Dietary Patterns, Cardiorespiratory and Muscular Fitness in 9–11-Year-Old Children from Dunedin, New Zealand

 , ,
, ,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
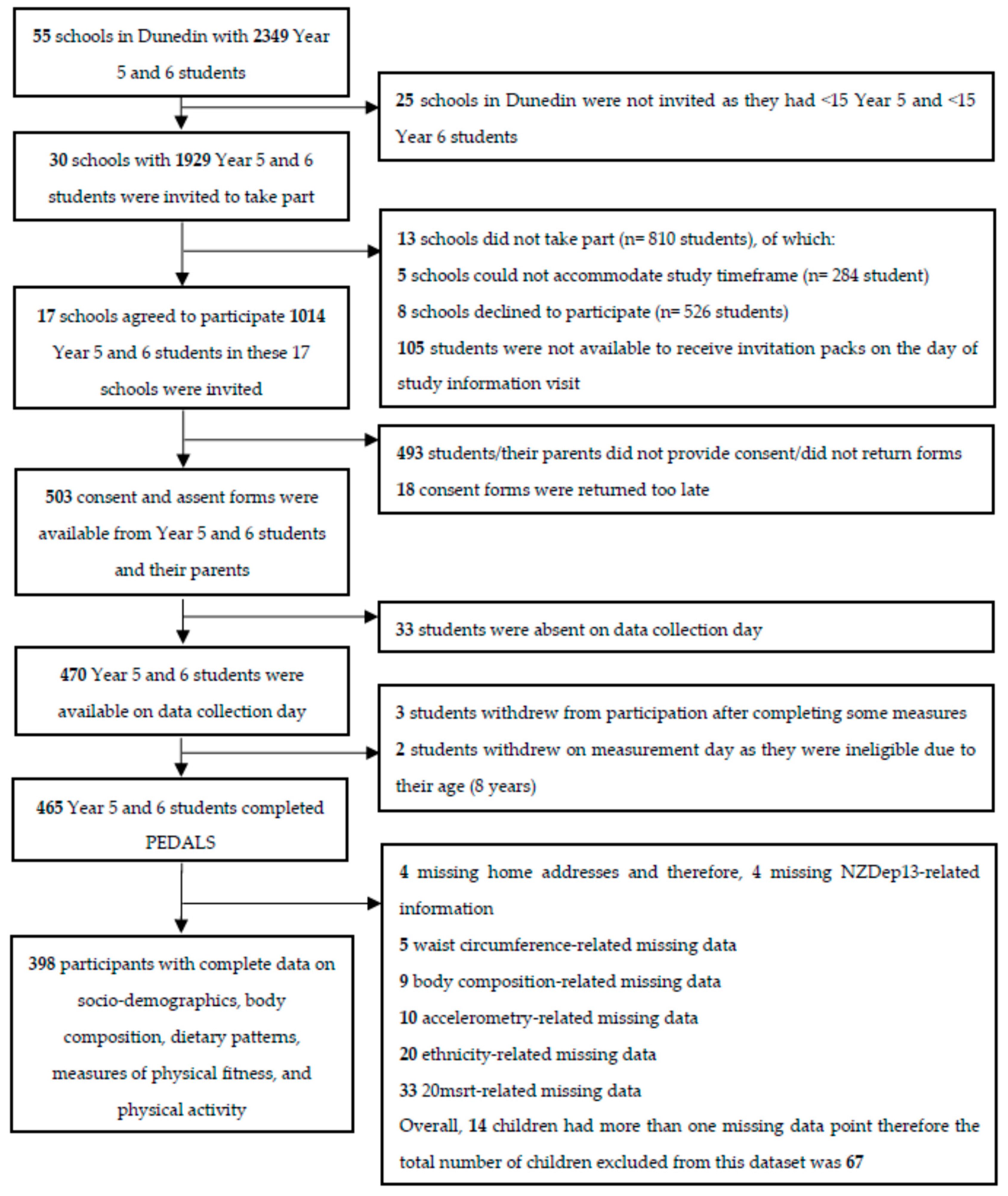
2.1. Study Design and Participants
2.2. Study Measurements
Cardiorespiratory Fitness (CRF)
2.3. Muscular Fitness
2.3.1. Dietary Intake
2.3.2. Assessment of Covariates
2.4. Sample Size
2.5. Statistical Analyses
3. Results
3.1. Characteristics of Participants
3.2. Dietary Intake and Identification of Dietary Patterns
3.3. Bivariable Predictors of CRF and Muscular Fitness
3.4. Independent Relationship Between Dietary Pattern Scores with CRF and Muscular Fitness
4. Discussion
4.1. Relationships between Dietary Patterns and CRF
4.2. Relationships between Dietary Patterns and Muscular Fitness
4.3. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organisation (WHO). Cardiovascular Disease; WHO: Geneva, Switzerland, 2016; Available online: http://www.who.int/cardiovascular_diseases/en/ (accessed on 1 February 2018).
- Bridger, T. Childhood obesity and cardiovascular disease. Paediatr. Child Health 2009, 14, 177–182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kehoe, S.H.; Krishnaveni, G.V.; Veena, S.R.; Guntupalli, A.M.; Margetts, B.M.; Fall, C.H.D.; Robinson, S.M. Diet patterns are associated with demographic factors and nutritional status in South Indian children. Matern. Child. Nutr. 2014, 10, 145–158. [Google Scholar] [CrossRef] [PubMed]
- Ruiz, J.R.; Ortega, F.B.; Meusel, D.; Harro, M.; Oja, P.; Sjöström, M. Cardiorespiratory fitness is associated with features of metabolic risk factors in children. Should cardiorespiratory fitness be assessed in a European health monitoring system? The European Youth Heart Study. J. Public Health 2006, 14, 94–102. [Google Scholar] [CrossRef]
- Benson, A.C.; Torode, M.E.; Singh, M.A.F. Muscular strength and cardiorespiratory fitness is associated with higher insulin sensitivity in children and adolescents. Int. J. Pediatr. Obes. IJPO Off. J. Int. Assoc. Study Obes. 2006, 1, 222–231. [Google Scholar] [CrossRef]
- Muros, J.J.; Cofre-Bolados, C.; Arriscado, D.; Zurita, F.; Knox, E. Mediterranean diet adherence is associated with lifestyle, physical fitness, and mental wellness among 10-y-olds in Chile. Nutrition 2017, 35, 87–92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zaqout, M.; Vyncke, K.; Moreno, L.A.; De Miguel-Etayo, P.; Lauria, F.; Molnar, D.; Lissner, L.; Hunsberger, M.; Veidebaum, T.; Tornaritis, M.; et al. Determinant factors of physical fitness in European children. Int. J. Public Health 2016, 61, 573–582. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arriscado, D.; Muros, J.J.; Zabala, M.; Dalmau, J.M. Factors associated with low adherence to a Mediterranean diet in healthy children in northern Spain. Appetite 2014, 80, 28–34. [Google Scholar] [CrossRef] [PubMed]
- Grao-Cruces, A.; Fernández-Martínez, A.; Nuviala, A. Association of fitness with life satisfaction, health risk behaviors, and adherence to the Mediterranean diet in Spanish adolescents. J. Strength Cond. Res. 2014, 28, 2164–2172. [Google Scholar] [CrossRef] [PubMed]
- Howe, A.S.; Skidmore, P.M.; Parnell, W.R.; Wong, J.E.; Lubransky, A.C.; Black, K.E. Cardiorespiratory fitness is positively associated with a healthy dietary pattern in New Zealand adolescents. Public Health Nutr. 2016, 19, 1279–1287. [Google Scholar] [CrossRef] [PubMed]
- Neville, C.E.; McKinley, M.C.; Murray, L.J.; Boreham, C.A.; Woodside, J.V.; Young Hearts Study Group. Fruit and vegetable consumption and muscle strength and power during adolescence: A cross-sectional analysis of the Northern Ireland Young Hearts Project 1999–2001. J. Musculoskelet. Neuronal. Interact. 2014, 14, 367–376. [Google Scholar] [PubMed]
- Yavari, A.; Javadi, M.; Mirmiran, P.; Bahadoran, Z. Exercise-Induced Oxidative Stress and Dietary Antoxidative. Asian J. Sports Med. 2015, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goswami, B.; Roy, A.S.; Dalui, R.; Bandyopadhyay, A. Impact of Pubertal Growth on Physical Fitness. Am. J. Sports Sci. Med. 2014, 2, 34–39. [Google Scholar] [CrossRef] [Green Version]
- Institute of Medicine (US) and National Research Council (US) Committee on the Science of Adolescence. The Psychology of Adolescence; The Science of Adolescent Risk-Taking; National Academies Press: Washington, DC, USA, 2011. Available online: https://www.ncbi.nlm.nih.gov/books/NBK53420/ (accessed on 23 March 2018).
- Léger, L.A.; Mercier, D.; Gadoury, C.; Lambert, J. The multistage 20 metre shuttle run test for aerobic fitness. J. Sports Sci. 1988, 6, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Matsuzaka, A.; Takahashi, Y.; Yamazoe, M.; Kumakura, N.; Ikeda, A.; Wilk, B.; Bar-Or, O. Validity of the Multistage 20-M Shuttle-Run Test for Japanese Children, Adolescents, and Adults. Pediatr. Exerc. Sci. 2004, 16, 113–125. [Google Scholar] [CrossRef]
- The Cooper Institute. FITNESSGRAM Test Administration Manual, 3rd ed.; Human Kinetics: Champaign, IL, USA, 2004. [Google Scholar]
- Artero, E.G.; España-Romero, V.; Castro-Piñero, J.; Ortega, F.B.; Suni, J.; Castillo-Garzon, M.J.; Ruiz, J.R. Reliability of Field-Based Fitness Tests in Youth. Int. J. Sports Med. 2011, 32, 159–169. [Google Scholar] [CrossRef] [PubMed]
- Castro-Piñero, J.; Artero, E.G.; España-Romero, V.; Ortega, F.B.; Sjöström, M.; Suni, J.; Ruiz, J.R. Criterion-related validity of field-based fitness tests in youth: A systematic review. Br. J. Sports Med. 2010, 44, 934–943. [Google Scholar] [CrossRef] [PubMed]
- Saeedi, P.; Skeaff, S.; Wong, J.; Skidmore, P. Reproducibility and relative validity of a short food frequency questionnaire in 9–10 year-old children. Nutrients 2016, 8, 271. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health (MOH). Ethnicity Data Protocols for the Health and Disability Sector; MOH: Wellington, New Zealand, 2004. Available online: http://www.health.govt.nz/publication/ethnicity-data-protocols-health-and-disability-sector (accessed on 10 March 2018).
- Atkinson, J.; Salmond, C.; Crampton, P. NZDep2013 Index of Deprivation User’s Manual; Department of Public Health, University of Otago: Wellington, New Zealand, 2014. [Google Scholar]
- Cole, T.J.; Lobstein, T. Extended international (IOTF) body mass index cut-offs for thinness, overweight and obesity. Pediatr. Obes. 2012, 7, 284–294. [Google Scholar] [CrossRef] [PubMed]
- Reilly, J.J.; Penpraze, V.; Hislop, J.; Davies, G.; Grant, S.; Paton, J.Y. Objective measurement of physical activity and sedentary behaviour: Review with new data. Arch. Dis. Child. 2008, 93, 614–619. [Google Scholar] [CrossRef] [PubMed]
- Rich, C.; Geraci, M.; Griffiths, L.; Sera, F.; Dezateux, C.; Cortina-Borja, M. Quality Control Methods in Accelerometer Data Processing: Defining Minimum Wear Time. PLoS ONE 2013, 8, e67206. [Google Scholar] [CrossRef] [PubMed]
- Chandler, J.L.; Brazendale, K.; Beets, M.W.; Mealing, B.A. Classification of physical activity intensities using a wrist-worn accelerometer in 8-12-year-old children. Pediatr. Obes. 2016, 11, 120–127. [Google Scholar] [CrossRef] [PubMed]
- Carlin, J.B.; Hocking, J. Design of cross-sectional surveys using cluster sampling: An overview with Australian case studies. Aust. N. Z. J. Public Health 1999, 23, 546–551. [Google Scholar] [CrossRef] [PubMed]
- Davison, B.; Saeedi, P.; Black, K.; Harrex, H.; Haszard, J.; Meredith-Jones, K.; Quigg, R.; Skeaff, S.; Stoner, L.; Wong, J.; et al. The Association between Parent Diet Quality and Child Dietary Patterns in Nine- to Eleven-Year-Old Children from Dunedin, New Zealand. Nutrients 2017, 9, 483. [Google Scholar] [CrossRef] [PubMed]
- Hardy, L.L.; King, L.; Hector, D.; Baur, L.A. Socio-cultural differences in Australian primary school children’s weight and weight-related behaviours: Socio-cultural differences in child BMI. J. Paediatr. Child Health 2013, 49, 641–648. [Google Scholar] [CrossRef] [PubMed]
- Jiménez Pavón, D.; Ortega, F.P.; Ruiz, J.R.; España Romero, V.; García Artero, E.; Moliner Urdiales, D.; Gómez Martínez, S.; Vicente Rodríguez, G.; Manios, Y.; Béghin, L.; et al. HELENA Study Group Socioeconomic status influences physical fitness in European adolescents independently of body fat and physical activity: The HELENA study. Nutr. Hosp. 2010, 25, 311–316. [Google Scholar] [CrossRef] [PubMed]
- Gonçalves, E.C.A.; Silva, D.A.S. Factors associated with low levels of aerobic fitness among adolescents. Rev. Paul. Pediatr. Engl. Ed. 2016, 34, 141–147. [Google Scholar] [CrossRef] [PubMed]
- Mota, J.; Guerra, S.; Leandro, C.; Pinto, A.; Ribeiro, J.C.; Duarte, J.A. Association of maturation, sex, and body fat in cardiorespiratory fitness. Am. J. Hum. Biol. Off. J. Hum. Biol. Counc. 2002, 14, 707–712. [Google Scholar] [CrossRef] [PubMed]
- Tsiros, M.D.; Coates, A.M.; Howe, P.R.C.; Walkley, J.; Hills, A.P.; Wood, R.E.; Buckley, J.D. Adiposity is related to decrements in cardiorespiratory fitness in obese and normal-weight children. Pediatr. Obes. 2016, 11, 144–150. [Google Scholar] [CrossRef] [PubMed]
- Pandey, A.; Park, B.D.; Ayers, C.; Das, S.R.; Lakoski, S.; Matulevicius, S.; de Lemos, J.A.; Berry, J.D. Determinants of Racial/Ethnic Differences in Cardiorespiratory Fitness (from the Dallas Heart Study). Am. J. Cardiol. 2016, 118, 499–503. [Google Scholar] [CrossRef] [PubMed]
- Jürimäe, T.; Hurbo, T.; Jürimäe, J. Relationship of handgrip strength with anthropometric and body composition variables in prepubertal children. Homo Int. Z. Vgl. Forsch. Am. Menschen 2009, 60, 225–238. [Google Scholar] [CrossRef] [PubMed]
- Leppänen, M.H.; Nyström, C.D.; Henriksson, P.; Pomeroy, J.; Ruiz, J.R.; Ortega, F.B.; Cadenas-Sánchez, C.; Löf, M. Physical activity intensity, sedentary behavior, body composition and physical fitness in 4-year-old children: Results from the ministop trial. Int. J. Obes. 2016, 40, 1126–1133. [Google Scholar] [CrossRef] [PubMed]
- Cashman, K.D. Diet, Nutrition, and Bone Health. J. Nutr. 2007, 137, 2507S–2512S. [Google Scholar] [CrossRef] [PubMed]
- Ortega, F.B.; Ruiz, J.R.; Castillo, M.J.; Sjöström, M. Physical fitness in childhood and adolescence: A powerful marker of health. Int. J. Obes. 2008, 32, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Bouchard, C.; Daw, E.W.; Rice, T.; Pérusse, L.; Gagnon, J.; Province, M.A.; Leon, A.S.; Rao, D.C.; Skinner, J.S.; Wilmore, J.H. Familial resemblance for VO2max in the sedentary state: The HERITAGE family study. Med. Sci. Sports Exerc. 1998, 30, 252–258. [Google Scholar] [CrossRef] [PubMed]
- Ruiz, J.R.; Rizzo, N.S.; Hurtig-Wennlöf, A.; Ortega, F.B.; Wärnberg, J.; Sjöström, M. Relations of total physical activity and intensity to fitness and fatness in children: The European Youth Heart Study. Am. J. Clin. Nutr. 2006, 84, 299–303. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health (MOH). Physical Activity; MOH: Wellington, New Zealand, 2015. Available online: http://www.health.govt.nz/our-work/preventative-health-wellness/physical-activity (accessed on 3 April 2018).
- Burns, R.; Hannon, J.C.; Brusseau, T.A.; Shultz, B.; Eisenman, P. Indices of Abdominal Adiposity and Cardiorespiratory Fitness Test Performance in Middle-School Students. J. Obes. 2013, 2013, 912460. [Google Scholar] [CrossRef] [PubMed]
- Ramírez-Vélez, R.; Daza, F.; González-Jiménez, E.; Schmidt-RioValle, J.; González-Ruíz, K.; Correa-Bautista, J.E. Cardiorespiratory Fitness, Adiposity, and Cardiometabolic Risk Factors in Schoolchildren: The FUPRECOL Study. West. J. Nurs. Res. 2017, 39, 1311–1329. [Google Scholar] [CrossRef] [PubMed]
- Albon, H.M.; Hamlin, M.J.; Ross, J.J. Secular trends and distributional changes in health and fitness performance variables of 10-14-year-old children in New Zealand between 1991 and 2003. Br. J. Sports Med. 2010, 44, 263–269. [Google Scholar] [CrossRef] [PubMed]
- Alkerwi, A.; Vernier, C.; Sauvageot, N.; Crichton, G.E.; Elias, M.F. Demographic and socioeconomic disparity in nutrition: Application of a novel Correlated Component Regression approach. BMJ Open 2015, 5, e006814. [Google Scholar] [CrossRef] [PubMed]
- Livingstone, M.B.E.; Robson, P.J. Measurement of dietary intake in children. Proc. Nutr. Soc. 2000, 59, 279–293. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Variable | n (%) | O2max, mL·kg−1·min−1 | Muscular Fitness, kg | ||
|---|---|---|---|---|---|
| Dominant Hand | |||||
| Mean ± SD | p Value | Mean ± SD | p Value | ||
| 48.7 ± 4.75 | - | 15.23 ± 3.29 | - | ||
| Sex | 0.002 | <0.001 | |||
| Boys | 198 (49.7) | 49.9 ± 5.18 | 16.0 ± 3.52 | ||
| Girls | 200 (50.3) | 47.6 ± 3.99 | 14.5 ± 2.88 | ||
| Ethnicity | 0.521 | 0.287 | |||
| Māori | 44 (11.1) | 48.4 ± 5.67 | 15.8 ± 3.39 | ||
| Non-Māori | 354 (88.9) | 48.8 ± 4.63 | 15.2 ± 3.28 | ||
| NZDep13 | 0.058 | 0.966 | |||
| Low deprivation | 175 (44.0) | 49.7 ± 5.11 | 15.3 ± 3.18 | ||
| Middle deprivation | 153 (38.4) | 48.5 ± 4.33 | 15.2 ± 3.31 | ||
| High deprivation | 70 (17.6) | 47.0 ± 4.13 | 15.2 ± 3.57 | ||
| BMI, kg·m−2 | <0.001 | 0.001 | |||
| Underweight-normal weight | 323 (81.2) | 49.5 ± 4.71 | 15.0 ± 3.19 | ||
| Overweight-obese | 75 (18.8) | 45.7 ± 3.59 | 16.3 ± 3.54 | ||
| β (95% CI) | p Value | β (95% CI) | p Value | ||
| BMI Z-score | −1.20 (−1.57, −0.83) | <0.001 | 0.96 (0.76, 1.16) | <0.001 | |
| FMI, kg·m−2 | −0.80 (−1.00, −0.60) | <0.001 | 0.24 (0.09, 0.39) | 0.002 | |
| FFMI, kg·m−2 | −0.47 (−0.80, −0.13) | 0.006 | 1.24 (0.98, 1.50) | <0.001 | |
| Moderate-vigorous physical activity, h | 0.02 (−0.07, 0.11) | 0.605 | 0.08 (−0.00, 0.17) | 0.062 | |
| Snacks score | −0.22 (−0.54, 0.10) | 0.179 | −0.02 (−0.36, 0.32) | 0.897 | |
| Fruit and Vegetables score | −0.04 (−0.41, 0.34) | 0.850 | 0.65 (0.30, 1.00) | <0.001 | |
| Age, year | −0.91 (−1.56, −0.27) | 0.005 | 1.35 (0.89, 1.81) | <0.001 | |
| Variable | Snacks | Fruit and Vegetables | ||||
|---|---|---|---|---|---|---|
| β | (95% CI) | p Value | β | (95% CI) | p Value | |
| O2max, mL·kg−1·min−1 | ||||||
| Model 1 | −0.33 | −0.69, 0.04 | 0.077 | 0.02 | −0.41, 0.46 | 0.913 |
| Model 2O2max | −0.22 | −0.49, 0.04 | 0.099 | 0.15 | −0.23, 0.53 | 0.430 |
| Muscular fitness (Dominant hand), kg | ||||||
| Model 1 | −0.17 | −0.45, 0.11 | 0.238 | 0.53 | 0.19, 0.88 | 0.003 |
| Model 2 Muscular fitness | −0.24 | −0.41, −0.06 | 0.007 | 0.31 | 0.02, 0.59 | 0.037 |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saeedi, P.; Black, K.E.; Haszard, J.J.; Skeaff, S.; Stoner, L.; Davidson, B.; Harrex, H.A.L.; Meredith-Jones, K.; Quigg, R.; Wong, J.E.; et al. Dietary Patterns, Cardiorespiratory and Muscular Fitness in 9–11-Year-Old Children from Dunedin, New Zealand. Nutrients 2018, 10, 887. https://doi.org/10.3390/nu10070887
Saeedi P, Black KE, Haszard JJ, Skeaff S, Stoner L, Davidson B, Harrex HAL, Meredith-Jones K, Quigg R, Wong JE, et al. Dietary Patterns, Cardiorespiratory and Muscular Fitness in 9–11-Year-Old Children from Dunedin, New Zealand. Nutrients. 2018; 10(7):887. https://doi.org/10.3390/nu10070887
Chicago/Turabian StyleSaeedi, Pouya, Katherine E. Black, Jillian J. Haszard, Sheila Skeaff, Lee Stoner, Brittany Davidson, Harriet A. L. Harrex, Kim Meredith-Jones, Robin Quigg, Jyh Eiin Wong, and et al. 2018. "Dietary Patterns, Cardiorespiratory and Muscular Fitness in 9–11-Year-Old Children from Dunedin, New Zealand" Nutrients 10, no. 7: 887. https://doi.org/10.3390/nu10070887