
Social Distancing in Chronic Migraine during the COVID-19 Outbreak: Results from a Multicenter Observational Study

 ,
,  , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Data Collection
2.3. Scoring Protocol
2.4. Statistical Analysis
3. Results
3.1. Study Population
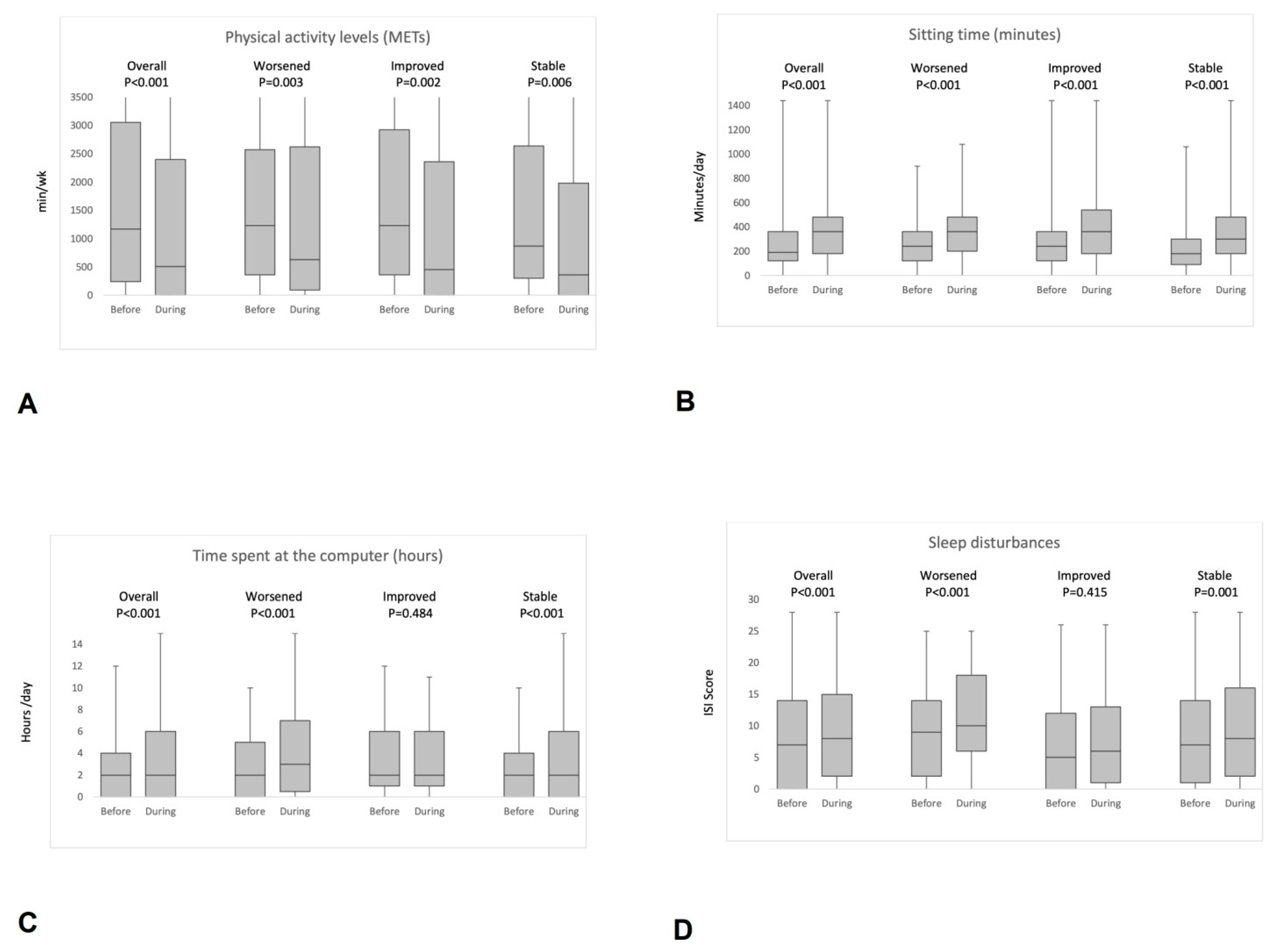
3.2. Physical Activity Levels and “Smart-Working”
3.3. Eating Habits and Lifestyle
3.4. Sleep Quality
4. Discussion
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bersano, A.; Pantoni, L. On being a neurologist in Italy at the time of the COVID-19 outbreak. Neurology 2020, 94, 905–906. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Q&A on Coronaviruses (COVID-19). 2020. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/question-and-answers-hub/q-a-detail/coronavirus-disease-covid-19 (accessed on 23 February 2021).
- Maugeri, G.; Castrogiovanni, P.; Battaglia, G.; Pippi, R.; D’Agata, V.; Palma, A.; Di Rosa, M.; Musumeci, G. The impact of physical activity on psychological health during Covid-19 pandemic in Italy. Heliyon 2020, 6, e04315. [Google Scholar] [CrossRef]
- Di Stefano, V.; Battaglia, G.; Giustino, V.; Gagliardo, A.; D’Aleo, M.; Giannini, O.; Palma, A.; Brighina, F. Significant reduction of physical activity in patients with neuromuscular disease during COVID-19 pandemic: The long-term consequences of quarantine. J. Neurol. 2021. Available online: http://www.ncbi.nlm.nih.gov/pubmed/32661716 (accessed on 13 July 2020). [CrossRef] [PubMed]
- de Seze, J.; Lebrun-Frenay, C. Covid-19, the pandemic war: Implication for neurologists. Rev. Neurol. 2020, 176, 223–224. [Google Scholar] [CrossRef] [PubMed]
- Velavan, T.P.; Meyer, C.G. The COVID-19 epidemic. Trop. Med. Int. Health 2020, 5, 278–280. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, P.; Mao, L.; Nassis, G.P.; Harmer, P.; Ainsworth, B.E.; Li, F. Coronavirus disease (COVID-19): The need to maintain regular physical activity while taking precautions. J. Sport Health Sci. 2020, 9, 103–104. [Google Scholar] [CrossRef]
- Jiménez-Pavón, D.; Carbonell-Baeza, A.; Lavie, C.J. Physical exercise as therapy to fight against the mental and physical con-sequences of COVID-19 quarantine: Special focus in older people. Prog. Cardiovasc. Dis. 2020, 63, 386–388. [Google Scholar] [CrossRef]
- Di Stefano, V.; Rispoli, M.G.; Pellegrino, N.; Graziosi, A.; Rotondo, E.; Napoli, C.; Pietrobon, D.; Brighina, F.; Parisi, P. Diagnostic and therapeutic aspects of hemiplegic migraine. J. Neurol. Neurosurg. Psychiatry 2020, 91, 764–771. [Google Scholar] [CrossRef]
- López-Bravo, A.; García-Azorín, D.; Belvís, R.; González-Oria, C.; Latorre, G.; Santos-Lasaosa, S.; Guerrero-Peral, Á.L. Impact of the COVID-19 pandemic on headache management in Spain: An analysis of the current situation and future perspectives. Neurología 2020, 35, 372–380. [Google Scholar] [CrossRef]
- Parodi, I.C.; Poeta, M.G.; Assini, A.; Schirinzi, E.; Del Sette, P. Impact of quarantine due to COVID infection on migraine: A survey in Genova, Italy. Neurol. Sci. 2020, 41, 2025–2027. [Google Scholar] [CrossRef]
- Al-Hashel, J.Y.; Ismail, I.I. Impact of coronavirus disease 2019 (COVID-19) pandemic on patients with migraine: A web-based survey study. J. Headache Pain 2020, 21, 1–9. [Google Scholar] [CrossRef]
- Barbanti, P.; Brighina, F.; Egeo, G.; Di Stefano, V.; Silvestro, M.; Russo, A. Migraine as a Cortical Brain Disorder. Headache; Blackwell Publishing Inc.: Hoboken, NJ, USA, 2020. [Google Scholar]
- Friedman, D.I.; Dye, T.D.V. Migraine and the Environment. Headache 2009, 49, 941–952. [Google Scholar] [CrossRef] [PubMed]
- Sandoe, C.H.; Sasikumar, S.; Lay, C.; Lawler, V. The Impact of Shift Work on Migraine: A Case Series and Narrative Review. Headache 2019, 59, 1631–1640. [Google Scholar] [CrossRef]
- Jukic, I.; Calleja-González, J.; Cos, F.; Cuzzolin, F.; Olmo, J.; Terrados, N.; Njaradi, N.; Sassi, R.; Requena, B.; Milanovic, L.; et al. Strategies and Solutions for Team Sports Athletes in Isolation due to COVID-19. Sports 2020, 8, 56. [Google Scholar] [CrossRef] [PubMed]
- Giustino, V.; Parroco, A.M.; Gennaro, A.; Musumeci, G.; Palma, A.; Battaglia, G. Physical Activity Levels and Related Energy Expenditure during COVID-19 Quarantine among the Sicilian Active Population: A Cross-Sectional Online Survey Study. Sustainability 2020, 12, 4356. [Google Scholar] [CrossRef]
- Szperka, C.L.; Ailani, J.; Barmherzig, R.; Klein, B.C.; Minen, M.T.; Halker Singh, R.B.; Shapiro, R.E. Migraine Care in the Era of COVID-19: Clinical Pearls and Plea to Insurers. Headache 2020, 60, 833–842. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Narici, M.; De Vito, G.; Franchi, M.; Paoli, A.; Moro, T.; Marcolin, G.; Grassi, B.; Baldassarre, G.; Zuccarelli, L.; Biolo, G.; et al. Impact of sedentarism due to the COVID-19 home confinement on neuromuscular, cardiovascular and metabolic health: Physiological and pathophysiological implications and recommendations for physical and nutritional countermeasures. Eur. J. Sport Sci. 2020, 1–22, 1–22. [Google Scholar] [CrossRef]
- Mikines, K.J.; Richter, E.A.; Dela, F.; Galbo, H. Seven days of bed rest decrease insulin action on glucose uptake in leg and whole body. J. Appl. Physiol. 1991, 70, 1245–1254. [Google Scholar] [CrossRef]
- Mortensen, B.; Friedrichsen, M.; Andersen, N.R.; Alibegovic, A.C.; Højbjerre, L.; Sonne, M.P.; Stallknecht, B.; Dela, F.; Wojtaszewski, J.F.; Vaag, A. Physical inactivity affects skeletal muscle insulin signaling in a birth weight-dependent manner. J. Diabetes Complicat. 2014, 28, 71–78. [Google Scholar] [CrossRef]
- Paddon-Jones, U.; Sheffield-Moore, M.; Cree, M.G.; Hewlings, S.J.; Aarsland, A.; Wolfe, R.R.; Ferrando, A.A. Atrophy and Impaired Muscle Protein Synthesis during Prolonged Inactivity and Stress. J. Clin. Endocrinol. Metab. 2006, 91, 4836–4841. [Google Scholar] [CrossRef] [Green Version]
- Hougaard, A.; Amin, F.; Hauge, A.W.; Ashina, M.; Olesen, J. Provocation of migraine with aura using natural trigger factors. Neurology 2013, 80, 428–431. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Busch, V.; Gaul, C. Exercise in Migraine Therapy—Is There Any Evidence for Efficacy? A Critical Review. Headache 2008, 48, 890–899. [Google Scholar] [CrossRef] [PubMed]
- Pilati, L.; Battaglia, G.; Di Stefano, V.; Di Marco, S.; Torrente, A.; Raieli, V.; Firenze, A.; Salemi, G.; Brighina, F. Migraine and Sport in a Physically Active Population of Students: Results of a Cross-Sectional Study. Headache 2020, 60, 2330–2339. [Google Scholar] [CrossRef]
- Varkey, E.; Hagen, K.; Zwart, J.-A.; Linde, M. Physical Activity and Headache: Results from the Nord-Trøndelag Health Study (HUNT). Cephalalgia 2008, 28, 1292–1297. [Google Scholar] [CrossRef] [PubMed]
- Martin, V.T.; Vij, B. Diet and Headache: Part 1. Headache 2016, 56, 1543–1552. [Google Scholar] [CrossRef]
- Cairns, B.E. Influence of pro-algesic foods on chronic pain conditions. Expert Rev Neurother. 2016, 16, 415–423. [Google Scholar] [CrossRef] [Green Version]
- Razeghi Jahromi, S.; Ghorbani, Z.; Martelletti, P.; Lampl, C.; Togha, M. Association of diet and headache. J. Headache Pain 2019, 20, 106. [Google Scholar] [CrossRef] [Green Version]
- Finocchi, C.; Sivori, G. Food as trigger and aggravating factor of migraine. Neurol. Sci. 2012, 33, 77–80. [Google Scholar] [CrossRef]
- Di Renzo, L.; Gualtieri, P.; Pivari, F.; Soldati, L.; Attinà, A.; Cinelli, G.; Leggeri, C.; Caparello, G.; Barrea, L.; Scerbo, F.; et al. Eating habits and lifestyle changes during COVID-19 lockdown: An Italian survey. J. Transl. Med. 2020, 18, 229. [Google Scholar] [CrossRef]
- Potter, G.D.M.; Skene, D.J.; Arendt, J.; Cade, J.E.; Grant, P.J.; Hardie, L.J. Circadian Rhythm and Sleep Disruption: Causes, Metabolic Consequences, and Countermeasures. Endocr. Rev. 2016, 37, 584–608. [Google Scholar] [CrossRef] [Green Version]
- Sher, L. COVID-19, anxiety, sleep disturbances and suicide. Sleep Med. 2020, 70, 124. [Google Scholar] [CrossRef]
- Huang, Y.; Zhao, N. Generalized anxiety disorder, depressive symptoms and sleep quality during COVID-19 outbreak in China: A web-based cross-sectional survey. Psychiatry Res. 2020, 288, 112954. [Google Scholar] [CrossRef] [PubMed]
- Stanton, R.; To, Q.G.; Khalesi, S.; Williams, S.L.; Alley, S.J.; Thwaite, T.L.; Fenning, A.S.; Vandelanotte, C. Depression, anxiety and stress during COVID-19: Associations with changes in physical activity, sleep, tobacco and alcohol use in Australian adults. Int. J. Environ. Res. Public Health 2020, 17, 4065. [Google Scholar] [CrossRef] [PubMed]
- Wells, R.E.; Strauss, L.D. The Value of Headache-Specific Recommendations During COVID-19. Headache 2020, 60, 820–823. [Google Scholar] [CrossRef] [PubMed]
- Chowdhury, D.; Datta, D. Managing migraine in the times of COVID-19 pandemic. Ann. Indian Acad. Neurol. 2020, 23, S33–S39. [Google Scholar] [PubMed]
- Battaglia, G.; Paoli, A.; Bellafiore, M.; Bianco, A.; Palma, A. Influence of a sport-specific training background on vertical jumping and throwing performance in young female basketball and volleyball players. J. Sports Med. Phys. Fit. 2014, 54, 581–587. [Google Scholar]
- Olesen, J. Headache Classification Committee of the International Headache Society (IHS) The International Classification of Headache Disorders, 3rd edition. Cephalalgia 2018, 38, 1–211. [Google Scholar]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity questionnaire: 12-Country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [Green Version]
- Castronovo, V.; Galbiati, A.; Marelli, S.; Brombin, C.; Cugnata, F.; Giarolli, L.; Anelli, M.M.; Rinaldi, F.; Ferini-Strambi, L. Validation study of the Italian version of the Insomnia Severity Index (ISI). Neurol. Sci. 2016, 37, 1517–1524. [Google Scholar] [CrossRef]
- Byrne, N.M.; Hills, A.P.; Hunter, G.R.; Weinsier, R.L.; Schutz, Y. Metabolic equivalent: One size does not fit all. J. Appl. Physiol. 2005, 99, 1112–1119. [Google Scholar] [CrossRef] [Green Version]
- Ainsworth, B.E.; Haskell, W.L.; Leon, A.S.; Jacobs, D.R.; Montoye, H.J.; Sallis, J.F.; Paffenbarger, R.S. Compendium of Physical Activities: Classification of energy costs of human physical activities. Med. Sci. Sports Exerc. 1993, 25, 71–80. [Google Scholar] [CrossRef]
- Constandt, B.; Thibaut, E.; De Bosscher, V.; Scheerder, J.; Ricour, M.; Willem, A. Exercising in times of lockdown: An analysis of the impact of COVID-19 on levels and patterns of exercise among adults in Belgium. Int. J. Environ. Res. Public Health 2020, 17, 4144. [Google Scholar] [CrossRef] [PubMed]
- Cotter, E.W.; Kelly, N.R. Stress-related eating, mindfulness, and obesity. Health Psychol. 2018, 37, 516–525. [Google Scholar] [CrossRef] [PubMed]
- Altena, E.; Baglioni, C.; Espie, C.A.; Ellis, J.; Gavriloff, D.; Holzinger, B.; Schlarb, A.; Frase, L.; Jernelöv, S.; Riemann, D. Dealing with sleep problems during home confinement due to the COVID-19 outbreak: Practical recommendations from a task force of the European CBT-I Academy. J. Sleep Res. 2020, 29, e13052. [Google Scholar] [CrossRef] [PubMed]
- Chabriat, H.; Danchot, J.; Michel, P.; Joire, J.; Henry, P. Precipitating Factors of Headache. A Prospective Study in a National Control-Matched Survey in Migraineurs and Nonmigraineurs. Headache 1999, 39, 335–338. [Google Scholar] [CrossRef]
- Pellegrino, A.B.W.; Davis-Martin, R.E.; Houle, T.T.; Turner, D.P.; Smitherman, T.A. Perceived triggers of primary headache disorders: A meta-analysis. Cephalalgia 2017, 38, 1188–1198. [Google Scholar] [CrossRef]
- Kelman, L. The Triggers or Precipitants of the Acute Migraine Attack. Cephalalgia 2007, 27, 394–402. [Google Scholar] [CrossRef]
- Andress-Rothrock, D.; King, W.; Rothrock, J. An Analysis of Migraine Triggers in a Clinic-Based Population. Headache 2009, 50, 1366–1370. [Google Scholar] [CrossRef]
- Bertisch, S.M.; Li, W.; Buettner, C.; Mostofsky, E.; Rueschman, M.; Kaplan, E.R.; Fung, J.; Huntington, S.; Murphy, T.; Stead, C.; et al. Nightly sleep duration, fragmentation, and quality and daily risk of migraine. Neurology 2019, 94, e489–e496. [Google Scholar] [CrossRef]
- Vgontzas, A.; Pavlović, J.M. Sleep Disorders and Migraine: Review of Literature and Potential Pathophysiology Mechanisms. Headache 2018, 58, 1030–1039. [Google Scholar] [CrossRef]
- Smith, M.T.; Edwards, R.R.; McCann, U.D.; Haythomthwaite, J.A. The effects of sleep deprivation on pain inhibition and sponta-neous pain in women. Sleep 2007, 30, 494–505. [Google Scholar] [CrossRef]
- Drummond, P. Tryptophan Depletion Increases Nausea, Headache and Photophobia in Migraine Sufferers. Cephalalgia 2006, 26, 1225–1233. [Google Scholar] [CrossRef] [Green Version]
- Schuh-Hofer, S.; Richter, M.; Geworski, L.; Villringer, A.; Israel, H.; Wenzel, R.; Munz, D.L.; Arnold, G. Increased serotonin transporter availability in the brainstem of migraineurs. J. Neurol. 2007, 254, 789–796. [Google Scholar] [CrossRef]
- Supornsilpchai, W.; Sanguanrangsirikul, S.; Maneesri, S.; Srikiatkhachorn, A. Serotonin Depletion, Cortical Spreading Depression, and Trigeminal Nociception. Headache: J. Head Face Pain 2006, 46, 34–39. [Google Scholar] [CrossRef] [PubMed]
- Saper, C.B.; Scammell, T.E.; Lu, J. Hypothalamic regulation of sleep and circadian rhythms. Nature 2005, 437, 1257–1263. [Google Scholar] [CrossRef] [PubMed]
- Lőrincz, M.L.; Adamantidis, A.R. Monoaminergic control of brain states and sensory processing: Existing knowledge and recent insights obtained with optogenetics. Prog. Neurobiol. 2017, 151, 237–253. [Google Scholar] [CrossRef] [PubMed]
- Haskell, W.L.; Lee, I.M.; Pate, R.R.; Powell, K.E.; Blair, S.N.; Franklin, B.A.; Macera, C.A.; Heath, G.W.; Thompson, P.D.; Bauman, A. Physical activity and public health: Updated recom-mendation for adults from the American College of Sports Medicine and the American Heart Association. Med. Sci. Sports Exerc. 2007, 39, 1423–1434. [Google Scholar] [CrossRef] [Green Version]
- Buman, M.P.; Phillips, B.A.; Youngstedt, S.D.; Kline, C.E.; Hirshkowitz, M. Does nighttime exercise really disturb sleep? Results from the 2013 National Sleep Foundation Sleep in America Poll. Sleep Med. 2014, 15, 755–761. [Google Scholar] [CrossRef]
- Kubitz, K.A.; Landers, D.M.; Petruzzello, S.J.; Han, M. The Effects of Acute and Chronic Exercise on Sleep A Meta-Analytic Review. Sports Med. 1996, 21, 277–291. [Google Scholar] [CrossRef]
- Youngstedt, S.D.; O’Connor, P.J.; Dishman, R.K. The Effects of Acute Exercise on Sleep: A Quantitative Synthesis. Sleep 1997, 20, 203–214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Blanco-Centurion, C.; Shiromani, P. Beneficial effects of regular exercise on sleep in old F344 rats. Neurobiol. Aging 2006, 27, 1859–1869. [Google Scholar] [CrossRef] [PubMed]
- Gong, H.; Szymusiak, R.; King, J.; Steininger, T.; McGinty, D. Sleep-related c-Fos protein expression in the preoptic hypothalamus: Effects of ambient warming. Am. J. Physiol. Integr. Comp. Physiol. 2000, 279, R2079–R2088. [Google Scholar] [CrossRef]
- Born, J.; Fehm, H.L. Hypothalamus-pituitary-adrenal activity during human sleep: A coordinating role for the limbic hippo-campal system. Exp. Clin. Endocrinol. Diabetes 1998, 106, 153–163. [Google Scholar] [CrossRef] [PubMed]
- Sandercock, G.R.H.; Bromley, P.D.; Brodie, D.A. Effects of Exercise on Heart Rate Variability: Inferences from Meta-Analysis. Med. Sci. Sports Exerc. 2005, 37, 433–439. [Google Scholar] [CrossRef]
- de Tommaso, M.; Delussi, M.; Vecchio, E.; Sciruicchio, V.; Invitto, S.; Livrea, P. Sleep features and central sensitization symptoms in primary headache patients. J. Headache Pain 2014, 26, 64. [Google Scholar] [CrossRef] [Green Version]
- Ma, M.; Bao, J.; Fang, J.; Li, C.; Changling, L.; Ge, W.; Zhang, Y.; Guo, J.; He, L. Impact of Headache Frequency and Sleep during the COVID-19 Pandemic among Migraine Patients. Curr. Neurovasc. Res. 2021, 18, 1. [Google Scholar] [CrossRef] [PubMed]
- Delussi, M.; Gentile, E.; Coppola, G.; Prudenzano, A.M.P.; Rainero, I.; Sances, G.; Abagnale, C.; Caponnetto, V.; De Cesaris, F.; Frattale, I.; et al. Investigating the Effects of COVID-19 Quarantine in Migraine: An Observational Cross-Sectional Study from the Italian National Headache Registry (RICe). Front Neurol. 2020, 11, 597881. [Google Scholar] [CrossRef]
- Papetti, L.; Di Loro, P.A.; Tarantino, S.; Grazzi, L.; Guidetti, V.; Parisi, P.; Raieli, V.; Sciruicchio, V.; Termine, C.; Toldo, I.; et al. I stay at home with headache. A survey to investigate how the lockdown for COVID-19 impacted on headache in Italian children. Cephalalgia 2020, 40, 1459–1473. [Google Scholar] [CrossRef]
- Gonzalez-Martinez, A.; Planchuelo-Gómez, Á.; Guerrero, Á.L.; García-Azorín, D.; Santos-Lasaosa, S.; Navarro-Pérez, M.P.; Odriozola-González, P.; Irurtia, M.J.; Quintas, S.; de Luis-García, R.; et al. Evaluation of the Impact of the COVID-19 Lockdown in the Clinical Course of Migraine. Pain Med. 2021. [Google Scholar] [CrossRef]
- Verhagen, I.E.; Van Casteren, D.S.; de Vries, L.S.; Terwindt, G.M. Effect of lockdown during COVID-19 on migraine: A longitudinal cohort study. Cephalalgia 2021. [Google Scholar] [CrossRef]
- Ito, E.; Inoue, Y. The International Classification of Sleep Disorders, third edition. American Academy of Sleep Medicine. Includes bibliographies and index. Nihon Rinsho 2015, 73, 916–923. [Google Scholar] [PubMed]


{kind=link}
| Overall (n = 261) | Worsened (n = 72) | Improved (n = 86) | Stable (n = 103) | p Value | |
|---|---|---|---|---|---|
| Female, n (%) | 227 (87.0) | 63 (87.5) | 75 (87.2) | 89 (86.4) | 0.975 |
| Age, median (IQR) | 45 (34.5–53) | 45 (33.5–52) | 45 (34–52) | 46 (35–56) | 0.689 |
| BMI, median (IQR) | 24 (21–26.5) | 24 (21–26) | 24 (21–26) | 24 (21–27) | 0.887 |
| Occupation | 0.632 | ||||
| Employed | 162 (62.1) | 4 (55.6) | 57 (66.3) | 65 (63.1) | |
| Unemployed | 71 (27.2) | 23 (31.9) | 22 (25.6) | 26 (25.2) | |
| Student | 22 (8.4) | 8 (11.1) | 6 (7.0) | 8 (7.8) | |
| Retired | 6 (2.3) | 1 (1.4) | 1 (1.2) | 4 (3.9) | |
| Works on video terminals, n (%) | 92 (35.2) | 25 (34.7) | 33 (38.4) | 34 (33.0) | 0.815 |
| Smart working during social distancing, n (%) | 79 (30.2) | 24 (33.3) | 26 (30.2) | 29 (28.2) | 0.755 |
| Chronic migraine, n (%) | 186 (71.3) | 50 (69.4) | 68 (79.1) | 68 (66.0) | 0.131 |
| Aura, n (%) | 69 (26.4) | 18 (25.0) | 27 (31.4) | 24 (23.3) | 0.458 |
| Triggers, n (%) | 174 (66.7) | 52 (67.8) | 60 (69.8) | 62 (60.2) | 0.904 |
| Food | 4 (1.5) | 1 (1.4) | 1 (1.4) | 2 (1.9) | |
| Climate | 22 (8.4) | 7 (9.7) | 7 (8.1) | 8 (7.8) | |
| Hormonal | 23 (8.8) | 6 (8.3) | 10 (11.6) | 7 (6.8) | |
| Psychic | 58 (22.2) | 17 (23.6) | 19 (22.1) | 22 (21.4) | |
| Multiple | 67 (25.7) | 21 (29.2) | 23 (26.7) | 23 (22.3) | |
| Monthly headache days, median (IQR) | |||||
| Before social distancing | 10 (5–16) | 8 (4–12) | 13 (7–18) | 10 (5–20) | <0.001 |
| During social distancing | 8 (4–16) | 12 (8–20) | 6 (2–9) | 10 (5–20) | <0.001 |
| Difference (p value) | 0.112 | <0.001 | <0.001 | 0.999 | |
| Headache intensity, median (IQR) | |||||
| Before social distancing | 7 (6–8) | 7 (5–8) | 8 (6–8) | 7 (6–8) | <0.001 |
| After social distancing | 7 (6–8) | 8 (6–8) | 6 (4–7) | 8 (7–8) | <0.001 |
| Difference (p value) | 0.638 | <0.001 | <0.001 | 0.062 | |
| Preventive treatment, n (%) | 145 (55.6) | 42 (58.3) | 43 (50.0) | 60 (58.3) | 0.449 |
| Stopped during social distancing | 24 (16.6) | 4 (9.5) | 7 (16.3) | 13 (21.7) | 0.267 |
| Overall (n = 261) | Worsened (n = 72) | Improved (n = 86) | Stable (n = 103) | ||
|---|---|---|---|---|---|
| ISI1a | Before | 0 (0–2) | 1 (0–2) | 0 (0–2) | 1 (0–2) |
| (difficulty falling asleep) | During | 1 (0–3) | 1 (0–3) | 0 (0–3) | 1 (0–3) |
| p value | <0.001 | <0.001 | 0.011 | 0.001 | |
| ISI1b | Before | 0 (0–2) | 1 (0–2) | 0 (0–2) | 0 (0–2) |
| (difficulty staying asleep) | During | 1 (0–3) | 2 (0–3) | 1 (0–2) | 1 (0–3) |
| p value | <0.001 | 0.001 | 0.046 | 0.006 | |
| ISI1c | Before | 0 (0–2) | 0 (0–2) | 0 (0–2) | 0 (0–2) |
| (problems waking up too early) | During | 0 (0–2) | 1 (0–3) | 0 (0–2) | 0 (0–2) |
| p value | <0.001 | <0.001 | 0.506 | 0.010 | |
| ISI2 | Before | 2 (0–3) | 2 (1–2) | 2 (0–3) | 2 (0–3) |
| (satisfied/dissatisfied with sleep pattern) | During | 2 (0–3) | 2 (1–3) | 1 (0–3) | 2 (0–3) |
| p value | 0.020 | 0.002 | 0.693 | 0.469 | |
| ISI3 | Before | 1 (0–3) | 1 (0–2) | 0 (0–2) | 1 (0–3) |
| (interference with daily functioning) | During | 1 (0–3) | 1 (0–3) | 0 (0–2) | 1 (0–3) |
| p value | 0.214 | 0.079 | 0.799 | 0.207 | |
| ISI4 | Before | 0 (0–2) | 1 (0–2) | 0 (0–2) | 0 (0–2) |
| (noticeability of impairment) | During | 0 (0–2) | 1 (0–2) | 0 (0–1) | 0 (0–2) |
| p value | 0.543 | 0.166 | 0.469 | 0.507 | |
| ISI5 | Before | 0 (0–2) | 1 (0–2) | 0 (0–2) | 1 (0–2) |
| (worried/distressed about sleep problem) | During | 1 (0–2) | 2 (0–3) | 0 (0–2) | 1 (0–3) |
| p value | <0.001 | 0.004 | 0.463 | 0.001 | |
| Total score | Before | 7 (0–14) | 9 (2–14) | 5 (0–12) | 7 (1–14) |
| During | 8 (2–15) | 10 (6–18) | 6 (1–13) | 8 (2–16) | |
| p value | <0.001 | <0.001 | 0.415 | 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Stefano, V.; Ornello, R.; Gagliardo, A.; Torrente, A.; Illuminato, E.; Caponnetto, V.; Frattale, I.; Golini, R.; Di Felice, C.; Graziano, F.; et al. Social Distancing in Chronic Migraine during the COVID-19 Outbreak: Results from a Multicenter Observational Study. Nutrients 2021, 13, 1361. https://doi.org/10.3390/nu13041361
Di Stefano V, Ornello R, Gagliardo A, Torrente A, Illuminato E, Caponnetto V, Frattale I, Golini R, Di Felice C, Graziano F, et al. Social Distancing in Chronic Migraine during the COVID-19 Outbreak: Results from a Multicenter Observational Study. Nutrients. 2021; 13(4):1361. https://doi.org/10.3390/nu13041361
Chicago/Turabian StyleDi Stefano, Vincenzo, Raffaele Ornello, Andrea Gagliardo, Angelo Torrente, Elisa Illuminato, Valeria Caponnetto, Ilaria Frattale, Raffaella Golini, Chiara Di Felice, Fabiola Graziano, and et al. 2021. "Social Distancing in Chronic Migraine during the COVID-19 Outbreak: Results from a Multicenter Observational Study" Nutrients 13, no. 4: 1361. https://doi.org/10.3390/nu13041361