mancin, L.; Paoli, A. Ketogenic diets, physical activity, and body composition: A review. Br. J. Nutr. 2021, 2021, 1–68. [Google Scholar] [CrossRef] [PubMed]
- Longo, R.; Peri, C.; Cricrì, D.; Coppi, L.; Caruso, D.; Mitro, N.; De Fabiani, E.; Crestani, M. Ketogenic Diet: A New Light Shining on Old but Gold Biochemistry. Nutrients 2019, 11, 2497. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yudkoff, M.; Daikhin, Y.; Nissim, I.; Horyn, O.; Lazarow, A.; Luhovyy, B.; Wehrli, S.; Nissim, I. Response of brain amino acid metabolism to ketosis. Neurochem. Int. 2005, 47, 119–128. [Google Scholar] [CrossRef] [PubMed]
- Abbasi, J. Interest in the ketogenic diet grows for weight loss and type 2 diabetes. JAMA 2018, 319, 215–217. [Google Scholar] [CrossRef]
- Merra, G.; Gratteri, S.; De Lorenzo, A.; Barrucco, S.; Perrone, M.A.; Avolio, E.; Bernardini, S.; Marchetti, M.; Di Renzo, L. Effects of very-low-calorie diet on body composition, metabolic state, and genes expression: A randomized double-blind placebo-controlled trial. Eur. Rev. Med. Pharmacol. Sci. 2017, 21, 329–345. [Google Scholar]
- Paoli, A.; Rubini, A.; Volek, J.S.; Grimaldi, K.A. Beyond weight loss: A review of the therapeutic uses of very-low-carbohydrate (ketogenic) diets. Eur. J. Clin. Nutr. 2013, 67, 789–796. [Google Scholar] [CrossRef] [Green Version]
- Cicero, A.F.; Benelli, M.; Brancaleoni, M.; Dainelli, G.; Merlini, D.; Negri, R. Middle and long-term impact of a very low-carbohydrate ketogenic diet on cardiometabolic factors: A multi-center, cross-sectional, clinical study. High Blood Press Cardiovasc. Prev. 2015, 22, 389–394. [Google Scholar] [CrossRef] [Green Version]
- Merra, G.; Miranda, R.; Barrucco, S.; Gualtieri, P.; Mazza, M.; Moriconi, E.; Marchetti, M.; Chang, T.F.M.; De Lorenzo, A.; Di Renzo, L. Very-low-calorie ketogenic diet with aminoacid supplement versus very low restricted-calorie diet for preserving muscle mass during weight loss: A pilot double-blind study. Eur. Rev. Med. Pharmacol. Sci. 2016, 20, 2613–2621. [Google Scholar]
- Antonio, J.; Ellerbroek, A.; Silver, T.; Vargas, L.; Tamayo, A.; Buehn, R.; Peacock, C.A. A high protein diet has no harmful efects: A oneyear crossover study in resistance-trained males. J. Nutr. Metab. 2016, 2016, 9104792. [Google Scholar] [CrossRef] [Green Version]
- Lafel, L. Ketone bodies: A review of physiology, pathophysiology and application of monitoring to diabetes. Diabetes Metab. Res. Rev. 1999, 15, 412–426. [Google Scholar] [CrossRef]
- McPherson, P.A.; McEneny, J. The biochemistry of ketogenesis and its role in weight management, neurological disease and oxidative stress. J. Physiol. Biochem. 2012, 68, 141–151. [Google Scholar] [CrossRef] [PubMed]
- Dehghan, M.; Mente, A.; Zhang, X.; Swaminathan, S.; Li, W.; Mohan, V.; Iqbal, R.; Kumar, R.; Wentzel-Viljoen, E.; Rosengren, A.; et al. Associations of fats and carbohydrate intake with cardiovascular disease and mortality in 18 countries from five continents (PURE): A prospective cohort study. Lancet 2017, 390, 2050–2062. [Google Scholar] [CrossRef] [Green Version]
- Currenti, W.; Galvano, F. Very low-calorie ketogenic diet (VLCKD): Indicazioni ed efficacia nel trattamento dell’obesità. L’Endocrinologo 2020, 21, 458–463. [Google Scholar] [CrossRef]
- Casanueva, F.F.; Castellana, M.; Bellido, D.; Trimboli, P.; Castro, A.I.; Sajoux, I.; Rodriguez-Carnero, G.; Gomez-Arbelaez, D.; Crujeiras, A.B.; Martinez-Olmos, M.A. Ketogenic diets as treatment of obesity and type 2 diabetes mellitus. Rev. Endocr. Metab. Disord. 2020, 21, 381–397. [Google Scholar] [CrossRef] [PubMed]
- Williams, K.V.; Mullen, M.L.; Kelley, D.E.; Wing, R.R. The effect of short periods of caloric restriction on weight loss and glycemic control in type 2 diabetes. Diabetes Care 1998, 21, 2–8. [Google Scholar] [CrossRef]
- Finnish Diabetes Association. Development Programme for the Prevention and Care of Diabetes in Finland 2000–2010. Tampere. FDA 2001. Available online: http://www.diabetes.fi/english/programme/programme/index.html (accessed on 2 May 2022).
- Capstick, F.; Brooks, B.A.; Burns, C.M.; Zilkens, R.R.; Steinbeck, K.S.; Yue, D.K. Very low calorie diet (VLCD): A useful alternative in the treatment of the obese NIDDM patient. Diabetes Res. Clin. Pract. 1997, 36, 105–111. [Google Scholar] [CrossRef]
- Alsharairi, N.A. The Role of Short-Chain Fatty Acids in the Interplay between a Very Low-Calorie Ketogenic Diet and the Infant Gut Microbiota and Its Therapeutic Implications for Reducing Asthma. Int. J. Mol. Sci. 2020, 21, 9580. [Google Scholar] [CrossRef]
- Gough, S.M.; Casella, A.; Ortega, K.J.; Hackam, A.S. Neuroprotection by the Ketogenic Diet: Evidence and Controversies. Front. Nutr. 2021, 8, 782657. [Google Scholar] [CrossRef]
- Schiavo, L.; Pierro, R.; Asteria, C.; Calabrese, P.; Di Biasio, A.; Coluzzi, I.; Severino, L.; Giovanelli, A.; Pilone, V.; Silecchia, G. Low-Calorie Ketogenic Diet with Continuous Positive Airway Pressure to Alleviate Severe Obstructive Sleep Apnea Syndrome in Patients with Obesity Scheduled for Bariatric/Metabolic Surgery: A Pilot, Prospective, Randomized Multicenter Comparative Study. Obes. Surg. 2021, 32, 634–642. [Google Scholar] [CrossRef]
- Li, R.J.; Liu, Y.; Liu, H.Q.; Li, J. Ketogenic diets and protective mechanisms in epilepsy, metabolic disorders, cancer, neuronal loss, and muscle and nerve degeneration. J. Food Biochem. 2020, 44, e13140. [Google Scholar] [CrossRef]
- Pekkarinen, T.; Mustajoki, P. Use of very low calorie diet in preoperative weight loss: Efficacy and safety. Obes. Res. 1997, 5, 595–602. [Google Scholar] [CrossRef] [PubMed]
- Willi, S.M.; Martin, K.; Datko, F.M.; Brant, B.P. Treatment of type 2 diabetes in childhood using a very-low-calorie diet. Diabetes Care 2004, 27, 48–53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zwiauer, K.; Schmidinger, H.; Klicpera, M.; Mayr, H.; Widhalm, K. 24-hours electrocardiographic monitoring in obese children and adolescents during a 3 week low calorie diet (500 kcal). Int. J. Obes. 1989, 13, 101–105. [Google Scholar] [PubMed]
- Watanabe, M.; Tuccinardi, D.; Ernesti, I.; Basciani, S.; Mariani, S.; Genco, A.; Manfrini, S.; Lubrano, C.; Gnessi, L. Scientific evidence underlying contraindications to the ketogenic diet: An update. Obes. Rev. 2020, 21, e13053. [Google Scholar] [CrossRef] [PubMed]
- Musa-Veloso, K.; Likhodii, S.S.; Cunnane, S.C. Breath acetone is a reliable indicator of ketosis in adults consuming ketogenic meals. Am. J. Clin. Nutr. 2002, 76, 65–70. [Google Scholar] [CrossRef] [PubMed]
- Kang, H.C.; Chung, D.E.; Kim, D.W.; Kim, H.D. Early- and late-onset complications of the ketogenic diet for intractable epilepsy. Epilepsia 2004, 45, 1116–1123. [Google Scholar] [CrossRef]
- Kossoff, E.H.; Zupec-Kania, B.A.; Amark, P.E.; Ballaban-Gil, K.R.; Christina Bergqvist, A.G.; Blackford, R.; Buchhalter, J.R.; Caraballo, R.H.; Cross, J.H.; Dahlin, M.G.; et al. Optimal clinical management of children receiving dietary therapies for epilepsy: Updated recommendations of the International Ketogenic Diet Study Group. Epilepsia 2018, 3, 175–192. [Google Scholar] [CrossRef]
- Atkinson, R.L. Low and very low calorie diets. Med. Clin. N. Am. 1989, 73, 203–215. [Google Scholar] [CrossRef]
- Kielb, S.; Koo, H.P.; Bloom, D.A.; Faerber, G.J. Nephrolithiasis associated with the ketogenic diet. J. Urol. 2000, 164, 464–466. [Google Scholar] [CrossRef]
- Everhart, J.E. Contributions of obesity and weight loss to gallstone disease. Ann. Intern. Med. 1993, 119, 1029–1035. [Google Scholar] [CrossRef]
- Masino, S.A.; Rho, J.M. Mechanisms of ketogenic diet action. In Jasper’s Basic Mechanisms of the Epilepsies, 4th ed.; Noebels, J.L., Avoli, M., Rogawski, M.A., Olsen, R.W., Delgado-Escueta, A.V., Eds.; National Center for Biotechnology Information: Bethesda, MD, USA, 2012. [Google Scholar]
- Sumithran, P.; Prendergast, L.A.; Delbridge, E.; Purcell, K.; Shulkes, A.; Kriketos, A.; Proietto, J. Ketosis and appetite-mediating nutrients and hormones after weight loss. Eur. J. Clin. Nutr. 2013, 67, 759–764. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, Z.; Mi, J.; Wang, Y.; Xue, L.; Liu, J.; Fan, M.; Zhang, D.; Wang, L.; Qian, H.; Li, Y. Effects of low-carbohydrate diet and ketogenic diet on glucose and lipid metabolism in type 2 diabetic mice. Nutrition 2021, 89, 111230. [Google Scholar] [CrossRef] [PubMed]
- Ma, S.; Huang, Q.; Tominaga, T.; Liu, C.; Suzuki, K. An 8-week ketogenic diet alternated interleukin-6, ketolytic and lipolytic gene expression, and enhanced exercise capacity in mice. Nutrients 2018, 10, 1696. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, Y.; Qiao, J. Association of Insulin Resistance and Elevated Androgen Levels with Polycystic Ovarian Syndrome (PCOS): A Review of Literature. J. Healthc. Eng. 2022, 2022, 9240569. [Google Scholar] [CrossRef] [PubMed]
- Mavropoulos, J.C.; Yancy, W.S.; Hepburn, J.; Westman, E.C. The effects of a low-carbohydrate, ketogenic diet on the polycystic ovary syndrome: A pilot study. Nutr. Metab. 2005, 2, 35. [Google Scholar] [CrossRef] [Green Version]
- Gower, B.A.; Chandler-Laney, P.C.; Ovalle, F.; Goree, L.L.; Azziz, R.; Desmond, R.A.; Granger, W.M.; Goss, A.M.; Bates, G.W. Favourable metabolic effects of a eucaloric lower-carbohydrate diet in women with PCOS. Clin. Endocrinol. 2013, 79, 550–557. [Google Scholar] [CrossRef] [Green Version]
- Paoli, A.; Mancin, L.; Giacona, M.C.; Bianco, A.; Caprio, M. Effects of a ketogenic diet in overweight women with polycystic ovary syndrome. J. Transl. Med. 2020, 18, 104. [Google Scholar] [CrossRef]
- Khan, S.S.; Ning, H.; Wilkins, J.T.; Allen, N.; Carnethon, M.; Berry, J.D.; Sweis, R.N.; Lloyd-Jones, D.M. Association of body mass index with lifetime risk of cardiovascular disease and compression of morbidity. JAMA Cardiol. 2018, 3, 280–287. [Google Scholar] [CrossRef]
- Palgi, A.; Read, J.L.; Greenberg, I.; Hoefer, M.A.; Bistrian, B.R.; Blackburn, G.L. Multidisciplinary treatment of obesity with a protein-sparing modified fast: Results in 668 outpatients. Am. J. Public Health 1985, 75, 1190–1194. [Google Scholar] [CrossRef] [Green Version]
- Yancy, W.S.; Westman, E.C.; McDuffie, J.R.; Grambow, S.C.; Jeffreys, A.S.; Bolton, J.; Chalecki, A.; Oddone, E.Z. A randomized trial of a low carbohydrate diet vs orlistat plus a low-fat diet for weight loss. Arch. Intern. Med. 2010, 170, 136–145. [Google Scholar] [CrossRef] [Green Version]
- Ferrannini, E.; Baldi, S.; Frascerra, S.; Astiarraga, B.; Heise, T.; Bizzotto, R.; Mari, A.; Pieber, T.M.; Muscelli, E. Shift to fatty substrate utilization in response to sodium-glucose cotransporter 2 inhibition in subjects without diabetes and patients with type 2 diabetes. Diabetes 2016, 65, 1190–1195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kimura, I.; Inoue, D.; Maeda, T.; Hara, T.; Ichimura, A.; Miyauchi, S.; Kobayashi, M.; Hirasawa, A.; Tsujimoto, G. Short-chain fatty acids and ketones directly regulate sympathetic nervous system via G protein-coupled receptor 41 (GPR41). Proc. Natl. Acad. Sci. USA 2011, 108, 8030–8035. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pietschner, R.; Kolwelter, J.; Bosch, A.; Striepe, K.; Jung, S.; Kannenkeril, D.; Ott, C.; Schiffer, M.; Achenbach, S.; Schmieder, R.E. Effect of empagliflozin on ketone bodies in patients with stable chronic heart failure. Cardiovasc. Diabetol. 2021, 20, 219. [Google Scholar] [CrossRef] [PubMed]
- Monda, V.; Polito, R.; Lovino, A.; Finaldi, A.; Valenzano, A.; Nigro, E.; Corso, G.; Sessa, F.; Asmundo, A.; Nunno, N.D.; et al. Short-Term Physiological Effects of a Very Low-Calorie Ketogenic Diet: Effects on Adiponectin Levels and Inflammatory States. Int. J. Mol. Sci. 2020, 21, 3228. [Google Scholar] [CrossRef]
- Forsythe, C.E.; Phinney, S.D.; Fernandez, M.L.; Quann, E.E.; Wood, R.J.; Bibus, D.M.; Kraemer, W.J.; Feinman, R.D.; Volek, J.S. Comparison of low fat and low carbohydrate diets on circulating fatty acid composition and markers of inflammation. Lipids 2008, 43, 65–77. [Google Scholar] [CrossRef]
Figure 1.
Phases of very low-calorie ketogenic diet (VLCKD) protocol. LCKD: low-calorie ketogenic diet. LCD: low carbohydrate diet.
Figure 1.
Phases of very low-calorie ketogenic diet (VLCKD) protocol. LCKD: low-calorie ketogenic diet. LCD: low carbohydrate diet.

Figure 2.
Metabolic effects of VLCKD and potential applications in Cushing’s syndrome comorbidities.
Figure 2.
Metabolic effects of VLCKD and potential applications in Cushing’s syndrome comorbidities.


{kind=link}
{kind=link}
Table 1.
Characteristics of classical ketogenic diet (KD), low-calorie ketogenic diet (LCKD) and very low-calorie ketogenic diet (VLCKD).
Table 1.
Characteristics of classical ketogenic diet (KD), low-calorie ketogenic diet (LCKD) and very low-calorie ketogenic diet (VLCKD).
| KD | LCKD | VLCKD | |
|---|---|---|---|
| Caloric intake | Normocaloric | 800–1200 Kcal/day | <800 Kcal/day |
| Carbohydrate (%) | 5–10 | 13 | 13 |
| Protein (%) | 15–20 | 29 | 44 |
| Fat (%) | 70–80 | 58 | 43 |
| Foods | Vegetable oils, fish, eggs, meat, cheese, olives, avocado, coconut | Natural high biological value proteins (1–2 servings) including meat, fish, eggs, processed meat | Replacement meals with high biological value proteins composed by 18 g of proteins, 4 g of carbohydrates and 3 g of fats |
| Recommendations for use [1] |
|
|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Guarnotta, V.; Emanuele, F.; Amodei, R.; Giordano, C. Very Low-Calorie Ketogenic Diet: A Potential Application in the Treatment of Hypercortisolism Comorbidities. Nutrients 2022, 14, 2388. https://doi.org/10.3390/nu14122388
AMA Style
Guarnotta V, Emanuele F, Amodei R, Giordano C. Very Low-Calorie Ketogenic Diet: A Potential Application in the Treatment of Hypercortisolism Comorbidities. Nutrients. 2022; 14(12):2388. https://doi.org/10.3390/nu14122388
Chicago/Turabian StyleGuarnotta, Valentina, Fabrizio Emanuele, Roberta Amodei, and Carla Giordano. 2022. "Very Low-Calorie Ketogenic Diet: A Potential Application in the Treatment of Hypercortisolism Comorbidities" Nutrients 14, no. 12: 2388. https://doi.org/10.3390/nu14122388
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.