Dietary Pattern and Dietary Energy from Fat Associated with Sarcopenia in Community-Dwelling Older Chinese People: A Cross-Sectional Study in Three Regions of China



Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Study Design
2.2. Questionnaire and Dietary Assignment
2.3. Anthropometric Measurements
2.4. Diagnosis of Sarcopenia
2.5. DV Score Calculation and DP Assessment
2.6. Statistical Analysis
3. Results
3.1. Particpants Characteristics
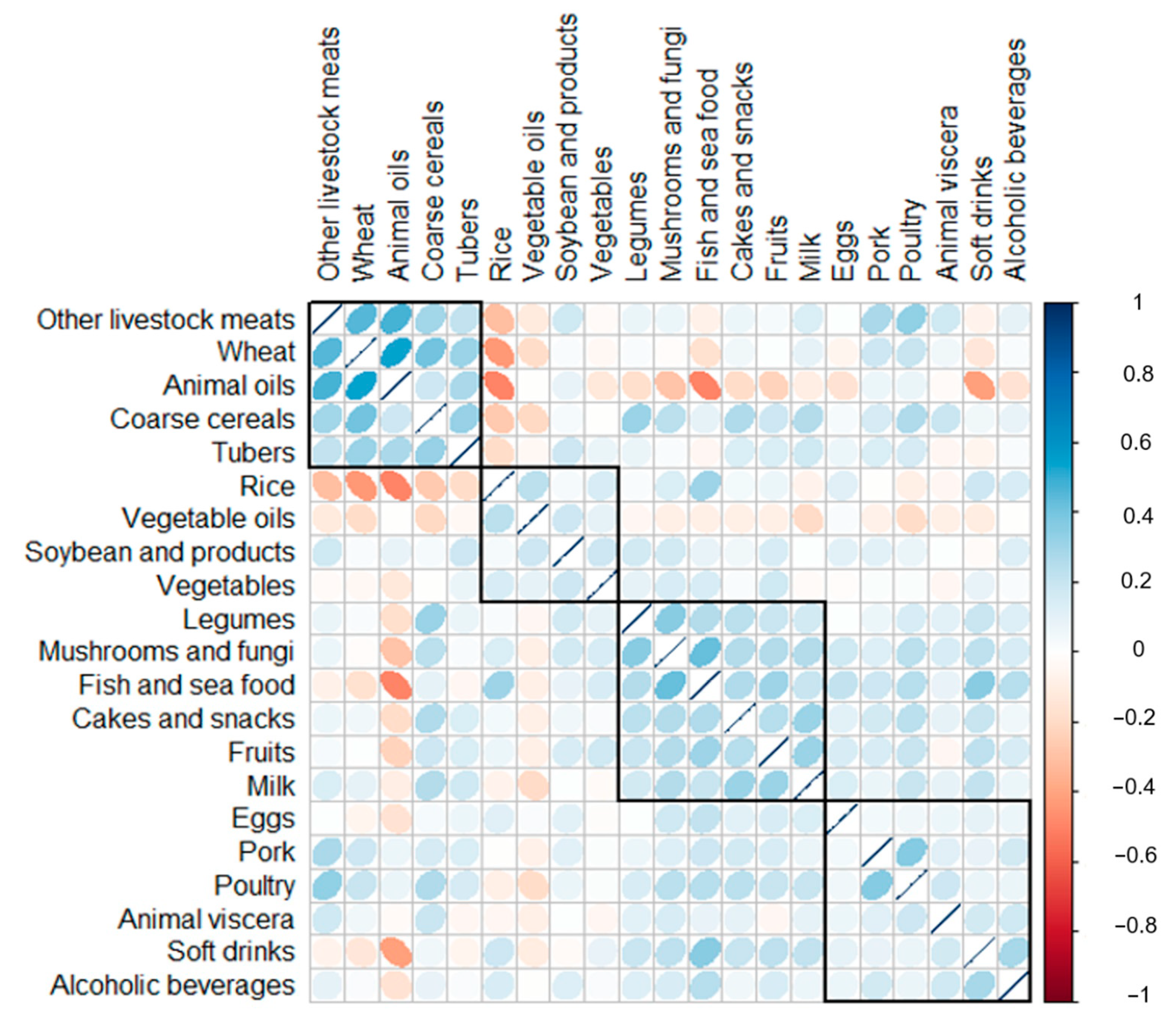
3.2. Consumption Correlations among Food Groups
3.3. Three Identified DPs in Older Subjects
3.4. Partical Correlations between DV Score, DPs Score, and Anthropometric Characteristics
3.5. Associations between DV, DPs, and Sarcopenia
3.6. Different DV Score and Nutrients Intake of Three Identified DPs
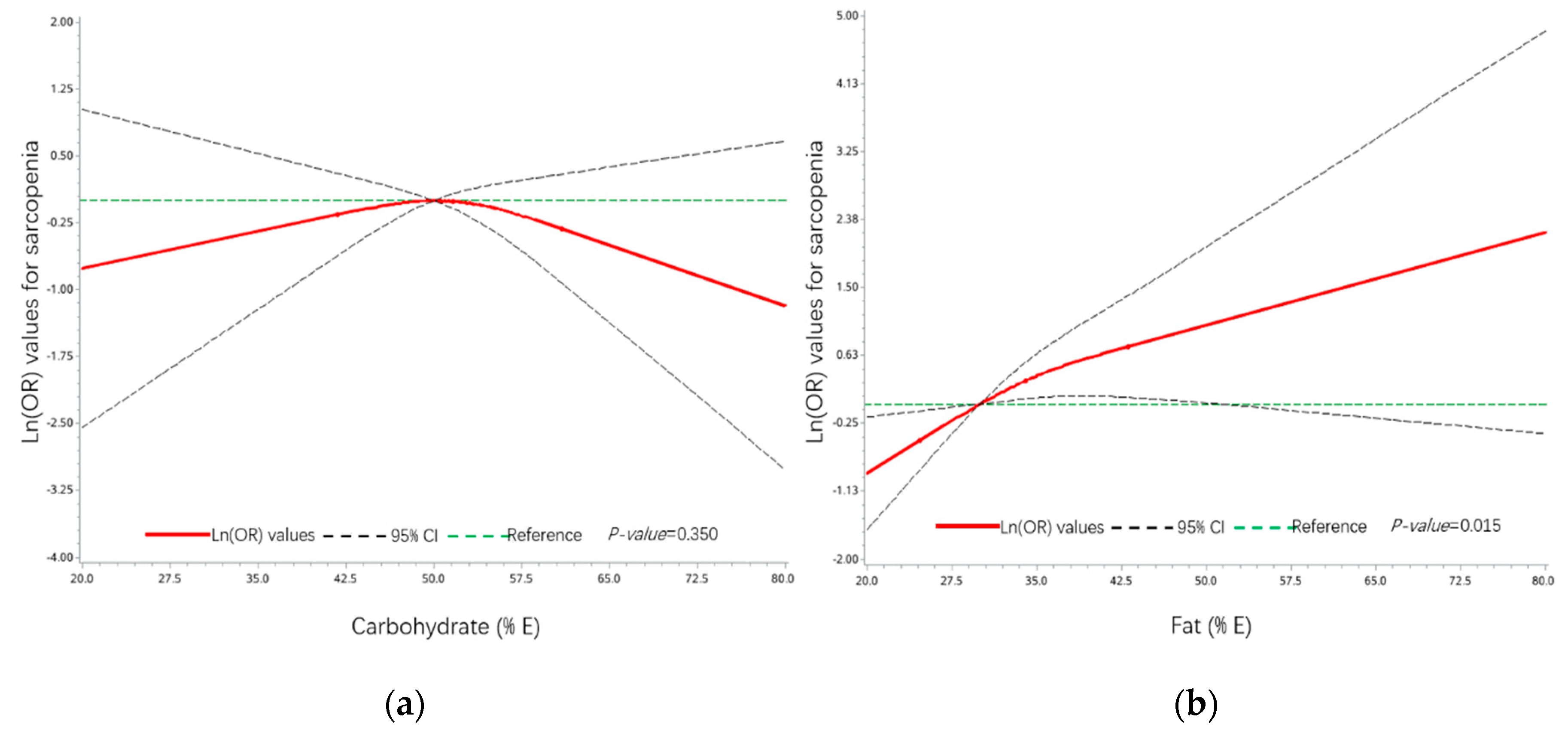
3.7. Associations between Sarcopenia and Dietary Energy Composition of Carbohydrate and Fat
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Anker, S.D.; Morley, J.E.; von Haehling, S. Welcome to the icd-10 code for sarcopenia. J. Cachexia Sarcopenia Muscle 2016, 7, 512–514. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Baeyens, J.P.; Bauer, J.M.; Boirie, Y.; Cederholm, T.; Landi, F.; Martin, F.C.; Michel, J.P.; Rolland, Y.; Schneider, S.M.; et al. Sarcopenia: European consensus on definition and diagnosis: Report of the european working group on sarcopenia in older people. Age Ageing 2010, 39, 412–423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bloom, I.; Shand, C.; Cooper, C.; Robinson, S. Diet quality and sarcopenia in older adults: A systematic review. Nutrients 2018, 10, 308. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Granic, A.; Sayer, A.A.; Robinson, S.M. Dietary patterns, skeletal muscle health, and sarcopenia in older adults. Nutrients 2019, 11, 745. [Google Scholar] [CrossRef] [Green Version]
- Rubio-Ruiz, M.E.; Guarner-Lans, V. Mechanisms underlying metabolic syndrome-related sarcopenia and possible therapeutic measures. Int. J. Mol. Sci. 2019, 20, 647. [Google Scholar] [CrossRef] [Green Version]
- Jones-McLean, E.M.; Shatenstein, B.; Whiting, S.J. Dietary patterns research and its applications to nutrition policy for the prevention of chronic disease among diverse north American populations. Appl. Physiol. Nutr. Metab. 2010, 35, 195–198. [Google Scholar] [CrossRef]
- Hu, F.B. Dietary pattern analysis: A new direction in nutritional epidemiology. Curr. Opin. Lipidol. 2002, 13, 3–9. [Google Scholar] [CrossRef]
- Ndanuko, R.N.; Tapsell, L.C.; Charlton, K.E. Dietary patterns and blood pressure in adults: A systematic review and meta-analysis of randomized controlled trials. Adv. Nutr. 2016, 7, 76–89. [Google Scholar] [CrossRef]
- Fabiani, R.; Naldini, G.; Chiavarini, M. Dietary patterns and metabolic syndrome in adult subjects: A systematic review and meta-analysis. Nutrients 2019, 11, 2056. [Google Scholar] [CrossRef] [Green Version]
- Pala, V.; Sieri, S.; Masala, G.; Palli, D.; Panico, S.; Vineis, P.; Sacerdote, C.; Mattiello, A.; Galasso, R.; Salvini, S.; et al. Associations between dietary pattern and lifestyle, anthropometry and other health indicators in the elderly participants of the epic-italy cohort. Nutr. Metab. Cardiovasc. Dis. 2006, 16, 186–201. [Google Scholar] [CrossRef]
- Fougère, B.; Mazzuco, S.; Spagnolo, P.; Guyonnet, S.; Vellas, B.; Cesari, M.; Gallucci, M. Association between the mediterranean-style dietary pattern score and physical performance: Results from trelong study. J. Nutr. Health Aging 2016, 20, 415–419. [Google Scholar] [CrossRef] [PubMed]
- Perälä, M.M.; von Bonsdorff, M.; Männistö, S.; Salonen, M.K.; Simonen, M.; Kanerva, N.; Pohjolainen, P.; Kajantie, E.; Rantanen, T.; Eriksson, J.G. A healthy nordic diet and physical performance in old age: Findings from the longitudinal helsinki birth cohort study. Br. J. Nutr. 2016, 115, 878–886. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robinson, S.M.; Westbury, L.D.; Cooper, R.; Kuh, D.; Ward, K.; Syddall, H.E.; Sayer, A.A.; Cooper, C. Adult lifetime diet quality and physical performance in older age: Findings from a british birth cohort. J. Gerontol. A Biol. Sci. Med. Sci. 2018, 73, 1532–1537. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paddon-Jones, D.; Rasmussen, B.B. Dietary protein recommendations and the prevention of sarcopenia. Curr. Opin. Clin. Nutr. Metab. Care 2009, 12, 86–90. [Google Scholar] [CrossRef] [Green Version]
- Cruz-Jentoft, A.J.; Kiesswetter, E.; Drey, M.; Sieber, C.C. Nutrition, frailty, and sarcopenia. Aging Clin. Exp. Res. 2017, 29, 43–48. [Google Scholar] [CrossRef]
- Ganapathy, A.; Nieves, J.W. Nutrition and sarcopenia—What do we know? Nutrients 2020, 12, 1755. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Sayer, A.A. Sarcopenia. Lancet 2019, 393, 2636–2646. [Google Scholar] [CrossRef]
- Oh, C.; Jeon, B.H.; Reid Storm, S.N.; Jho, S.; No, J.K. The most effective factors to offset sarcopenia and obesity in the older korean: Physical activity, vitamin d, and protein intake. Nutrition 2017, 33, 169–173. [Google Scholar] [CrossRef]
- Polyzos, S.A.; Margioris, A.N. Sarcopenic obesity. Hormones 2018, 17, 321–331. [Google Scholar] [CrossRef]
- Ewaschuk, J.B.; Almasud, A.; Mazurak, V.C. Role of n-3 fatty acids in muscle loss and myosteatosis. Appl. Physiol. Nutr. Metab. 2014, 39, 654–662. [Google Scholar] [CrossRef]
- Tessier, A.J.; Chevalier, S. An update on protein, leucine, omega-3 fatty acids, and vitamin d in the prevention and treatment of sarcopenia and functional decline. Nutrients 2018, 10, 1099. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fan, M.; Lyu, J.; He, P. Chinese guidelines for data processing and analysis concerning the international physical activity questionnaire. Zhonghua Liu Xing Bing Xue Za Zhi 2014, 35, 961–964. [Google Scholar]
- He, Y.; Li, Y.; Yang, X.; Hemler, E.C.; Fang, Y.; Zhao, L.; Zhang, J.; Yang, Z.; Wang, Z.; He, L.; et al. The dietary transition and its association with cardiometabolic mortality among Chinese adults, 1982–2012: A cross-sectional population-based study. Lancet Diabetes Endocrinol. 2019, 7, 540–548. [Google Scholar] [CrossRef]
- Yin, Z.; Chen, J.; Zhang, J.; Ren, Z.; Dong, K.; Kraus, V.B.; Wang, Z.; Zhang, M.; Zhai, Y.; Song, P. Dietary patterns associated with cognitive function among the older people in underdeveloped regions: Finding from the NCDFaC study. Nutrients 2018, 10, 464. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, Y.; Wang, G.; Pan, X. China Food Composition; Peking University Medical Press: Beijing, China, 2002. [Google Scholar]
- Tosato, M.; Marzetti, E.; Cesari, M.; Savera, G.; Miller, R.R.; Bernabei, R.; Landi, F.; Calvani, R. Measurement of muscle mass in sarcopenia: From imaging to biochemical markers. Aging Clin. Exp. Res. 2017, 29, 19–27. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised european consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, L.K.; Liu, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Bahyah, K.S.; Chou, M.Y.; Chen, L.Y.; Hsu, P.S.; Krairit, O.; et al. Sarcopenia in Asia: Consensus report of the Asian working group for sarcopenia. J. Am. Med. Dir. Assoc. 2014, 15, 95–101. [Google Scholar] [CrossRef]
- Liu, X.; Hao, Q.; Hou, L.; Xia, X.; Zhao, W.; Zhang, Y.; Ge, M.; Liu, Y.; Zuo, Z.; Yue, J.; et al. Ethnic groups differences in the prevalence of sarcopenia using the awgs criteria. J. Nutr. Health Aging 2020, 24, 665–671. [Google Scholar] [CrossRef]
- Chen, L.-K.; Woo, J.; Assantachai, P.; Auyeung, T.-W.; Chou, M.-Y.; Iijima, K.; Jang, H.C.; Kang, L.; Kim, M.; Kim, S.; et al. Asian working group for sarcopenia: 2019 consensus update on sarcopenia diagnosis and treatment. J. Am. Med. Dir. Assoc. 2020, 21, 300–307. [Google Scholar] [CrossRef]
- Kim, S.; Haines, P.S.; Siega-Riz, A.M.; Popkin, B.M. The diet quality index-international (DQI-I) provides an effective tool for cross-national comparison of diet quality as illustrated by China and the United States. J. Nutr. 2003, 133, 3476–3484. [Google Scholar] [CrossRef]
- Woo, J.; Cheung, B.; Ho, S.; Sham, A.; Lam, T.H. Influence of dietary pattern on the development of overweight in a Chinese population. Eur. J. Clin. Nutr. 2008, 62, 480–487. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chan, R.; Chan, D.; Woo, J. Associations between dietary patterns and demographics, lifestyle, anthropometry and blood pressure in Chinese community-dwelling older men and women. J. Nutr. Sci. 2012, 1, e20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hashemi, R.; Motlagh, A.D.; Heshmat, R.; Esmaillzadeh, A.; Payab, M.; Yousefinia, M.; Siassi, F.; Pasalar, P.; Baygi, F. Diet and its relationship to sarcopenia in community dwelling iranian elderly: A cross sectional study. Nutrition 2015, 31, 97–104. [Google Scholar] [CrossRef] [PubMed]
- Chan, R.; Leung, J.; Woo, J. A prospective cohort study to examine the association between dietary patterns and sarcopenia in Chinese community-dwelling older people in Hong Kong. J. Am. Med. Dir. Assoc. 2016, 17, 336–342. [Google Scholar] [CrossRef] [PubMed]
- Tieland, M.; Borgonjen-Van den Berg, K.J.; van Loon, L.J.; de Groot, L.C. Dietary protein intake in community-dwelling, frail, and institutionalized elderly people: Scope for improvement. Eur. J. Nutr. 2012, 51, 173–179. [Google Scholar] [CrossRef]
- Groen, B.B.; Res, P.T.; Pennings, B.; Hertle, E.; Senden, J.M.; Saris, W.H.; van Loon, L.J. Intragastric protein administration stimulates overnight muscle protein synthesis in elderly men. Am. J. Physiol. Endocrinol. Metab. 2012, 302, 52–60. [Google Scholar] [CrossRef]
- Scott, D.; Blizzard, L.; Fell, J.; Giles, G.; Jones, G. Associations between dietary nutrient intake and muscle mass and strength in community-dwelling older adults: The tasmanian older adult cohort study. J. Am. Geriatr. Soc. 2010, 58, 2129–2134. [Google Scholar] [CrossRef]
- Morais, J.A.; Chevalier, S.; Gougeon, R. Protein turnover and requirements in the healthy and frail elderly. J. Nutr. Health Aging 2006, 10, 272–283. [Google Scholar]
- Bauer, J.; Biolo, G.; Cederholm, T.; Cesari, M.; Cruz-Jentoft, A.J.; Morley, J.E.; Phillips, S.; Sieber, C.; Stehle, P.; Teta, D.; et al. Evidence-based recommendations for optimal dietary protein intake in older people: A position paper from the prot-age study group. J. Am. Med. Dir. Assoc. 2013, 14, 542–559. [Google Scholar] [CrossRef]
- Deutz, N.E.; Bauer, J.M.; Barazzoni, R.; Biolo, G.; Boirie, Y.; Bosy-Westphal, A.; Cederholm, T.; Cruz-Jentoft, A.; Krznariç, Z.; Nair, K.S.; et al. Protein intake and exercise for optimal muscle function with aging: Recommendations from the espen expert group. Clin. Nutr. 2014, 33, 929–936. [Google Scholar] [CrossRef] [Green Version]
- Lancha, A.H., Jr.; Zanella, R., Jr.; Tanabe, S.G.; Andriamihaja, M.; Blachier, F. Dietary protein supplementation in the elderly for limiting muscle mass loss. Amino Acids 2017, 49, 33–47. [Google Scholar] [CrossRef] [PubMed]
- Granic, A.; Mendonça, N.; Sayer, A.A.; Hill, T.R.; Davies, K.; Siervo, M.; Mathers, J.C.; Jagger, C. Effects of dietary patterns and low protein intake on sarcopenia risk in the very old: The newcastle 85+ study. Clin. Nutr. 2020, 39, 166–173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santos, C.S.; Nascimento, F.E.L. Isolated branched-chain amino acid intake and muscle protein synthesis in humans: A biochemical review. Einstein 2019, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jackman, S.R.; Witard, O.C.; Philp, A.; Wallis, G.A.; Baar, K.; Tipton, K.D. Branched-chain amino acid ingestion stimulates muscle myofibrillar protein synthesis following resistance exercise in humans. Front. Physiol. 2017, 8, 390. [Google Scholar] [CrossRef] [PubMed]
- Komar, B.; Schwingshackl, L.; Hoffmann, G. Effects of leucine-rich protein supplements on anthropometric parameter and muscle strength in the elderly: A systematic review and meta-analysis. J. Nutr. Health Aging 2015, 19, 437–446. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization, Food and Agriculture Organization of the United Nations, United Nations University. Protein and Amino Acid Requirements in Human Nutrition; Report of a Joint FAO/WHO/UNU Expert Consultation (WHO Technical Report Series 935); World Health Organization: Geneva, Switzerland, 2007; pp. 1–265. [Google Scholar]
- Cleasby, M.E.; Jamieson, P.M.; Atherton, P.J. Insulin resistance and sarcopenia: Mechanistic links between common co-morbidities. J. Endocrinol. 2016, 229, 67–81. [Google Scholar] [CrossRef]
- Morales, P.E.; Bucarey, J.L. Muscle lipid metabolism: Role of lipid droplets and perilipins. J. Diabetes Res. 2017, 2017, 1789395. [Google Scholar] [CrossRef]
- Pellegrinelli, V.; Rouault, C.; Rodriguez-Cuenca, S.; Albert, V.; Edom-Vovard, F.; Vidal-Puig, A.; Clément, K.; Butler-Browne, G.S.; Lacasa, D. Human adipocytes induce inflammation and atrophy in muscle cells during obesity. Diabetes 2015, 64, 3121–3134. [Google Scholar] [CrossRef] [Green Version]
- Jeppesen, J.; Albers, P.H.; Rose, A.J.; Birk, J.B.; Schjerling, P.; Dzamko, N.; Steinberg, G.R.; Kiens, B. Contraction-induced skeletal muscle fat/cd36 trafficking and fa uptake is ampk independent. J. Lipid. Res. 2011, 52, 699–711. [Google Scholar] [CrossRef] [Green Version]
- Li, X.; Li, Z.; Zhao, M.; Nie, Y.; Liu, P.; Zhu, Y.; Zhang, X. Skeletal muscle lipid droplets and the athlete’s paradox. Cells 2019, 8, 249. [Google Scholar] [CrossRef] [Green Version]
- Bickel, P.E.; Tansey, J.T.; Welte, M.A. Pat proteins, an ancient family of lipid droplet proteins that regulate cellular lipid stores. Biochim. Biophys. Acta 2009, 1791, 419–440. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonen, A.; Jain, S.S.; Snook, L.A.; Han, X.X.; Yoshida, Y.; Buddo, K.H.; Lally, J.S.; Pask, E.D.; Paglialunga, S.; Beaudoin, M.S.; et al. Extremely rapid increase in fatty acid transport and intramyocellular lipid accumulation but markedly delayed insulin resistance after high fat feeding in rats. Diabetologia 2015, 58, 2381–2391. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rinnankoski-Tuikka, R.; Hulmi, J.J.; Torvinen, S.; Silvennoinen, M.; Lehti, M.; Kivelä, R.; Reunanen, H.; Kujala, U.M.; Kainulainen, H. Lipid droplet-associated proteins in high-fat fed mice with the effects of voluntary running and diet change. Metabolism 2014, 63, 1031–1040. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Engin, A.B. What is lipotoxicity? Adv. Exp. Med. Biol. 2017, 960, 197–220. [Google Scholar] [PubMed]
- Meng, S.J.; Yu, L.J. Oxidative stress, molecular inflammation and sarcopenia. Int. J. Mol. Sci. 2010, 11, 1509–1526. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dimitriadis, G.; Mitrou, P.; Lambadiari, V.; Maratou, E.; Raptis, S.A. Insulin effects in muscle and adipose tissue. Diabetes Res. Clin. Pract. 2011, 93 (Suppl. S1), 52–59. [Google Scholar] [CrossRef]
- Abdulla, H.; Smith, K.; Atherton, P.J.; Idris, I. Role of insulin in the regulation of human skeletal muscle protein synthesis and breakdown: A systematic review and meta-analysis. Diabetologia 2016, 59, 44–55. [Google Scholar] [CrossRef]
- Tardif, N.; Salles, J.; Guillet, C.; Tordjman, J.; Reggio, S.; Landrier, J.F.; Giraudet, C.; Patrac, V.; Bertrand-Michel, J.; Migne, C.; et al. Muscle ectopic fat deposition contributes to anabolic resistance in obese sarcopenic old rats through eif2α activation. Aging Cell 2014, 13, 1001–1011. [Google Scholar] [CrossRef]
- Wang, X.; Hu, Z.; Hu, J.; Du, J.; Mitch, W.E. Insulin resistance accelerates muscle protein degradation: Activation of the ubiquitin-proteasome pathway by defects in muscle cell signaling. Endocrinology 2006, 147, 4160–4168. [Google Scholar] [CrossRef] [Green Version]
- Jeon, J.Y.; Choi, S.E.; Ha, E.S.; Lee, H.B.; Kim, T.H.; Han, S.J.; Kim, H.J.; Kim, D.J.; Kang, Y.; Lee, K.W. Glp-1 improves palmitate-induced insulin resistance in human skeletal muscle via sirt1 activity. Int. J. Mol. Med. 2019, 44, 1161–1171. [Google Scholar] [CrossRef]
- Nieuwoudt, S.; Mulya, A.; Fealy, C.E.; Martelli, E.; Dasarathy, S.; Naga Prasad, S.V.; Kirwan, J.P. In vitro contraction protects against palmitate-induced insulin resistance in c2c12 myotubes. Am. J. Physiol. Cell Physiol. 2017, 313, 575–583. [Google Scholar] [CrossRef] [PubMed]
- Tardif, N.; Salles, J.; Landrier, J.F.; Mothe-Satney, I.; Guillet, C.; Boue-Vaysse, C.; Combaret, L.; Giraudet, C.; Patrac, V.; Bertrand-Michel, J.; et al. Oleate-enriched diet improves insulin sensitivity and restores muscle protein synthesis in old rats. Clin. Nutr. 2011, 30, 799–806. [Google Scholar] [CrossRef] [PubMed]
- Coll, T.; Eyre, E.; Rodríguez-Calvo, R.; Palomer, X.; Sánchez, R.M.; Merlos, M.; Laguna, J.C.; Vázquez-Carrera, M. Oleate reverses palmitate-induced insulin resistance and inflammation in skeletal muscle cells. J. Biol. Chem. 2008, 283, 11107–11116. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Characteristic | Total | Sarcopenia | ||
|---|---|---|---|---|
| Yes | No | p-Value | ||
| Subjects | 861 (100.0) | 132 (15.3) | 729 (84.7) | |
| Age (y) | 71.0 ± 4.8 | 74.2 ± 5.4 | 70.4 ± 4.4 | <0.001 |
| BMI (kg/m2) | 23.8 ± 3.6 | 21.2 ± 3.5 | 24.3 ± 3.4 | <0.001 |
| Gender | ||||
| Male | 405 (47.0) | 62 (15.3) | 343 (84.7) | 0.986 |
| Female | 456 (53.0) | 70 (15.4) | 386 (84.6) | |
| Region | ||||
| South China (Yuexiu) | 286 (33.2) | 35 (12.2) | 251 (87.8) | 0.092 |
| Middle China (Taicang) | 311 (36.1) | 47 (15.1) | 264 (84.9) | |
| North China (Wuyuan) | 264 (30.7) | 50 (18.9) | 214 (81.1) | |
| Exercise activity | ||||
| Low | 20 (2.3) | 5 (25.0) | 15 (75.0) | 0.257 |
| Moderate | 485 (56.3) | 79 (16.3) | 406 (83.7) | |
| Heavy | 356 (41.4) | 48 (13.5) | 308 (86.5) | |
| Lifestyle | ||||
| Living alone | 87 (10.1) | 13 (14.9) | 74 (85.1) | 0.401 |
| Living with spouse | 656 (76.2) | 96 (14.6) | 560 (85.4) | |
| Living with others | 118 (13.7) | 23 (19.5) | 95 (80.5) | |
| Current smoker | ||||
| Yes | 204 (23.7) | 41 (20.1) | 163 (79.9) | 0.031 |
| No | 657 (76.3) | 91 (13.9) | 566 (86.2) | |
| NCDs | ||||
| Hypertension | 417 (48.4) | 63 (15.1) | 354 (84.9) | 0.86 |
| T2D | 113 (13.1) | 13 (11.5) | 100 (88.5) | 0.226 |
| CVD | 178 (20.7) | 31 (17.4) | 147 (82.6) | 0.386 |
| Cluster | Food Group | DP1 | DP2 | DP3 |
|---|---|---|---|---|
| Cluster 1 | Other livestock meats | 0.351 | −0.013 | 0.689 |
| Wheat | 0.653 | −0.036 | 0.240 | |
| Animal oils | 0.583 | −0.373 | 0.129 | |
| Coarse cereals | 0.442 | 0.416 | 0.069 | |
| Tubers | 0.550 | 0.149 | 0.056 | |
| Cluster 2 | Rice | −0.714 | 0.120 | 0.031 |
| Vegetable oils | −0.351 | −0.144 | −0.015 | |
| Soybean and products | −0.016 | 0.309 | 0.182 | |
| Vegetables | −0.111 | 0.173 | −0.059 | |
| Cluster 3 | Legumes | 0.064 | 0.353 | 0.105 |
| Mushrooms and fungi | 0.141 | 0.596 | 0.104 | |
| Fish and seafood | −0.244 | 0.428 | 0.235 | |
| Cakes and snacks | 0.183 | 0.512 | 0.055 | |
| Fruits | −0.023 | 0.553 | 0.050 | |
| Milk | 0.243 | 0.583 | −0.049 | |
| Cluster 4 | Eggs | −0.026 | 0.216 | 0.194 |
| Pork | −0.031 | 0.112 | 0.697 | |
| Poultry | 0.126 | 0.092 | 0.733 | |
| Animal viscera | −0.053 | 0.019 | 0.380 | |
| Soft drinks | −0.070 | 0.305 | −0.058 | |
| Alcoholic beverages | −0.319 | −0.025 | 0.129 | |
| Variance explained (%) | 13.8 | 10 | 7 | |
| Characteristic | DV Score | DP1 Score | DP2 Score | DP3 Score | ||||
|---|---|---|---|---|---|---|---|---|
| r | p-Value | r | p-Value | r | p-Value | r | p-Value | |
| MUAC | 0.02 | 0.574 | 0.03 | 0.402 | 0.04 | 0.254 | −0.03 | 0.4 |
| CC | 0.02 | 0.512 | 0.07 | 0.056 | 0.12 | <0.001 | −0.06 | 0.09 |
| WC | −0.02 | 0.51 | 0.09 | 0.007 | 0.04 | 0.212 | −0.03 | 0.34 |
| PBF | −0.03 | 0.376 | 0.21 | <0.001 | 0.02 | 0.588 | −0.03 | 0.325 |
| VFA | −0.02 | 0.619 | 0.20 | <0.001 | 0.04 | 0.264 | −0.03 | 0.333 |
| FFM | 0.07 | 0.037 | 0.06 | 0.061 | 0.12 | <0.001 | <0.01 | 0.99 |
| BMC | 0.08 | 0.016 | 0.02 | 0.511 | 0.12 | <0.001 | −0.02 | 0.62 |
| Grip strength | 0.08 | 0.014 | 0.05 | 0.128 | 0.07 | 0.044 | 0.08 | 0.015 |
| Gait speed | 0.08 | 0.014 | 0.07 | 0.032 | 0.09 | 0.009 | 0.05 | 0.169 |
| SMI | 0.03 | 0.426 | 0.06 | 0.075 | 0.11 | 0.002 | −0.03 | 0.362 |
| DP | Model 1 | Model 2 | Model 3 | Model 4 | ||||
|---|---|---|---|---|---|---|---|---|
| OR 95%CI | p-Trend | OR 95%CI | p-Trend | OR 95%CI | p-Trend | OR 95%CI | p-Trend | |
| DV score | ||||||||
| Q1 a | Ref | 0.008 | Ref | 0.071 | Ref | 0.059 | Ref | 0.099 |
| Q2 | 0.64 (0.38, 1.07) | 0.69 (0.40, 1.19) | 0.51 (0.28, 0.95) | 0.51 (0.28, 0.96) | ||||
| Q3 | 0.37 (0.20, 0.71) | 0.41 (0.21, 0.81) | 0.33 (0.15, 0.70) | 0.35 (0.16, 0.75) | ||||
| Q4 | 0.50 (0.30, 0.84) | 0.59 (0.33, 1.08) | 0.49 (0.24, 0.97) | 0.52 (0.26, 1.05) | ||||
| DP1 | ||||||||
| Q1 b | Ref | 0.45 | Ref | 0.345 | Ref | 0.619 | Ref | 0.689 |
| Q2 | 0.76 (0.44, 1.32) | 0.67 (0.36, 1.22) | 0.63 (0.31, 1.28) | 0.63 (0.31, 1.27) | ||||
| Q3 | 1.18 (0.71, 1.96) | 1.03 (0.45, 2.34) | 1.28 (0.51, 3.17) | 1.28 (0.51, 3.23) | ||||
| Q4 | 1.07 (0.64, 1.80) | 0.68 (0.27, 1.76) | 0.80 (0.28, 2.30) | 0.85 (0.29, 2.47) | ||||
| DP2 | ||||||||
| Q1 c | Ref | <0.001 | Ref | <0.001 | Ref | 0.006 | Ref | 0.009 |
| Q2 | 0.64 (0.40, 1.04) | 0.71 (0.41, 1.20) | 0.82 (0.46, 1.48) | 0.81 (0.45, 1.46) | ||||
| Q3 | 0.46 (0.28, 0.77) | 0.47 (0.26, 0.85) | 0.53 (0.27, 1.03) | 0.53 (0.27, 1.04) | ||||
| Q4 | 0.29 (0.17, 0.52) | 0.30 (0.15, 0.60) | 0.32 (0.14, 0.75) | 0.33 (0.14, 0.77) | ||||
| DP3 | ||||||||
| Q1 d | Ref | 0.313 | Ref | 0.673 | Ref | 0.863 | Ref | 0.807 |
| Q2 | 0.87 (0.52, 1.45) | 0.81 (0.48, 1.38) | 0.63 (0.34, 1.16) | 0.63 (0.34, 1.17) | ||||
| Q3 | 0.87 (0.52, 1.46) | 0.91 (0.53, 1.56) | 0.79 (0.42, 1.47) | 0.82 (0.43, 1.52) | ||||
| Q4 | 0.75 (0.44, 1.27) | 0.85 (0.48, 1.52) | 0.91 (0.44, 1.89) | 0.87 (0.41, 1.82) | ||||
| Characteristic | DP1 (n = 215) | DP2 (n = 215) | DP3 (n = 215) | p-Value |
|---|---|---|---|---|
| Generalcharacteristic | ||||
| Age (y) | 71.3 ± 5.1 | 70.4 ± 4.6 | 69.9 ± 4.2 a | 0.025 |
| BMI (kg/m2) | 23.9 ± 4.0 | 24.1 ± 3.2 | 23.6 ± 3.3 | 0.318 |
| Male (n, %) | 104 (48.4) | 100 (46.5) | 138 (64.2) ab | <0.001 |
| Sarcopenia (n, %) | 35 (16.3) | 18 (8.4) a | 29 (13.5) | 0.044 |
| Food variety score of DQI-I | ||||
| Overall food variety score | 10.3 ± 3.3 | 13.4 ± 2.2 a | 11.2 ± 2.8 ab | <0.001 |
| Protein variety score | 2.0 ± 1.3 | 3.3 ± 1.2 a | 2.7 ± 1.3 ab | <0.001 |
| Total variety score | 12.7 ± 4.6 | 17.5 ± 3.2 a | 14.4 ± 3.9 ab | <0.001 |
| Dietary nutrients intake and composition | ||||
| Energy (kcal) | 2190.8 ± 855.2 | 2468.4 ± 788.5 a | 2555.1 ± 776.8 a | <0.001 |
| Carbohydrate (g) | 272.9 ± 121.0 | 324.7 ± 106.6 a | 283.7 ± 102.6 b | <0.001 |
| Protein (g) | 77.6 ± 42.7 | 101.5 ± 39.3 a | 102.1 ± 42.1 a | <0.001 |
| Protein per weight (g/kg) | 1.3 ± 0.7 | 1.7 ± 0.7 a | 1.7 ± 0.7 a | <0.001 |
| Fat (g) | 89.6 ± 46.3 | 87.1 ± 41.5 | 108.5 ± 44.6 ab | <0.001 |
| PEC (%E) | 49.9 ± 11.8 | 53.4 ± 9.5 a | 44.6 ± 10.0 ab | <0.001 |
| PEP (%E) | 13.7 ± 2.8 | 16.4 ± 2.9 a | 16.0 ± 3.6 a | <0.001 |
| PEF (%E) | 37.2 ± 12.1 | 31.2 ± 8.6 a | 38.3 ± 10.3 b | <0.001 |
| Calcium (mg) | 553.2 ± 379.0 | 871.1 ± 373.8 a | 620.9 ± 343.6 ab | <0.001 |
| Phosphorus (mg) | 1246.9 ± 643.6 | 1624.6 ± 575.9 a | 1468.6 ± 592.0 ab | <0.001 |
| Magnesium (mg) | 372.8 ± 204.5 | 483.5 ± 186.9 a | 409.8 ± 178.8 ab | <0.001 |
| Potassium (mg) | 2418.9 ± 1317.3 | 3368.3 ± 1242.1 a | 2790.8 ± 1245.1 ab | <0.001 |
| Valine (mg/kg) | 44.6 ± 27.0 | 55.8 ± 30.1 a | 58.5 ± 30.5 a | <0.001 |
| Leucine (mg/kg) | 68.6 ± 42.9 | 85.6 ± 47.3 a | 89.5 ± 47.9 a | <0.001 |
| Isoleucine (mg/kg) | 37.5 ± 23.7 | 47.7 ± 26.6 a | 50.6 ± 27.2 a | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, C.; Kang, B.; Zhang, T.; Gu, H.; Song, P.; Chen, J.; Wang, X.; Xu, B.; Zhao, W.; Zhang, J. Dietary Pattern and Dietary Energy from Fat Associated with Sarcopenia in Community-Dwelling Older Chinese People: A Cross-Sectional Study in Three Regions of China. Nutrients 2020, 12, 3689. https://doi.org/10.3390/nu12123689
Li C, Kang B, Zhang T, Gu H, Song P, Chen J, Wang X, Xu B, Zhao W, Zhang J. Dietary Pattern and Dietary Energy from Fat Associated with Sarcopenia in Community-Dwelling Older Chinese People: A Cross-Sectional Study in Three Regions of China. Nutrients. 2020; 12(12):3689. https://doi.org/10.3390/nu12123689
Chicago/Turabian StyleLi, Cheng, Bingxian Kang, Ting Zhang, Hongru Gu, Pengkun Song, Jingyi Chen, Xile Wang, Bin Xu, Wenhua Zhao, and Jian Zhang. 2020. "Dietary Pattern and Dietary Energy from Fat Associated with Sarcopenia in Community-Dwelling Older Chinese People: A Cross-Sectional Study in Three Regions of China" Nutrients 12, no. 12: 3689. https://doi.org/10.3390/nu12123689