
Malnutrition, Sarcopenia, and Malnutrition-Sarcopenia Syndrome in Older Adults with COPD

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
- -
- age 60 years and more,
- -
- COPD diagnosed based on recommendations from the Global Initiative for Chronic Obstructive Lung Disease (GOLD) [1],
- -
- good verbal communication, absence of cognitive impairment,
- -
- absence of active inflammation
- -
- informed, written consent to participate in the study.
- -
- active malignancy,
- -
- contraindications for the body composition analysis with a bioimpedance method (metal implants, implanted cardiac devices, oedemas).
2.1. Assessment of Cognitive Performance
2.2. Assessment of Malnutrition
- (1)
- unintentional body weight loss: the loss of >5% habitual body mass within the past six months, or the loss of >10% in more than six months,
- (2)
- low body mass index (BMI): <20 kg/m2 in subjects below 70 years and <22 kg/m2 in individuals 70 years or older,
- (3)
- low muscle mass (LMM): muscle mass was assessed based on the measurement of appendicular lean mass and calculation of the Appendicular Lean Mass (ALM) and an ALM index, which represents the ratio of ALM (kg) and square of height (m2). ALM index below the cut-off points for the Polish population (5.6 kg/m2 in women and 7.4 kg/m2 in men) [26] was indicative of low muscle mass (LMM).
- (1)
- reduced food intake or assimilation was recognized in subjects declaring any reduction in food intake within the past three months in the MNA-SF questionnaire,
- (2)
- the disease burden/inflammatory condition was recognized in all participants with a COPD diagnosis.
2.3. Assessment of Sarcopenia
2.3.1. Assessment of Muscle Strength
2.3.2. Assessment of the Muscle Mass
2.4. Pulmonary Function Tests—Spirometry
- GOLD 1 (mild obstruction) FEV1 ≥ 80%
- GOLD 2 (moderate obstruction) FEV1 ≥ 50%
- GOLD 3 (severe obstruction) FEV1 ≥ 30%
- GOLD 4 (very severe obstruction) FEV1 < 30%
2.5. Exercise Capacity
2.6. Statistical Analysis
3. Results
3.1. Characteristics of the Study Population
3.2. Malnutrition
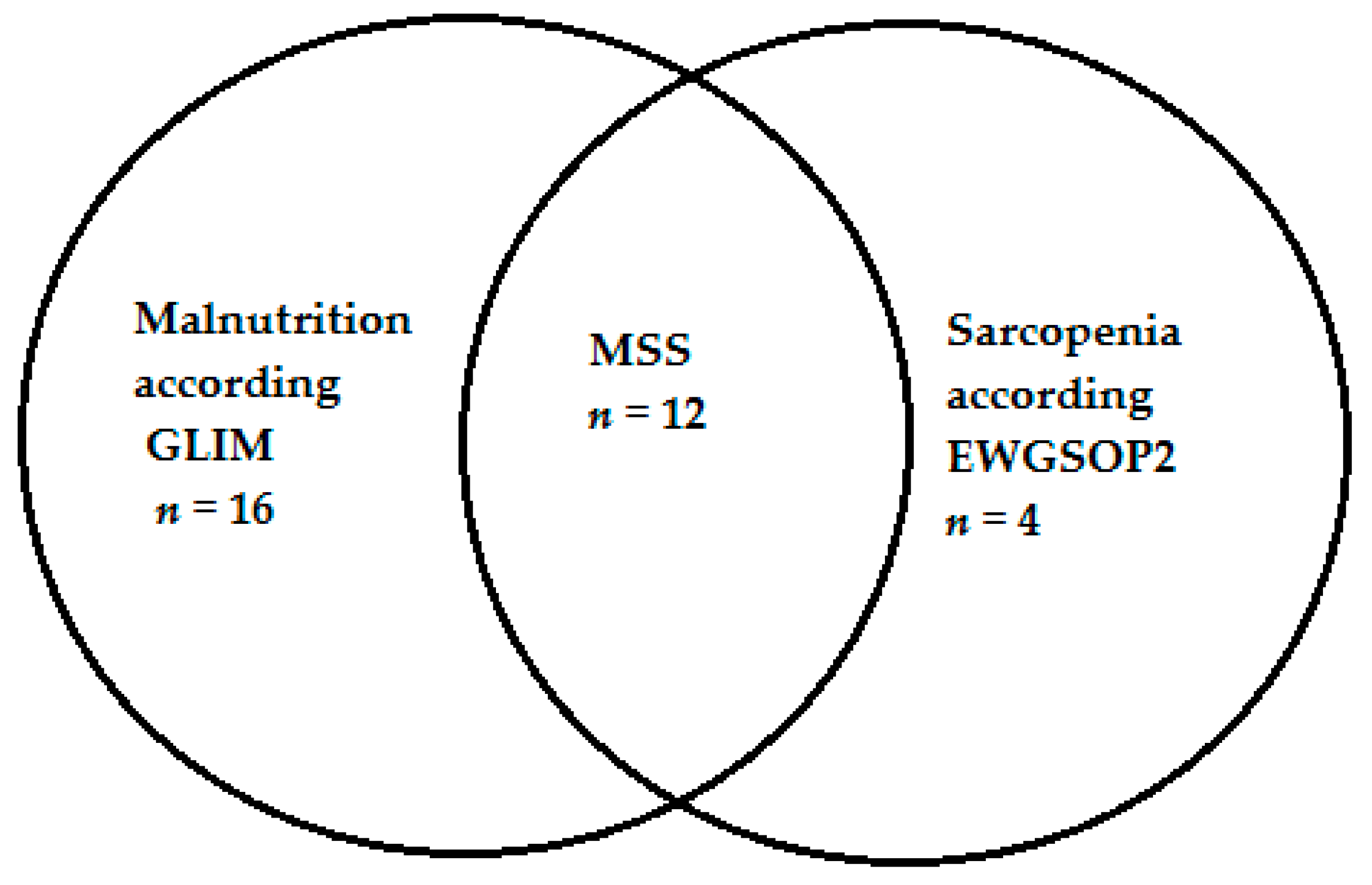
3.3. Sarcopenia and MSS
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- 2021 GOLD Reports. Available online: https://goldcopd.org/2021-gold-reports/ (accessed on 3 August 2021).
- Varmaghani, M.; Dehghani, M.; Heidari, E.; Sharifi, F.; Saeedi Moghaddam, S.; Farzadfar, F. Global Prevalence of Chronic Obstructive Pulmonary Disease: Systematic Review and Meta-Analysis. East Mediterr. Health J. 2019, 25, 47–57. [Google Scholar] [CrossRef]
- Munhoz da Rocha Lemos Costa, T.; Costa, F.M.; Jonasson, T.H.; Moreira, C.A.; Boguszewski, C.L.; Borba, V.Z.C. Body Composition and Sarcopenia in Patients with Chronic Obstructive Pulmonary Disease. Endocrine 2018, 60, 95–102. [Google Scholar] [CrossRef] [PubMed]
- Matkovic, Z.; Cvetko, D.; Rahelic, D.; Esquinas, C.; Zarak, M.; Miravitlles, M.; Tudoric, N. Nutritional Status of Patients with Chronic Obstructive Pulmonary Disease in Relation to Their Physical Performance. COPD 2017, 14, 626–634. [Google Scholar] [CrossRef]
- Raad, S.; Smith, C.; Allen, K. Nutrition Status and Chronic Obstructive Pulmonary Disease: Can We Move Beyond the Body Mass Index? Nutr. Clin. Pract. 2019, 34, 330–339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Collins, P.F.; Yang, I.A.; Chang, Y.-C.; Vaughan, A. Nutritional Support in Chronic Obstructive Pulmonary Disease (COPD): An Evidence Update. J. Thorac. Dis. 2019, 11, S2230–S2237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Itoh, M.; Tsuji, T.; Nemoto, K.; Nakamura, H.; Aoshiba, K. Undernutrition in Patients with COPD and Its Treatment. Nutrients 2013, 5, 1316–1335. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, H.T.; Collins, P.F.; Pavey, T.G.; Nguyen, N.V.; Pham, T.D.; Gallegos, D.L. Nutritional Status, Dietary Intake, and Health-Related Quality of Life in Outpatients with COPD. Int. J. Chron. Obstruct. Pulmon. Dis. 2019, 14, 215–226. [Google Scholar] [CrossRef] [Green Version]
- Ter Beek, L.; van der Vaart, H.; Wempe, J.B.; Dzialendzik, A.O.; Roodenburg, J.L.; van der Schans, C.P.; Keller, H.H.; Jager-Wittenaar, H. Dietary Resilience in Patients with Severe COPD at the Start of a Pulmonary Rehabilitation Program. Int. J. Chron. Obstruct. Pulmon. Dis. 2018, 13, 1317–1324. [Google Scholar] [CrossRef] [Green Version]
- Sepúlveda-Loyola, W.; Osadnik, C.; Phu, S.; Morita, A.A.; Duque, G.; Probst, V.S. Diagnosis, Prevalence, and Clinical Impact of Sarcopenia in COPD: A Systematic Review and Meta-analysis. J. Cachexia Sarcopenia Muscle 2020, 11, 1164–1176. [Google Scholar] [CrossRef]
- Benz, E.; Trajanoska, K.; Lahousse, L.; Schoufour, J.D.; Terzikhan, N.; De Roos, E.; de Jonge, G.B.; Williams, R.; Franco, O.H.; Brusselle, G.; et al. Sarcopenia in COPD: A Systematic Review and Meta-Analysis. Eur. Respir. Rev. 2019, 28, 190049. [Google Scholar] [CrossRef] [Green Version]
- Hancu, A. Nutritional Status as a Risk Factor in COPD. Maedica 2019, 14, 140–143. [Google Scholar] [CrossRef] [PubMed]
- Hu, X.; Zhang, L.; Wang, H.; Hao, Q.; Dong, B.; Yang, M. Malnutrition-Sarcopenia Syndrome Predicts Mortality in Hospitalized Older Patients. Sci. Rep. 2017, 7, 3171. [Google Scholar] [CrossRef] [Green Version]
- Dubé, B.-P.; Laveneziana, P. Effects of Aging and Comorbidities on Nutritional Status and Muscle Dysfunction in Patients with COPD. J. Thorac. Dis. 2018, 10, S1355–S1366. [Google Scholar] [CrossRef]
- Korkmaz, C.; Demirbas, S.; Vatansev, H.; Yildirim, E.; Teke, T.; Zamani, A. Effects of Comprehensive and Intensive Pulmonary Rehabilitation and Nutritional Support on Quality of Life and Functional Status in Patients with Chronic Obstructive Pulmonary Disease. J. Int. Med. Res. 2020, 48, 0300060520919567. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schols, A.M.; Ferreira, I.M.; Franssen, F.M.; Gosker, H.R.; Janssens, W.; Muscaritoli, M.; Pison, C.; Rutten-van Mölken, M.; Slinde, F.; Steiner, M.C.; et al. Nutritional Assessment and Therapy in COPD: A European Respiratory Society Statement. Eur. Respir. J. 2014, 44, 1504–1520. [Google Scholar] [CrossRef]
- Cederholm, T.; Jensen, G.L.; Correia, M.I.T.D.; Gonzalez, M.C.; Fukushima, R.; Higashiguchi, T.; Baptista, G.; Barazzoni, R.; Blaauw, R.; Coats, A.; et al. GLIM Criteria for the Diagnosis of Malnutrition—A Consensus Report from the Global Clinical Nutrition Community. Clin. Nutr. 2019, 38, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European Consensus on Definition and Diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [Green Version]
- Dávalos-Yerovi, V.; Marco, E.; Sánchez-Rodríguez, D.; Duran, X.; Meza-Valderrama, D.; Rodríguez, D.A.; Muñoz, E.; Tejero-Sánchez, M.; Muns, M.D.; Guillén-Solà, A.; et al. Malnutrition According to GLIM Criteria Is Associated with Mortality and Hospitalizations in Rehabilitation Patients with Stable Chronic Obstructive Pulmonary Disease. Nutrients 2021, 13, 369. [Google Scholar] [CrossRef] [PubMed]
- Tsekoura, M.; Tsepis, E.; Billis, E.; Gliatis, J. Sarcopenia in Patients with Chronic Obstructive Pulmonary Disease: A Study of Prevalence and Associated Factors in Western Greek Population. Lung India 2020, 37, 479–484. [Google Scholar] [CrossRef] [PubMed]
- Marco, E.; Sanchez-Rodriguez, D.; López-Escobar, J.; Meza, D.; Dávalos-Yerovi, V.; Duran, X.; Messaggi-Sartor, M.; Guillén-Solà, A.; Muniesa, J.M.; Duarte, E. Is Peak Expiratory Flow an Accurate Sarcopenia Screening Tool in Older Patients Referred to Respiratory Rehabilitation? Eur. Geriatr. Med. 2020, 11, 297–306. [Google Scholar] [CrossRef] [PubMed]
- Araújo, B.E.d.; Teixeira, P.P.; Valduga, K.; Fink, J.d.S.; Silva, F.M. Prevalence, Associated Factors, and Prognostic Value of Sarcopenia in Patients with Acute Exacerbated Chronic Obstructive Pulmonary Disease: A Cohort Study. Clin. Nutr. ESPEN 2021, 42, 188–194. [Google Scholar] [CrossRef] [PubMed]
- Dávalos-Yerovi, V.; Marco, E.; Sánchez-Rodríguez, D.; Guillen-Solà, A.; Duran, X.; Pascual, E.M.; Muniesa, J.M.; Escalada, F.; Duarte, E. Sarcopenia According to the Revised European Consensus on Definition and Diagnosis (EWGSOP2) Criteria Predicts Hospitalizations and Long-Term Mortality in Rehabilitation Patients With Stable Chronic Obstructive Pulmonary Disease. J. Am. Med. Dir. Assoc. 2019, 20, 1047–1049. [Google Scholar] [CrossRef] [PubMed]
- Romanik, W.; Lazarewicz, M. The Polish Version of the Abbreviated Mental Test Score (AMTS)—Methodology Issues. Psychiatr. I Psychol. Klin. 2017, 17, 203–207. [Google Scholar] [CrossRef]
- Kaiser, M.J.; Bauer, J.M.; Ramsch, C.; Uter, W.; Guigoz, Y.; Cederholm, T.; Thomas, D.R.; Anthony, P.; Charlton, K.E.; Maggio, M.; et al. Validation of the Mini Nutritional Assessment Short-Form (MNA-SF): A Practical Tool for Identification of Nutritional Status. J. Nutr. Health Aging 2009, 13, 782–788. [Google Scholar] [CrossRef] [PubMed]
- Krzymińska-Siemaszko, R.; Fryzowicz, A.; Czepulis, N.; Kaluźniak-Szymanowska, A.; Dworak, L.B.; Wieczorowska-Tobis, K. The Impact of the Age Range of Young Healthy Reference Population on the Cut-off Points for Low Muscle Mass Necessary for the Diagnosis of Sarcopenia. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 4321–4332. [Google Scholar] [CrossRef] [PubMed]
- Krzymińska-Siemaszko, R.; Deskur-Śmielecka, E.; Kaluźniak-Szymanowska, A.; Styszyński, A.; Wieczorowska-Tobis, K. Polish Version of SARC-F to Assess Sarcopenia in Older Adults: An Examination of Reliability and Validity. PLoS ONE 2020, 15, e0244001. [Google Scholar] [CrossRef]
- Bohannon, R.W. Sit-to-Stand Test for Measuring Performance of Lower Extremity Muscles. Percept. Mot. Skills 1995, 80, 163–166. [Google Scholar] [CrossRef]
- Agarwala, P.; Salzman, S.H. Six-Minute Walk Test: Clinical Role, Technique, Coding, and Reimbursement. Chest 2020, 157, 603–611. [Google Scholar] [CrossRef]
- Celli, B.; Tetzlaff, K.; Criner, G.; Polkey, M.I.; Sciurba, F.; Casaburi, R.; Tal-Singer, R.; Kawata, A.; Merrill, D.; Rennard, S. The 6-Minute-Walk Distance Test as a Chronic Obstructive Pulmonary Disease Stratification Tool. Insights from the COPD Biomarker Qualification Consortium. Am. J. Respir. Crit. Care Med. 2016, 194, 1483–1493. [Google Scholar] [CrossRef] [Green Version]
- Spruit, M.A.; Watkins, M.L.; Edwards, L.D.; Vestbo, J.; Calverley, P.M.A.; Pinto-Plata, V.; Celli, B.R.; Tal-Singer, R.; Wouters, E.F.M. Evaluation of COPD Longitudinally to Identify Predictive Surrogate Endpoints (ECLIPSE) study investigators Determinants of Poor 6-Min Walking Distance in Patients with COPD: The ECLIPSE Cohort. Respir. Med. 2010, 104, 849–857. [Google Scholar] [CrossRef]
- Perez, T.; Deslée, G.; Burgel, P.R.; Caillaud, D.; Le Rouzic, O.; Zysman, M.; Escamilla, R.; Jebrak, G.; Chanez, P.; Court-Fortune, I.; et al. Predictors in Routine Practice of 6-Min Walking Distance and Oxygen Desaturation in Patients with COPD: Impact of Comorbidities. Int. J. Chron. Obstruct. Pulmon. Dis. 2019, 14, 1399–1410. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vandewoude, M.F.J.; Alish, C.J.; Sauer, A.C.; Hegazi, R.A. Malnutrition-Sarcopenia Syndrome: Is This the Future of Nutrition Screening and Assessment for Older Adults? J. Aging Res. 2012, 2012, 651570. [Google Scholar] [CrossRef] [PubMed]
- De Blasio, F.; Di Gregorio, A.; de Blasio, F.; Bianco, A.; Bellofiore, B.; Scalfi, L. Malnutrition and Sarcopenia Assessment in Patients with Chronic Obstructive Pulmonary Disease According to International Diagnostic Criteria, and Evaluation of Raw BIA Variables. Respir. Med. 2018, 134, 1–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mete, B.; Pehlivan, E.; Gülbaş, G.; Günen, H. Prevalence of Malnutrition in COPD and Its Relationship with the Parameters Related to Disease Severity. Int. J. Chron. Obstruct. Pulmon. Dis. 2018, 13, 3307–3312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, S.H.; Shin, M.J.; Shin, Y.B.; Kim, K.U. Sarcopenia Associated with Chronic Obstructive Pulmonary Disease. J. Bone Metab. 2019, 26, 65–74. [Google Scholar] [CrossRef]
- Perrot, L.; Greil, A.; Boirie, Y.; Farigon, N.; Mulliez, A.; Costes, F.; Caillaud, D. Prevalence of Sarcopenia and Malnutrition during Acute Exacerbation of COPD and after 6 Months Recovery. Eur. J. Clin. Nutr. 2020, 74, 1556–1564. [Google Scholar] [CrossRef]
- De Araújo, B.E.; Kowalski, V.; Leites, G.M.; da Silva Fink, J.; Silva, F.M. AND-ASPEN and ESPEN Consensus, and GLIM Criteria for Malnutrition Identification in AECOPD Patients: A Longitudinal Study Comparing Concurrent and Predictive Validity. Eur. J. Clin. Nutr. 2021, 1–8. [Google Scholar] [CrossRef]
- Lengelé, L.; Bruyère, O.; Beaudart, C.; Reginster, J.-Y.; Locquet, M. Malnutrition, Assessed by the Global Leadership Initiative on Malnutrition (GLIM) Criteria but Not by the Mini Nutritional Assessment (MNA), Predicts the Incidence of Sarcopenia over a 5-Year in the SarcoPhAge Cohort. Aging Clin. Exp. Res. 2021, 33, 1507–1517. [Google Scholar] [CrossRef]
- Kaluźniak-Szymanowska, A.; Krzymińska-Siemaszko, R.; Lewandowicz, M.; Deskur-Śmielecka, E.; Stachnik, K.; Wieczorowska-Tobis, K. Diagnostic Performance and Accuracy of the MNA-SF against GLIM Criteria in Community-Dwelling Older Adults from Poland. Nutrients 2021, 13, 2183. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Without Malnutrition n = 96 | Malnutrition n = 28 | p-Value | |
|---|---|---|---|
| Age (years) | 69.4 ± 6.1 | 69.4 ± 6.0 | 0.9332 a |
| AMTS | 9.6 ± 0.7 | 9.6 ± 0.6 | 0.5590 a |
| Height (cm) | 167.5 ± 8.7 | 162.8 ± 10.2 | 0.0111 a |
| Body weight (kg) | 82.9 ± 18.3 | 61.0 ± 19.2 | 0.0000 a |
| BMI (kg/m2) | 29.5 ± 6.0 | 22.8 ± 6.0 | 0.0000 a |
| BFM (kg) | 28.7 ± 12.2 | 17.6 ± 11.1 | 0.0000 a |
| SMM (kg) | 30.0 ± 6.2 | 23.4 ± 6.3 | 0.0000 a |
| PBF (%) | 33.6 ± 9.4 | 26.9 ± 10.0 | 0.0019 a |
| FFM (kg) | 22.4 ± 5.0 | 16.9 ± 5.1 | 0.0000 a |
| MNA-SF | 13.1 ± 1.1 | 8.6 ± 2.6 | 0.0000 a |
| Low ALM index | 10 (10.4) | 18 (64.3) | 0.0000 c |
| Low upper limb strength | 32 (33.3) | 14 (50.0) | 0.1082 c |
| Chair Stand Test(s) | 14.2 ± 5.7 | 17.1 ± 7.9 | 0.0567 a |
| 4-m usual walking speed test (m/s) | 0.9 ± 0.2 | 0.8 ± 0.2 | 0.0112 b |
| SARC-F | 2.0 ± 1.6 | 3.0 ± 2.0 | 0.0336 a |
| Risk of sarcopenia according SARC-F | 18 (18.8) | 11 (39.3) | 0.0239 c |
| FEV1/FVC EX | 51.5 ± 13.1 | 49.3 ± 10.9 | 0.2781 a |
| FEV1 | 51.0 ± 18.7 | 49.3 ± 19.5 | 0.5620 a |
| GOLD 1 + GOLD 2 | 49 (81.7) | 11 (18.3) | 0.2734 c |
| GOLD 3 + GOLD 4 | 47 (73.4) | 17 (26.6) | |
| 6 MWT (m) | 372.2 ± 118.3 | 281.0 ± 143.4 | 0.0079 a |
| Without Sarcopenia n = 108 | Sarcopenia n = 16 | p-Value | |
|---|---|---|---|
| Age (years) | 69.2 ± 5.9 | 70.4 ± 7.5 | 0.6542 a |
| AMTS | 9.6 ± 0.7 | 9.8 ± 0.6 | 0.2243 a |
| Height (cm) | 166.8 ± 9.3 | 163.7 ± 8.8 | 0.0722 a |
| Body weight (kg) | 81.3 ± 19.5 | 55.2 ± 11.2 | 0.0000 a |
| BMI (kg/m2) | 29.1 ± 6.3 | 20.6 ± 3.6 | 0.0000 a |
| BFM (kg) | 27.9 ± 12.6 | 14.4 ± 6.7 | 0.0000 a |
| SMM (kg) | 29.5 ± 6.5 | 21.9 ± 4.0 | <0.0001 b |
| PBF (%) | 33.2 ± 9.8 | 25.1 ± 8.2 | 0.0020 a |
| FFM (kg) | 21.9 ± 5.4 | 16.0 ± 3.5 | <0.0001 b |
| MNA-SF | 12.5 ± 2.1 | 9.3 ± 3.1 | 0.0000 a |
| Low ALM index | 12 (11.1) | 16 (100) | 0.0000 c |
| Low upper limb strength | 32 (29.6) | 14 (87.5) | <0.0001 c |
| Chair Stand Test(s) | 14.4 ± 6.0 | 18.6 ± 7.9 | 0.0536 a |
| 4-m usual walking speed test (m/s) | 0.9 ± 0.2 | 0.8 ± 0.2 | 0.0395 b |
| SARC-F | 2.1 ± 1.7 | 3.0 ± 1.9 | 0.1819 a |
| Risk of sarcopenia according EWGSOP2 | 24 (22.2) | 5 (31.3) | 0.4391 c |
| FEV1/FVC EX | 52.0 ± 12.8 | 44.1 ± 8.8 | 0.0396 a |
| FEV1 | 52.5 ± 18.8 | 38.3 ± 14.0 | 0.0171 a |
| GOLD 1 + GOLD 2 | 58 (53.7) | 2 (12.5) | 0.0011 c |
| GOLD 3 + GOLD 4 | 50 (46.3) | 14 (87.5) | |
| 6 MWT (m) | 371.3 ± 119.7 | 220 ± 118.7 | 0.0002 a |
| Without MSS n = 112 | MSS n = 12 | p-Value | |
|---|---|---|---|
| Age (years) | 69.2 ± 5.9 | 70.6 ± 7.3 | 0.6354 a |
| AMTS | 9.6 ± 0.7 | 9.8 ± 0.6 | 0.2243 a |
| Height (cm) | 166.9 ± 9.2 | 162.0 ± 9.5 | 0.0722 a |
| Body weight (kg) | 80.9 ± 19.4 | 50.9 ± 8.1 | 0.0000 a |
| BMI (kg/m2) | 28.9 ± 6.3 | 19.5 ± 3.1 | 0.0000 a |
| BFM (kg) | 27.7 ± 12.5 | 12.3 ± 5.3 | 0.0000 a |
| SMM (kg) | 29.4 ± 6.5 | 20.5 ± 3.3 | 0.0000 b |
| PBF (%) | 33.0 ± 9.7 | 23.5 ± 8.3 | 0.0020 a |
| FFM (kg) | 21.9 ± 5.3 | 14.7 ± 3.0 | 0.0000 b |
| MNA-SF | 12.5 ± 2.0 | 8.2 ± 2.6 | 0.0000 a |
| Low ALM index | 16 (14.3) | 12 (100) | 0.0000 c |
| Low upper limb strength | 35 (31.3) | 11 (91.7) | 0.0000 c |
| Chair Stand Test(s) | 14.4 ± 6.0 | 18.6 ± 7.9 | 0.0536 a |
| 4-m usual walking speed test (m/s) | 0.9 ± 0.2 | 0.7 ± 0.2 | 0.0159 b |
| SARC-F | 2.1 ± 1.6 | 3.1 ± 2.2 | 0.1819 a |
| Risk of sarcopenia according SARC-F | 24 (21.4) | 5 (41.7) | 0.1377 c |
| FEV1/FVC EX | 51.7 ± 12.8 | 44.7 ± 8.9 | 0.0396 a |
| FEV1 | 51.9 ± 18.9 | 39.1 ± 14.1 | 0.0171 a |
| GOLD 1 + GOLD 2 | 59 (52.7) | 1 (8.3) | 0.0016 c |
| GOLD 3 + GOLD 4 | 53 (47.3) | 11 (91.7) | |
| 6 MWT (m) | 368.5 ± 119.7 | 204.6 ± 122.4 | 0.0002 a |
| Without Malnutrition or Sarcopenia a n = 92 | Malnutrition or Sarcopenia b n = 20 | Malnutrition-Sarcopenia Syndrome c n = 12 | p-Value | |
|---|---|---|---|---|
| Age (years) | 69.4 ± 6.0 | 68.8 ± 5.8 | 70.6 ±7.3 | NS |
| AMTS | 9.6 ± 0.7 | 9.5 ± 0.6 | 9.8 ± 0.6 | NS |
| Height (cm) | 167.4 ± 8.9 | 164.5 ± 10.1 | 162.0 ± 9.5 | NS |
| Body weight (kg) | 83.6 ± 18.3 | 68.4 ± 19.7 | 50.9 ± 8.1 | a vs. b p = 0.0054 d a vs. c p = 0.0000 d b vs. c p = 0.0480 d |
| BMI (kg/m2) | 29.8 ± 6.0 | 25.1 ± 6.0 | 19.5 ± 3.1 | a vs. b p = 0.0083 d a vs. c p = 0.0000 d b vs. c p = 0.0471 d |
| BFM (kg) | 29.1 ± 12.3 | 21.4 ± 11.7 | 12.3 ± 5.3 | a vs. b p = 0.0398 d a vs. c p < 0.0001 d |
| SMM (kg) | 30.2 ± 6.2 | 25.7 ± 6.5 | 20.5 ± 3.3 | a vs. b p = 0.0117 d a vs. c p < 0.0001 d |
| PBF (%) | 33.8 ± 9.5 | 29.5 ± 9.9 | 23.5 ± 8.3 | a vs. c p = 0.0027 d |
| FFM (kg) | 22.5 ± 5.1 | 18.8 ± 5.2 | 14.7 ± 3.0 | a vs. b p = 0.0103 d a vs. c p < 0.0001 d |
| MNA-SF | 13.2 ± 1.1 | 9.7 ± 2.9 | 8.2 ± 2.6 | a vs. b p = 0.0000 d a vs. c p = 0.0000 d |
| Low ALM index | 6 (6.5) | 10 (50) | 12 (100) | p = 0.0000 e |
| Low upper limb strength | 29 (31.5) | 6 (30) | 11 (91.7) | p = 0.0002 e |
| Chair Stand Test(s) | 14.2 ± 5.8 | 15.5 ± 7.2 | 18.6 ± 7.9 | NS |
| 4-m usual walking speed test (m/s) | 0.9 ± 0.2 | 0.8 ± 0.2 | 0.7 ± 0.2 | NS |
| SARC-F | 2.0 ± 1.6 | 2.9 ± 1.7 | 3.1 ± 2.2 | NS |
| Sarcopenia risk according to SARC-F | 18 (19.6) | 6 (30.0) | 5 (41.7) | NS |
| FEV1/FVC EX | 51.9 ± 13.2 | 50.6 ± 11.5 | 44.7 ± 8.9 | NS |
| FEV1 | 51.7 ± 18.6 | 52.8 ± 20.5 | 39.1 ± 14.1 | NS |
| GOLD 1 + GOLD 2 | 48 (52.2) | 11 (55.0) | 1 (8.3) | p = 0.0068 e |
| GOLD 3 + GOLD 4 | 44 (47.8) | 9 (45.0) | 11 (91.7) | |
| 6MWT (m) | 375.6 ± 118.2 | 335.0 ± 124.5 | 204.6 ± 122.4 | a vs. c p = 0.0003 d b vs. c p = 0.0315 d |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kaluźniak-Szymanowska, A.; Krzymińska-Siemaszko, R.; Deskur-Śmielecka, E.; Lewandowicz, M.; Kaczmarek, B.; Wieczorowska-Tobis, K. Malnutrition, Sarcopenia, and Malnutrition-Sarcopenia Syndrome in Older Adults with COPD. Nutrients 2022, 14, 44. https://doi.org/10.3390/nu14010044
Kaluźniak-Szymanowska A, Krzymińska-Siemaszko R, Deskur-Śmielecka E, Lewandowicz M, Kaczmarek B, Wieczorowska-Tobis K. Malnutrition, Sarcopenia, and Malnutrition-Sarcopenia Syndrome in Older Adults with COPD. Nutrients. 2022; 14(1):44. https://doi.org/10.3390/nu14010044
Chicago/Turabian StyleKaluźniak-Szymanowska, Aleksandra, Roma Krzymińska-Siemaszko, Ewa Deskur-Śmielecka, Marta Lewandowicz, Beata Kaczmarek, and Katarzyna Wieczorowska-Tobis. 2022. "Malnutrition, Sarcopenia, and Malnutrition-Sarcopenia Syndrome in Older Adults with COPD" Nutrients 14, no. 1: 44. https://doi.org/10.3390/nu14010044