
Breakfast Consumption May Improve Fasting Insulin, HOMA-IR, and HbA1c Levels in Predominately Low-Income, Hispanic Children 7–12 Years of Age


 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
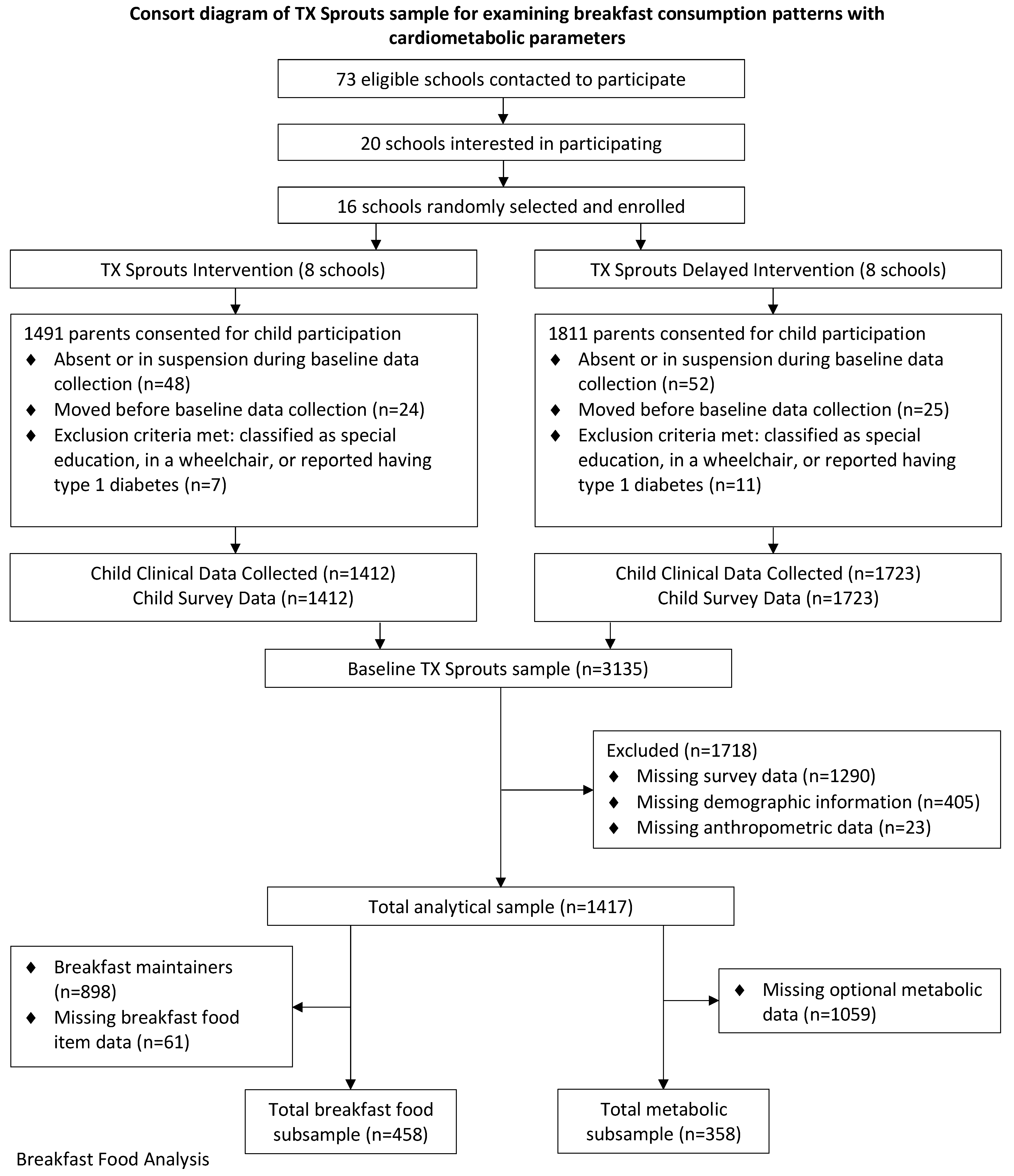
2.1. Study Design
2.2. TX Sprouts Intervention
2.3. Recruitment
2.4. Survey Measurements
2.5. Anthropometric and Physiological Measurements at Baseline and Post-Intervention
2.6. Metabolic Measurements at Baseline and Post-Intervention
2.7. Participants
2.8. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fryar, C.; Carroll, M.; Ogden, C. Prevalence of Overweight, Obesity, and Severe Obesity among Children and Adolescents Aged 2–19 Years. Available online: https://www.cdc.gov/nchs/data/hestat/obesity-child-17-18/obesity-child.htm#Suggested%20citation (accessed on 9 May 2022).
- Kopelman, P. Health risks associated with overweight and obesity. Obes. Rev. 2007, 8 (Suppl. 1), 13–17. [Google Scholar] [CrossRef] [PubMed]
- Caprio, S.; Santoro, N.; Weiss, R. Childhood obesity and the associated rise in cardiometabolic complications. Nat. Metab. 2020, 2, 223–232. [Google Scholar] [CrossRef]
- Apovian, C.M. Obesity: Definition, comorbidities, causes, and burden. Am. J. Manag. Care 2016, 22, s176–s185. [Google Scholar] [PubMed]
- Rao, W.W.; Zong, Q.Q.; Zhang, J.W.; An, F.R.; Jackson, T.; Ungvari, G.S.; Xiang, Y.; Su, Y.Y.; D’Arcy, C.; Xiang, Y.T. Obesity increases the risk of depression in children and adolescents: Results from a systematic review and meta-analysis. J. Affect. Disord. 2020, 267, 78–85. [Google Scholar] [CrossRef] [PubMed]
- Wijnhoven, T.M.; van Raaij, J.M.; Yngve, A.; Sjoberg, A.; Kunesova, M.; Duleva, V.; Petrauskiene, A.; Rito, A.I.; Breda, J. WHO European Childhood Obesity Surveillance Initiative: Health-risk behaviours on nutrition and physical activity in 6–9-year-old schoolchildren. Public Health Nutr. 2015, 18, 3108–3124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mustafa, A.E.M.; Assery, A.A.A.; Asiri, F.M.A.; Alfarhan, N.M.; Alqarni, A.M.; Alqahtani, F.M.S. Childhood obesity and its relation with dietary habits among children in Aseer region, Southern Saudi Arabia. J. Family Med. Prim. Care 2021, 10, 3760–3764. [Google Scholar] [CrossRef] [PubMed]
- Rampersaud, G.C.; Pereira, M.A.; Girard, B.L.; Adams, J.; Metzl, J.D. Breakfast habits, nutritional status, body weight, and academic performance in children and adolescents. J. Am. Diet. Assoc. 2005, 105, 743–760. [Google Scholar] [CrossRef]
- Gimenez-Legarre, N.; Flores-Barrantes, P.; Miguel-Berges, M.L.; Moreno, L.A.; Santaliestra-Pasias, A.M. Breakfast Characteristics and Their Association with Energy, Macronutrients, and Food Intake in Children and Adolescents: A Systematic Review and Meta-Analysis. Nutrients 2020, 12, 2460. [Google Scholar] [CrossRef]
- Patterson, K.A.E.; Ferrar, K.; Gall, S.L.; Venn, A.J.; Blizzard, L.; Dwyer, T.; Cleland, V.J. Cluster patterns of behavioural risk factors among children: Longitudinal associations with adult cardio-metabolic risk factors. Prev. Med. 2020, 130, 105861. [Google Scholar] [CrossRef]
- Monzani, A.; Ricotti, R.; Caputo, M.; Solito, A.; Archero, F.; Bellone, S.; Prodam, F. A Systematic Review of the Association of Skipping Breakfast with Weight and Cardiometabolic Risk Factors in Children and Adolescents. What Should We Better Investigate in the Future? Nutrients 2019, 11, 387. [Google Scholar] [CrossRef] [Green Version]
- Deshmukh-Taskar, P.; Nicklas, T.A.; Radcliffe, J.D.; O’Neil, C.E.; Liu, Y. The relationship of breakfast skipping and type of breakfast consumed with overweight/obesity, abdominal obesity, other cardiometabolic risk factors and the metabolic syndrome in young adults. The National Health and Nutrition Examination Survey (NHANES): 1999–2006. Public Health Nutr. 2013, 16, 2073–2082. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kupers, L.K.; de Pijper, J.J.; Sauer, P.J.; Stolk, R.P.; Corpeleijn, E. Skipping breakfast and overweight in 2- and 5-year-old Dutch children-the GECKO Drenthe cohort. Int. J. Obes. 2014, 38, 569–571. [Google Scholar] [CrossRef] [PubMed]
- Wijtzes, A.I.; Jansen, W.; Bouthoorn, S.H.; van Lenthe, F.J.; Franco, O.H.; Hofman, A.; Jaddoe, V.W.V.; Raat, H. Meal-Skipping Behaviors and Body Fat in 6-Year-Old Children. J. Pediatr. 2016, 168, 118–125.e2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ricotti, R.; Caputo, M.; Monzani, A.; Pigni, S.; Antoniotti, V.; Bellone, S.; Prodam, F. Breakfast Skipping, Weight, Cardiometabolic Risk, and Nutrition Quality in Children and Adolescents: A Systematic Review of Randomized Controlled and Intervention Longitudinal Trials. Nutrients 2021, 13, 3331. [Google Scholar] [CrossRef] [PubMed]
- Terry, A.L.; Wambogo, E.; Ansai, N.; Ahluwalia, N. Breakfast Intake among Children and Adolescents: United States, 2015–2018. NCHS Data Brief 2020, 386, 1–8. [Google Scholar]
- Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z. The metabolic syndrome. Lancet 2005, 365, 1415–1428. [Google Scholar] [CrossRef]
- Kit, B.K.; Kuklina, E.; Carroll, M.D.; Ostchega, Y.; Freedman, D.S.; Ogden, C.L. Prevalence of and trends in dyslipidemia and blood pressure among US children and adolescents, 1999–2012. JAMA Pediatr. 2015, 169, 272–279. [Google Scholar] [CrossRef] [Green Version]
- Centers for Disease Control and Prevention. National Diabetes Statistics Report, 2020; Centers for Disease Control and Prevention, US Department of Health and Human Services: Atlanta, GA, USA, 2020. [Google Scholar]
- Goran, M.I.; Lane, C.; Toledo-Corral, C.; Weigensberg, M.J. Persistence of pre-diabetes in overweight and obese Hispanic children: Association with progressive insulin resistance, poor beta-cell function, and increasing visceral fat. Diabetes 2008, 57, 3007–3012. [Google Scholar] [CrossRef] [Green Version]
- Kanjilal, S.; Gregg, E.W.; Cheng, Y.J.; Zhang, P.; Nelson, D.E.; Mensah, G.; Beckles, G.L. Socioeconomic status and trends in disparities in 4 major risk factors for cardiovascular disease among US adults, 1971–2002. Arch. Intern. Med. 2006, 166, 2348–2355. [Google Scholar] [CrossRef] [Green Version]
- Puolakka, E.; Pahkala, K.; Laitinen, T.T.; Magnussen, C.G.; Hutri-Kahonen, N.; Tossavainen, P.; Jokinen, E.; Sabin, M.A.; Laitinen, T.; Elovainio, M.; et al. Childhood Socioeconomic Status in Predicting Metabolic Syndrome and Glucose Abnormalities in Adulthood: The Cardiovascular Risk in Young Finns Study. Diabetes Care 2016, 39, 2311–2317. [Google Scholar] [CrossRef] [Green Version]
- Chung, A.; Backholer, K.; Wong, E.; Palermo, C.; Keating, C.; Peeters, A. Trends in child and adolescent obesity prevalence in economically advanced countries according to socioeconomic position: A systematic review. Obes. Rev. 2016, 17, 276–295. [Google Scholar] [CrossRef] [PubMed]
- Leidy, H.J.; Hoertel, H.A.; Douglas, S.M.; Higgins, K.A.; Shafer, R.S. A high-protein breakfast prevents body fat gain, through reductions in daily intake and hunger, in “Breakfast skipping” adolescents. Obesity 2015, 23, 1761–1764. [Google Scholar] [CrossRef] [PubMed]
- Jeans, M.R.; Asigbee, F.M.; Landry, M.J.; Vandyousefi, S.; Ghaddar, R.; Leidy, H.J.; Davis, J.N. Breakfast Consumption in Low-Income Hispanic Elementary School-Aged Children: Associations with Anthropometric, Metabolic, and Dietary Parameters. Nutrients 2020, 12, 2038. [Google Scholar] [CrossRef] [PubMed]
- Davis, J.N.; Perez, A.; Asigbee, F.M.; Landry, M.J.; Vandyousefi, S.; Ghaddar, R.; Hoover, A.; Jeans, M.; Nikah, K.; Fischer, B.; et al. School-based gardening, cooking and nutrition intervention increased vegetable intake but did not reduce BMI: Texas sprouts—A cluster randomized controlled trial. Int. J. Behav. Nutr. Phys. Act. 2021, 18, 18. [Google Scholar] [CrossRef]
- Landry, M.J.; van den Berg, A.E.; Hoelscher, D.M.; Asigbee, F.M.; Vandyousefi, S.; Ghaddar, R.; Jeans, M.R.; Waugh, L.; Nikah, K.; Sharma, S.V.; et al. Impact of a School-Based Gardening, Cooking, Nutrition Intervention on Diet Intake and Quality: The TX Sprouts Randomized Controlled Trial. Nutrients 2021, 13, 3081. [Google Scholar] [CrossRef] [PubMed]
- Davis, J.; Nikah, K.; Asigbee, F.M.; Landry, M.J.; Vandyousefi, S.; Ghaddar, R.; Hoover, A.; Jeans, M.; Pont, S.J.; Richards, D.; et al. Design and participant characteristics of TX sprouts: A school-based cluster randomized gardening, nutrition, and cooking intervention. Contemp. Clin. Trials 2019, 85, 105834. [Google Scholar] [CrossRef]
- Cicchetti, D.; Lynch, M. Toward an ecological/transactional model of community violence and child maltreatment: Consequences for children’s development. Psychiatry 1993, 56, 96–118. [Google Scholar] [CrossRef]
- Corder, K.; van Sluijs, E.M.; Steele, R.M.; Stephen, A.M.; Dunn, V.; Bamber, D.; Goodyer, I.; Griffin, S.J.; Ekelund, U. Breakfast consumption and physical activity in British adolescents. Br. J. Nutr. 2011, 105, 316–321. [Google Scholar] [CrossRef] [Green Version]
- Evans, A.; Ranjit, N.; Hoelscher, D.; Jovanovic, C.; Lopez, M.; McIntosh, A.; Ory, M.; Whittlesey, L.; McKyer, L.; Kirk, A.; et al. Impact of school-based vegetable garden and physical activity coordinated health interventions on weight status and weight-related behaviors of ethnically diverse, low-income students: Study design and baseline data of the Texas, Grow! Eat! Go! (TGEG) cluster-randomized controlled trial. BMC Public Health 2016, 16, 973. [Google Scholar] [CrossRef] [Green Version]
- Centers for Disease Control and Prevention. Anthropometry Procedures Manual; CDC: Atlanta, GA, USA, 2007. [Google Scholar]
- Centers for Disease Control and Prevention. Clinical Growth Charts; CDC: Atlanta, GA, USA, 2000. [Google Scholar]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis model assessment: Insulin resistance and ?-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef] [Green Version]
- Friedewald, W.T.; Levy, R.I.; Fredrickson, D.S. Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin. Chem. 1972, 18, 499–502. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. Diagnosis and classification of diabetes mellitus. Diabetes Care 2014, 37 (Suppl. 1), S81–S90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jeans, M.R.; Landry, M.J.; Asigbee, F.M.; Vandyousefi, S.; Ghaddar, R.; Bray, M.S.; Leidy, H.J.; Davis, J.N. Comparison of School vs. Home Breakfast Consumption with Cardiometabolic and Dietary Parameters in Low-Income, Multi-Racial/Ethnic Elementary School-Aged Children. J. Acad. Nutr. Diet. 2021, 122, 833–847. [Google Scholar] [CrossRef] [PubMed]
- DeBoer, M.D.; Dong, L.; Gurka, M.J. Racial/ethnic and sex differences in the ability of metabolic syndrome criteria to predict elevations in fasting insulin levels in adolescents. J. Pediatr. 2011, 159, 975–981.e3. [Google Scholar] [CrossRef] [Green Version]
- Landry, M.J.; Khazaee, E.; Markowitz, A.K.; Vandyousefi, S.; Ghaddar, R.; Pilles, K.; Asigbee, F.M.; Gatto, N.M.; Davis, J.N. Impact of food security on glycemic control among low-income primarily Hispanic/Latino children in Los Angeles, California: A cross-sectional study. J. Hunger. Environ. Nutr. 2019, 14, 709–724. [Google Scholar] [CrossRef]
- Smith, K.J.; Gall, S.L.; McNaughton, S.A.; Blizzard, L.; Dwyer, T.; Venn, A.J. Skipping breakfast: Longitudinal associations with cardiometabolic risk factors in the Childhood Determinants of Adult Health Study. Am. J. Clin. Nutr. 2010, 92, 1316–1325. [Google Scholar] [CrossRef]
- Marlatt, K.L.; Farbakhsh, K.; Dengel, D.R.; Lytle, L.A. Breakfast and fast food consumption are associated with selected biomarkers in adolescents. Prev. Med. Rep. 2016, 3, 49–52. [Google Scholar] [CrossRef] [Green Version]
- Farshchi, H.R.; Taylor, M.A.; Macdonald, I.A. Deleterious effects of omitting breakfast on insulin sensitivity and fasting lipid profiles in healthy lean women. Am. J. Clin. Nutr. 2005, 81, 388–396. [Google Scholar] [CrossRef] [Green Version]
- Arslanian, S.; Kim, J.Y.; Nasr, A.; Bacha, F.; Tfayli, H.; Lee, S.; Toledo, F.G.S. Insulin sensitivity across the lifespan from obese adolescents to obese adults with impaired glucose tolerance: Who is worse off? Pediatr. Diabetes 2018, 19, 205–211. [Google Scholar] [CrossRef]
- Tagi, V.M.; Giannini, C.; Chiarelli, F. Insulin Resistance in Children. Front. Endocrinol. 2019, 10, 342. [Google Scholar] [CrossRef] [Green Version]
- Sherwani, S.I.; Khan, H.A.; Ekhzaimy, A.; Masood, A.; Sakharkar, M.K. Significance of HbA1c Test in Diagnosis and Prognosis of Diabetic Patients. Biomark. Insights 2016, 11, 95–104. [Google Scholar] [CrossRef] [PubMed]
- Khaw, K.T.; Wareham, N.; Luben, R.; Bingham, S.; Oakes, S.; Welch, A.; Day, N. Glycated haemoglobin, diabetes, and mortality in men in Norfolk cohort of european prospective investigation of cancer and nutrition (EPIC-Norfolk). BMJ 2001, 322, 15–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Donin, A.S.; Nightingale, C.M.; Owen, C.G.; Rudnicka, A.R.; Perkin, M.R.; Jebb, S.A.; Stephen, A.M.; Sattar, N.; Cook, D.G.; Whincup, P.H. Regular Breakfast Consumption and Type 2 Diabetes Risk Markers in 9- to 10-Year-Old Children in the Child Heart and Health Study in England (CHASE): A Cross-Sectional Analysis. PLoS Med. 2014, 11, e1001703. [Google Scholar] [CrossRef] [PubMed]
- Jakubowicz, D.; Barnea, M.; Wainstein, J.; Froy, O. High caloric intake at breakfast vs. dinner differentially influences weight loss of overweight and obese women. Obesity 2013, 21, 2504–2512. [Google Scholar] [CrossRef]
- Chowdhury, E.A.; Richardson, J.D.; Holman, G.D.; Tsintzas, K.; Thompson, D.; Betts, J.A. The causal role of breakfast in energy balance and health: A randomized controlled trial in obese adults. Am. J. Clin. Nutr. 2016, 103, 747–756. [Google Scholar] [CrossRef]
- Jakubowicz, D.; Barnea, M.; Wainstein, J.; Froy, O. Effects of caloric intake timing on insulin resistance and hyperandrogenism in lean women with polycystic ovary syndrome. Clin. Sci. 2013, 125, 423–432. [Google Scholar] [CrossRef] [Green Version]
- US Department of Agriculture, Agricultural Research Service. Percentages of Selected Nutrients Contributed by Food and Beverages Consumed at Breakfast, by Race/Ethnicity and Age. In What We Eat in America NHANES 2017–2018; Food Surveys Research Group: Beltsville, MD, USA, 2017. [Google Scholar]
- Poggiogalle, E.; Jamshed, H.; Peterson, C.M. Circadian regulation of glucose, lipid, and energy metabolism in humans. Metabolism 2018, 84, 11–27. [Google Scholar] [CrossRef] [Green Version]
- Sato, M.; Nakamura, K.; Ogata, H.; Miyashita, A.; Nagasaka, S.; Omi, N.; Yamaguchi, S.; Hibi, M.; Umeda, T.; Nakaji, S.; et al. Acute effect of late evening meal on diurnal variation of blood glucose and energy metabolism. Obes. Res. Clin. Pract. 2011, 5, e169–e266. [Google Scholar] [CrossRef]
- Bandin, C.; Scheer, F.A.; Luque, A.J.; Avila-Gandia, V.; Zamora, S.; Madrid, J.A.; Gomez-Abellan, P.; Garaulet, M. Meal timing affects glucose tolerance, substrate oxidation and circadian-related variables: A randomized, crossover trial. Int. J. Obes. 2015, 39, 828–833. [Google Scholar] [CrossRef]
- Merten, M.J.; Williams, A.L.; Shriver, L.H. Breakfast consumption in adolescence and young adulthood: Parental presence, community context, and obesity. J. Am. Diet. Assoc. 2009, 109, 1384–1391. [Google Scholar] [CrossRef]
- Leatherdale, S.T.; Stefanczyk, J.M.; Kirkpatrick, S.I. School Breakfast-Club Program Changes and Youth Eating Breakfast During the School Week in the COMPASS Study. J. Sch. Health 2016, 86, 568–577. [Google Scholar] [CrossRef] [PubMed]
- O’Dea, J.A.; Wagstaff, S. Increased breakfast frequency and nutritional quality among schoolchildren after a national breakfast promotion campaign in Australia between 2000 and 2006. Health Educ. Res. 2011, 26, 1086–1096. [Google Scholar] [CrossRef] [PubMed]
- Ritchie, L.D.; Rosen, N.J.; Fenton, K.; Au, L.E.; Goldstein, L.H.; Shimada, T. School Breakfast Policy Is Associated with Dietary Intake of Fourth- and Fifth-Grade Students. J. Acad. Nutr. Diet. 2016, 116, 449–457. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Traub, M.; Lauer, R.; Kesztyus, T.; Wartha, O.; Steinacker, J.M.; Kesztyus, D.; Research Group Join the Healthy, B. Skipping breakfast, overconsumption of soft drinks and screen media: Longitudinal analysis of the combined influence on weight development in primary schoolchildren. BMC Public Health 2018, 18, 363. [Google Scholar] [CrossRef]
- Bauer, K.W.; Foster, G.D.; Weeks, H.M.; Polonsky, H.M.; Davey, A.; Sherman, S.; Abel, M.L.; Ruth, K.J.; Dale, L.C.; Fisher, J.O. Breakfast in the Classroom Initiative and Students’ Breakfast Consumption Behaviors: A Group Randomized Trial. Am. J. Public Health 2020, 110, 540–546. [Google Scholar] [CrossRef]
- Polonsky, H.M.; Bauer, K.W.; Fisher, J.O.; Davey, A.; Sherman, S.; Abel, M.L.; Hanlon, A.; Ruth, K.J.; Dale, L.C.; Foster, G.D. Effect of a Breakfast in the Classroom Initiative on Obesity in Urban School-aged Children: A Cluster Randomized Clinical Trial. JAMA Pediatr. 2019, 173, 326–333. [Google Scholar] [CrossRef]
- Kobel, S.; Wirt, T.; Schreiber, A.; Kesztyus, D.; Kettner, S.; Erkelenz, N.; Wartha, O.; Steinacker, J.M. Intervention effects of a school-based health promotion programme on obesity related behavioural outcomes. J. Obes. 2014, 2014, 476230. [Google Scholar] [CrossRef]
- Michels, N.; De Henauw, S.; Breidenassel, C.; Censi, L.; Cuenca-Garcia, M.; Gonzalez-Gross, M.; Gottrand, F.; Hallstrom, L.; Kafatos, A.; Kersting, M.; et al. European adolescent ready-to-eat-cereal (RTEC) consumers have a healthier dietary intake and body composition compared with non-RTEC consumers. Eur. J. Nutr. 2015, 54, 653–664. [Google Scholar] [CrossRef] [Green Version]
- Affenito, S.G.; Thompson, D.; Dorazio, A.; Albertson, A.M.; Loew, A.; Holschuh, N.M. Ready-to-eat cereal consumption and the School Breakfast Program: Relationship to nutrient intake and weight. J. Sch. Health 2013, 83, 28–35. [Google Scholar] [CrossRef]
- Albertson, A.M.; Thompson, D.; Franko, D.L.; Kleinman, R.E.; Barton, B.A.; Crockett, S.J. Consumption of breakfast cereal is associated with positive health outcomes: Evidence from the National Heart, Lung, and Blood Institute Growth and Health Study. Nutr. Res. 2008, 28, 744–752. [Google Scholar] [CrossRef]
- Fayet-Moore, F.; Kim, J.; Sritharan, N.; Petocz, P. Impact of Breakfast Skipping and Breakfast Choice on the Nutrient Intake and Body Mass Index of Australian Children. Nutrients 2016, 8, 487. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van den Boom, A.; Serra-Majem, L.; Ribas, L.; Ngo, J.; Perez-Rodrigo, C.; Aranceta, J.; Fletcher, R. The contribution of ready-to-eat cereals to daily nutrient intake and breakfast quality in a Mediterranean setting. J. Am. Coll. Nutr. 2006, 25, 135–143. [Google Scholar] [CrossRef] [PubMed]
- Gimenez-Legarre, N.; Miguel-Berges, M.L.; Flores-Barrantes, P.; Santaliestra-Pasias, A.M.; Moreno, L.A. Breakfast Characteristics and Its Association with Daily Micronutrients Intake in Children and Adolescents-A Systematic Review and Meta-Analysis. Nutrients 2020, 12, 3201. [Google Scholar] [CrossRef] [PubMed]
- Leidy, H.J.; Gwin, J.A.; Roenfeldt, C.A.; Zino, A.Z.; Shafer, R.S. Evaluating the Intervention-Based Evidence Surrounding the Causal Role of Breakfast on Markers of Weight Management, with Specific Focus on Breakfast Composition and Size. Adv. Nutr. 2016, 7, 563S–575S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jakubowicz, D.; Wainstein, J.; Landau, Z.; Ahren, B.; Barnea, M.; Bar-Dayan, Y.; Froy, O. High-energy breakfast based on whey protein reduces body weight, postprandial glycemia and HbA1C in Type 2 diabetes. J. Nutr. Biochem. 2017, 49, 1–7. [Google Scholar] [CrossRef]
- Kung, B.; Anderson, G.H.; Pare, S.; Tucker, A.J.; Vien, S.; Wright, A.J.; Goff, H.D. Effect of milk protein intake and casein-to-whey ratio in breakfast meals on postprandial glucose, satiety ratings, and subsequent meal intake. J. Dairy Sci. 2018, 101, 8688–8701. [Google Scholar] [CrossRef]
- Leidy, H.J.; Ortinau, L.C.; Douglas, S.M.; Hoertel, H.A. Beneficial effects of a higher-protein breakfast on the appetitive, hormonal, and neural signals controlling energy intake regulation in overweight/obese, “breakfast-skipping,” late-adolescent girls. Am. J. Clin. Nutr. 2013, 97, 677–688. [Google Scholar] [CrossRef]
- Hu, X.; Gao, J.; Zhang, Q.; Fu, Y.; Li, K.; Zhu, S.; Li, D. Soy fiber improves weight loss and lipid profile in overweight and obese adults: A randomized controlled trial. Mol. Nutr. Food Res. 2013, 57, 2147–2154. [Google Scholar] [CrossRef]
- Fayet-Moore, F.; McConnell, A.; Tuck, K.; Petocz, P. Breakfast and Breakfast Cereal Choice and Its Impact on Nutrient and Sugar Intakes and Anthropometric Measures among a Nationally Representative Sample of Australian Children and Adolescents. Nutrients 2017, 9, 1045. [Google Scholar] [CrossRef]


{kind=link}
| Variable | Survey Question | Response Options |
|---|---|---|
| Breakfast Consumption [30] | How many school days each week do you typically eat breakfast? | 0–5 (0 = None, 1 = 1 school day, 2 = 2 school days, 3 = 3 school days, 4 = 4 school days, 5 = 5 school days) |
| How many weekend days each week do you typically eat breakfast? | 0–2 (0 = None, 1 = 1 weekend day, 2 = 2 weekend days) | |
| Breakfast Weekday Location [30] | Where do you typically eat breakfast during the school week? (only select one option) | 0–4 (0 = At home (by myself), 1 = At home (with family), 2 = At school (in cafeteria), 3 = At school (in class), 4 = Other |
| Moderate to Vigorous Physical Activity [31] | Yesterday, did you do any moderate to vigorous (very active) physical activities for about 30 min (about the time you get to eat lunch at school) DURING THE DAY? (list of 12 examples) | 0, 1 (0 = No, 1 = Yes) |
| Variable | Total | Maintainers | Decreasers | Increasers | p-Value a |
|---|---|---|---|---|---|
| Sample size (n) | 1417 | 898 | 220 | 299 | |
| Sex (M), n (%) | 753 (53.1) | 475 (33.5) | 117 (8.3) | 161 (11.4) | 0.96 |
| Age (years), mean ± SD | 9.3 ± 0.9 | 9.3 ± 0.9 | 9.3 ± 0.9 | 9.3 ± 0.9 | 0.66 |
| Race and Ethnicity, n (%) | 0.09 | ||||
| Hispanic | 825 (58.2) | 502 (35.4) | 140 (9.9) | 183 (12.9) | |
| Non-Hispanic White | 405 (28.6) | 283 (20.0) | 51 (3.6) | 71 (5.0) | |
| Non-Hispanic Black | 113 (8.0) | 69 (4.9) | 17 (1.2) | 27 (1.9) | |
| Other b | 74 (5.2) | 44 (3.1) | 12 (0.8) | 18 (1.3) | |
| Free/Reduced-Price School Meal, n (%) | 888 (62.7) | 516 (36.4) | 167 (11.8) | 205 (14.5) | <0.001 |
| Breakfast Weekday Location, n(%) | 0.16 | ||||
| Home | 734 (51.8) | 487 (54.2) | 101 (45.9) | 146 (48.8) | |
| School | 628 (44.3) | 379 (42.2) | 110 (50.0) | 139 (46.5) | |
| Other | 55 (3.9) | 32 (3.6) | 9 (4.1) | 14 (4.7) | |
| BMI categories, c n (%) | 0.13 | ||||
| Underweight | 38 (2.7) | 26 (1.8) | 2 (0.1) | 10 (0.7) | |
| Normal | 760 (53.6) | 503 (35.5) | 108 (7.6) | 149 (10.5) | |
| Overweight | 254 (17.9) | 150 (10.6) | 45 (3.2) | 59 (4.2) | |
| Obese | 365 (25.8) | 219 (15.5) | 65 (4.6) | 81 (5.7) |
| Maintainers | Decreasers (D) | Increasers (I) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Variable | Baseline Mean ± SD | Post Mean ± SD | Absolute Change Mean ± SD | Baseline Mean ± SD | Post Mean ± SD | Absolute Change Mean ± SD | Baseline Mean ± SD | Post Mean ± SD | Absolute Change Mean ± SD | p-Value c | Bonferroni |
| Anthropometric parameters d | |||||||||||
| Sample size (n) | 898 | 898 | 898 | 220 | 220 | 220 | 299 | 299 | 299 | ||
| Waist circumference (cm) | 69.5 ± 11.7 | 70.8 ± 12.0 | 1.4 ± 3.7 | 71.8 ± 12.2 | 73.3 ± 12.8 | 1.5 ± 4.2 | 70.7 ± 12.6 | 72.2 ± 13.0 | 1.5 ± 3.4 | 0.50 | -- |
| Total body fat (%) | 24.8 ± 8.5 | 24.3 ± 8.8 | −0.5 ± 2.6 | 26.7 ± 8.8 | 26.4 ± 9.2 | −0.3 ± 3.0 | 26.3 ± 9.1 | 25.8 ± 9.3 | −0.5 ± 3.0 | 0.64 | -- |
| BMIe percentile | 66.7 ± 30.3 | 65.8 ± 30.8 | 0.8 ± 9.3 | 72.4 ± 28.5 | 72.0 ± 29.1 | 0.4 ± 9.1 | 71.5 ± 28.2 | 70.5 ± 28.4 | 1.1 ± 7.9 | 0.88 | -- |
| Physiological parameters f | |||||||||||
| Systolic blood pressure (mmHg) | 102.1 ± 11.3 | 102.4 ± 11.2 | 0.2 ± 11.7 | 103.7 ± 11.5 | 104.4 ± 10.5 | 0.7 ± 12.5 | 103.1 ± 13.4 | 103.3 ± 12.1 | 0.2 ± 12.8 | 0.44 | -- |
| Diastolic blood pressure (mmHg) | 66.3 ± 9.1 | 67.2 ± 9.4 | 0.9 ± 11.1 | 67.4 ± 9.3 | 67.0 ± 7.3 | −0.4 ± 10.4 | 67.3 ± 11.6 | 67.1 ± 10.0 | −0.2 ± 11.5 | 0.43 | -- |
| Metabolic parameters g | |||||||||||
| Sample size (n) | 229 | 229 | 229 | 59 | 59 | 59 | 70 | 70 | 70 | ||
| Fasting glucose (mg/dL) h | 89.8 ± 8.9 | 96.1 ± 9.4 | 6.3 ± 11.3 | 88.6 ± 9.0 | 96.6 ± 9.9 | 8.0 ± 11.4 | 88.1 ± 7.8 | 94.5 ± 9.4 | 6.3 ± 10.7 | 0.07 | -- |
| Insulin (µIU/mL) i | 15.3 ± 11.0 | 15.8 ± 10.3 | 0.6 ± 8.3 | 16.9 ± 12.3 | 21.0 ± 23.9 | 4.1 ± 15.5 | 19.0 ± 17.8 | 18.7 ± 18.4 | −0.3 ± 13.6 | 0.01 | D vs. I, 0.01 |
| HOMA-IR j | 3.4 ± 2.5 | 3.8 ± 2.6 | 0.4 ± 2.2 | 3.7 ± 2.7 | 5.2 ± 6.8 | 1.5 ± 4.9 | 4.1 ± 3.7 | 4.5 ± 4.9 | 0.4 ± 3.5 | 0.007 | D vs. I, 0.006 |
| Cholesterol (mg/dL) k | 149.7 ± 23.2 | 146.7 ± 24.4 | −3.0 ± 18.6 | 150.4 ± 28.6 | 150.9 ± 26.2 | 0.5 ± 17.2 | 156.5 ± 31.9 | 149.3 ± 30.1 | −7.2 ± 14.4 | 0.36 | -- |
| HDL (mg/dL) | 48.9 ± 9.9 | 50.0 ± 10.8 | 1.1 ± 6.6 | 45.0 ± 10.9 | 46.6 ± 10.9 | 1.6 ± 4.9 | 48.6 ± 10.4 | 47.7 ± 10.1 | −0.9 ± 6.0 | 0.25 | -- |
| Non-HDL (mg/dL) | 100.8 ± 21.5 | 96.8 ± 22.0 | −4.0 ± 15.0 | 105.5 ± 25.9 | 104.4 ± 24.2 | −1.1 ± 15.2 | 108.0 ± 29.9 | 101.7 ± 29.1 | −6.3 ± 12.6 | 0.36 | -- |
| LDL (mg/dL) | 83.2 ± 18.1 | 79.1 ± 19.9 | −4.1 ± 14.7 | 84.5 ± 22.0 | 82.8 ± 21.7 | −1.7 ± 14.8 | 87.6 ± 29.0 | 83.1 ± 28.3 | −4.5 ± 11.8 | 0.44 | -- |
| Triglycerides (mg/dL) l | 88.7 ± 41.1 | 88.5 ± 46.2 | −0.2 ± 37.8 | 105.2 ± 49.2 | 108.3 ± 54.1 | 3.0 ± 37.9 | 101.6 ± 50.1 | 93.1 ± 41.9 | −8.5 ± 41.7 | 0.48 | -- |
| HbA1c (%) | 5.2 ± 0.3 | 5.3 ± 0.3 | 0.02 ± 0.2 | 5.2 ± 0.3 | 5.3 ± 0.3 | 0.06 ± 0.2 | 5.2 ± 0.2 | 5.2 ± 0.2 | 0.01 ± 0.2 | 0.12 | -- |
| Variable | Β | 95% CI | p-Value b |
|---|---|---|---|
| Anthropometric c parameters c (n = 1417) | |||
| Waist circumference (cm) | 0.01 | (−0.09, 0.11) | 0.88 |
| Total body fat (%) | −0.02 | (−0.09, 0.06) | 0.67 |
| BMI percentile | −0.09 | (−0.33, 0.15) | 0.34 |
| Systolic blood pressure (mmHg) | −0.08 | (−0.33, 0.18) | 0.56 |
| Diastolic blood pressure (mmHg) | −0.01 | (−0.22, 0.24) | 0.91 |
| Metabolic parameters d (n = 358) | |||
| Fasting glucose (mg/dL) e | −0.42 | (−0.93, 0.08) | 0.10 |
| Insulin (µIU/mL) f | −0.44 | (−1.04, 0.16) | 0.003 |
| HOMA-IR g | −0.11 | (−0.29, 0.06) | 0.002 |
| Cholesterol (mg/dL) h | −0.02 | (−0.96, 0.91) | 0.72 |
| HDL (mg/dL) | −0.23 | (−0.58, 0.11) | 0.22 |
| Non-HDL (mg/dL) | 0.14 | (−0.64, 0.92) | 0.93 |
| LDL (mg/dL) | 0.21 | (−0.55, 0.97) | 0.99 |
| Triglycerides (mg/dL) i | −0.35 | (−2.35, 1.66) | 0.93 |
| HbA1c (%) | −0.01 | (−0.02, −0.001) | 0.03 |
| Decreasers (n = 198) | Increasers (n = 260) | ||||||
|---|---|---|---|---|---|---|---|
| Survey Items | Response n (%) | Response n (%) | p-Value a | ||||
| 0–2 x/Week | 3–4 x/Week | 5–7 x/Week | 0–2 x/Week | 3–4 x/Week | 5–7 x/Week | ||
| Cereal (with milk) | 143 (72.2%) | 29 (14.7%) | 26 (13.1%) | 161 (61.9%) | 53 (20.4%) | 46 (17.7%) | 0.07 |
| Oatmeal | 176 (88.9%) | 16 (8.1%) | 6 (3.0%) | 228 (87.7%) | 19 (7.3%) | 13 (5.0%) | 0.56 |
| Fruit | 117 (59.0%) | 50 (25.3%) | 31 (15.7%) | 145 (55.7%) | 61 (23.5%) | 54 (20.8%) | 0.38 |
| Eggs/meat | 132 (66.7%) | 46 (23.2%) | 20 (10.1%) | 178 (68.4%) | 55 (21.2%) | 27 (10.4%) | 0.50 |
| Breakfast sandwich | 164 (82.9%) | 27 (13.6%) | 7 (3.5%) | 224 (86.1%) | 20 (7.7%) | 16 (6.2%) | 0.06 |
| Milk/yogurt | 146 (73.7%) | 23 (11.6%) | 29 (14.7%) | 190 (73.1%) | 46 (17.7%) | 24 (9.2%) | 0.06 |
| Bread/bagel | 159 (80.3%) | 26 (13.1%) | 13 (6.6%) | 211 (81.1%) | 29 (11.2%) | 20 (7.7%) | 0.75 |
| Pastries/sweets | 157 (79.3%) | 21 (10.6%) | 20 (10.1%) | 201 (77.3%) | 30 (11.5%) | 29 (11.2%) | 0.88 |
| Juice b | 132 (66.6%) | 37 (18.7%) | 29 (14.7%) | 161 (61.9%) | 45 (17.3%) | 54 (20.8%) | 0.24 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jeans, M.R.; Vandyousefi, S.; Landry, M.J.; Leidy, H.J.; Gray, M.J.; Bray, M.S.; Widen, E.M.; Davis, J.N. Breakfast Consumption May Improve Fasting Insulin, HOMA-IR, and HbA1c Levels in Predominately Low-Income, Hispanic Children 7–12 Years of Age. Nutrients 2022, 14, 2320. https://doi.org/10.3390/nu14112320
Jeans MR, Vandyousefi S, Landry MJ, Leidy HJ, Gray MJ, Bray MS, Widen EM, Davis JN. Breakfast Consumption May Improve Fasting Insulin, HOMA-IR, and HbA1c Levels in Predominately Low-Income, Hispanic Children 7–12 Years of Age. Nutrients. 2022; 14(11):2320. https://doi.org/10.3390/nu14112320
Chicago/Turabian StyleJeans, Matthew R., Sarvenaz Vandyousefi, Matthew J. Landry, Heather J. Leidy, Megan J. Gray, Molly S. Bray, Elizabeth M. Widen, and Jaimie N. Davis. 2022. "Breakfast Consumption May Improve Fasting Insulin, HOMA-IR, and HbA1c Levels in Predominately Low-Income, Hispanic Children 7–12 Years of Age" Nutrients 14, no. 11: 2320. https://doi.org/10.3390/nu14112320