
Psychometric Properties of the Greek Version of the Medical Office on Patient Safety Culture in Primary Care Settings

Abstract
:1. Introduction
2. Methods
2.1. Data Source
2.2. Instrument
2.3. Translation Process
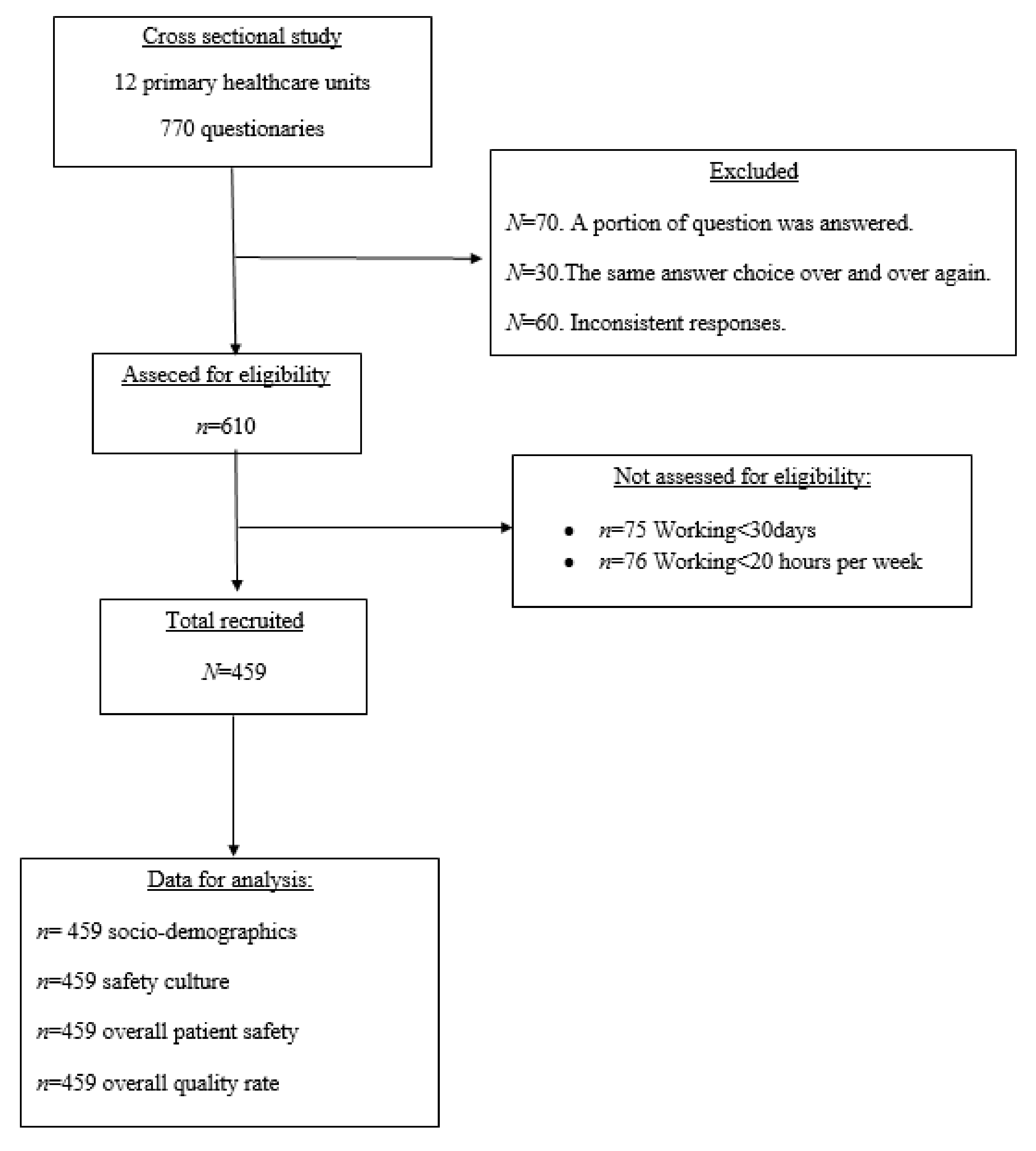
2.4. Sample
2.5. Statistical Analysis
2.6. Ethics
3. Results
3.1. Sample
3.2. Factor Analysis and Internal Consistency
3.3. Safety Culture Composite Measures and Overall Rating in Patient Safety and Quality
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AHRQ | agency of healthcare research and quality |
| MOSPSC | medical survey on patient safety culture |
| PHU | primary healthcare unit |
| G-MSOPSC | Greek version of medical survey on patient safety culture |
| SOPS | surveys on patient safety culture |
| PEDY | national primary health care network |
| FICT | free and informed consent term |
References
- Committee on Diagnostic Error in Health Care; Board on Health Care Services; Institute of Medicine; The National Academies of Sciences, Engineering, and Medicine; Balogh, E.P.; Miller, B.T.; Ball, J.R. Improving Diagnosis in Health Care; National Academies Press: Washington, DC, USA, 2015. Available online: https://www.ncbi.nlm.nih.gov/books/NBK338596 (accessed on 10 June 2017).
- Graber, M.L.; Franklin, N.; Gordon, R. Diagnostic Error in Internal Medicine. Arch. Intern. Med. 2005, 165, 1493–1499. [Google Scholar] [CrossRef] [PubMed]
- Schiff, G.D.; Hasan, O.; Kim, S.; Abrams, R.; Cosby, K.; Lambert, B.L.; Elstein, A.S.; Hasler, S.; Kabongo, M.L.; Krosnjar, N.; et al. Diagnostic Error in Medicine. Arch. Intern. Med. 2009, 169, 1881–1887. [Google Scholar] [CrossRef]
- Singh, H. Editorial: Helping Health Care Organizations to Define Diagnostic Errors as Missed Opportunities in Diagnosis. Jt. Comm. J. Qual. Patient Saf. 2014, 40, 99–101. [Google Scholar] [CrossRef]
- World Health Organization. Primary Health Care: Main Terminology. 2016. Available online: https://www.euro.who.int/en/health-topics/Health-systems/primary-health-care/main-terminology (accessed on 14 June 2016).
- Kostopoulou, O.; Delaney, B.C.; Munro, C.W. Diagnostic difficulty and error in primary care--a systematic review. Fam. Pract. 2008, 25, 400–413. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, H.; Sittig, D.F. Setting the record straight on measuring diagnostic errors. Reply to: ’Bad assumptions on primary care diagnostic errors’ by Dr Richard Young. BMJ Qual. Saf. 2015, 24, 345–348. [Google Scholar] [CrossRef] [PubMed]
- Goyder, C.R.; Jones, C.H.D.; Heneghan, C.J.; Thompson, M.J. Missed opportunities for diagnosis: Lessons learned from diagnostic errors in primary care. Br. J. Gen. Pract. 2015, 65, e838–e844. [Google Scholar] [CrossRef] [Green Version]
- Panesar, S.S.; de Silva, D.; Carson-Stevens, A.; Cresswell, K.M.; Salvilla, S.A.; Slight, S.P.; Javad, S.; Netuveli, G.; Larizgoitia, I.; Donaldson, L.J.; et al. How safe is primary care? A systematic review. BMJ Qual. Saf. 2015, 25, 544–553. [Google Scholar] [CrossRef] [Green Version]
- Ely, J.W.; Kaldjian, L.C.; D’Alessandro, D.M. Diagnostic Errors in Primary Care: Lessons Learned. J. Am. Board Fam. Med. 2012, 25, 87–97. [Google Scholar] [CrossRef]
- Gandhi, T.K.; Kachalia, A.; Thomas, E.J.; Puopolo, A.L.; Yoon, C.; Brennan, T.A.; Studdert, D.M. Missed and Delayed Diagnoses in the Ambulatory Setting: A Study of Closed Malpractice Claims. Ann. Intern. Med. 2006, 145, 488–496. [Google Scholar] [CrossRef]
- Silk, N. What Went Wrong in 1000 Negligence Claims; Health Care Risk Report; Medical Protection Society: London, UK, 2000. [Google Scholar]
- Singh, H.; Schiff, G.D.; Graber, M.L.; Onakpoya, I.; Thompson, M.J. The global burden of diagnostic errors in primary care. BMJ Qual. Saf. 2016, 1–11. [Google Scholar] [CrossRef] [Green Version]
- The Council of the European Union. Council Recommendation of 9 June 2009 on Patient Safety, Including the Prevention and Control of Healthcare Associated Infections; Official Journal of the European Union: Brussels, Belgium, 2009. [Google Scholar]
- Slawomirski, L.; Auraaen, A.; Klazinga, N. The Economics of Patient Safety: Strengthening a Value-Based Approach to Reducing Patient Harm at National Level; OECD Health Working Papers, No. 96; OECD Publishing: Paris, France, 2017. [Google Scholar] [CrossRef]
- Pettker, C.M.; Thung, S.F.; Raab, C.A.; Donohue, K.P.; Copel, J.A.; Lockwood, C.J.; Funai, E.F. A comprehensive obstetrics patient safety pro-gram improves safety climate and culture. Am. J. Obstet. Gynecol. 2011, 204, 216.e1–216.e6. [Google Scholar] [CrossRef] [PubMed]
- Donnelly, L.F.; Dickerson, J.M.; Goodfriend, M.A.; Muething, S.E. Improving patient safety: Effects of a safety program on perfor-mance and culture in a department of radiology. Am. J. Roentgenol. 2009, 193, 165–171. [Google Scholar] [CrossRef] [PubMed]
- HSE. ACSNI Human Factors Study Group: Third Report–Organising for Safety HSE Books; HSE: London, UK, 1993. [Google Scholar]
- Goh, S.C.; Chan, C.; Kuziemsky, C. Teamwork, organizational learning, patient safety and job outcomes. Int. J. Health Care Qual. Assur. 2013, 26, 420–432. [Google Scholar] [CrossRef]
- McFadden, K.L.; Henagan, S.C.; Gowen, C.R. The patient safety chain: Transformational leadership’s effect on patient safety cul-ture, initiatives, and outcomes. J. Oper. Manag. 2009, 27, 390–404. [Google Scholar] [CrossRef]
- Singla, A.K.; Kitch, B.T.; Weissman, J.S.; Campbell, E.G. Assessing Patient Safety Culture. J. Patient Saf. 2008, 2. [Google Scholar] [CrossRef]
- Singh, H.; Giardina, T.D.; Meyer, A.; Forjuoh, S.N.; Reis, M.D.; Thomas, E.J. Types and Origins of Diagnostic Errors in Primary Care Settings. JAMA Intern. Med. 2013, 173, 418–425. [Google Scholar] [CrossRef] [Green Version]
- Rosser, W.; Dovey, S.; Bordman, R.; White, D.; Crighton, E.; Drummond, N. Medical errors in primary care: Results of an interna-tional study of family practice. Can Fam. Physician 2005, 51, 386–387. [Google Scholar] [PubMed]
- Koper, D.; Kamenski, G.; Flamm, M.; Böhmdorfer, B.; Sönnichsen, A. Frequency of medication errors in primary care patients with polypharmacy. Fam. Pract. 2012, 30, 313–319. [Google Scholar] [CrossRef] [Green Version]
- Parker, D.; Wensing, M.; Esmail, A.; Valderas, J.M. Measurement tools and process indicators of patient safety culture in primary care. A mixed methods study by the LINNEAUS collaboration on patient safety in primary care. Eur. J. Gen. Pract. 2015, 21, 26–30. [Google Scholar] [CrossRef] [Green Version]
- Feng, X.; Acord, L.; Cheng, Y.; Zeng, J.; Song, J. The relationship between management safety commitment and patient safety culture. Int. Nurs. Rev. 2011, 58, 249–254. [Google Scholar] [CrossRef]
- Ricci-Cabello, I.; Avery, A.J.; Reeves, D.; Kadam, U.T.; Valderas, J.M. Measuring Patient Safety in Primary Care: The Development and Validation of the “Patient Reported Experiences and Outcomes of Safety in Primary Care” (PREOS-PC). Ann. Fam. Med. 2016, 14, 253–261. [Google Scholar] [CrossRef] [Green Version]
- Smits, M.; Keizer, E.; Giesen, P.; Deilkås, E.C.T.; Hofoss, D.; Bondevik, G.T. Patient safety culture in out-of-hours primary care services in the Netherlands: A cross-sectional survey. Scand. J. Prim. Health Care 2018, 36, 28–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bondevik, G.T.; Hofoss, D.; Hansen, E.H.; Deilkås, E.C.T. Patient safety culture in Norwegian primary care: A study in out-of-hours casualty clinics and GP practices. Scand. J. Prim. Health Care 2014, 32, 132–138. [Google Scholar] [CrossRef] [Green Version]
- Deilkås, E.C.T.; Hofoss, D.; Hansen, E.H.; Bondevik, G.T. Variation in staff perceptions of patient safety climate across work sites in Norwegian general practitioner practices and out-of-hour clinics. PLoS ONE 2019, 14, e0214914. [Google Scholar] [CrossRef] [PubMed]
- Zachariadou, T.; Zannetos, S.; Pavlakis, A. Organizational culture in the primary healthcare setting of Cyprus. BMC Health Serv. Res. 2013, 13, 112. [Google Scholar] [CrossRef] [Green Version]
- Economou, C. Greece: Health system review. Health Syst Transit. 2017, 92, 1–166. [Google Scholar]
- Agency for Healthcare Research and Quality. Medical Office Survey on Patient Safety Culture: User’s Guide; AHRQ: Rockville, MD, USA, 2016.
- Agency for Healthcare Research and Quality Home Page. Available online: https://www.ahrq.gov/sites/default/files/wysiwyg/sops/quality-patient-safety/patientsafetyculture/mosurvey-form.pdf (accessed on 18 July 2021).
- Field, A. Discovering Statistics Using IBM SPSS Statistics, 4th ed.; SAGE Publications: Thousand Oaks, CA, USA, 2013. [Google Scholar]
- Famolaro, T.; Hare, R.; Thornton, S.; Yount, N.D.; Fan, L.; Liu, H.; Sorra, J. Surveys on Patient Safety Culture TM (SOPSTM) Medical Office Survey: 2020 User Database Report. (Prepared by Westat, Rockville, MD, under Contract No. HHSP233201500026I); AHRQ Publication No. 20-0034; Agency for Healthcare Research and Quality: Rockville, MD, USA, March 2020.
- Eiras, M.; Escoval, A.; Silva, C. Patient Safety Culture in Portuguese Primary Care: Validation of the Portuguese Version of the Medical Office Survey, Vignettes in Patient Safety—Volume 4; Stawicki, S.P., Firstenberg, M.S., Eds.; IntechOpen: London, UK, 2018. [Google Scholar] [CrossRef] [Green Version]
- Hernández, V.N.; Satué, G.E.M.; Basora, G.J.; Flores, M.G.; Gens, B.M. Traducción, adaptación y valida-ción en catalán de un cuestionario sobre cultura de seguridad del paciente: El cuestionario MOSPSC (Medical Office Survey on Patient Safety Culture). J. Healthc. Qual. Res. 2019, 34, 248–257. [Google Scholar] [CrossRef] [PubMed]
- Dal, P.S.; Langendorf, T.F.; Rodrigues, M.C.S.; Romero, M.P.; Loro, M.M.; Kolankiewicz, A.C.B. Psychometric validation of a tool that assesses safety culture in Primary Care. ACTA Paul. Enferm. 2019, 32, 642–650. [Google Scholar]
- Webair, H.H.; Al-Assani, S.S.; Al-Haddad, R.H.; Al-Shaeeb, W.H.; Bin Selm, M.A.; Alyamani, A.S. Assessment of patient safety culture in primary care setting, Al-Mukala, Yemen. BMC Fam. Pract. 2015, 16, 136. [Google Scholar] [CrossRef] [Green Version]
- Raczkiewicz, D.; Owoc, J.; Krakowiak, J.; Rzemek, C.; Owoc, A.; Bojar, I. Patient safety culture in Polish Primary Healthcare Centers. Int. J. Qual. Health Care 2019. [Google Scholar] [CrossRef]
- WHO. Regional Office for Europe. Health for All Database; WHO Regional Office for Europe: Copenhagen, Denmark, 2018; Available online: http://www.euro.who.int/hfadb (accessed on 10 May 2018).
- Lancet, T. Prioritising primary care in the USA. Lancet 2019, 394, 273. [Google Scholar] [CrossRef]
- Lionis, C.; Papadakis, S.; Tatsi, C.; Bertsias, A.; Duijker, G.; Mekouris, P.B.; Boerma, W.; Schäfer, W. Informing primary care reform in Greece: Patient expectations and experiences (the QUALICOPC study). BMC Health Serv. Res. 2017, 17, 255. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Patient Safety Culture Dimensions | Definition | Items |
|---|---|---|
| Communication about error | Staff are willing to report mistakes they observe and do not feel like their mistakes are held against them, and providers and staff talk openly about office problems and how to prevent errors from happening | 4 (D7R, D8, D11,D12) |
| Communication Openness | Providers in the office are open to staff ideas about how to improve office processes, and staff are encouraged to express alternative viewpoints and do not find it difficult to voice disagreement | 4 (D7R, D8, D11, D12) |
| Office Processes and Standardization | The office is organized, has an effective workflow, has standardized processes for completing tasks, and has good procedures for checking the accuracy of work performed | 4 (C8R, C9, C12R, C15) |
| Organizational Learning | The office has a learning culture that facilitates making changes in office processes to improve the quality of patient care and evaluates changes for effectiveness. | 3 (F1, F5, F7) |
| Overall Perceptions of Patient Safety and Quality | The quality of patient care is more important than getting more work done, office processes are good at preventing mistakes, and mistakes do not happen more than they should | 4 (F2, F3R, F4R, F6R) |
| Owner/Managing Partner/Leadership Support for Patient Safety | Office leadership actively supports quality and patient safety, places a high priority on improving patient care processes, does not overlook mistakes, and makes decisions based on what is best for patients. | 4 (E1R, E2R, E3, E4R) |
| Patient Care Tracking/Follow up | The office reminds patients about appointments, documents how well patients follow treatment plans, follows up with patients who need monitoring, and follows up when reports from an outside provider are not received. | 4 (D3, D5, D6, D9) |
| Staff Training | The office provides staff with effective on-the-job training, trains staff on new processes, and does not assign staff tasks they have not been trained to perform. | 3 (C4, C7, C10R) |
| Teamwork | The office has a culture of teamwork, mutual respect, and close working relationships among staff and providers | 4 (C1, C2, C5, C13) |
| Work Pressure and Pace | There are enough staff and providers to handle the patient load, and the office work pace is not hectic | 4 (C3R, C6R, C11, C14R) |
| Services of PHU * | n (67) | (%) | |
|---|---|---|---|
| Medical | 35 | 52 | |
| Microbiology | 22 | 33 | |
| Radiology | 10 | 15 | |
| Respondents | N (459) | (%) | |
| Staff position | Nurses | 190 | 41 |
| Physicians | 95 | 21 | |
| Midwifes | 80 | 17 | |
| Administration | 55 | 12 | |
| Other | 39 | 9 | |
| Female | 312 | 68 | |
| Age of respondents | <30 years old | 50 | 11 |
| 30-39 years old | 152 | 33 | |
| 40-49 years old | 124 | 27 | |
| ≥50 years old | 116 | 25 | |
| No answer for age | 17 | 4 | |
| Primary work | Medical | 316 | 69 |
| Radiology | 45 | 10 | |
| Microbiology laboratory | 43 | 9 | |
| Clerical staff | 55 | 12 | |
| Length of time in PHU | 1 to 5 years | 115 | 25 |
| 6 to 10 years | 160 | 35 | |
| More than 10 | 184 | 40 | |
| Working hours per week | 25 to 32 h per week | 72 | 16 |
| 33 to 40 h per week | 350 | 76 | |
| ≥41 h per week | 37 | 8 |
| Items | Mean | SD | Composite 1 | Composite 2 | Composite 3 | Composite 4 | Composite 5 | Composite 6 | Composite 7 | Composite 8 |
|---|---|---|---|---|---|---|---|---|---|---|
| D11 | 4.22 | 1.106 | 0.94 | |||||||
| C2 | 4.26 | 1.067 | 0.94 | |||||||
| D8 | 4.21 | 1.081 | 0.94 | |||||||
| C5 | 4.24 | 1.101 | 0.94 | |||||||
| D12 | 4.18 | 1.051 | 0.91 | |||||||
| F5 | 4.21 | 1.108 | 0.90 | |||||||
| C13 | 4.2 | 1.045 | 0.89 | |||||||
| F7 | 4.18 | 1.152 | 0.89 | |||||||
| D1 | 4.08 | 1.183 | 0.84 | |||||||
| D2 | 4.06 | 1.154 | 0.80 | |||||||
| F1 | 4.01 | 1.084 | 0.68 | |||||||
| D7R | 3.83 | 1.168 | 0.66 | |||||||
| E3 | 4.07 | 1.252 | 0.57 | |||||||
| E2R | 3.85 | 1.168 | 0.87 | |||||||
| D10R | 3.59 | 1.345 | 0.86 | |||||||
| E4R | 3.67 | 1.368 | 0.83 | |||||||
| D4R | 3.8 | 1.305 | 0.77 | |||||||
| C12R | 4.02 | 1.136 | 0.86 | |||||||
| C8R | 4.2 | 1.063 | 0.84 | |||||||
| C15 | 3.83 | 1.268 | 0.77 | |||||||
| C9 | 3.81 | 1.071 | 0.77 | |||||||
| C3R | 3.49 | 1.443 | 0.85 | |||||||
| E1R | 3.38 | 1.432 | 0.84 | |||||||
| C14R | 3.84 | 1.318 | 0.74 | |||||||
| F4R | 3.93 | 0.899 | 0.95 | |||||||
| F3R | 3.95 | 0.877 | 0.95 | |||||||
| F6R | 3.94 | 1.152 | 0.65 | |||||||
| C7 | 3.83 | 1.046 | 0.88 | |||||||
| C4 | 3.75 | 0.97 | 0.88 | |||||||
| C10R | 3.57 | 1.272 | 0.73 | |||||||
| D5 | 3.97 | 1.111 | 0.97 | |||||||
| D6 | 4.04 | 1.098 | 0.96 | |||||||
| C11 | 3.59 | 1.307 | 0.86 | |||||||
| C6R | 3.39 | 1.357 | 0.81 |
| MOSPSC Factor Analysis | G-MOSPSC * Factor Analysis | |||||
|---|---|---|---|---|---|---|
| Composites | Items | Cronbach’s α American Data | Cronbach’s α Greek Data | Composites | Items | Cronbach’s α |
| 1. Teamwork | 4 | 0.83 | 0.82 | 1. Teamwork (C2, C5, C13) + 3. Organizational learning (F1, F5, F7) + 6. Owner/Managing Partner/Leadership Support for Patient Safety (E3) + 7. Communication About Error + 8. Communication Openness (D1, D2) | 13 | 0.96 |
| 2. Patient Care Tracking/Follow up | 4 | 0.78 | 0.74 | 2. Patient Care Tracking/Follow up (D5, D6) | 2 | 0.964 |
| 3. Organizational learning | 3 | 0.82 | 0.80 | 4. Overall Perceptions of Patient Safety and Quality (F4R, F3R, F6R) | 3 | 0.834 |
| 4. Overall Perceptions of Patient Safety and Quality | 4 | 0.74 | 0.70 | 5. Staff Training * | 3 | 0.790 |
| 5. Staff Training | 3 | 0.63 | 0.72 | 6. Owner/Managing Partner/Leadership Support for Patient (E2R, E4R) + 8. Communication Openness (D4R, D10R) | 4 | 0.890 |
| 6. Owner/Managing Partner/Leadership Support for Patient Safety | 4 | 0.76 | 0.71 | 6. Owner/Managing Partner/Leadership Support for Patient Safety(E1R) + 10. Work Pressure and Pace(C3R, C14R) | 3 | 0.838 |
| 7. Communication About Error | 4 | 0.80 | 0.72 | 9. Office Processes and Standardization * | 4 | 0.839 |
| 8. Communication Openness | 4 | 0.81 | 0.72 | 10. Work Pressure and Pace (C11, C6R) | 2 | 0.692 |
| 9. Office Processes and Standardization | 4 | 0.78 | 0.71 | |||
| 10. Work Pressure and Pace | 4 | 0,76 | 0.72 | |||
| Patient Safety Culture Composite Measures | Average (%) Positive Response | |
|---|---|---|
| AHRQ Database | This Study | |
| Patient Care Tracking/Follow up | 88 | 80 |
| Teamwork | 86 | 82 |
| Organizational Learning | 81 | 80 |
| Overall Perceptions of Patient Safety and Quality | 80 | 77 |
| Staff Training | 75 | 70 |
| Communication About Error | 74 | 70 |
| Communication Openness | 72 | 64 |
| Office Processes and Standardization | 70 | 67 |
| Owner/Managing Partner/Leadership Support for Patient Safety | 69 | 62 |
| Work Pressure and Pace | 49 | 46 |
| This Study (%) | AHRQ Database 2020 | ||
|---|---|---|---|
| Excellent/Very Good | Excellent/Very Good | ||
| Overall rating on quality issues | Patient centered | 75 | 71 |
| Effective | 75 | 71 | |
| Timely | 65 | 56 | |
| Efficient | 63 | 62 | |
| Equitable | 85 | 84 | |
| Overall rating on patient safety | 70 | 68 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Antonakos, I.; Souliotis, K.; Psaltopoulou, T.; Tountas, Y.; Papaefstathiou, A.; Kantzanou, M. Psychometric Properties of the Greek Version of the Medical Office on Patient Safety Culture in Primary Care Settings. Medicines 2021, 8, 42. https://doi.org/10.3390/medicines8080042
Antonakos I, Souliotis K, Psaltopoulou T, Tountas Y, Papaefstathiou A, Kantzanou M. Psychometric Properties of the Greek Version of the Medical Office on Patient Safety Culture in Primary Care Settings. Medicines. 2021; 8(8):42. https://doi.org/10.3390/medicines8080042
Chicago/Turabian StyleAntonakos, Ioannis, Kyriakos Souliotis, Theodora Psaltopoulou, Yannis Tountas, Athanasios Papaefstathiou, and Maria Kantzanou. 2021. "Psychometric Properties of the Greek Version of the Medical Office on Patient Safety Culture in Primary Care Settings" Medicines 8, no. 8: 42. https://doi.org/10.3390/medicines8080042