Effect of a Mediterranean Diet-Based Nutritional Intervention on the Risk of Developing Gestational Diabetes Mellitus and Other Maternal-Fetal Adverse Events in Hispanic Women Residents in Spain

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
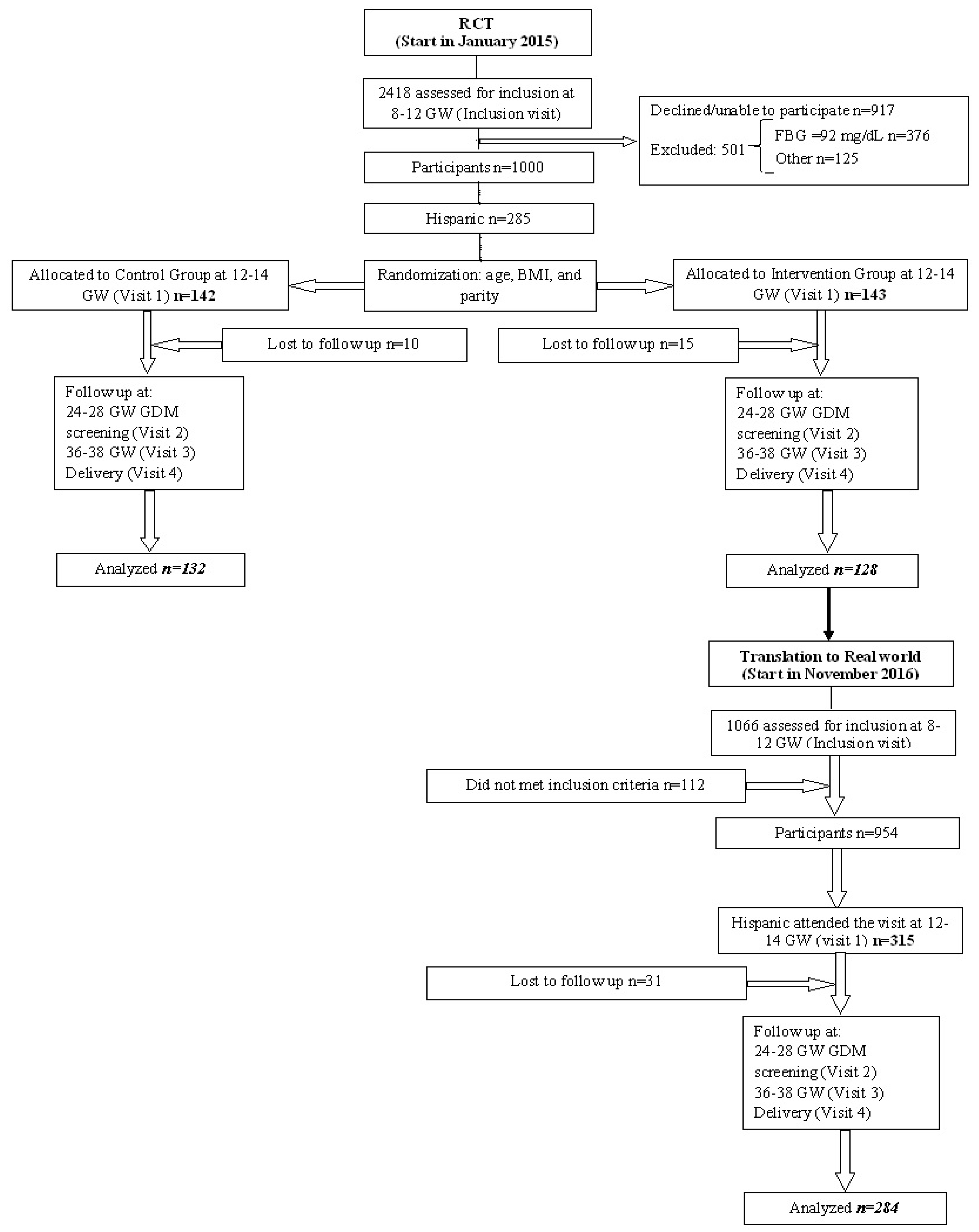
2.1. Study Design
2.2. Participants
2.3. Pregnancy Follow-Up
2.3.1. Clinical and Anthropometric Data
2.3.2. Biochemical Analysis
2.3.3. Dietary and Lifestyle Assessment
2.3.4. Maternal, Delivery and Neonatal Outcomes
2.4. Sample Size
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Data Availability
References
- Capobianco, G.; Gulotta, A.; Tupponi, G.; Dessole, F.; Pola, M.; Virdis, G.; Petrillo, M.; Mais, V.; Olzai, G.; Antonucci, R.; et al. Materno-Fetal and Neonatal Complications of Diabetes in Pregnancy: A Retrospective Study. J. Clin. Med. 2020, 9, 2707. [Google Scholar] [CrossRef]
- Domanski, G.; Lange, A.E.; Ittermann, T.; Allenberg, H.; Spoo, R.A.; Zygmunt, M.; Heckmann, M. Evaluation of neonatal and maternal morbidity in mothers with gestational diabetes: A population-based study. BMC Pregnancy Childbirth 2018, 18, 367. [Google Scholar] [CrossRef] [PubMed]
- Xiong, X.; Saunders, L.D.; Wang, F.L.; Demianczuk, N.N. Gestational diabetes mellitus: Prevalence, risk factors, maternal and infant outcomes. Int. J. Gynecol. Obstet. 2001, 75, 221–228. [Google Scholar] [CrossRef]
- Johns, E.C.; Denison, F.C.; Norman, J.E.; Reynolds, R.M. Gestational Diabetes Mellitus: Mechanisms, Treatment, and Complications. Trends Endocrinol. Metab. 2018, 29, 743–754. [Google Scholar] [CrossRef] [PubMed]
- Zhang, R.; Han, S.; Chen, G.C.; Li, Z.N.; Silva-Zolezzi, I.; Parés, G.V.; Wang, Y.; Qin, L.Q. Effects of low-glycemic-index diets in pregnancy on maternal and newborn outcomes in pregnant women: A meta-analysis of randomized controlled trials. Eur. J. Nutr. 2018, 57, 167–177. [Google Scholar] [CrossRef] [PubMed]
- Rogozińska, E.; Chamillard, M.; Hitman, G.; Khan, K.; Thangaratinam, S. Nutritional Manipulation for the Primary Prevention of Gestational Diabetes Mellitus: A Meta-Analysis of Randomised Studies. PLoS ONE 2015, 10, e0115526. [Google Scholar] [CrossRef] [Green Version]
- Shepherd, E.; Gomersall, J.C.; Tieu, J.; Han, S.; Crowther, C.A.; Middleton, P. Combined diet and exercise interventions for preventing gestational diabetes mellitus. Cochrane Database Syst. Rev. 2017, 13, CD010443. [Google Scholar] [CrossRef] [PubMed]
- Song, C.; Li, J.; Leng, J.; Ma, R.; Yang, X. Lifestyle intervention can reduce the risk of gestational diabetes: A meta-analysis of randomized controlled trials. Obes. Rev. 2016, 17, 960–969. [Google Scholar] [CrossRef]
- Koivusalo, S.; RoÈnoÈ, K.; Klemetti, M.; Roine, R.P.; LindstroÈm, J.; Erkkola, M.; Kaaja, R.J.; Pöyhönen-Alho, M.; Tiitinen, A.; Huvinen, E.; et al. Gestational Diabetes Mellitus Can Be Prevented by Lifestyle Intervention: The Finnish Gestational Diabetes Prevention Study (RADIEL). Diabetes Care 2016, 39, 24–30. [Google Scholar] [CrossRef] [Green Version]
- Assaf-Balut, C.; García De La Torre, N.; Durán, A.; Fuentes, M.; Bordiú, E.; Del Valle, L.; Familiar, C.; Ortolá, A.; Jiménez, I.; Herraiz, M.A.; et al. A Mediterranean diet with additional extra virgin olive oil and pistachios reduces the incidence of gestational diabetes mellitus (GDM): A randomized controlled trial: The St. Carlos GDM prevention study. PLoS ONE 2017, 12, e0185873. [Google Scholar] [CrossRef]
- Al Wattar, B.H.; Dodds, J.; Placzek, A.; Beresford, L.; Spyreli, E.; Moore, A.; Gonzalez Carreras, F.J.; Austin, F.; Murugesu, N.; Roseboom, T.J.; et al. Mediterranean-style diet in pregnant women with metabolic risk factors (ESTEEM): A pragmatic multicentre randomised trial. PLoS Med. 2019, 16, e1002857. [Google Scholar] [CrossRef] [PubMed]
- Dodd, J.M.; Turnbull, D.; McPhee, A.J.; Deussen, A.R.; Grivell, R.M.; Yelland, L.N.; Owens, J.A.; Robinson, J.S.; for the LIMIT Randomised Trial Group. Antenatal lifestyle advice for women who are overweight or obese: LIMIT randomised trial. BMJ. 2014, 348, g1285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poston, L.; Bell, R.; Croker, H.; Flynn, A.C.; Godfrey, K.M.; Goff, L.; Hayes, L.; Khazaezadeh, N.; Nelson, S.M.; Oteng-Ntimet, E.; et al. Effect of a behavioural intervention in obese pregnant women (the UPBEAT study): A multicentre, randomised controlled trial. Lancet Diabetes Endocrinol. 2015, 3, 767–777. [Google Scholar] [CrossRef]
- Amati, F.; Swaka, A.; Hassounah, S. The impact of Mediterranean Dietary patterns during pregnancy on maternal and offspring health. Nutrients 2019, 11, 1098. [Google Scholar] [CrossRef] [Green Version]
- Assaf-Balut, C.; García de la Torre, N.; del Valle, L.; Valerio, J.; Durán, A.; Bordiú, E.; Barabash, A.; Rubio, M.A.; Calle-Pascual, A.L. Gestational diabetes mellitus and Mediterranean diet principles. In The Mediterranean Diet: An Evidence-Based Approach, 2nd ed.; Victor, R.P., Watson, R.R., Eds.; Academic Press: London, UK; Oxford, UK; San Diego, CA, USA; Cambrigde, UK; Elsevier Inc.: London, UK, 2020; pp. 314–323. [Google Scholar]
- Garcia de la Torre, N.; Assaf-Balut, C.; Jimenez Varas, I.; Del Valle, L.; Durán, A.; Fuentes, M.; Del Prado, N.; Bordiú, E.; Valerio, J.J.; Herraiz, M.A.; et al. Effectiveness of following mediterranean diet recommendations in the real world in the incidence of gestational diabetes mellitus (GDM) and adverse maternal-foetal outcomes: A prospective, universal, interventional study with a single group. the St Carlos study. Nutrients 2019, 11, 1210. [Google Scholar] [CrossRef] [Green Version]
- INEbase /Demografía y Población/Padrón.Población por Municipios/Padrón Continuo. Available online: https://www.ine.es/dyngs/INEbase/es/operacion.htm?c=Estadistica_C&cid=1254736177012&menu=ultiDatos&idp=1254734710990 (accessed on 27 September 2020).
- Bardenheier, B.H.; Imperatore, G.; Gilboa, S.M.; Geiss, L.S.; Saydah, S.H.; Devlin, H.M.; Kim, S.Y.; Gregg, E.W. Trends in Gestational Diabetes among Hospital Deliveries in 19 U.S. States, 2000-2010. Am. J. Prev. Med. 2015, 49, 12–19. [Google Scholar] [CrossRef] [Green Version]
- Xiang, A.H.; Black, M.H.; Li, B.H.; Martinez, M.P.; Sacks, D.A.; Lawrence, J.M.; Buchanan, T.A.; Jacobsen, S.J. Racial and ethnic disparities in extremes of fetal growth after gestational diabetes mellitus. Diabetologia 2015, 58, 272–281. [Google Scholar] [CrossRef]
- Homko, C.J.; Sivan, E.; Nyirjesy, P.; Reece, E.A. The interrelationship between ethnicity and gestational diabetes in fetal macrosomia. Diabetes Care 1995, 18, 1442–1445. [Google Scholar] [CrossRef]
- Danso, K. Nativity and health disparities: Predictors of immigrant health. Soc. Work Public Health 2016, 31, 175–187. [Google Scholar] [CrossRef]
- Blumberg, J.; Ballares, V.; Durbin, J.L. Ethnic variations on gestational diabetes mellitus and evidence-based first- line interventions. J. Matern. Neonatal Med. 2018, 31, 2641–2647. [Google Scholar] [CrossRef]
- Pu, J.; Zhao, B.; Wang, E.J.; Nimbal, V.; Osmundson, S.; Kunz, L.; Popat, R.A.; Chung, S.; Palaniappan, L.P. Racial/Ethnic Differences in Gestational Diabetes Prevalence and Contribution of Common Risk Factors. Paediatr. Perinat. Epidemiol. 2015, 29, 436–443. [Google Scholar] [CrossRef] [PubMed]
- Moore Simas, T.A.; Waring, M.E.; Callaghan, K.; Leung, K.; Ward Harvey, M.; Buabbud, A.; Chasan-Taber, L. Weight gain in early pregnancy and risk of gestational diabetes mellitus among Latinas. Diabetes Metab. 2019, 45, 26–31. [Google Scholar] [CrossRef] [PubMed]
- Perera, M.J.; Reina, S.A.; Elfassy, T.; Potter, J.N.E.; Sotres Alvarez, D.; Simon, M.A.; Isasi, C.R.; Stuebe, A.M.; Schneiderman, N.; Llabre, M.M. Gestational diabetes and cardiovascular risk factors and disease in U.S. Hispanics/Latinas in the Hispanic Community Health Study/Study of Latinos (HCHS/SOL). Women Health 2019, 59, 481–495. [Google Scholar] [CrossRef]
- Pérez-Ferre, N.; Fernández, M.D.; Torrejón, M.J.; Del Prado, N.; Runkle, I.; Rubio, M.A.; Montañez, C.; Bordiu, E.; Calle-Pascual, A. Effect of lifestyle on the risk of gestational diabetes and obstetric outcomes in immigrant Hispanic women living in Spain. J. Diabetes 2012, 4, 432–438. [Google Scholar] [CrossRef] [PubMed]
- International Association of Diabetes and Pregnancy Study Groups Consensus Panel. International Association of Diabetes and Pregnancy Study Groups recommendations on the diagnosis and classification of hyperglycemia in pregnancy. Diabetes Care 2010, 33, 676–682. [Google Scholar] [CrossRef] [Green Version]
- Assaf-Balut, C.; Garcia de la Torre, N.; Duran, A.; Fuentes, M.; Bordiú, E.; del Valle, L.; Valerio, J.J.; Familiar, C.; Jiménez, I.; Herraiz, M.A.; et al. Medical nutrition therapy for gestational diabetes mellitus based on Mediterranean Diet principles: A subanalysis of the St Carlos GDM Prevention Study. BMJ Open Diab Res Care 2018, 6, e000550. [Google Scholar] [CrossRef] [Green Version]
- Carolan-Olah, M.; Duarte-Gardea, M.; Lechuga, J. A systematic review of interventions for Hispanic women with or at risk of Gestational diabetes mellitus (GDM). Sex. Reprod. Healthc. 2017, 13, 14–22. [Google Scholar] [CrossRef]
- Guo, X.Y.; Shu, J.; Fu, X.H.; Chen, X.P.; Zhang, L.; Ji, M.X.; Liu, X.M.; Yu, T.T.; Sheng, J.Z.; Huang, H.F. Improving the effectiveness of lifestyle interventions for gestational diabetes prevention: A meta-analysis and meta-regression. BJOG 2019, 126, 311–320. [Google Scholar] [CrossRef] [Green Version]
- Wang, Z.; Kanguru, L.; Hussein, J.; Fitzmaurice, A.; Ritchie, K. Incidence of adverse outcomes associated with gestational diabetes mellitus in low- and middle-income countries. Int. J. Gynecol. Obstet. 2013, 121, 14–19. [Google Scholar] [CrossRef]
- Ménard, V.; Sotunde, O.F.; Weiler, H.A. Ethnicity and Immigration Status as Risk Factors for Gestational Diabetes Mellitus, Anemia and Pregnancy Outcomes Among Food Insecure Women Attending the Montreal Diet Dispensary Program. Can. J. Diabetes 2020, 44, 139–145.e1. [Google Scholar] [CrossRef]
- de Castro, M.B.T.; de Souza, R.A.G.; Vilela, A.A.F.; Kac, G. Association between sociodemographics factors and dietary patterns during pregnancy. Rev. Nutr. 2014, 27, 173–181. [Google Scholar] [CrossRef] [Green Version]
- Northstone, K.; Emmett, P.; Rogers, I. Dietary patterns in pregnancy and associations with socio-demographic and lifestyle factors. Eur. J. Clin. Nutr. 2008, 62, 471–479. [Google Scholar] [CrossRef] [PubMed]
- Singh, H.; Soyoltulga, K.; Fong, T.; Billimek, J. Delivery Outcomes, Emergency Room Visits, and Psychological Aspects of Gestational Diabetes: Results from a Community Hospital Multiethnic Cohort. Diabetes Educ. 2018, 44, 465–474. [Google Scholar] [CrossRef] [PubMed]
- Betrn, A.P.; Gulmezoglu, A.M.; Robson, M.; Merialdi, M.; Souza, J.P.; Wojdyla, D.; Widmer, M.; Carroli, G.; Torloni, M.R.; Langer, A.; et al. WHO global survey on maternal and perinatal health in Latin America: Classifying caesarean sections. Reprod. Health 2009, 6, 18. [Google Scholar] [CrossRef] [Green Version]
- Janevic, T.; Loftfield, E.; Savitz, D.A.; Bradley, E.; Illuzzi, J.; Lipkind, H. Disparities in cesarean delivery by ethnicity and nativity in New York City. Matern. Child Health J. 2014, 18, 250–257. [Google Scholar] [CrossRef]


{kind=link}
| RCT | SS | RW Group | SS | ||
|---|---|---|---|---|---|
| CG (n = 142) | IG (n= 143) | P | RW (n = 315) | p | |
| Age (years) | 31.3 ± 5.6 | 31.7 ± 5.4 | 0.573 | 31.4 ± 5.7 | 0.895 |
| Years of Residency in Spain | 10.0 ± 5.0 | 10.2 ± 5.8 | 0.773 | 10.1 ± 5.5 | 0.965 |
| Family history of T2DM | 37 (26.0) | 41 (28.7) | 0.102 | 90 (28.6) | 0.520 |
| MetS (>2 components) | 20 (14.1) | 20 (14.0) | 0.402 | 46 (14.6) | 0.101 |
| Previous history of | 0.449 | 0.127 | |||
| - GDM | 7 (4.9) | 4 (2.8) | 8 (2.5) | ||
| - Miscarriages | 57 (40.1) | 62 (43.4) | 160 (50.8) | ||
| Educational status | 0.067 | 0.127 | |||
| Elementary School Education | 28 (19.7) | 18 (12.6) | 35 (11.2) | ||
| Secondary School Degree | 67 (47.2) | 66 (46.2) | 160 (50.8) | ||
| University Degree | 45 (31.7) | 58 (40.6) | 112 (35.5) | ||
| Unknown | 2 (1.4) | 1 (0.7) | 8 (2.5) | ||
| Unemployed | 98 (69.0) | 97 (67.8) | 0.241 | 231 (73.3) | 0.194 |
| Number of pregnancies | 0.172 | 0.660 | |||
| Primiparous | 36 (25.4) | 42 (29.4) | 97 (20.8) | ||
| Second pregnancy | 45 (31.7) | 49 (34.3) | 94 (29.8) | ||
| >2 pregnancies | 61 (42.9) | 52 (36.3) | 124 (39.4) | ||
| Smoker | 0.111 | 0.847 | |||
| Never | 105 (73.9) | 96 (67.1) | 241 (76.5) | ||
| Current | 1 (0.7) | 1 (0.7) | 5 (1.6) | ||
| Gestational Age (weeks) | 12.1 ± 0.8 | 12.0 ± 0.6 | 0.811 | 12.1 ± 0.6 | 0.791 |
| Body Weight (kg) | |||||
| Pre-pregnancy | 62.5 ± 12.2 | 60.2 ±9.6 | 0.068 | 58.9 ± 9.4 | 0.001 |
| At baseline | 64.3 ± 12.9 | 62.2 ± 9.7 | 0.061 | 60.9 ± 9.9 | 0.001 |
| Weigth gain | 2.3 ± 4.1 | 3.3 ± 1.6 | 0.188 | 2.1 ± 4.9 | 0.743 |
| Pre-pregnancy BMI (kg/m2) | 24.4 ± 4.0 | 24.1 ± 3.4 | 0.259 | 23.4 ± 3.6 | 0.033 |
| Systolic BP(mm Hg) | 105 ± 10 | 106 ± 10 | 0.443 | 108 ± 10 | 0.011 |
| Diastolic BP (mm Hg) | 63 ± 10 | 64 ± 9 | 0.684 | 66 ± 8 | 0.029 |
| Fasting Blood Glucose (mg/dL) | 81.3 ± 7.0 | 80.8 ± 6.0 | 0.604 | 80.2 ± 6.1 | 0.066 |
| TSH mcUI/mL | 2.0 ± 1.3 | 1.9 ± 1.5 | 0.575 | 1.9 ± 1.4 | 0.582 |
| MEDAS Score | 4.6 ± 1.8 | 4.2 ± 1.7 | 0.691 | 4.0 ± 1.6 | 0.323 |
| Nutrition Score | −0.1 ± 3.3 | −0.4 ± 3.1 | 0.510 | −0.5 ± 3.0 | 0.423 |
| Physical Activity Score | −1.6 ± 1.1 | −1.8 ± 1.0 | 0.091 | −1.8 ± 1.0 | 0.057 |
| AT BASELINE | 24–28 GW | 36–38 GW | P TREND | ||
|---|---|---|---|---|---|
| EVOO (mL/day) | CG | 23 ± 22 | 28 ± 26 | 30 ± 22 | 0.020 |
| IG | 29 ± 29 | 32 ± 19 | 40 ± 33 | 0.001 | |
| p IG vs. CG | 0.100 | 0.023 | 0.043 | ||
| RW | 23 ± 21 | 28 ± 27 | 28 ± 23 | 0.012 | |
| p RW vs. CG | 0.873 | 0.123 | 0.143 | ||
| Pistachio/Nuts (days/week) | CG | 0.8 ± 1.6 | 1.0 ± 1.9 | 2.0 ± 2.9 | 0.128 |
| IG | 0.8 ± 1.5 | 2.9 ± 2.7 | 3.0 ± 2.5 | 0.001 | |
| p IG vs. CG | 0.885 | 0.001 | 0.063 | ||
| RW | 1.0 ± 1.8 | 1.9 ± 2.2 | 2.7 ± 2.2 | 0.001 | |
| p RW vs. CG | 0.123 | 0.043 | 0.965 | ||
| Nutrition Score | CG | −0.1 ± 3.3 | 0.2 ± 3.5 | 3.1 ± 4.0 | 0.001 |
| IG | −0.4 ± 3.1 | 3.3 ± 3.0 | 4.0 ± 3.7 | 0.001 | |
| p IG vs. CG | 0.510 | 0.001 | 0.112 | ||
| RW | −0.5 ± 3.0 | 1.3 ± 3.5 | 2.8 ± 4.0 | 0.001 | |
| p RW vs. CG | 0.423 | 0.001 | 0.516 | ||
| MedDiet Score | CG | 4.6 ± 1.8 | 5.7 ± 1.8 | 5.0 ± 2.0 | 0.098 |
| IG | 4.2 ± 1.7 | 7.4 ± 1.4 | 7.5 ± 1.6 | 0.010 | |
| p IG vs. CG | 0.691 | 0.001 | 0.034 | ||
| RW | 4.0 ± 1.6 | 6.3 ± 1.8 | 5.9 ± 22 | 0.001 | |
| p RW vs. CG | 0.323 | 0.001 | 0.043 | ||
| Physical Activity Score | CG | −1.6 ± 1.1 | −1.7 ± 0.9 | −1.8 ± 0.6 | 0.081 |
| IG | −1.8 ± 1.0 | −1.9 ± 0.9 | −1.7 ± 0.8 | 0.601 | |
| p IG vs. CG | 0.091 | 0.168 | 0.299 | ||
| RW | −1.8 ± 1.0 | −1.7 ± 0.9 | −1.5 ± 0.9 | 0. 078 | |
| p RW vs. CG | 0.057 | 0.260 | 0.065 | ||
| RCT | SS vs. CG | SS vs. CG | |||
|---|---|---|---|---|---|
| CG (n = 132) | IG (n = 128) | p | RW (n = 284) | p | |
| MATERNAL OUTCOMES | |||||
| GDM | 34 (25.8) | 19 (14.8) | 0.021 | 38 (13.4) | 0.011 |
| RR (95% CI) | 1 | 0.72 (0.50–0.97) | 0.037 | 0.77 (0.61–0.97) | 0.008 |
| 75 g-OGTT 24–28 GW | |||||
| Fasting Blood Glucose (mg/dL) | 86.3 ± 7.0 | 84.3 ± 6.7 | 0.022 | 84.7 ± 6.2 | 0.018 |
| ≥92 mg/dL | 24 (18.2) | 17 (13.3) | 0.167 | 28 (8.8) | 0.032 |
| RR (95% CI) | 1 | 0.81 (0.55–1.19) | 0.308 | 0.79 (0.61–1.03) | 0.058 |
| 1 h Blood Glucose (mg/dL) | 118.3 ± 34.7 | 116.5 ± 28.4 | 0.705 | 114.5 ± 27.3 | 0.569 |
| ≥180 mg/dL | 6 (4.5) | 2 (1.6) | 0.146 | 4 (1.4) | 0.077 |
| RR (95% CI) | 1 | 0.50 (0.15–1.66) | 0.281 | 0.60 (0.28–1.28) | 0.092 |
| 2 h Blood Glucose (mg/dL) | 107.7 ± 24.3 | 104.5 ± 21.5 | 0.419 | 101.8 ± 21.4 | 0.054 |
| ≥153 mg/dL | 9 (6.8) | 4 (3.1) | 0.130 | 5 (1.8) | 0.016 |
| RR (95% CI) | 1 | 0.60 (0.27–1.38) | 0.253 | 0.53 (0.26–1.00) | 0.019 |
| HbA1c (%) 24–28 GW | 5.1 ± 0.3 | 5.0 ± 0.3 | 0.021 | 5.0 ± 0.3 | 0.001 |
| >5.5% | 12 (9.1) | 5 (3.9) | 0.081 | 6 (2.1) | 0.004 |
| HbA1c (%) 36–38 GW | 5.5 ± 0.3 | 5.3 ± 0.2 | 0.001 | 5.3 ± 0.3 | 0.001 |
| >5.5% | 50 (38.0) | 20 (15.2) | 0.002 | 59 (20.8) | 0.015 |
| RR (95% CI) | 1 | 0.49 (0.33–075) | 0.003 | 0.44 (0.22–0.87) | 0.024 |
| FBG 36–38 GW (mg/dL) | 78.4 ± 9.4 | 74.8 ± 4.4 | 0.006 | 79.5 ± 10.8 | 0.495 |
| Fasting Serum Insulin (mcUI/mL) | |||||
| 24–28 GW | 9.9 ± 5.8 | 9.8 ± 4.5 | 0.787 | 9.7 ± 6.9 | 0.232 |
| 36–38 GW | 12.4 ± 14.8 | 12.1 ± 11.6 | 0.846 | 15.7 ± 20.0 | 0.258 |
| HOMA-IR | |||||
| 24–28 GW | 2.4 ± 1.4 | 2.0 ± 1.0 | 0.045 | 2.4 ± 3.8 | 0.835 |
| 36–38 GW | 2.6 ± 4.3 | 2.2 ± 2.3 | 0.050 | 3.6 ± 5.8 | 0.225 |
| Treatment of GDM | |||||
| Nutritional | 22 (64.7) | 15 (78.9) | 29 (76.3) | ||
| Insulin | 12 (35.3) | 4 (21.1) | 0.039 | 9 (23.7) | 0.001 |
| Basal | 10 (83.3) | 2 (50) | 5 (55.5) | ||
| Basal/Bolus | 2 (16.7) | 2 (50) | 4 (44.5) | ||
| RR (95% CI) for IT | 1 | 0.44 (0.12–1.00) | 0.041 | 0.61 (0.38–0.96) | 0.049 |
| Weight gain (Kg) to 24–28 GW | 7.6 ± 4.8 | 6.7 ± 3.8 | 0.102 | 6.9 ± 4.6 | 0.237 |
| Weight gain (Kg) to 36–38 GW | 11.3 ± 6.3 | 12.3 ± 5.4 | 0.209 | 12.5 ± 6.6 | 0.075 |
| Systolic BP (mm Hg) 24–28 GW | 104 ± 11 | 106 ± 11 | 0.131 | 105 ± 11 | 0.164 |
| Diastolic BP (mm Hg) 24–28 GW | 63 ± 9 | 63 ± 9 | 0.864 | 63 ± 9 | 0.413 |
| Systolic BP (mm Hg) 36–38 GW | 115 ± 16 | 113 ± 13 | 0.631 | 115 ± 14 | 0.256 |
| Diastolic BP (mm Hg) 36–38 GW | 72 ± 9 | 72 ± 9 | 0.192 | 71 ± 10 | 0.589 |
| Pregnancy-induced | |||||
| hypertension | 8 (6.1) | 7 (5.5) | 0.525 | 6 (2.1) | 0.050 |
| Preeclampsia | 6 (4.5) | 5 (3.9) | 0.521 | 4 (1.4) | 0.245 |
| Albuminuria | 3 (2.3) | 0 (0) | 0.129 | 0 (0) | 0.037 |
| Urinary Tract Infection | 25 (18.9) | 9 (7.0) | 0.003 | 18 (6.3) | 0.001 |
| RR (95% CI) | 1 | 0.53 (0.30–0.94) | 0.008 | 0.60 (0.41–0.86) | 0.001 |
| Delivery | |||||
| Vaginal | 95 (72.0) | 92 (71.9) | 192 (67.6) | ||
| Instrumental | 14 (10.6) | 16 (12.5) | 32 (11.3) | ||
| Cesarean section (CS) | 23 (17.4) | 20 (15.6) | 0.848 | 60 (21.1) | 0.708 |
| Emergency (CS) | 10 (7.6) | 2 (1.6) | 0.020 | 5 (1.8) | 0.004 |
| RR (95% CI) for Emergency CS | 1 | 0.70 (0.22–2.27) | 0.383 | 0.15 (0.04–0.50) | 0.001 |
| Perineal Trauma | 15 (11.4) | 4 (3.1) | 0.009 | 4 (1.6) | 0.001 |
| RR (95% CI) | 1 | 0.52 (0.24–0.99) | 0.033 | 0.31 (0.13–0.75) | 0.001 |
| NEONATAL OUTCOMES | |||||
| SHOULDER DYSTOCIA | 1 (0.8) | 0 (0) | 0.508 | 1 (0.4) | 0.315 |
| Gestational Age at birth (weeks) | 39.4 ± 1.4 | 39.3 ± 1.3 | 0.561 | 39.5 ± 1.5 | 0.359 |
| <37 GW | 8 (6.1) | 4 (3.1) | 0.203 | 15 (5.3) | 0.337 |
| <34 GW | 0 | 0 | 1 (0.4) | ||
| Birthweight (g) | 3260 ± 437 | 3243 ± 363 | 0.518 | 3297 ± 471 | 0.789 |
| Percentile | 50.8 ± 25.9 | 52.7 ± 25.4 | 0.677 | 51.7 ± 28.8 | 0.882 |
| Length (cm) | 49.3 ± 2.2 | 49.1 ± 2.0 | 0.560 | 49.5 ± 2.1 | 0.516 |
| Percentile | 43.5 ± 28.7 | 41.1 ± 28.1 | 0.597 | 44.7 ± 29.2 | 0.874 |
| LGA >90 percentile | 8 (6.1) | 1 (0.8) | 0.020 | 11 (3.9) | 0.457 |
| >4500 g | 2 (0.5) | 0 | 3 (1.1) | ||
| SGA <10 percentile | 7 (5.3) | 1 (0.8) | 0.036 | 9 (3.2) | 0.307 |
| Ph Cord Blood | 7.30 ± 0.27 | 7.29 ± 0.07 | 0.573 | 7.28 ± 0.08 | 0.202 |
| ≤7 | 0 (0) | 0 (0) | 2 (0.7) | 0.435 | |
| Apgar Score at 1 min | 8.8 ± 0.7 | 8.8 ± 0.7 | 0.830 | 8.73 ± 1.0 | 0.271 |
| <5 | 3 (2.2) | 3 (2.3) | 0.967 | 3 (1.2) | 0.088 |
| Apgar Score at 5 min | 9.9 ± 0.6 | 9.8 ± 0.5 | 0.338 | 9.8 ± 0.8 | 0.058 |
| <7 | 0 | 0 | 2 (0.8) | ||
| Neonatal | |||||
| Hypoglycemia | 2 (1.5) | 2 (1.6) | 0.677 | 1 (0.4) | 0.599 |
| Respiratory distress | 2 (1.5) | 2 (1.6) | 0.677 | 0 (0) | 0.135 |
| Hiperbilurrubinemia | 15 (11.4) | 13 (10.2) | 0.455 | 10 (3.5) | 0.491 |
| NICU admittance | 5 (3.8) | 5 (3.9) | 0.606 | 7 (2.5) | 0.273 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Melero, V.; García de la Torre, N.; Assaf-Balut, C.; Jiménez, I.; del Valle, L.; Durán, A.; Bordiú, E.; Valerio, J.J.; Herraiz, M.A.; Izquierdo, N.; et al. Effect of a Mediterranean Diet-Based Nutritional Intervention on the Risk of Developing Gestational Diabetes Mellitus and Other Maternal-Fetal Adverse Events in Hispanic Women Residents in Spain. Nutrients 2020, 12, 3505. https://doi.org/10.3390/nu12113505
Melero V, García de la Torre N, Assaf-Balut C, Jiménez I, del Valle L, Durán A, Bordiú E, Valerio JJ, Herraiz MA, Izquierdo N, et al. Effect of a Mediterranean Diet-Based Nutritional Intervention on the Risk of Developing Gestational Diabetes Mellitus and Other Maternal-Fetal Adverse Events in Hispanic Women Residents in Spain. Nutrients. 2020; 12(11):3505. https://doi.org/10.3390/nu12113505
Chicago/Turabian StyleMelero, Verónica, Nuria García de la Torre, Carla Assaf-Balut, Inés Jiménez, Laura del Valle, Alejandra Durán, Elena Bordiú, Johanna J. Valerio, Miguel A Herraiz, Nuria Izquierdo, and et al. 2020. "Effect of a Mediterranean Diet-Based Nutritional Intervention on the Risk of Developing Gestational Diabetes Mellitus and Other Maternal-Fetal Adverse Events in Hispanic Women Residents in Spain" Nutrients 12, no. 11: 3505. https://doi.org/10.3390/nu12113505