The Effect of Timing of Exercise and Eating on Postprandial Response in Adults: A Systematic Review

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
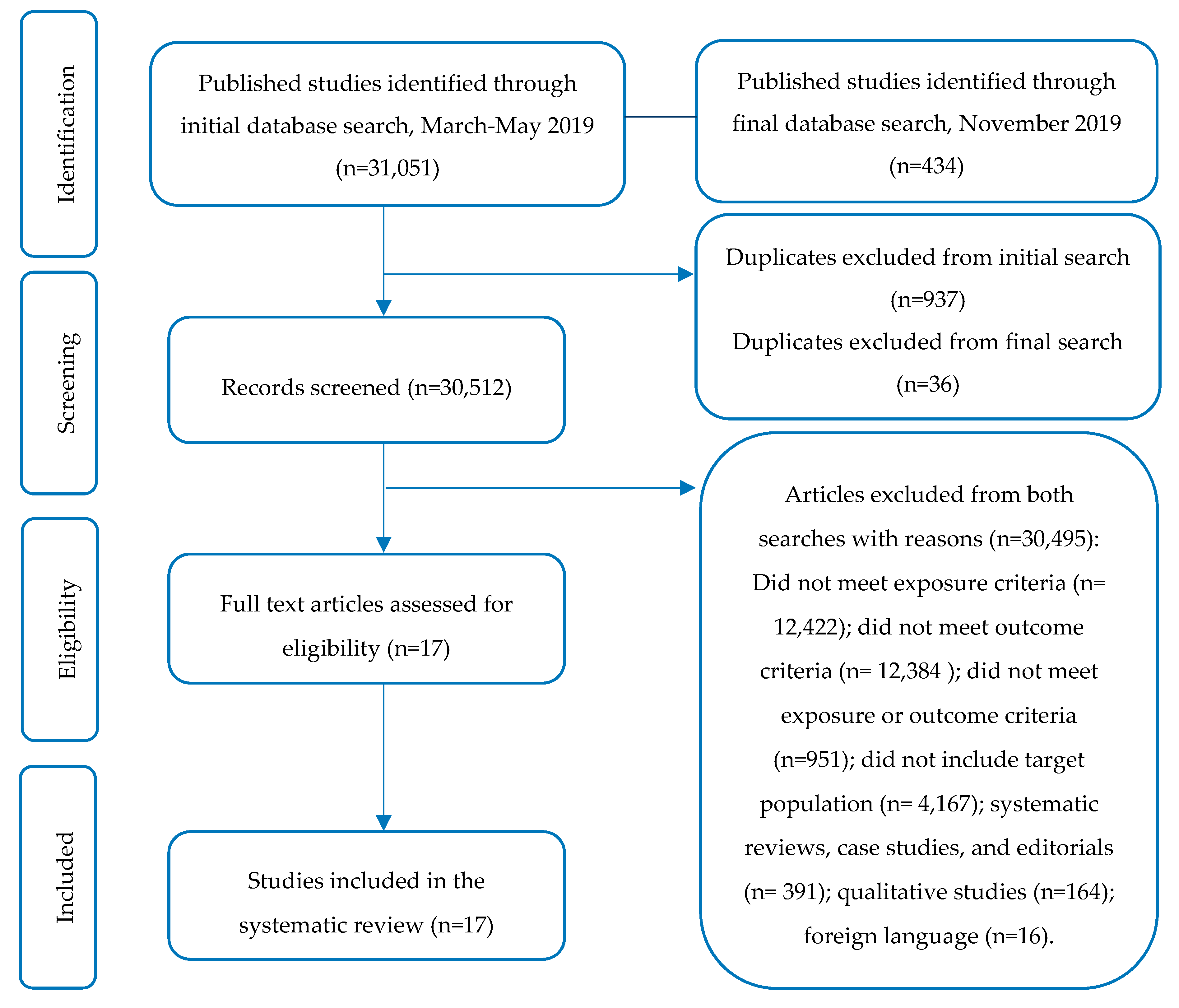
2.1. Literature Search Strategy
2.2. Types of Studies and Eligibility Criteria
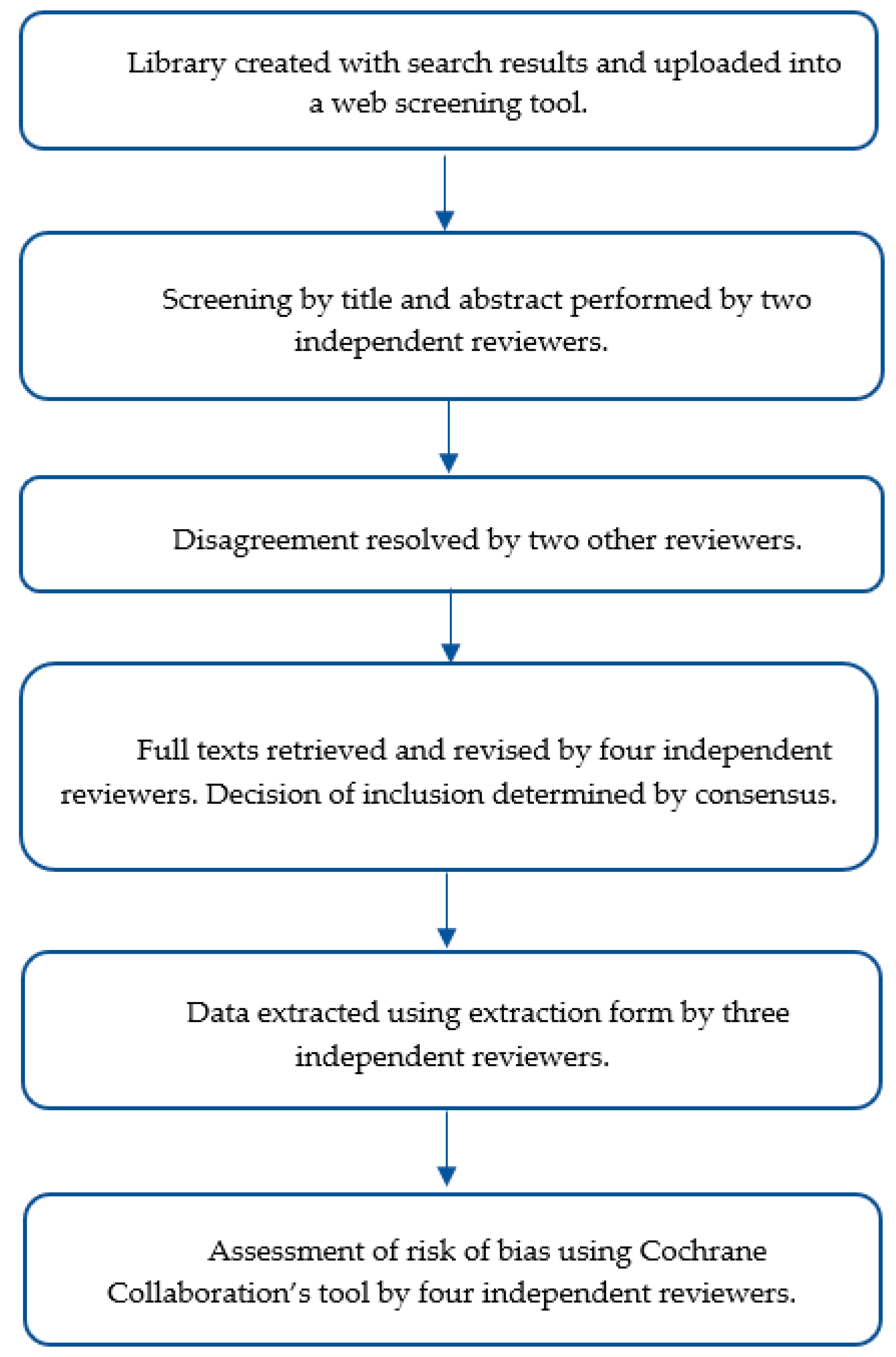
2.3. Study Selection
2.4. Data Collection and Extraction
2.5. Study Quality and Assessment of Risk of Bias in Included Studies
2.6. Data Synthesis and Analysis
3. Results
3.1. Characteristics of Studies Included in the Review
3.2. Risk of Bias Assessment
3.3. Exercise Relative to Breakfast/Morning Meal Consumption
3.4. Exercise Relative to Dinner/Evening Meal Consumption
3.5. Divided Exercise Bouts vs. Conventional Continuous Sessions Performed Pre- or Post-Meals Consumed Throughout the Day
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Centers for Disease Control and Prevention. National Diabetes Statistics Report: Estimates of Diabetes and its Burden in the United States. 2017. Available online: https://www.cdc.gov/diabetes/pdfs/data/statistics/national-diabetes-statistics-report.pdf (accessed on 15 October 2019).
- Klein, S.; Sheard, N.F.; Pi-Sunyer, X.; Daly, A.; Wylie-Rosett, J.; Kulkarni, K.; Clark, N.G. Weight Management Through Lifestyle Modification for the Prevention and Management of Type 2 Diabetes: Rationale and Strategies. Diabetes Care 2004, 27, 2067–2073. [Google Scholar] [CrossRef] [Green Version]
- Scientific Report of the 2015 Dietary Guidelines Advisory Committee: Advisory Report to the Secretary of Health and Human Services and the Secretary of Agriculture; 2015; pp. 1–436. Available online: https://health.gov/dietaryguidelines/2015-scientific-report/PDFs/Scientific-Report-of-the-2015-Dietary-Guidelines-Advisory-Committee.pdf (accessed on 20 September 2019).
- Gillies, C.L.; Abrams, K.R.; Lambert, P.C.; Cooper, N.J.; Sutton, A.J.; Hsu, R.T.; Khunti, K. Pharmacological and lifestyle interventions to prevent or delay type 2 diabetes in people with impaired glucose tolerance: Systematic review and meta-analysis. BMJ 2007, 334, 299. [Google Scholar] [CrossRef] [Green Version]
- Exercise and Type 2 Diabetes: American College of Sports Medicine and the American Diabetes Association. Med. Sci. Sports Exerc. 2010, 42, 2282–2303. [CrossRef] [PubMed]
- Swift, D.L.; McGee, J.E.; Earnest, C.P.; Carlisle, E.; Nygard, M.; Johannsen, N.M. The Effects of Exercise and Physical Activity on Weight Loss and Maintenance. Prog. Cardiovasc. Dis. 2018, 61, 206–213. [Google Scholar] [CrossRef] [PubMed]
- Sjøberg, K.A.; Frøsig, C.; Kjøbsted, R.; Sylow, L.; Kleinert, M.; Betik, A.C.; Shaw, C.S.; Kiens, B.; Wojtaszewski, J.F.P.; Rattigan, S.; et al. Exercise Increases Human Skeletal Muscle Insulin Sensitivity via Coordinated Increases in Microvascular Perfusion and Molecular Signaling. Diabetes 2017, 66, 1501–1510. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boulé, N.G.; Haddad, E.; Kenny, G.P.; Wells, G.A.; Sigal, R.J.; Boulé, N.G.; Haddad, E.; Kenny, G.P.; Wells, G.A.; Sigal, R.J. Effects of exercise on glycemic control and body mass in type 2 diabetes mellitus: A meta-analysis of controlled clinical trials. JAMA 2001, 286, 1218–1250. [Google Scholar] [CrossRef] [PubMed]
- Kollannoor-Samuel, G.; Chhabra, J.; Fernandez, M.L.; Vega-López, S.; Pérez, S.S.; Damio, G.; Calle, M.C.; D’Agostino, D.; Pérez-Escamilla, R. Determinants of Fasting Plasma Glucose and Glycosylated Hemoglobin Among Low Income Latinos with Poorly Controlled Type 2 Diabetes. J. Immigr. Minor. Health 2011, 13, 809–817. [Google Scholar] [CrossRef] [Green Version]
- Marinac, C.R.; Sears, D.D.; Natarajan, L.; Gallo, L.C.; Breen, C.I.; Patterson, R.E. Frequency and Circadian Timing of Eating May Influence Biomarkers of Inflammation and Insulin Resistance Associated with Breast Cancer Risk. PLoS ONE 2015, 10, e0136240. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.B.; Patterson, R.E.; Ang, A.; Emond, J.A.; Shetty, N.; Arab, L. Timing of energy intake during the day is associated with the risk of obesity in adults. J. Hum. Nutr. Diet. 2014, 27, 255–262. [Google Scholar] [CrossRef]
- Jakubowicz, D.; Barnea, M.; Wainstein, J.; Froy, O. High Caloric intake at breakfast vs. dinner differentially influences weight loss of overweight and obese women: Effect of High-Calorie Breakfast vs. Dinner. Obesity 2013, 21, 2504–2512. [Google Scholar] [CrossRef]
- St-Onge, M.-P.; Ard, J.; Baskin, M.L.; Chiuve, S.E.; Johnson, H.M.; Kris-Etherton, P.; Varady, K. Meal Timing and Frequency: Implications for Cardiovascular Disease Prevention: A Scientific Statement from the American Heart Association. Circulation 2017, 135, e96–e121. [Google Scholar] [CrossRef] [PubMed]
- Reutrakul, S.; Hood, M.M.; Crowley, S.J.; Morgan, M.K.; Teodori, M.; Knutson, K.L. The Relationship Between Breakfast Skipping, Chronotype, and Glycemic Control in Type 2 Diabetes. Chronobiol. Int. 2014, 31, 64–71. [Google Scholar] [CrossRef] [PubMed]
- Chomistek, A.K.; Shiroma, E.J.; Lee, I.-M. The Relationship between Time of Day of Physical Activity and Obesity in Older Women. J. Phys. Act. Health 2016, 13, 416–418. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Jastremski, C.A.; Wallace, J.P. Time of day for exercise on blood pressure reduction in dipping and nondipping hypertension. J. Hum. Hypertens. 2005, 19, 597–605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, T.; Lu, C.; Schumann, M.; Le, S.; Yang, Y.; Zhuang, H.; Lu, Q.; Liu, J.; Wiklund, P.; Cheng, S. Timing of Exercise Affects Glycemic Control in Type 2 Diabetes Patients Treated with Metformin. J. Diabetes Res. 2018, 2018, 2483273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Francois, M.E.; Baldi, J.C.; Manning, P.J.; Lucas, S.J.E.; Hawley, J.A.; Williams, M.J.A.; Cotter, J.D. ‘Exercise snacks’ before meals: A novel strategy to improve glycaemic control in individuals with insulin resistance. Diabetologia 2014, 57, 1437–1445. [Google Scholar] [CrossRef] [PubMed]
- Farah, N.M.F.; Gill, J.M.R. Effects of exercise before or after meal ingestion on fat balance and postprandial metabolism in overweight men. Br. J. Nutr. 2013, 109, 2297–2307. [Google Scholar] [CrossRef] [Green Version]
- Erickson, M.L.; Little, J.P.; Gay, J.L.; McCully, K.K.; Jenkins, N.T. Effects of postmeal exercise on postprandial glucose excursions in people with type 2 diabetes treated with add-on hypoglycemic agents. Diabetes Res. Clin. Pract. 2017, 126, 240–247. [Google Scholar] [CrossRef]
- Terada, T.; Wilson, B.J.; Myette-Côté, E.; Kuzik, N.; Bell, G.J.; McCargar, L.J.; Boulé, N.G. Targeting specific interstitial glycemic parameters with high-intensity interval exercise and fasted-state exercise in type 2 diabetes. Metabolism 2016, 65, 599–608. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Altman, D.G.; Gotzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Z.; Hu, Y.; Yan, R.; Li, H.; Zhang, D.; Li, F.; Su, X.; Ma, J. Twenty Minute Moderate-Intensity Post-Dinner Exercise Reduces the Postprandial Glucose Response in Chinese Patients with Type 2 Diabetes. Med. Sci. Monit. 2018, 24, 7170–7177. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, A.N.; Mann, J.I.; Williams, S.; Venn, B.J. Advice to walk after meals is more effective for lowering postprandial glycaemia in type 2 diabetes mellitus than advice that does not specify timing: A randomised crossover study. Diabetologia 2016, 59, 2572–2578. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oberlin, D.J.; Mikus, C.R.; Kearney, M.L.; Hinton, P.S.; Manrique, C.; Leidy, H.J.; Kanaley, J.A.; Rector, R.S.; Thyfault, J.P. One Bout of Exercise Alters Free-Living Postprandial Glycemia in Type 2 Diabetes. Med. Sci. Sports Exerc. 2014, 46, 232–238. [Google Scholar] [CrossRef] [Green Version]
- Heden, T.D.; Winn, N.C.; Mari, A.; Booth, F.W.; Rector, R.S.; Thyfault, J.P.; Kanaley, J.A. Postdinner resistance exercise improves postprandial risk factors more effectively than predinner resistance exercise in patients with type 2 diabetes. J. Appl. Physiol. 2015, 118, 624–634. [Google Scholar] [CrossRef] [Green Version]
- Colberg, S.R.; Zarrabi, L.; Bennington, L.; Nakave, A.; Thomas Somma, C.; Swain, D.P.; Sechrist, S.R. Postprandial Walking is Better for Lowering the Glycemic Effect of Dinner than Pre-Dinner Exercise in Type 2 Diabetic Individuals. J. Am. Med. Dir. Assoc. 2009, 10, 394–397. [Google Scholar] [CrossRef]
- Poirier, P.; Mawhinney, S.; Grondin, L.; Tremblay, A.; Broderick, T.; CléRoux, J.; Catellier, C.; TancréDe, G.; Nadeau, A. Prior meal enhances the plasma glucose lowering effect of exercise in type 2 diabetes. Med. Sci. Sports Exerc. 2001, 33, 1259–1264. [Google Scholar] [CrossRef]
- Rees, J.L.; Chang, C.R.; François, M.E.; Marcotte-Chénard, A.; Fontvieille, A.; Klaprat, N.D.; Dyck, R.A.; Funk, D.R.; Snydmiller, G.; Bastell, K.; et al. Minimal effect of walking before dinner on glycemic responses in type 2 diabetes: Outcomes from the multi-site E-PAraDiGM study. Acta Diabetol. 2019, 56, 755–765. [Google Scholar] [CrossRef] [PubMed]
- Manohar, C.; Levine, J.A.; Nandy, D.K.; Saad, A.; Dalla Man, C.; McCrady-Spitzer, S.K.; Basu, R.; Cobelli, C.; Carter, R.E.; Basu, A.; et al. The Effect of Walking on Postprandial Glycemic Excursion in Patients with Type 1 Diabetes and Healthy People. Diabetes Care 2012, 35, 2493–2499. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nygaard, H.; Tomten, S.E.; Høstmark, A.T. Slow postmeal walking reduces postprandial glycemia in middle-aged women. Appl. Physiol. Nutr. Metab. 2009, 34, 1087–1092. [Google Scholar] [CrossRef] [PubMed]
- Høstmark, A.T.; Ekeland, G.S.; Beckstrøm, A.C.; Meen, H.D. Postprandial light physical activity blunts the blood glucose increase. Prev. Med. 2006, 42, 369–371. [Google Scholar] [CrossRef]
- Nelson, J.D.; Poussier, P.; Marliss, E.B.; Albisser, A.M.; Zinman, B. Metabolic response of normal man and insulin-infused diabetics to postprandial exercise. Am. J. Physiol. Endocrinol. Metab. 1982, 242, E309–E316. [Google Scholar] [CrossRef]
- Lunde, M.S.H.; Hjellset, V.T.; Høstmark, A.T. Slow Post Meal Walking Reduces the Blood Glucose Response: An Exploratory Study in Female Pakistani Immigrants. J. Immigr. Minor. Health 2012, 14, 816–822. [Google Scholar] [CrossRef]
- Haxhi, J.; Scotto di Palumbo, A.; Sacchetti, M. Exercising for Metabolic Control: Is Timing Important. Ann. Nutr. Metab. 2013, 62, 14–25. [Google Scholar] [CrossRef]
- Derave, W.; Mertens, A.; Muls, E.; Pardaens, K.; Hespel, P. Effects of Post-absorptive and Postprandial Exercise on Glucoregulation in Metabolic Syndrome. Obesity 2007, 15, 704–711. [Google Scholar] [CrossRef] [Green Version]
- Jessen, N.; Goodyear, L.J. Contraction signaling to glucose transport in skeletal muscle. J. Appl. Physiol. 2005, 99, 330–337. [Google Scholar] [CrossRef] [Green Version]
- Little, J.P.; Francois, M.E. High-Intensity Interval Training for Improving Postprandial Hyperglycemia. Res. Q. Exerc. Sport 2014, 85, 451–456. [Google Scholar] [CrossRef]
- Cassidy, S.; Thoma, C.; Houghton, D.; Trenell, M.I. High-intensity interval training: A review of its impact on glucose control and cardiometabolic health. Diabetologia 2017, 60, 7–23. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Citation | Study Length | n (M: F) | Age (Years) Mean ± SD | Disease Condition | Intervention/ Comparison | Treatment Effects (↑, ↓, ↔) | Assessment Duration | Glycemic Response | |
|---|---|---|---|---|---|---|---|---|---|
| PP Plasma Glucose | Glucose AUC | ||||||||
| Exercise relative to breakfast/morning meal consumption | |||||||||
| Erickson et al. [20] | 2 days | 8 (5:3) | 60 ± 10.7 | Obesity/T2D | Control day (no exercise) vs. exercise post-breakfast | ↓ glucose | 2 h | Exercise post-breakfast: Significantly lower PG peak and decreasing glucose over time | Significant difference in average on 2 h iAUC |
| Huang et al. [17] | 4 days | 26 (12:14) | 53.8 ± 8.6 | OW/T2D | No exercise (control) vs. exercise post-breakfast (EX30) vs. exercise 60 min post-breakfast (EX60) vs. exercise 90 min post-breakfast (EX90) | ↓ PPG | NA | Compared to control, declines in PG immediately post-exercise were larger in EX30, EX60, and EX90; capillary glucose decreased significantly after exercise in EX30, EX60, and EX90 | Not reported |
| Nelson et al. [33] | 2 days | 7 (4:3) | 33.3 ± 2 | Healthy | Control (no exercise) vs. post-breakfast exercise | ↓ glycemia | 0, 30, 75, 95, 135, 180 min. | Post-breakfast exercise: Significant ↓ in glycemia | Not reported |
| Oberlin et al. [25] | 4 days | 9 (4:5) | 60.1 ± 1 | Obesity/T2D | Control (no exercise) vs. pre-breakfast exercise | ↓ 24 h average blood glucose | 24 h avg glucose, 4 h glucose AUC, 2 h PPG | Pre-breakfast exercise significantly lowered avg. PG concentration during first 24 h period compared to control (5.98 vs. 6.62 mmol/L) | Main effect of exercise to lower PPG-AUC across all 6 meals compared to control |
| Poirier et al. [28] | 2 days | 10 (10:0) | 54 ± 5 | Sedentary/T2D | Exercise pre-meal vs. post-breakfast exercise | ↓ plasma glucose (post-meal exercise) | 2 h | Mean decrease in PG concentration was 4.8 ± 1.9 mmol/L (60 ± 14% of baseline) vs. 1.0 ± 0.8 mmol/L (91 ± 6% of baseline) in post-meal vs. pre-meal exercise, respectively. Significantly lower PG level in post-meal vs. pre-meal condition (7.6 vs. 10.0 mmol/L) | Not reported |
| Terada et al. [21] | 5 days | 10 (8:2) | 60 ± 6 | Obesity/T2D | Control (no exercise) vs. pre-breakfast HIIE vs. post-breakfast HIIE vs. pre-breakfast MICE vs. post-breakfast MICE | ↓ PPG | 24 h mean interstitial glucose concentration, 1 h mean PPG | Compared to post-meal exercise, pre-meal condition significantly attenuated PP glycemic increments | Comparing all exercise conditions to control, pre-meal HIIE significantly lowered total post-meal iAUC |
| Farah et al. [19] | 3 days | 10 (10:0) | 28.1 ± 10.7 | OW | Control (no exercise) vs. pre-breakfast vs. post-breakfast exercise | ↔ PPG | 7 h PPG | No difference in glycemic response between conditions | Not reported |
| Lunde et al. [34] | 3 days | 11 (0:11) | 44 ± NA | Obesity/diabetes prone | Control (no exercise) vs. post-breakfast 20 min. walk vs. post-breakfast 40 min walk | ↓ PPG | 2 h PPG | PPG and PG peak value significantly decreased with increasing duration of slow post-breakfast walking | 2 h glucose iAUC decreased with increasing duration of slow post-meal walking |
| Høstmark et al. [32] | 2 days | 39 (0:39) | Trained young: 22.5 ± 0.5 Trained middle-age: 49.2 ± 1.3 Sedentary young: 24.1 ± 0.7 Sedentary middle-age: 59.2 ± 1.7 | Sedentary and trained | Control vs. exercise post- breakfast | ↓ peak glucose value ↓ blood glucose | NA | Exercise post-breakfast: Peak PG was lower than control | Not reported |
| Nygaard et al. [31] | 3 days | 13 (0:13) | Not listed | Healthy | Control (no exercise) vs. post-breakfast 15 min. walk vs. post-breakfast 40 min walk | ↓ blood glucose | 15, 22.5, 30, 37.5, 45, 55, 65, 75, 90, 105, 120 min | Compared to control, peak PG value was 0.8 mmol/L lower (significant) in post-breakfast 40 min walk condition | Significant main effect of walking time on 2 h iAUC; participants with the largest 2 h PG iAUC on the control day demonstrated the greatest reduction in PPG response when walking 40 min post-breakfast |
| Exercise relative to dinner/ evening meal consumption | |||||||||
| Colberg et al. [27] | 3 days | 12 (6:6) | 61.47 ± 2.7 | Obesity/T2D | Control day (no exercise) vs. exercise pre-dinner vs. exercise post-dinner | ↓ plasma glucose | 4 h | Exercise post-dinner: Significantly lower PG levels at the end of exercise compared to at the same time point when participants had exercised pre-dinner | Total glucose AUC over 4 h was not significantly different among trials |
| Heden et al. [26] | 3 days | 13 (5:8) | 48.5 ± 11.9 | Obesity/T2D | No resistance exercise (control) vs. pre-dinner resistance exercise vs. post-dinner resistance exercise | ↓ glucose iAUC (exercise pre-meal) | NA | Not reported | Significant reduction in glucose iAUC by ~18% and 30% in pre- and post-dinner exercise, respectively |
| Li et al. [23] | 2 days | 29 (22:7) | 51 ± 11.2 | T2D | Control (no exercise) vs. post-dinner exercise | ↓ PP hyperglycemia | 2 h PPG | Post-dinner exercise vs. control: Significant lowering in 2 h PPG spike (1.9 ± 1.3 vs. 2.7 ± 1.4 mmol/L), 2 h PP peak glucose (9.3 ± 1.6 vs. 10.3 ± 2.3 mmol/L), and 2 h PP mean glucose levels (8.2 ± 1.3 vs. 8.9 ± 2.0 mmol/L) | Post-dinner exercise: Glucose tAUC 1 h after exercise was significantly lower than control (493.9 ± 84.0 vs. 559.3 ± 130.5 mmol/L × 60 min) |
| Rees et al. [29] | 1 week | 73 (33:40) | 63.5 ± 9.1 | Obesity/T2D | Control (no exercise) vs. pre-dinner walking | ↓ blood glucose | 24 h glucose, 2 h PPG | Exercise had no effect on PPG or 24 h glucose variability; significant reduction in PG concentration during walking in exercise condition vs. control (−1.56 mmol/L) | Not reported |
| Divided bouts vs. conventional continuous exercise performed pre- or post-meals consumed throughout the day | |||||||||
| Francois et al. [18] | 3 days | 9 (7:2) | 48 ± 6 | Obesity/insulin resistant T2D | Control (continuous exercise pre-dinner) vs. exercise snacking pre-mean meals (ES) vs. composite exercise snacking pre- main meals (CES) | ↓ mean PPG (post- dinner and breakfast) | 3 h PPG and mean PPG, 24 h glucose concentration | ES significantly attenuated mean 3 h PPG concentrations following breakfast (0.4 ± 1.0 mmol/L) and 24 h mean PG concentrations by 0.7± 0.6 mmol/L relative to baseline | Not reported |
| Manohar et al. [30] | 3 days | 12 (5:7) | 37.7 ± 13.7 | Healthy | Control (no exercise) vs. post-meal exercise | ↓ PPG excursions | NA | Baseline CGM PG concentration lower with post-meal exercise vs. control (5.61 mmol/L vs. 5.58 mmol/L); peak CGM PG concentration lower with post-meal exercise vs. control (8.25 mmol/L and 11.99 mmol/L) | Post-meal exercise: iAUC was estimated to be significantly lower than control (4.5 mmol/L/270 min vs. 9.6 mmol/L/270 min), respectively |
| Reynolds et al. [24] | 2 weeks | 41 (26:15) | 60 ± 9.9 | Obesity/T2D | 30 min walk at any time of day vs. 10 min walk post 3 main meals | ↓ PPG | 3 h | Significantly lower 3 h mean PG levels following evening meal with post-meal walking compared to conventional condition (−0.50 mmol/L) | Glucose iAUC was 12% lower in the post-meal compared to conventional condition |
| Author [ref] | Random Sequence Generation | Allocation Concealment | Selective Reporting | Blinding | Incomplete Outcome Data | Other Bias | |
|---|---|---|---|---|---|---|---|
| Participants/personnel | Outcomes assessment | ||||||
| Colberg et al. [27] | U | L | L | L | U | U | L |
| Erickson et al. [20] | H | L | L | L | U | L | L |
| Farah et al. [19] | L | L | L | L | U | U | L |
| Francois et al. [18] | U | L | L | L | U | L | L |
| Heden et al. [26] | U | L | L | L | U | U | L |
| Høstmark et al. [32] | H | L | L | L | U | U | L |
| Huang et al. [17] | U | L | L | L | U | L | L |
| Li et al. [23] | U | L | L | L | U | L | L |
| Lunde et al. [34] | H | L | L | L | U | L | L |
| Manohar et al. [30] | U | L | L | L | U | L | M |
| Nelson et al. [33] | U | L | L | L | U | L | M |
| Nygaard et al. [31] | U | L | L | L | U | L | L |
| Oberlin et al. [25] | U | L | L | L | U | U | L |
| Poirier et al. [28] | U | L | L | L | U | L | L |
| Rees et al. [29] | L | L | L | L | U | L | L |
| Reynolds et al. [24] | L | L | L | L | L | L | L |
| Terada et al. [21] | L | L | L | L | U | U | L |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aqeel, M.; Forster, A.; Richards, E.A.; Hennessy, E.; McGowan, B.; Bhadra, A.; Guo, J.; Gelfand, S.; Delp, E.; Eicher-Miller, H.A. The Effect of Timing of Exercise and Eating on Postprandial Response in Adults: A Systematic Review. Nutrients 2020, 12, 221. https://doi.org/10.3390/nu12010221
Aqeel M, Forster A, Richards EA, Hennessy E, McGowan B, Bhadra A, Guo J, Gelfand S, Delp E, Eicher-Miller HA. The Effect of Timing of Exercise and Eating on Postprandial Response in Adults: A Systematic Review. Nutrients. 2020; 12(1):221. https://doi.org/10.3390/nu12010221
Chicago/Turabian StyleAqeel, Marah, Anna Forster, Elizabeth A. Richards, Erin Hennessy, Bethany McGowan, Anindya Bhadra, Jiaqi Guo, Saul Gelfand, Edward Delp, and Heather A. Eicher-Miller. 2020. "The Effect of Timing of Exercise and Eating on Postprandial Response in Adults: A Systematic Review" Nutrients 12, no. 1: 221. https://doi.org/10.3390/nu12010221