Dietary Intake and Its Determinants Among Adults Living in the Metropolitan Area of Puerto Rico

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Sociodemographic and Lifestyle Measures
2.3. Dietary Assessment
2.4. Statistical Analyses
3. Results
3.1. Participant Characteristics
3.2. Nutrient and Food Intake
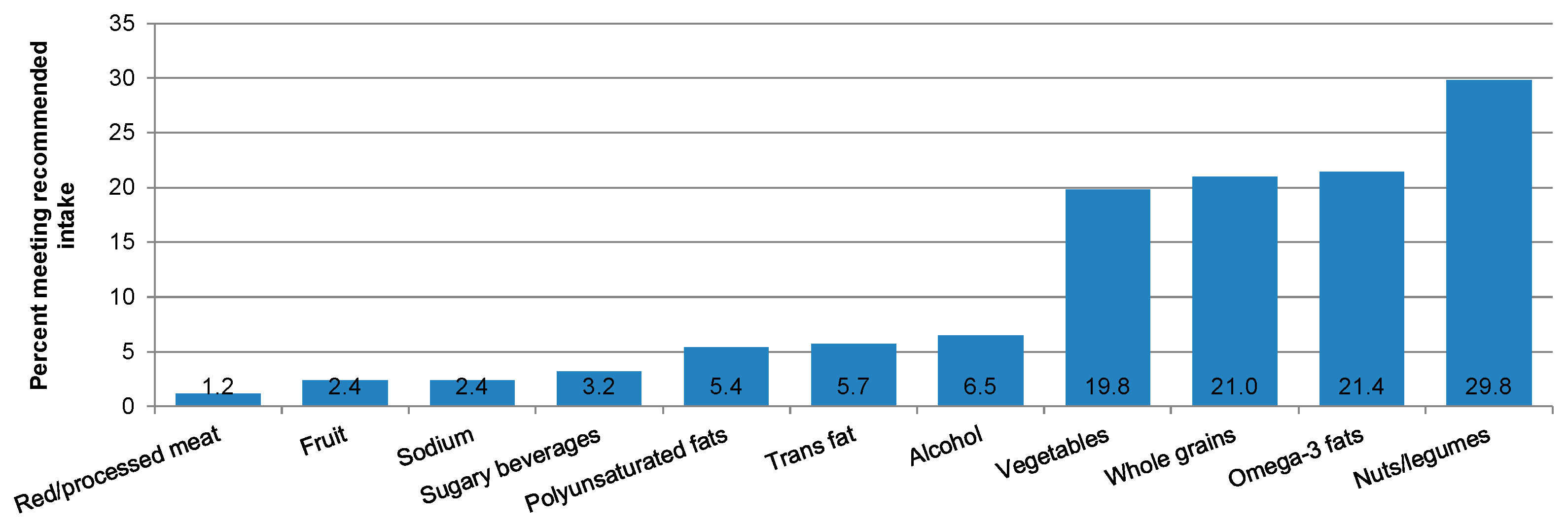
3.3. Diet Quality
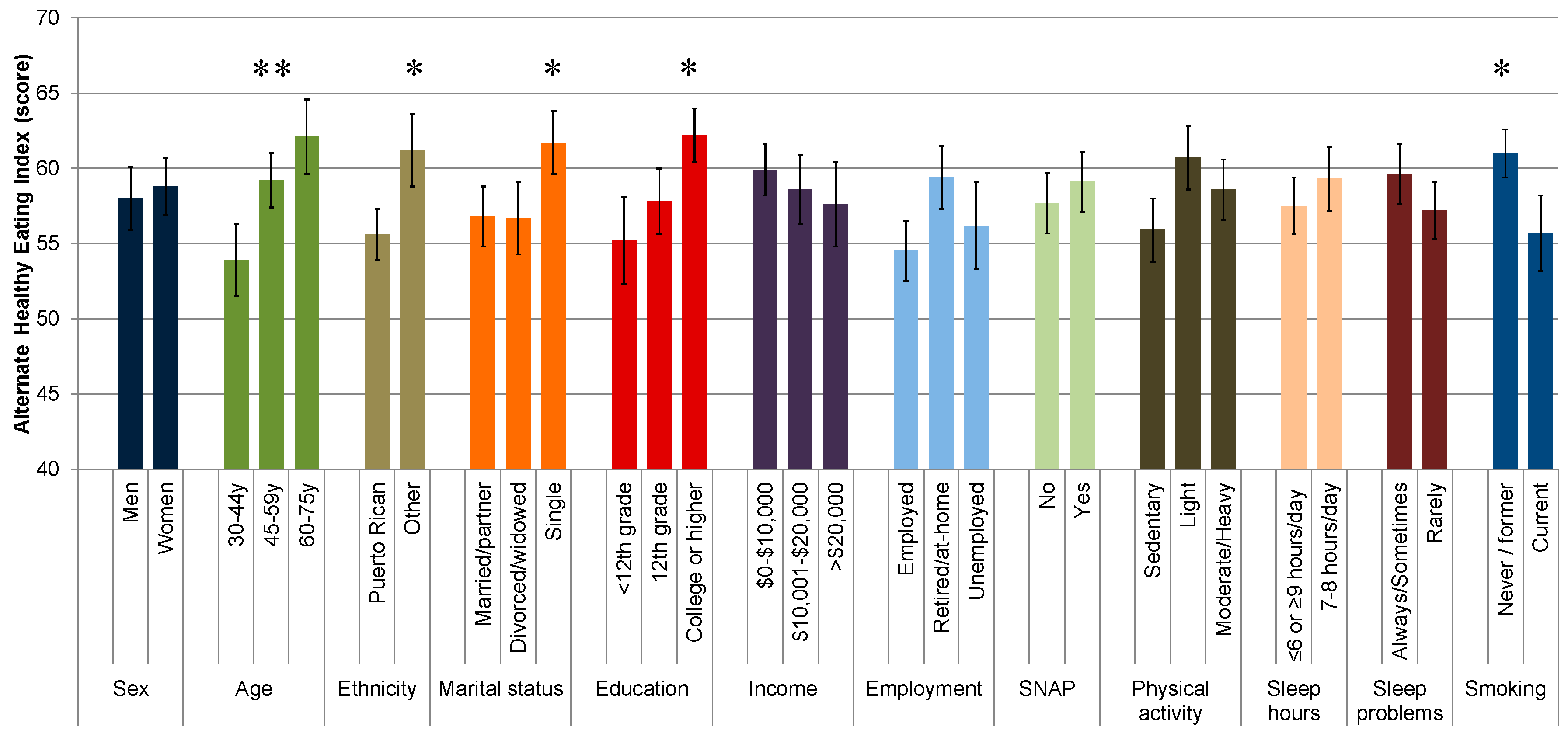
3.4. Determinants of Diet Quality
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Willett, W.C.; Koplan, J.P.; Nugent, R.; Dusenbury, C.; Puska, P.; Gaziano, T.A. Prevention of Chronic Disease by Means of Diet and Lifestyle Changes. In Disease Control Priorities in Developing Countries, 2nd ed.; Jamison, D.T., Breman, J.G., Measham, A.R., Alleyne, G., Claeson, M., Evans, D.B., Jha, P., Mills, A., Musgrove, P., Eds.; World Bank and Oxford University Press: Washington, DC, USA, 2006. [Google Scholar]
- Belin, R.J.; Greenland, P.; Allison, M.; Martin, L.; Shikany, J.M.; Larson, J.; Tinker, L.; Howard, B.V.; Lloyd-Jones, D.; Van Horn, L. Diet quality and the risk of cardiovascular disease: The Women’s Health Initiative (WHI). Am. J. Clin. Nutr. 2011, 94, 49–57. [Google Scholar] [CrossRef] [PubMed]
- Fung, T.T.; McCullough, M.; van Dam, R.M.; Hu, F.B. A prospective study of overall diet quality and risk of type 2 diabetes in women. Diabetes Care 2007, 30, 1753–1757. [Google Scholar] [CrossRef] [PubMed]
- Kwan, L.L.; Bermudez, O.I.; Tucker, K.L. Low vitamin B-12 intake and status are more prevalent in Hispanic older adults of Caribbean origin than in neighborhood-matched non-Hispanic whites. J. Nutr. 2002, 132, 2059–2064. [Google Scholar] [CrossRef] [PubMed]
- Mattei, J.; Bhupathiraju, S.; Tucker, K.L. Higher adherence to a diet score based on American Heart Association recommendations is associated with lower odds of allostatic load and metabolic syndrome in Puerto Rican adults. J. Nutr. 2013, 143, 1753–1759. [Google Scholar] [CrossRef] [PubMed]
- Mattei, J.; Sotos-Prieto, M.; Bigornia, S.J.; Noel, S.E.; Tucker, K.L. The Mediterranean Diet Score Is More Strongly Associated with Favorable Cardiometabolic Risk Factors over 2 Years Than Other Diet Quality Indexes in Puerto Rican Adults. J. Nutr. 2017, 147, 661–669. [Google Scholar] [CrossRef] [PubMed]
- Mattei, J.; Sotres-Alvarez, D.; Daviglus, M.L.; Gallo, L.C.; Gellman, M.; Hu, F.B.; Tucker, K.L.; Willett, W.C.; Siega-Riz, A.M.; Van Horn, L.; et al. Diet Quality and Its Association with Cardiometabolic Risk Factors Vary by Hispanic and Latino Ethnic Background in the Hispanic Community Health Study/Study of Latinos. J. Nutr. 2016, 146, 2035–2044. [Google Scholar] [CrossRef] [Green Version]
- Siega-Riz, A.M.; Sotres-Alvarez, D.; Ayala, G.X.; Ginsberg, M.; Himes, J.H.; Liu, K.; Loria, C.M.; Mossavar-Rahmani, Y.; Rock, C.L.; Rodriguez, B.; et al. Food-group and nutrient-density intakes by Hispanic and Latino backgrounds in the Hispanic Community Health Study/Study of Latinos. Am. J. Clin. Nutr. 2014, 99, 1487–1498. [Google Scholar] [CrossRef]
- Sotos-Prieto, M.; Bhupathiraju, S.N.; Falcon, L.M.; Gao, X.; Tucker, K.L.; Mattei, J. Association between a Healthy Lifestyle Score and inflammatory markers among Puerto Rican adults. Nutr. Metab. Cardiovasc. Dis. 2016, 26, 178–184. [Google Scholar] [CrossRef]
- Satia-Abouta, J. Dietary Acculturation: Definition, Process, Assessment, and Implications. Int. J. Hum. Ecol. 2003, 4, 71–86. [Google Scholar]
- Colon-Ramos, U.; Perez-Cardona, C.M.; Monge-Rojas, R. Socio-demographic, behavioral, and health correlates of nutrition transition dietary indicators in San Juan, Puerto Rico. Rev. Panam. Salud Publica 2013, 34, 330–335. [Google Scholar]
- Colon-Lopez, V.; Banerjee, G.; Gertz, A.M.; Ortiz, A.P.; Calo, W.; Finney-Rutten, L.J.; Colon-Ramos, U.; Hesse, B.W.; Tortolero, G. Behavioral correlates of fruit and vegetable intake in Puerto Rico: Results from the Health Information National Trends Survey. P. R. Health Sci. J. 2013, 32, 194–199. [Google Scholar] [PubMed]
- Soltero, S.M.; Palacios, C. Association between dietary patterns and body composition in a group or Puerto Rican obese adults: A pilot study. P. R. Health Sci. J. 2011, 30, 22–27. [Google Scholar] [PubMed]
- Suarez-Martinez, E.B.; Perez, C.M.; Cruz, S.K.; Khorsandi, S.; Chardon, C.; Ferder, L. Importance of vitamin D and vitamin D levels status in Puerto Ricans. J. Health Care Poor Underserved 2011, 24, 38–47. [Google Scholar] [CrossRef] [PubMed]
- Truesdell, E.; Schelske-Santos, M.; Nazario, C.M.; Rosario-Rosado, R.V.; McCann, S.E.; Millen, A.E.; Ramirez-Marrero, F.A.; Freudenheim, J.L. Foods Contributing to Macronutrient Intake of Women Living in Puerto Rico Reflect Both Traditional Puerto Rican and Western-Type Diets. Nutrients 2018, 10, 1242. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Ayuso, I.R. Encuesta de Consumo de Alimentos en Establecimientos de Comida Rápida 2013; Instituto de Estadísticas de Puerto Rico: San Juan, Puerto Rico, 2017; Available online: https://estadisticas.pr/files/Publicaciones/Encuesta_consumo_comida_rapida_20170619.pdf (accessed on 13 May 2019).
- Lopez-Cepero, A.; Valencia, A.; Jimenez, J.; Lemon, S.C.; Palacios, C.; Rosal, M.C. Comparison of Dietary Quality Among Puerto Ricans Living in Massachusetts and Puerto Rico. J. Immigr. Minority Health 2017, 19, 494–498. [Google Scholar] [CrossRef] [PubMed]
- Tucker, K.L.; Mattei, J.; Noel, S.E.; Collado, B.M.; Mendez, J.; Nelson, J.; Griffith, J.; Ordovas, J.M.; Falcon, L.M. The Boston Puerto Rican Health Study, a longitudinal cohort study on health disparities in Puerto Rican adults: Challenges and opportunities. BMC Public Health 2010, 10, 107. [Google Scholar] [CrossRef] [PubMed]
- Mattei, J.; Rodriguez-Orengo, J.F.; Tamez, M.; Corujo, F.; Claudio, A.; Villanueva, H.; Campos, H.; Willett, W.C.; Tucker, K.L.; Rios-Bedoya, C.F. Challenges and opportunities in establishing a collaborative multisite observational study of chronic diseases and lifestyle factors among adults in Puerto Rico. BMC Public Health 2017, 17, 136. [Google Scholar] [CrossRef]
- Lachat, C.; Hawwash, D.; Ocke, M.C.; Berg, C.; Forsum, E.; Hornell, A.; Larsson, C.; Sonestedt, E.; Wirfalt, E.; Akesson, A.; et al. Strengthening the Reporting of Observational Studies in Epidemiology-Nutritional Epidemiology (STROBE-nut): An Extension of the STROBE Statement. PLoS Med. 2016, 13, e1002036. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)--a metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef]
- Paffenbarger, R.S., Jr.; Wing, A.L.; Hyde, R.T. Physical activity as an index of heart attack risk in college alumni. Am. J. Epidemiol. 1978, 108, 161–175. [Google Scholar] [CrossRef]
- Sotos-Prieto, M.; Bhupathiraju, S.N.; Falcon, L.M.; Gao, X.; Tucker, K.L.; Mattei, J. A Healthy Lifestyle Score Is Associated with Cardiometabolic and Neuroendocrine Risk Factors among Puerto Rican Adults. J. Nutr. 2015, 145, 1531–1540. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tucker, K.L.; Bianchi, L.A.; Maras, J.; Bermudez, O.I. Adaptation of a food frequency questionnaire to assess diets of Puerto Rican and non-Hispanic adults. Am. J. Epidemiol. 1998, 148, 507–518. [Google Scholar] [CrossRef] [PubMed]
- Palacios, C.; Trak, M.A.; Betancourt, J.; Joshipura, K.; Tucker, K.L. Validation and reproducibility of a semi-quantitative FFQ as a measure of dietary intake in adults from Puerto Rico. Public Health Nutr. 2015, 18, 2550–2558. [Google Scholar] [CrossRef] [PubMed]
- Bermudez, O.I.; Ribaya-Mercado, J.D.; Talegawkar, S.A.; Tucker, K.L. Hispanic and non-Hispanic white elders from Massachusetts have different patterns of carotenoid intake and plasma concentrations. J. Nutr. 2005, 135, 1496–1502. [Google Scholar] [CrossRef] [PubMed]
- Gao, X.; Martin, A.; Lin, H.; Bermudez, O.I.; Tucker, K.L. Alpha-Tocopherol intake and plasma concentration of Hispanic and non-Hispanic white elders is associated with dietary intake pattern. J. Nutr. 2006, 136, 2574–2579. [Google Scholar] [CrossRef] [PubMed]
- Chiuve, S.E.; Fung, T.T.; Rimm, E.B.; Hu, F.B.; McCullough, M.L.; Wang, M.; Stampfer, M.J.; Willett, W.C. Alternative dietary indices both strongly predict risk of chronic disease. J. Nutr. 2012, 142, 1009–1018. [Google Scholar] [CrossRef] [PubMed]
- Mattei, J.; Malik, V.; Hu, F.B.; Campos, H. Substituting homemade fruit juice for sugar-sweetened beverages is associated with lower odds of metabolic syndrome among Hispanic adults. J. Nutr. 2012, 142, 1081–1087. [Google Scholar] [CrossRef]
- Malik, V.S.; Popkin, B.M.; Bray, G.A.; Despres, J.P.; Hu, F.B. Sugar-sweetened beverages, obesity, type 2 diabetes mellitus, and cardiovascular disease risk. Circulation 2010, 121, 1356–1364. [Google Scholar] [CrossRef]
- Noel, S.E.; Newby, P.K.; Ordovas, J.M.; Tucker, K.L. A traditional rice and beans pattern is associated with metabolic syndrome in Puerto Rican older adults. J. Nutr. 2009, 139, 1360–1367. [Google Scholar] [CrossRef]
- Feng, R.; Du, S.; Chen, Y.; Zheng, S.; Zhang, W.; Na, G.; Li, Y.; Sun, C. High carbohydrate intake from starchy foods is positively associated with metabolic disorders: A Cohort Study from a Chinese population. Sci. Rep. 2015, 5, 16919. [Google Scholar] [CrossRef]
- Bahadoran, Z.; Mirmiran, P.; Azizi, F. Fast Food Pattern and Cardiometabolic Disorders: A Review of Current Studies. Health Promot. Perspect. 2015, 5, 231–240. [Google Scholar] [CrossRef]
- Sun, Q.; Spiegelman, D.; van Dam, R.M.; Holmes, M.D.; Malik, V.S.; Willett, W.C.; Hu, F.B. White rice, brown rice, and risk of type 2 diabetes in US men and women. Arch. Intern. Med. 2010, 170, 961–969. [Google Scholar] [CrossRef] [PubMed]
- Mattei, J.; Hu, F.B.; Campos, H. A higher ratio of beans to white rice is associated with lower cardiometabolic risk factors in Costa Rican adults. Am. J. Clin. Nutr. 2011, 94, 869–876. [Google Scholar] [CrossRef] [PubMed]
- Song, M.; Fung, T.T.; Hu, F.B.; Willett, W.C.; Longo, V.D.; Chan, A.T.; Giovannucci, E.L. Association of Animal and Plant Protein Intake with All-Cause and Cause-Specific Mortality. JAMA Intern. Med. 2016, 176, 1453–1463. [Google Scholar] [CrossRef]
- Wolk, A. Potential health hazards of eating red meat. J. Intern. Med. 2017, 281, 106–122. [Google Scholar] [CrossRef] [PubMed]
- Whelton, P.K. Sodium and Potassium Intake in US Adults. Circulation 2018, 137, 247–249. [Google Scholar] [CrossRef]
- Forrest, K.Y.; Stuhldreher, W.L. Prevalence and correlates of vitamin D deficiency in US adults. Nutr. Res. 2011, 31, 48–54. [Google Scholar] [CrossRef]
- Pilz, S.; Marz, W.; Cashman, K.D.; Kiely, M.E.; Whiting, S.J.; Holick, M.F.; Grant, W.B.; Pludowski, P.; Hiligsmann, M.; Trummer, C.; et al. Rationale and Plan for Vitamin D Food Fortification: A Review and Guidance Paper. Front. Endocrinol. 2018, 9, 373. [Google Scholar] [CrossRef]
- Bordelon, P.; Ghetu, M.V.; Langan, R.C. Recognition and management of vitamin D deficiency. Am. Fam. Physician 2009, 80, 841–846. [Google Scholar]
- Resnik, D. Trans fat bans and human freedom. Am. J. Bioeth. 2010, 10, 27–32. [Google Scholar] [CrossRef]
- Wanders, A.J.; Zock, P.L.; Brouwer, I.A. Trans Fat Intake and Its Dietary Sources in General Populations Worldwide: A Systematic Review. Nutrients 2017, 9, 840. [Google Scholar] [CrossRef] [PubMed]
- Noel, S.E.; Newby, P.K.; Ordovas, J.M.; Tucker, K.L. Adherence to an (n-3) fatty acid/fish intake pattern is inversely associated with metabolic syndrome among Puerto Rican adults in the Greater Boston area. J. Nutr. 2010, 140, 1846–1854. [Google Scholar] [CrossRef] [PubMed]
- Bigornia, S.J.; Scott, T.M.; Harris, W.S.; Tucker, K.L. Prospective Associations of Erythrocyte Composition and Dietary Intake of n-3 and n-6 PUFA with Measures of Cognitive Function. Nutrients 2018, 10, 1253. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.D.; Leung, C.W.; Li, Y.; Ding, E.L.; Chiuve, S.E.; Hu, F.B.; Willett, W.C. Trends in dietary quality among adults in the United States, 1999 through 2010. JAMA Intern. Med. 2014, 174, 1587–1595. [Google Scholar] [CrossRef] [PubMed]
- Cohn, D.; Patten, E.; Lopez, M.H. Puerto Rican Population Declines on Island, Grows on U.S. Mainland. Pew Research Center. 2014. Available online: https://www.pewhispanic.org/2014/08/11/puerto-rican-population-declines-on-island-grows-on-u-s-mainland/ (accessed on 13 May 2019).
- Thompson, B. Impact of the Financial and Economic Crisis on Nutrition—Policy and Programme Responses. FAO: Nutrition and Consumer Protection Division. 2019. Available online: http://www.fao.org/ag/agn/nutrition/docs/Impact%20of%20the%20financial%20and%20economic%20crisis%20on%20nutrition.pdf (accessed on 13 May 2019).
- Mattei, J.; McClain, A.C.; Falcon, L.M.; Noel, S.E.; Tucker, K.L. Dietary Acculturation among Puerto Rican Adults Varies by Acculturation Construct and Dietary Measure. J. Nutr. 2018, 148, 1804–1813. [Google Scholar] [CrossRef] [Green Version]
- Mattei, J.; Tamez, M.; Rios-Bedoya, C.F.; Xiao, R.S.; Tucker, K.L.; Rodriguez-Orengo, J.F. Health conditions and lifestyle risk factors of adults living in Puerto Rico: A cross-sectional study. BMC Public Health 2018, 18, 491. [Google Scholar] [CrossRef] [PubMed]
- Colon-Ramos, U.; Finney Rutten, L.J.; Moser, R.P.; Colon-Lopez, V.; Ortiz, A.P.; Yaroch, A.L. The association between fruit and vegetable intake, knowledge of the recommendations, and health information seeking within adults in the U.S. mainland and in Puerto Rico. J. Health Commun. 2015, 20, 105–111. [Google Scholar] [CrossRef]
- Centers for Disease C & Prevention Needs assessment following hurricane Georges—Dominican Republic, 1998. MMWR Morb. Mortal. Wkly. Rep. 1999, 48, 93–95.
- Rose, D.; Bodor, J.N.; Rice, J.C.; Swalm, C.M.; Hutchinson, P.L. The effects of Hurricane Katrina on food access disparities in New Orleans. Am. J. Public Health 2011, 101, 482–484. [Google Scholar] [CrossRef]
- Ziebarth, D.; Healy-Haney, N.; Gnadt, B.; Cronin, L.; Jones, B.; Jensen, E.; Viscuso, M. A community-based family intervention program to improve obesity in Hispanic families. WMJ 2012, 111, 261–266. [Google Scholar]
- Carbone, E.T.; Zoellner, J.M. Nutrition and health literacy: A systematic review to inform nutrition research and practice. J. Acad. Nutr. Diet. 2012, 112, 254–265. [Google Scholar] [CrossRef] [PubMed]
- Everyone Has a Role in Supporting Healthy Eating Patterns. The Social-Ecological Model. Dietary Guidelines 2015–2020. Available online: https://health.gov/dietaryguidelines/2015/guidelines/chapter-3/social-ecological-model/ (accessed on 13 May 2019).



{kind=link}
{kind=link}
| Dietary Intake a | Overall b | Sex c | Age d | |||
|---|---|---|---|---|---|---|
| (n = 248) | Men (n = 77) | Women (n = 171) | 30–45 y (n = 68) | 46–60 y (n = 125) | 61–75 y (n = 55) | |
| Total energy, kcal/d | 2228 (940) | 2388 (109) * | 2117 (75) | 2440 (118) | 2293 (84) | 2026 (132) |
| Percent from total energy | ||||||
| Carbohydrate % | 53.4 (7.4) | 54.0 (0.9) | 53.7 (0.6) | 53.4 (0.9) | 52.7 (0.7) | 55.5 (1.1) |
| Protein % | 15.1 (2.8) | 14.6 (0.3) | 15.1 (0.2) | 14.8 (0.3) | 15.3 (0.2) | 14.5 (0.4) |
| Fat % | 30.9 (5.9) | 30.5 (0.7) | 30.7 (0.5) | 30.8 (0.7) | 31.3 (0.5) | 29.7 (0.8) |
| Alcohol % e | 0.7 (2.1) | 1.0 (0.3) | 0.5 (0.2) | 1.0 (0.3) | 0.7 (0.2) | 0.5 (0.3) |
| Total carbohydrate, g/d | 299 (43) | 302 (5.0) | 301 (3.5) | 301 (5.4) | 296 (3.9) | 308 (6.1) |
| Dietary fiber | 24.1 (7.7) | 24.1 (0.9) | 24.5 (0.6) | 22.0 (0.9) ** | 23.9 (0.7) | 27.2 (1.1) |
| Starch | 106 (25) | 107 (3) | 107 (2) | 108 (3) | 103 (2) | 109(4) |
| Added sugar | 75.0 (35.8) | 76.5 (4.2) | 74.8 (2.9) | 79.4 (4.6) | 73.9 (3.3) | 73.7 (5.1) |
| Starch to total fiber ratio | 4.7 (1.6) | 4.7 (0.2) | 4.7 (0.1) | 5.2 (0.2) ** | 4.6 (0.1) | 4.3 (0.2) |
| Total protein, g/d | 85.5 (16.2) | 83.5 (1.9) | 85.1 (1.3) | 84.0 (2.0) | 87.0 (1.5) | 82.0 (2.3) |
| Vegetable protein | 27.2 (6.6) | 26.9 (0.8) | 27.6 (0.5) | 26.8 (0.8) | 26.6 (0.6) | 28.4 (0.9) |
| Animal protein | 51.3 (16.0) | 49.0 (1.9) | 51.0 (1.3) | 49.8 (2.0) | 53.1 (1.4) | 47.0 (2.3) |
| Total fat, g/d | 79.5 (14.5) | 78.1 (1.7) | 79.7 (1.2) | 78.0 (1.8) | 80.2 (1.3) | 78.5 (2.1) |
| Monounsaturated fatty acids | 26.3 (5.4) | 25.6 (0.6) | 26.4 (0.4) | 25.3 (0.7) | 26.6 (0.5) | 26.2 (0.8) |
| Polyunsaturated fatty acids | 15.8 (4.4) | 15.5 (0.5) | 15.8 (0.4) | 16.0 (0.6) | 15.9 (0.4) | 15.1 (0.6) |
| Omega-3 fatty acids | 1.7 (0.6) | 1.7 (0.1) | 1.7 (0.0) | 1.7 (0.1) | 1.8 (0.1) | 1.6 (0.1) |
| Saturated fatty acids | 23.0 (5.7) | 22.5 (0.7) | 23.3 (0.5) | 22.6 (0.7) | 23.2 (0.5) | 22.6 (0.8) |
| Trans fatty acids | 2.8 (1.0) | 2.7 (0.1) | 2.7 (0.1) | 2.8 (0.1) | 2.8 (0.1) | 2.5 (0.1) |
| Cholesterol, mg/d | 355.7 (202.3) | 366.7 (23.7) | 339.7 (16.3) | 335.5 (25.6) | 380.7 (18.3) | 343.3 (28.8) |
| Total alcohol e, g/d | 2.6 (10.7) | 4.2 (1.3) | 1.7 (0.9) | 4.1 (1.4) | 3.1 (1.0) | 1.7 (1.7) |
| Caffeine, g/d | 132.4 (138.9) | 140.0 (16.4) | 131.6 (11.3) | 128.7 (17.9) | 131.6 (12.7) | 147.0 (19.9) |
| Vitamin D, mcg/d | 4.7 (2.6) | 4.1 (0.3) | 4.8 (0.2) | 4.1 (0.3) | 4.9 (0.2) | 4.3 (0.4) |
| Vitamin B12, mcg/d | 9.7 (8.2) | 8.8 (1.0) | 9.4 (0.7) | 10.2 (1.0) * | 10.3 (0.7) | 7.0 (1.2) |
| Vitamin B6, mg/d | 2.3 (1.1) | 2.4 (0.1) | 2.3 (0.1) | 2.2 (0.1) | 2.4 (0.1) | 2.4 (0.2) |
| Folate, mcg/d | 453 (128) | 440 (15) | 461 (10) | 441 (16) | 449 (12) | 462 (18) |
| Calcium, mg/d | 954 (295) | 911 (35) | 973 (24) | 912 (37) | 951 (27) | 963 (42) |
| Magnesium, mg/d | 317 (70) | 309 (8) | 322 (6) | 296 (9) * | 316 (6) | 334 (10) |
| Iron, mg/d | 15.5 (3.5) | 14.6 (0.4) * | 15.6 (0.3) | 15.3 (0.4) | 15.5 (0.3) | 14.6 (0.5) |
| Sodium, mg/d | 3754 (790) | 3701 (93) | 3762 (64) | 3780 (100) | 3752 (72) | 3665 (113) |
| Potassium, mg/d | 3366 (810) | 3388 (93) | 3399 (64) | 3149 (101) ** | 3356 (72) | 3675 (114) |
| Dietary Intake a | Overall | Sex | Age | |||
|---|---|---|---|---|---|---|
| (n = 248) | Men (n = 77) | Women (n = 171) | 30–45 y (n = 68) | 46–60 y (n = 125) | 61–75 y (n = 55) | |
| Vitamin D, mcg/d | 3.6 | 1.3 | 4.7 | 1.5 | 6.4 | 0 |
| Vitamin B12, mcg/d | 94.8 | 96.1 | 98.3 | 98.5 | 99.2 | 92.7 * |
| Vitamin B6, mg/d | 99.2 | 97.4 | 100 | 100 | 98.4 | 100 |
| Folate, mcg/d | 90.3 | 88.3 | 91.2 | 92.7 | 92.0 | 83.6 |
| Calcium, mg/d | 55.7 | 62.3 | 52.6 | 70.6 | 51.2 | 47.3 * |
| Magnesium, mg/d | 60.5 | 19.5 | 79.9 *** | 58.8 | 59.2 | 65.5 |
| Potassium, mg/d | 6.9 | 7.8 | 6.4 | 0 | 7.2 | 14.6 ** |
| Food Group | % of Daily Energy Intake a | Servings/Day a | Sample Foods Included in the Food Group Category |
|---|---|---|---|
| All sugary beverages | 11.79 (9.43) | 2.32 (2.13) | Includes juices, sodas and other sugary beverages |
| Juices | 7.93 (8.10) | 1.48 (1.62) | Fruit drinks (Sunny Delight, Kool-Aid), fruit juices, tomato or vegetable juice, and nectars |
| Sodas and other sugary beverages | 3.85 (4.71) | 0.84 (1.11) | Presweetened coffee or tea, sodas (cola, 7-up, ginger ale), sport drinks (Gatorade, Powerade), energy drinks (Red Bull), chocolate milk (whole, fat free, low fat, soy) |
| Sweets and desserts | 10.21 (6.79) | 3.89 (2.99) | Cakes, brownies, pies, sorbets, ice cream, candy, chocolate, cookies, honey, jelly |
| Dairy | 8.49 (6.23) | 1.82 (1.54) | Cheese, sour cream, milk (soy, low fat, whole, nonfat), yogurt (whole, nonfat, low fat) |
| Mixed dishes | 7.62 (5.83) | 0.87 (0.83) | Mixed dishes and soups |
| Mixed dishes | 5.40 (4.07) | 0.43 (0.38) | Enchiladas, tamales, quesadillas, burritos, pot pies, empanadas, rice mixed dishes |
| Soups | 2.22 (3.21) | 0.44 (0.58) | Vegetables soups, clam chowder, chicken or beef broths |
| Starchy vegetables | 6.25 (6.29) | 1.10 (1.38) | Plantains, potatoes, and sweet potatoes |
| Potatoes | 3.69 (4.38) | 0.71 (1.01) | Baked or boiled potatoes, mashed potatoes; excluding French fries |
| Plantains | 1.42 (1.92) | 0.14 (0.18) | Plantains and green bananas, including pasteles |
| Sweet potato | 1.14 (1.82) | 0.25 (0.42) | Boiled or baked sweet potatoes |
| Fast foods | 5.50 (5.02) | 0.44 (0.47) | Hamburgers (Burger King, McDonalds), French fries, pizza (Pizza Hut), tacos (Taco Bell) |
| Rice | 4.86 (4.26) | 0.53 (0.49) | Brown and white rice |
| Fats | 4.15 (2.52) | 0.87 (0.57) | Butter, margarine, lard, mayonnaise, and dressings |
| Refined grains | 4.13 (3.26) | 0.57 (0.47) | Ready-to-eat cereals (e.g., Froot Loops, Cheerios, Corn Pops, Corn Flakes), grits, white bread, flour tortilla, bagels, waffles, pancakes, cornbread |
| Fruit | 3.85 (3.90) | 1.13 (1.08) | Fresh, frozen, dried, and canned fruits |
| All vegetables | 3.81 (3.29) | 3.34 (2.56) | Yellow, green, and other vegetables, tomatoes |
| Yellow vegetables | 0.59 (1.05) | 0.31 (0.43) | Raw, cooked, and canned yellow vegetables (e.g., carrots, pumpkin, squash) |
| Green vegetables | 0.40 (0.56) | 0.40 (0.46) | Raw, cooked, and canned dark-green vegetables (e.g., broccoli, spinach, romaine, collards) |
| Tomatoes | 0.35 (0.33) | 0.44 (0.42) | Raw, cooked, and canned tomato, tomato sauce, tomato puree, tomato paste, tomato-based sauce, excluding ketchup |
| Other vegetables | 2.46 (2.14) | 2.20 (1.79) | Raw, cooked, and canned vegetables (e.g., corn, peppers, cucumber, radish, onion, mushrooms, eggplant) |
| Processed meats | 3.64 (3.10) | 0.72 (0.82) | Lunchmeats, sausages, ham, bacon |
| Eggs | 3.59 (3.94) | 0.66 (0.80) | Boiled, scrambled, and whole eggs, including egg substitutes (e.g., Egg Beaters) |
| Whole grains | 3.54 (3.09) | 0.53 (0.47) | Corn tortilla, oats, whole wheat bread, whole wheat pasta, whole grain cereals (100% Bran, Oat Bran Flakes, All-Bran Wheat Flakes, granola) |
| Legumes | 3.14 (2.81) | 0.63 (0.58) | Pinto, black, kidney, lima beans, chickpeas, green peas |
| Poultry | 2.92 (2.68) | 0.32 (0.28) | Turkey, chicken (breast, leg) |
| Fish and seafood | 2.28 (2.95) | 0.37 (0.48) | Cod, salmon, sardines, haddock, tuna, catfish (cooked from fresh or frozen), clams, crab, scallops, lobster, oyster |
| Snacks | 2.25 (2.83) | 0.41 (0.70) | Crackers, popcorn, chips, pretzels |
| Red meats | 2.22 (2.27) | 0.28 (0.35) | Beef of ground beef, pork, lamb, organs |
| Pasta | 2.12 (2.53) | 0.21 (0.24) | Lasagna, spaghetti, noodles |
| Oils | 2.06 (2.08) | 0.34 (0.34) | Canola, corn, olive, sesame, or soybean oils |
| Nuts | 1.31 (2.40) | 0.23 (0.46) | Almonds, cashews, peanuts, pecans, pine nuts, sunflower seeds, walnuts, pistachios, peanut butter |
| Alcohol | 0.86 (2.49) | 0.24 (0.89) | Beer, liquor, wine |
| Artificial-sweetened beverages | 0.80 (3.09) | 0.13 (0.43) | Diet sodas, low-calorie milkshakes (e.g., Slim-Fast) |
| Spices and condiments | 0.55 (0.55) | 3.03 (2.29) | Pickles, horseradish, hot pepper, hot sauce, vinegar, oregano, paprika, turmeric, cumin, Italian seasoning, chili powder, cinnamon, mustard |
| Unsweetened beverages | 0.17 (0.19) | 1.41 (1.49) | Unsweetened tea, coffee |
| Salt | 0.00 (0.00) | 0.47 (0.41) | Salt |
| Water | 0.00 (0.00) | 3.90 (3.40) | Bottled or tap water, sparkling water |
| Overall a | Sex a | Age a | ||||
|---|---|---|---|---|---|---|
| n = 248 | Men (n = 77) | Women (n = 171) | 30–45 y (n = 68) | 46–60 y (n = 125) | 61–75 y (n = 55) | |
| Total AHEI score | 59.8 (11.0) | 59.4 (10.7) | 60.0 (11.2) | 58.0 (11.0) | 59.7 (11.0) | 62.3 (10.9) |
| Vegetable score | 6.3 (2.9) | 6.4 (2.9) | 6.2 (3.0) | 5.8 (2.7) | 6.3 (2.9) | 6.9 (3.2) |
| Whole fruit score | 2.9 (2.6) | 2.8 (2.2) | 3.0 (2.6) | 2.2 (2.2) | 2.9 (2.4) | 3.9 (2.3) ** |
| Whole grains score | 5.3 (3.5) | 4.7 (3.6) | 5.5 (3.4) | 4.8 (3.5) | 5.3 (3.5) | 5.8 (3.5) |
| Sugary beverages and fruit juice score | 1.4 (2.6) | 1.3 (2.6) | 1.4 (2.7) | 1.5 (2.9) | 1.2 (2.4) | 1.7 (2.9) |
| Nuts and legumes score | 6.4 (3.2) | 6.5 (3.0) | 6.3 (3.3) | 6.8 (2.8) | 6.2 (3.3) | 6.2 (3.4) |
| Red/processed meat score | 4.9 (3.5) | 4.6 (3.7) | 5.0 (3.4) | 4.0 (3.4) | 4.9 (3.5) | 6.0 (3.4) ** |
| Trans fat score | 7.9 (1.3) | 7.9 (1.2) | 7.9 (1.4) | 7.9 (1.1) | 7.8 (1.4) | 8.2 (1.3) |
| Omega-3 fatty acids score | 7.2 (3.3) | 7.3 (3.4) | 7.2 (3.3) | 7.2 (3.3) | 7.4 (3.4) | 6.8 (3.2) |
| Polyunsaturated fatty acids (PUFA) score | 6.1 (2.2) | 6.1 (2.3) | 6.1 (2.2) | 6.3 (1.7) | 6.1 (2.4) | 5.8 (2.3) |
| Sodium score | 5.2 (3.3) | 4.8 (3.4) | 5.4 (3.2) | 5.1 (3.4) | 5.4 (3.2) | 5.0 (3.3) |
| Alcohol score | 6.2 (1.8) | 7.2 (1.7) | 5.8 (6.1) *** | 6.5 (2.1) | 6.3 (1.8) | 5.9 (1.3) |
| Vegetable b, serv/d | 3.7 (2.6) | 3.9 (2.8) | 3.6 (2.5) | 3.0 (1.7) | 3.7 (2.8) | 4.4 (3.0) * |
| Whole fruit b, serv/d | 1.2 (1.1) | 1.1 (1.1) | 1.2 (1.1) | 0.90 (0.92) | 1.2 (1.0) | 1.6 (1.4) ** |
| Whole grains b, g/d | 52.2 (50.5) | 51.3 (54.1) | 52.6 (49.0) | 40.8 (33.1) | 52.5 (49.2) | 65.6 (66.4) * |
| SSB, fruit juice b, serv/d | 2.2 (2.1) | 2.5 (2.4) | 2.0 (1.9) | 2.3 (2.2) | 2.3 (2.2) | 1.8 (1.6) |
| Nuts and legumes b, serv/d | 0.85 (0.73) | 0.80 (0.64) | 0.88 (0.77) | 0.93 (0.80) | 0.85 (0.76) | 0.77 (0.54) |
| Red/processed meat b, serv/d | 0.98 (0.99) | 1.1 (1.0) | 0.95 (0.96) | 1.2 (1.2) | 0.98 (0.95) | 0.68 (0.73) ** |
| Trans fat, % of energy | 1.2 (0.5) | 1.2 (0.4) | 1.2 (0.5) | 1.3 (0.4) | 1.3 (0.5) | 1.1 (0.5) |
| Omega-3 fatty acids, mg/d | 330 (331) | 331 (312) | 331 (340) | 274 (222) | 392 (396) | 261 (250) * |
| PUFA, % of energy | 7.0 (2.0) | 6.9 (2.0) | 7.0 (2.0) | 7.1 (1.6) | 7.0 (2.1) | 6.7 (2.0) |
| Sodium, mg/d | 4097 (1978) | 4416 (2245) | 3954 (1834) | 4429 (2265) | 4146 (1882) | 3579 (1727) |
| Alcohol b, drinks/d | 0.24 (0.89) | 0.38 (1.4) | 0.18 (0.50) | 0.35 (1.1) | 0.24 (0.95) | 0.10 (0.34) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mattei, J.; Tamez, M.; Bigornia, S.J.; Noel, S.E.; Xiao, R.S.; Ríos-Bedoya, C.F.; Rodríguez-Orengo, J.F.; Tucker, K.L. Dietary Intake and Its Determinants Among Adults Living in the Metropolitan Area of Puerto Rico. Nutrients 2019, 11, 1598. https://doi.org/10.3390/nu11071598
Mattei J, Tamez M, Bigornia SJ, Noel SE, Xiao RS, Ríos-Bedoya CF, Rodríguez-Orengo JF, Tucker KL. Dietary Intake and Its Determinants Among Adults Living in the Metropolitan Area of Puerto Rico. Nutrients. 2019; 11(7):1598. https://doi.org/10.3390/nu11071598
Chicago/Turabian StyleMattei, Josiemer, Martha Tamez, Sherman J. Bigornia, Sabrina E. Noel, Rui S. Xiao, Carlos F. Ríos-Bedoya, José F. Rodríguez-Orengo, and Katherine L. Tucker. 2019. "Dietary Intake and Its Determinants Among Adults Living in the Metropolitan Area of Puerto Rico" Nutrients 11, no. 7: 1598. https://doi.org/10.3390/nu11071598