Dietary Contributors to Food Group Intake in Preschool Children Attending Family Childcare Homes: Differences between Latino and Non-Latino Providers

 , , , ,
, , , ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Measures
2.1.1. FCCPs and Children Demographics
2.1.2. Child Dietary Intake
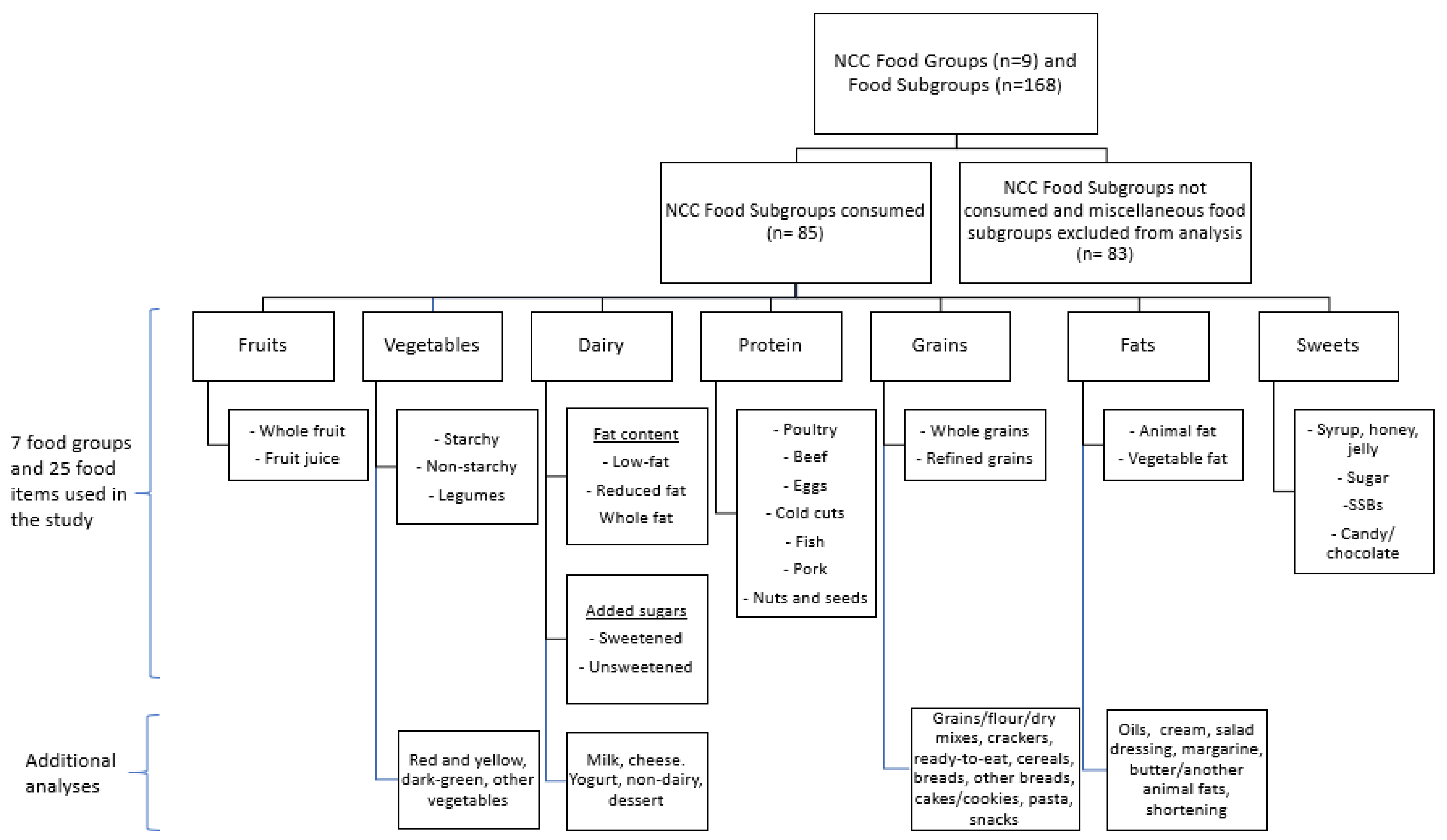
2.1.3. Food Groups and Food Items
2.2. Statistical Analysis
2.2.1. Food Item and Food Group Intake in FCCH
2.2.2. Contribution of Food Items to Major Food Groups
2.2.3. Differences between Latino and non-Latino FCCPs
3. Results
3.1. Demographics
3.2. Food Group Intake
3.3. Contribution of Food Items to Major Food Groups
3.4. Differences between Latino and non-Latino FCCPs
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Birch, L.L.; Fisher, J. Development of eating behaviors among children and adolescents. Pediatrics 1998, 101, 539–549. [Google Scholar] [PubMed]
- Ventura, A.K.; Worobey, J. Early Influences on the Development of Food Preferences. Curr. Biol. 2013, 23, R401–R408. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reidy, K.C.; Deming, D.M.; Briefel, R.R.; Fox, M.K.; Saavedra, J.M.; Eldridge, A.L. Early development of dietary patterns: Transitions in the contribution of food groups to total energy—Feeding Infants and Toddlers Study, 2008. BMC Nutr. 2017, 3, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Larson, N.; Story, M. A review of environmental influences on food choices. Ann. Behav. Med. 2009, 38, 56–73. [Google Scholar] [CrossRef] [PubMed]
- Mikkelsen, M.V.; Husby, S.; Skov, L.R.; Perez-cueto, F.J.A. A systematic review of types of healthy eating interventions in preschools. Nutr. J. 2014, 13, 1–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Summary Report: Interventions on Diet and Physical Activity: What Works? World Health Organization Press: Geneva, Switzerland, 2009. [Google Scholar]
- Gerritsen, S.; Dean, B.; Morton, S.M.B.; Wall, C.R. Do childcare menus meet nutrition guidelines? Quantity, variety and quality of food provided in New Zealand Early Childhood Education services. Aust. N. Z. J. Public Health 2017, 41, 345–351. [Google Scholar] [CrossRef] [PubMed]
- Francis, L.; Shodeinde, L.; Black, M.M.; Allen, J. Examining the Obesogenic Attributes of the Family Child Care Home Environment: A Literature Review. J. Obes. 2018. [Google Scholar] [CrossRef]
- Federal Interagency Forum on Child and Family. Statistics. America’s Children: Key National Indicators of Well-Being; Federal Interagency Forum on Child and Family: Washington, DC, USA, 2002. [Google Scholar]
- Laughlin, L. Who’s Minding the Kids? Child. Care Arrangements: Spring 2011. In Current Population Reports; U.S. Census Bureau: Washington, DC, USA, 2013. [Google Scholar]
- Jones, B.; Fiese, B.; Team, S.K. Parent routines, child routines, and family demographics associated with obesity in parents and preschool-aged children. Front. Psychol. 2014, 29, 374. [Google Scholar] [CrossRef] [Green Version]
- Benjamin-neelon, S.E.; Vaughn, A.E.; Tovar, A.; Østbye, T.; Mazzucca, S.; Ward, D.S. The family child care home environment and children’s diet quality. Appetite 2018, 126, 108–113. [Google Scholar] [CrossRef]
- Larson, N.; Ward, D.S.; Neelon, S.B.; Story, M. What Role Can Child-Care Settings Play in and Call for Research Efforts. JADA 2011, 111, 1343–1362. [Google Scholar] [CrossRef]
- Erinosho, T.O.; Ball, S.C.; Hanson, P.P.; Vaughn, A.E.; Ward, D.S. Assessing foods offered to children at child-care centers using the Healthy Eating Index-2005. J. Acad Nutr Diet. 2017, 46, 1247–1262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benjamin, S.E.; Copeland, K.A.; Cradock, A.; Neelon, B.; Walker, E.; Slining, M.M.; Gillman, M.W. Menus in Child Care: A Comparison of State Regulations with National Standards. J. Am. Diet. Assoc. 2009, 109, 109–115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brennan, L.; Castro, S.; Brownson, R.C.; Claus, J.; Orleans, C.T. Accelerating Evidence Reviews and Broadening Evidence Standards to Identify Effective, Promising, and Emerging Policy and Environmental Strategies for Prevention of Childhood Obesity. Annu. Rev. Public Health 2011, 32, 199–223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lindsay, A.C.; Salkeld, J.A.; Greaney, M.L.; Sands, F.D. Latino Family Childcare Providers’ Beliefs, Attitudes, and Practices Related to Promotion of Healthy Behaviors among Preschool Children: A Qualitative Study. J. Obes. 2015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosenthal, M.S.; Crowley, A.A.; Curry, L. Family Child Care Providers’ Self-perceived Role in Obesity Prevention: Working with Children, Parents, and External Influences. J. Nutr. Educ. Behav. 2013, 45, 595–601. [Google Scholar] [CrossRef] [PubMed]
- Otten, J.J.; Hirsch, T.; Lim, C. Factors Influencing the Food Purchases of Early Care and Education Providers. J. Acad. Nutr. Diet. 2017, 117, 725–734. [Google Scholar] [CrossRef]
- US Department of Agriculture Child and Adult Care Food Program (CACFP): Why CACFP is Important. Available online: https://www.fns.usda.gov/cacfp/why-cacfp-important (accessed on 22 May 2019).
- Korenman, S.; Abner, K.S.; Kaestner, R.; Gordon, R.A. The Child and Adult Care Food Program and the Nutrition of Preschoolers. Early Child. Res. Q. 2013, 28, 220–231. [Google Scholar] [CrossRef] [Green Version]
- Tovar, A.; Risica, P.; Mena, N.; Lawson, E.; Ankoma, A.; Gans, K.M. An Assessment of Nutrition Practices and Attitudes in Family Child-Care Homes: Implications for Policy Implementation. Public Health Res. Pract. Policy 2015, 12, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Gans, K.M.; Tovar, A.; Jiang, Q.; Mello, J.; Dionne, L.; Kang, A.; Mena, N.Z.; Palomo, V.; Risica, P.M. Nutrition-related practices of family child care providers and differences by ethnicity. Child. Obes. 2019, 15, 167–184. [Google Scholar] [CrossRef]
- Tovar, A.; Risica, P.M.; Ramirez, A.; Mena, N.; Lofgren, I.E.; Stowers, K.C.; Gans, K.M. Exploring the provider-level socio-demographic determinants of diet quality of preschool-aged children attending family childcare homes. Nutrients 2020, 12, 1368. [Google Scholar] [CrossRef]
- Freedman, M.R.; Alvarez, K.P. Early Childhood Feeding: Assessing Knowledge, Attitude, and Practices of Multi-Ethnic Child-Care Providers. JADA 2010, 110, 447–451. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tovar, A.; Mena, N.Z.; Risica, P.; Gorham, G.; Gans, K.M. Nutrition and physical activity environments of home-based child care: What hispanic providers have to say. Child. Obes. 2015, 11, 521–529. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hiza, H.; Casavale, K.; Guenther, P.M.; Davis, C. Diet Quality of Americans Differs by Age, Sex, Race/Ethinicty, Income and Education Level. J. Acad. Nutr. Diet. 2012, 113, 297–306. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.D.; Leung, C.W.; Li, Y.; Ding, E.L.; Chiuve, S.E.; Hu, F.B.; Willet, W.C. Trends in Dietary Quality Among Adults in the United States, 1999 Through 2010. JAMA Intern. Med. 2014, 176, 1587–1595. [Google Scholar] [CrossRef] [PubMed]
- Kong, A.; Schiffer, L.; Antonic, M.; Braunschweig, C.; Odoms-Young, A.; Fitzgibbon, M. The relationship between home- and individual-level diet quality among African American and Hispanic/Latino households with young children. Int. J. Behav. Nutr. Phys. Act. 2018, 15, 1–12. [Google Scholar] [CrossRef]
- Andreyeva, T.; Kenney, E.L.; O’Connell, M.; Sun, X.; Henderson, K.E. Predictors of Nutrition Quality in Early Child Education Settings in Connecticut. J. Nutr. Educ. Behav. 2018, 50, 458–467. [Google Scholar] [CrossRef]
- Zaltz, D.A.; Hecht, A.A.; Pate, R.R.; Neelon, B.; O’Neill, J.R.; Benjamin-Neelon, S.E. Participation in the Child and Adult Care Food Program is associated with fewer barriers to serving healthier foods in early care and education. BMC Public Health 2020, 20, 1–9. [Google Scholar] [CrossRef]
- Kenney, E.L.; Poole, M.K.; Cory, H.; Cradock, A.L. Impact of changes to the Child and Adult Care Food Program on children’s dietary intake in family child care homes. Public Health Nutr. 2020, 23, 2016–2023. [Google Scholar] [CrossRef]
- Gurzo, K.; Lee, D.L.; Ritchie, K.; Yoshida, S.; Homel Vitale, E.; Hecht, K.; Ritchie, L.D. Child Care Sites Participating in the Federal Child and Adult Care Food Program Provide More Nutritious Foods and Beverages. J. Nutr. Educ. Behav. 2020, 52, 697–704. [Google Scholar] [CrossRef]
- Butte, N.F.; Fox, M.K.A.Y.; Briefel, R.R.; Siega-riz, A.M.; Dwyer, J.T.; Deming, D.M.; Reidy, K.C. Nutrient Intakes of US Infants, Toddlers, and Preschoolers Meet or Exceed Dietary Reference Intakes. J. Am. Diet. Assoc. 2010, 110, S27–S37. [Google Scholar] [CrossRef]
- Ball, S.; Benjamin, S.; Ward, D. Dietary intakes in North Carolina child-care centers: Are children meeting current recommendations? J. Amdiet Assoc. 2008, 108, 718–721. [Google Scholar] [CrossRef] [PubMed]
- Frampton, A.M.; Sisson, S.B.; Horm, D.; Campbell, J.E.; Lora, K.; Ladner, J.L. What’s for Lunch? An Analysis of Lunch Menus in 83 Urban and Rural Oklahoma Child-Care Centers Providing All-Day Care to Preschool Children. J. Acad. Nutr. Diet. 2014, 114, 1367–1374. [Google Scholar] [CrossRef] [PubMed]
- Rasbold, A.H.; Adamiec, R.; Anderson, M.P.; Campbell, J.E.; Horm, D.M.; Sitton, L.K.; Sisson, S.B. Macronutrient and micronutrient intakes of children in Oklahoma child-care centres, USA. Public Health Nutr. 2015, 19, 1498–1505. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Romo-Palafox, M.J.; Ranjit, N.; Sweitzer, S.J.; Roberts-gray, C.; Hoelscher, D.M.; Byrd-williams, C.E.; Briley, M.E. Dietary quality of preschoolers’ sack lunches as measured by the Healthy Eating Index. J. Acad. Nutr. Diet. 2015, 115, 1779–1788. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nayak, K.; Hunter, K.; Owens, J.; Harrington, J. Nutritional Assessment of Snacks and Beverages in Southeastern Virginia Daycare Centers. Clin. Pediatr. 2018, 57, 410–416. [Google Scholar] [CrossRef] [PubMed]
- Copeland, K.A.; Benjamin Neelon, S.E.; Howald, A.E.; Wosje, K.S. Nutritional Quality of Meals Compared to Snacks in Child Care. Child. Obes. 2013, 9, 223–232. [Google Scholar] [CrossRef] [Green Version]
- Hasnin, S.; Dev, D.A.; Tovar, A. Participation in the CACFP Ensures Availability but not Intake of Nutritious Foods at Lunch in Preschool Children in Child-Care Centers. J. Acad. Nutr. Diet. 2020, in press, 6–8. [Google Scholar]
- Trost, S.G.; Messner, L.; Fitzgerald, K.; Roths, B. Nutrition and Physical Activity Policies and Practices in Family Child Care Homes. Am. J. Prev. Med. 2009, 37, 537–540. [Google Scholar] [CrossRef]
- Tovar, A.; Benjamin-neelon, S.E.; Vaughn, A.E.; Tsai, M.; Burney, R.; Østbye, T.; Ward, D.S. Nutritional Quality of Meals and Snacks Served and Consumed in Family Child Care. J. Acad. Nutr. Diet. 2018, 118, 2280–2286. [Google Scholar] [CrossRef] [Green Version]
- Monsivais, P.; Johnson, D.B. Improving nutrition in home child care: Are food costs a barrier? Public Health Nutr. 2012, 15, 370–376. [Google Scholar] [CrossRef] [Green Version]
- Cuadrado-Soto, E.; Risica, P.M.; Gans, K.M.; Mena, N.Z.; Ellis, C.; Araujo, C.D.; Lofgren, I.E.; Stowers, K.C.; Tovar, A. Micronutrient Adequacy in Preschool Children Attending Family Child Care Homes. Nutrients 2019, 11, 2134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Risica, P.; Tovar, A.; Palomo, V.; Dionne, L.; Mena, N.; Magid, K.; Ward, D.S.; Gans, K. Improving Nutrition and Physical Activity Environments of Family Child Care Homes: The rationale, design and study protocol of the ‘Healthy Start/Comienzos Sanos’ cluster randomized trial. BMC Public Health 2019, 19, 419. [Google Scholar] [CrossRef] [PubMed]
- Ball, S.C.; Benjamin, S.E.; Ward, D.S. Development and Reliability of an Observation Method to Assess Food Intake of Young Children in Child Care. J. Am. Diet. Assoc. 2007, 107, 656–661. [Google Scholar] [CrossRef] [PubMed]
- University of Minnesota. NDSR Nutrition Data System for Research 2018 User Manual; Doung, H., Ed.; University of Minnesota: Minneapolis, MI, USA, 2018. [Google Scholar]
- US Department of Agriculture and US Department of Health and Human Services. Dietary Guidelines for Americans 2015–2020, 8th ed.; Government Printing Office: Washington, DC, USA, 2015. [Google Scholar]
- National Center for Health Statistics NHANES Dietary Web Tutorial: Estimate Ratios and Identify Important Food Group Sources of Nutrients. Available online: http://www.cdc.gov/nchs/tutorials/dietary/Basic/Ratios/intro.htm (accessed on 15 July 2019).
- Story, M.; Kaphingst, K.; French, S. The role of child care settings in obesity prevention. Futur. Child. 2006, 16, 143–168. [Google Scholar] [CrossRef]
- Tandon, P.S.; Garrison, M.M.; Christakis, D.A. Physical Activity and Beverages in Home- and Center-based Child Care Programs. J. Nutr. Educ. Behav. 2012, 44, 355–359. [Google Scholar] [CrossRef]
- Fox, M.K.; Condon, E.; Briefel, R.R.; Reidy, K.C.; Deming, D.M. Food Consumption Patterns of Young Preschoolers: Are They Starting Off on the Right Path? J. Am. Diet. Assoc. 2008, 110, S52–S59. [Google Scholar] [CrossRef]
- Office of Superintendent of Public Instruction Child and Adult Care Food Program Meal Patterns. Available online: http://www.k12.wa.us/ChildNutrition/Programs/CACFP/pubdocs/CACFPchildmealpattern.pdf (accessed on 12 January 2020).
- Maalouf, J.; Evers, S.C.; Griffin, M.; Lyn, R. Assessment of Mealtime Environments and Nutrition Practices in Child Care Centers in Georgia. Child. Obes. 2013, 9, 437–445. [Google Scholar] [CrossRef]
- Lindsay, A.C.; Greaney, M.L.; Wallington, S.F.; Sands, F.D.; Wright, J.A.; Salkeld, J. Latino parents’ perceptions of the eating and physical activity experiences of their pre-school children at home and at family child-care homes: A qualitative study. Public Health Nutr. 2016, 20, 346–356. [Google Scholar] [CrossRef] [Green Version]
- Cole, N.; Fox, M.K. Diet Quality of American School-Age Children by School Lunch Participation Status: Data from the National Health and Nutrition Examination Survey, 1999-2004. Nutrition Assistance Program Report Series No.CN-08-NH; United States Department of Agriculture, Food and Nutrition Service, Office of Research, Nutrition and Analysis: Alexandria, VA, USA,, 2008. [Google Scholar]
- Keast, D.R.; Fulgoni, V.L.; Nicklas, T.A.; O’Neil, C.E. Food sources of energy and nutrients among children in the United States: National Health and Nutrition Examination Survey 2003–2006. Nutrients 2013, 5, 283–301. [Google Scholar] [CrossRef] [Green Version]
- Ford, C.; Slining, M.; Popkin, B. Trends in Dietary Intake among US 2- to 6-Year-Old Children, 1989–2008. J. Acad Nutr Diet. 2013, 113, 25–42. [Google Scholar] [CrossRef] [Green Version]
- Ford, C.; Ng, S.; Popkin, B. Ten-year beverage intake trends among US preschool children: Rapid declines between 2003 and 2010 but stagnancy in recent years. Pediatr Obes. 2016, 11, 47–53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Costa, S.; Adams, J.; Gonzalez-Nahm, S.; Neelon, S.E.B. Childcare in Infancy and Later Obesity: A Narrative Review of Longitudinal Studies. N. Engl. J. Med. 2017, 379, 118–131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krebs-Smith, S.M.; Guenther, P.M.; Subar, A.F.; Kirkpatrick, S.I.; Dodd, K.W. Americans Do Not Meet Federal Recommendations. J. Nutr. 2010, 140, 1832–1838. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Pan, L.; Sherry, B.; Li, R. The Association of Sugar-Sweetened Beverage Intake during Infancy with Sugar-Sweetened Beverage Intake at 6 Years of Age. Pediatrics 2014, 134, S56–S62. [Google Scholar] [CrossRef] [Green Version]
- Kirkpatrick, S.I.; Dodd, K.W.; Reedy, J.; Krebs-Smith, S. Income and race/ethnicity are associated with adherence to food-based dietary guidance amoing US adults and children. J. Acad Nutr Diet. 2012, 112, 624–635. [Google Scholar] [CrossRef] [Green Version]
- O’Neil, C.E.; Nicklas, T.A.; Keast, D.R.; Fulgoni, V.L. Ethnic disparities among food sources of energy and nutrients of public health concern and nutrients to limit in adults in the United States: NHANES 2003–2006. Food Nutr. Res. 2014, 58, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Batres-Marquez, S.P.; Jensen, H.H.; Upton, J. Rice Consumption in the United States: Recent Evidence from Food Consumption Surveys. J. Am. Diet. Assoc. 2009, 109, 1719–1727. [Google Scholar] [CrossRef]
- De Hoog, M.L.; Kleinman, K.P.; Gillman, M.W.; Vrijkotte, T.G.; van Eijsden, M.; Taveras, E.M. Racial/ethnic and immigrant differences in early childhood diet quality. Public Health Nutr. 2014, 17, 1308–1317. [Google Scholar] [CrossRef]
- Luna, R.; Polk, S.; Thompson, D. Understanding the use of whole milk and flavored powders in children of low-income, immigrant Latina mothers: A descriptive study. Clin. Pediatr 2017, 56, 480–484. [Google Scholar] [CrossRef] [Green Version]
- Wechsler, H.; Wernick, S.M. A social marketing campaign to promote low-fat milk consumption in an inner-city Latino community. Public Health Rep. 1992, 107, 202–207. [Google Scholar]
- Rehm, C.D.; Drewnowski, A.; Monsivais, P. Potential population-level nutritional impact of replacing whole and reduced-fat milk with low-fat and skim milk among us children aged 2–19 Years. J. Nutr. Educ. Behav. 2015, 47, 61–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siega-Riz, A.M.; Pace, N.D.; Butera, N.M.; Van Horn, L.; Daviglus, M.L.; Harnack, L.; Mossavar-rahmani, Y.; Rock, C.L.; Pereira, R.I.; Sotres-alvarez, D. How Well Do US Hispanics Adhere to the Dietary Guidelines for Americans? Results from the Hispanic Community Health Study/Study of Latinos. Health Equity 2019, 3, 319–327. [Google Scholar] [CrossRef] [PubMed]
- Livingstone, M.; Robson, P.; Wallace, J. Issues in dietary intake assessment of children and adolescents. Br. J. Nutr. 2004, 92, S213–S222. [Google Scholar] [CrossRef] [PubMed]
- Erinosho, T.; Hales, D.; Vaughn, A.; Gizlice, Z.; Ward, D. The Quality of Nutrition and Physical Activity Environments of Family Child-Care Homes in a State in the Southern United States. J. Acad. Nutr. Diet. 2019, 119, 1–8. [Google Scholar] [CrossRef]
- Natale, R.; Scott, S.; Messiah, S.; Schrack, M.; Uhlhorn, S.; Delamater, A.; Natale, R.; Scott, S.H.; Messiah, S.E.; Schrack, M.M.; et al. Design and methods for evaluat- ing an early childhood obesity prevention program in the childcare center setting. Bmc Public Health 2013, 13, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Welker, E.B.; Jacquier, E.F.; Catellier, D.J.; Anater, A.S.; Story, M.T. Room for improvement remains in food consumption patterns of young children Aged 2–4 years. J. Nutr. 2018, 148, 1536S–1546S. [Google Scholar] [CrossRef]


{kind=link}
| Mean (SD) or n (%) | ||
|---|---|---|
| Characteristics | Providers | Children |
| Sex, n (%) | ||
| 120 (100%) | 180 (48.7%) |
| 48.9 (9.0) | 3.43 (0.9) |
| ||
| 81 (67.5%) | 208 (57.6%) |
| 39 (32.5%) | 153 (42.4%) |
| Marital status, n (%) | ||
| 11 (9.2%) | |
| 90 (75.0%) | |
| 10 (8.3%) | |
| 9 (7.5%) | |
| Education level, n (%) | ||
| 13 (10.9%) | |
| 39 (32.5%) | |
| 68 (56.6%) | |
| Annual Household Income, n (%) | ||
| 16 (13.8%) | |
| 57 (49.2%) | |
| 24 (20.7%) | |
| 19 (16.3%) | |
| 62.4 (±13.8) | |
| 7.7 (±3.1) | |
| CACFP Participation, n (%) | ||
| 99 (82.5%) | |
| Program participation, n (%) | ||
| 4 (3.3%) | |
| 4 (3.3%) | |
| 1 (0.9%) | |
| 111 (92.5%) | |
| Hours spent in childcare, mean (SD) | 7.6 (0.9) | |
| Days per week in the FCCH, mean (SD) | 4.8 (0.8) | |
| Overall (n = 120) | Latino Providers (n = 81) | Non-Latino Providers (n = 39) | ||||||
|---|---|---|---|---|---|---|---|---|
| Food Group/ Food Items | Mean Serving (SD) | % | Mean Serving (SD) | % | Mean Serving (SD) | % | p Value for Means b | p Value for % b |
| FRUITS | 0.37 (0.23) | 0.40 (0.30) | 0.35 (0.23) | 0.31 | ||||
| Whole fruit | 0.29 (0.20) | 15 | 0.10 (0.19) | 18 | 0.04 (0.08) | 10 | 0.26 | 0.05 |
| Fruit juice | 0.08 (0.16) | 85 | 0.28 (0.20) | 82 | 0.31 (0.23) | 90 | 0.45 | <0.001 * |
| VEGETABLES | 0.17 (0.14) | 0.18 (0.14) | 0.14 (0.14) | 0.17 | ||||
| Non-starchy c | 0.09 (0.10) | 61 | 0.08 (0.10) | 52 | 0.11 (0.11) | 82 | 0.01 | <0.001 * |
| 0.04 (0.06) | 24 | 0.04 (0.05) | 23 | 0.05 (0.08) | 29 | 0.02 | <0.001 * |
| 0.01 (0.03) | 7 | 0.01 (0.04) | 7 | 0.01 (0.02) | 7 | 0.19 | 0.85 |
| 0.04 (0.06) | 29 | 0.03 (0.05) | 23 | 0.05 (0.06) | 45 | 0.02 | <0.001 * |
| Starchy e | 0.03 (0.07) | 15 | 0.04 (0.07) | 15 | 0.03 (0.06) | 13 | 0.31 | 0.16 |
| Legumes | 0.04 (0.06) | 24 | 0.06 (0.07) | 33 | 0.00 (0.00) | 5 | <0.001 * | <0.001 * |
| DAIRY/ ALTERNATIVE | 0.35 (0.18) | 0.33 (0.16) | 0.38 (0.21) | 0.01 | 0.01 | |||
| Dairy products | ||||||||
| Milk | 0.25 (0.04) | 71 | 0.24 (0.13) | 72 | 0.27 (0.21) | 69 | 0.07 | 0.13 |
| Cheese | 0.05 (0.03) | 14 | 0.05 (0.08) | 13 | 0.07 (0.12) | 16 | 0.52 | 0.36 |
| Yogurt | 0.04 (0.03) | 11 | 0.04 (0.04) | 12 | 0.02 (0.03) | 9 | 0.72 | 0.65 |
| Non-dairy | 0.00 (0.01) | 1 | 0.00 (0.02) | 1 | 0.01 (0.03) | 2 | 0.68 | 0.12 |
| Desserts f | 0.01 (0.01) | 2 | 0.00 (0.01) | 1 | 0.01 (0.03) | 4 | 0.82 | 0.62 |
| According to fat content g | ||||||||
| Low-fat | 0.25 (0.17) | 71 | 0.23 (0.15) | 68 | 0.29 (0.21) | 77 | 0.11 | <0.001 * |
| Reduced | 0.03 (0.07) | 10 | 0.03 (0.06) | 11 | 0.04 (0.08) | 8 | 0.06 | 0.13 |
| Whole fat | 0.06 (0.08) | 19 | 0.06 (0.09) | 21 | 0.05 (0.06) | 15 | 0.05 | 0.16 |
| According to added sugar h | ||||||||
| Sweetened | 0.04 (0.05) | 15 | 0.04 (0.04) | 14 | 0.03 (0.05) | 17 | 0.48 | 0.64 |
| Unsweetened | 0.25 (0.16) | 85 | 0.24 (0.13) | 86 | 0.27 (0.22) | 83 | 0.24 | 0.53 |
| PROTEIN | 0.31 (0.25) | 0.31 (0.24) | 0.31 (0.26) | 0.18 | ||||
| Poultry | 0.14 (0.14) | 44 | 0.16 (0.20) | 48 | 0.12 (0.16) | 34 | 0.50 | <0.001 * |
| Beef | 0.05 (0.11) | 14 | 0.05 (0.10) | 15 | 0.06 (0.14) | 12 | 0.76 | 0.84 |
| Eggs | 0.03 (0.06) | 10 | 0.03 (0.06) | 10 | 0.03 (0.05) | 9 | 0.34 | 0.79 |
| Cold cuts | 0.04 (0.10) | 12 | 0.03 (0.09) | 10 | 0.05 (0.13) | 16 | 0.02 | 0.22 |
| Fish | 0.01 (0.05) | 5 | 0.02 (0.06) | 6 | 0.01 (0.04) | 4 | 0.60 | 0.87 |
| Pork | 0.01 (0.06) | 5 | 0.01 (0.05) | 5 | 0.02 (0.08) | 4 | 0.31 | 0.35 |
| Nuts and seeds | 0.02 (0.06) | 10 | 0.02 (0.05) | 5 | 0.04 (0.08) | 21 | 0.17 | <0.001 * |
| GRAINS | 0.63 (0.29) | 0.60 (0.27) | 0.70 (0.32) | <0.001 * | ||||
| Grain product | ||||||||
| Grain, flour, dry mixes i | 0.18 (0.07) | 28 | 0.24 (0.18) | 34 | 0.14 (0.29) | 13 | 0.02 | <0.001 * |
| Crackers | 0.11 (0.05) | 17 | 0.05 (0.07) | 15 | 0.08 (0.11) | 20 | 0.17 | 0.47 |
| Ready-to-eat cereals | 0.07 (0.04) | 11 | 0.05 (0.06) | 13 | 0.02 (0.04) | 7 | 0.18 | 0.17 |
| Bread | 0.09 (0.04) | 15 | 0.08 (0.10) | 12 | 0.17 (0.15) | 20 | 0.34 | 0.01 |
| Other breads j | 0.08 (0.04) | 12 | 0.09 (0.14) | 9 | 0.17 (0.21) | 16 | 0.60 | 0.05 |
| Cakes/cookies k | 0.04 (0.03) | 7 | 0.03 (0.07) | 7 | 0.03 (0.07) | 6 | 0.52 | 0.70 |
| Pasta | 0.04 (0.03) | 7 | 0.05 (0.10) | 6 | 0.06 (0.08) | 8 | 0.71 | 0.61 |
| Snacks l | 0.03 (0.03) | 4 | 0.01 (0.03) | 2 | 0.03 (0.05) | 8 | 0.30 | <0.001 * |
| Type of grain | ||||||||
| Whole grain | 0.14 (0.16) | 25 | 0.13 (0.15) | 26 | 0.15 (0.18) | 24 | 0.09 | 0.55 |
| Refined grain | 0.49 (0.29) | 75 | 0.47 (0.28) | 74 | 0.55 (0.30) | 76 | 0.08 | 0.55 |
| FATS | 0.19 (0.17) | 0.19 (0.15) | 0.18 (0.21) | 0.27 | ||||
| Oils | 0.05 (0.07) | 59 | 0.12 (0.11) | 73 | 0.05 (0.11) | 27 | <0.001 * | <0.001 * |
| Butter/other animal fats | 0.03 (0.04) | 16 | 0.03 (0.09) | 11 | 0.04 (0.01) | 26 | 0.50 | <0.001 * |
| Salad dressings | 0.01 (0.03) | 7 | 0.00 (0.01) | 6 | 0.01 (0.02) | 12 | 0.16 | <0.001 * |
| Margarine | 0.02 (0.03) | 8 | 0.02 (0.08) | 4 | 0.05 (0.14) | 18 | 0.10 | <0.001 * |
| Shortening | 0.01 (0.03) | 5 | 0.01 (0.05) | 5 | 0.01 (0.08) | 6 | 0.17 | 0.15 |
| Cream | 0.01 (0.03) | 5 | 0.00 (0.02) | 1 | 0.01 (0.03) | 11 | 0.39 | <0.001 * |
| Vegetable vs. animal origin | ||||||||
| Vegetable | 0.15 (0.15) | 81 | 0.16 (0.13) | 89 | 0.12 (0.19) | 63 | <0.001 * | <0.001 * |
| Animal | 0.04 (0.08) | 19 | 0.03 (0.09) | 11 | 0.05 (0.06) | 37 | 0.11 | <0.001 * |
| SWEETS | 0.07 (0.18) | 0.07 (0.20) | 0.06 (0.14) | 0.07 | ||||
| Syrup, honey, jelly | 0.03 (0.03) | 50 | 0.01 (0.03) | 54 | 0.01 (0.02) | 44 | 0.57 | 0.66 |
| Sugar m | 0.02 (0.09) | 32 | 0.02 (0.10) | 30 | 0.02 (0.07) | 37 | 0.09 | 0.09 |
| SSBs | 0.01 (0.03) | 12 | 0.01 (0.03) | 15 | 0.01 (0.03) | 8 | 0.55 | 0.45 |
| Chocolate/candy | 0.00 (0.01) | 5 | 0.00 (0.00) | 2 | 0.00 (0.01) | 6 | 0.10 | 0.03 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ramirez, A.; Vadiveloo, M.; Risica, P.M.; Gans, K.M.; Greaney, M.L.; Mena, N.Z.; Cooksey Stowers, K.; Tovar, A. Dietary Contributors to Food Group Intake in Preschool Children Attending Family Childcare Homes: Differences between Latino and Non-Latino Providers. Nutrients 2020, 12, 3686. https://doi.org/10.3390/nu12123686
Ramirez A, Vadiveloo M, Risica PM, Gans KM, Greaney ML, Mena NZ, Cooksey Stowers K, Tovar A. Dietary Contributors to Food Group Intake in Preschool Children Attending Family Childcare Homes: Differences between Latino and Non-Latino Providers. Nutrients. 2020; 12(12):3686. https://doi.org/10.3390/nu12123686
Chicago/Turabian StyleRamirez, Andrea, Maya Vadiveloo, Patricia M. Risica, Kim M. Gans, Mary L. Greaney, Noereem Z. Mena, Kristen Cooksey Stowers, and Alison Tovar. 2020. "Dietary Contributors to Food Group Intake in Preschool Children Attending Family Childcare Homes: Differences between Latino and Non-Latino Providers" Nutrients 12, no. 12: 3686. https://doi.org/10.3390/nu12123686